Embed Size (px)
Citation preview
1
THROMBOSIS
Karmel L. Tambunan, Lugyanti Sukrisman
Div of Hematology-Medical Oncology
Dept of Internal Medicine
Faculty of Medicine, Univ of Indonesia

2
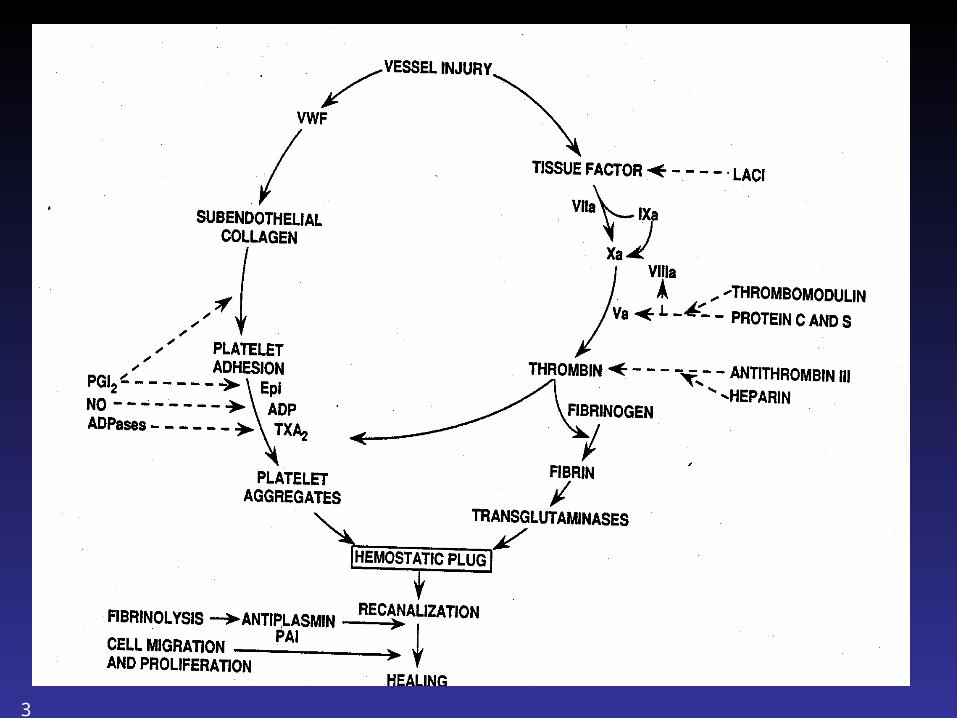
Overview of Hemostasis
Vascular Injury
Platelet adhesion& aggregation
Vasoconstriction Blood coagulation
HEMOSTASIS
Exposed subendothelium
Exposed tissue factor
thrombin
PF3
3
4
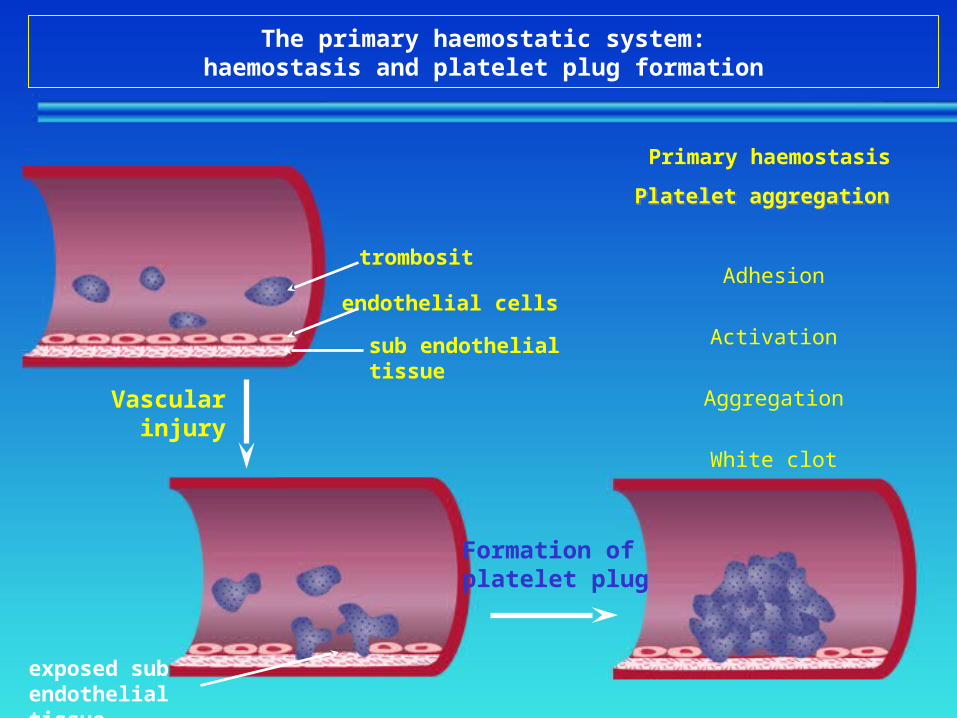
The primary haemostatic system:haemostasis and platelet plug formation
Vascularinjury
Formation ofplatelet plug
exposed sub endothelial tissue
trombosit
endothelial cells
sub endothelial tissue
Platelet aggregationPlatelet aggregation
Adhesion
Activation
Aggregation
White clot
Primary haemostasis

5
The haemostatic system:secondary haemostasis and clot formation
ThrombinProthrombin
FibrinExtrinsic pathway
Intrinsic pathway
Factor Xa
Fibrin threads
Coagulation cascadeleads to clot formation
Clot growth
Fibrinogen
Activation of the coagulation cascade leads to generation of thrombin and, in turn, fibrin
6
7
What is thrombosis ?
Thrombosis is the formation or presence of a blood clot inside a blood vessel or cavity of the heart

8
Thrombosis
1. Arterial thrombosis (white thrombus)
2. Venous thrombosis (red thrombus)
9
Thrombosis
Mortality : Cause of death (>60%) in the western country
(Turpie G.L., 1996) About 2 million individual die each year from
an arterial or venous thrombosis or of the consequence thereof (Bick R.L., 1997)

10
Thrombosis
Morbidity : Paralysis (non fatal thrombotic state) Cardiac disability (repeated coronary event) Fetal loss syndrome (placenta vascular
thrombosis) Loss of vision (retinal vascular thrombosis) Loss of hearing (?) Stasis ulcers and others manifestations of
postphlebitic syndrome (recurrent DVT)
11
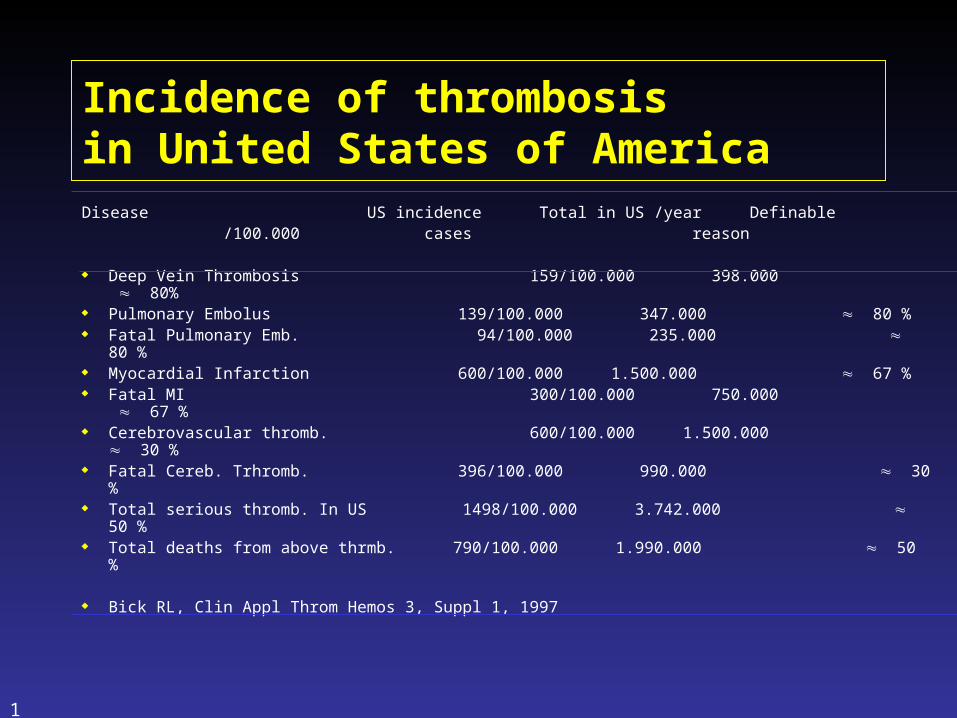
Incidence of thrombosis in United States of AmericaDisease US incidence Total in US /year Definable
/100.000 cases reason
Deep Vein Thrombosis 159/100.000 398.000 80%
Pulmonary Embolus 139/100.000 347.000 80 % Fatal Pulmonary Emb. 94/100.000 235.000 80 % Myocardial Infarction 600/100.000 1.500.000 67 % Fatal MI 300/100.000 750.000 67 % Cerebrovascular thromb. 600/100.000 1.500.000 30 % Fatal Cereb. Trhromb. 396/100.000 990.000 30 % Total serious thromb. In US 1498/100.000 3.742.000 50 % Total deaths from above thrmb. 790/100.000 1.990.000 50 %
Bick RL, Clin Appl Throm Hemos 3, Suppl 1, 1997

12
CV thrombosis1,000,000
Other causes400,000
COPD90,000
Cancer500,000
Pulmonary disease/flu80,000
Trauma/accident90,000
Leading causing Mortality in the USA
Semin Thromb 21,Sup 1, 2000
13
Thrombosis in Indonesia
Epidemiology data: not available Mortality The first cause of death 20.5%, (11.8 % cerebrovascular, 8.7 % coronary
heart disease) (Ministry of Health 1997)
14
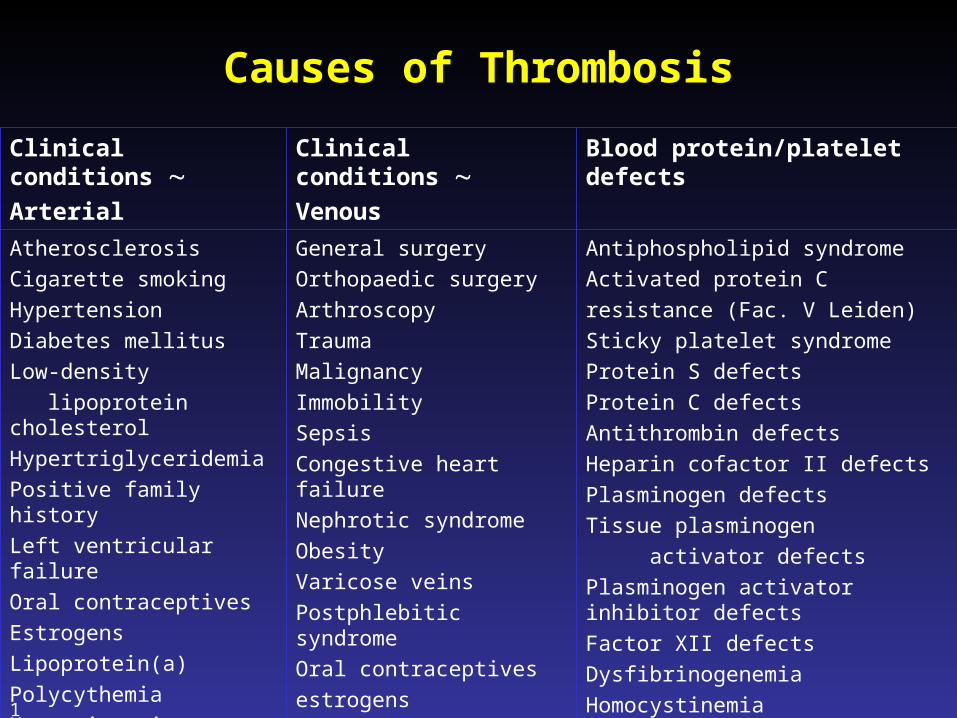
Causes of Thrombosis
Clinical conditions Arterial
Clinical conditions Venous
Blood protein/platelet defects
Atherosclerosis
Cigarette smoking
Hypertension
Diabetes mellitus
Low-density
lipoprotein cholesterol
Hypertriglyceridemia
Positive family history
Left ventricular failure
Oral contraceptives
Estrogens
Lipoprotein(a)
Polycythemia
Hyperviscosity syndrome
Leukostasis syndromes
General surgery
Orthopaedic surgery
Arthroscopy
Trauma
Malignancy
Immobility
Sepsis
Congestive heart failure
Nephrotic syndrome
Obesity
Varicose veins
Postphlebitic syndrome
Oral contraceptives
estrogens
Antiphospholipid syndrome
Activated protein C
resistance (Fac. V Leiden)
Sticky platelet syndrome
Protein S defects
Protein C defects
Antithrombin defects
Heparin cofactor II defects
Plasminogen defects
Tissue plasminogen
activator defects
Plasminogen activator inhibitor defects
Factor XII defects
Dysfibrinogenemia
Homocystinemia
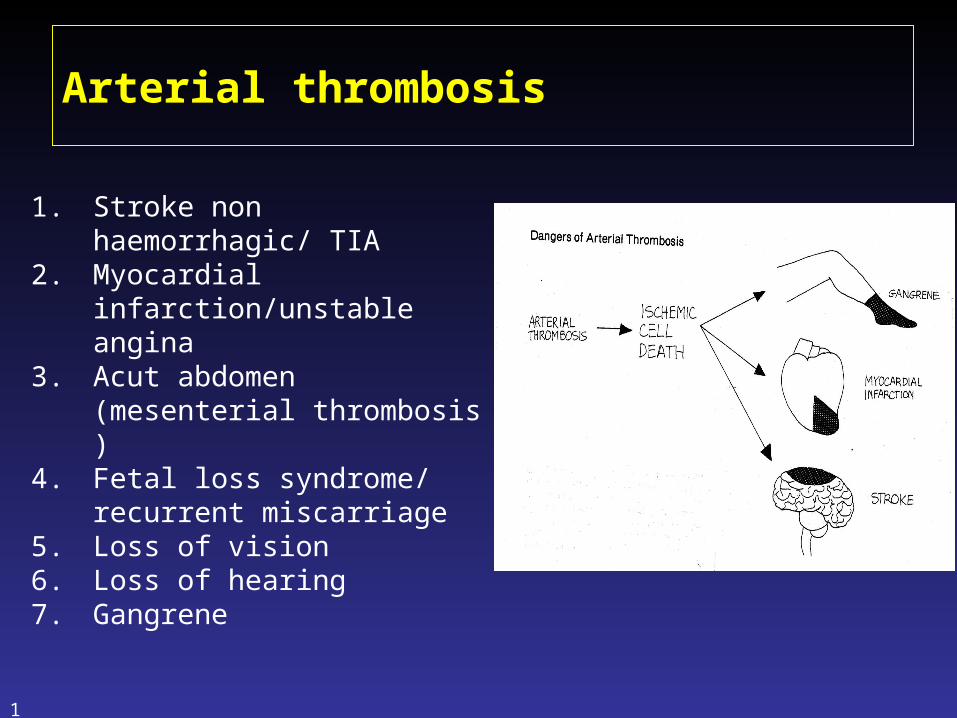
Arterial thrombosis
1. Stroke non haemorrhagic/ TIA
2. Myocardial infarction/unstable angina
3. Acut abdomen (mesenterial thrombosis )
4. Fetal loss syndrome/ recurrent miscarriage
5. Loss of vision6. Loss of hearing7. Gangrene
15
16
17
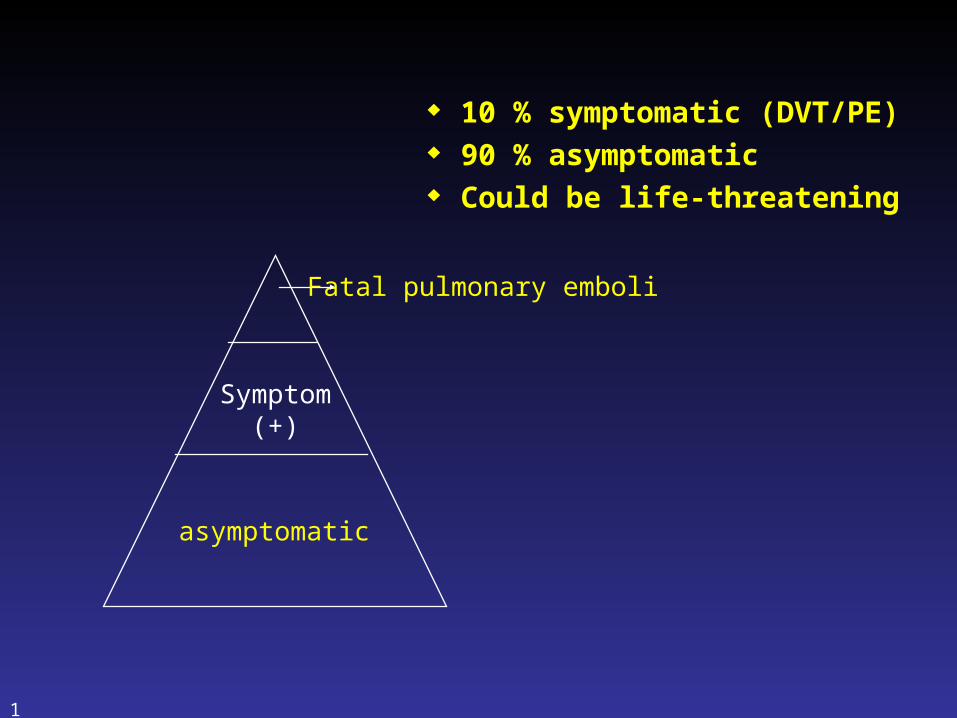
10 % symptomatic (DVT/PE) 90 % asymptomatic Could be life-threatening
asymptomatic
Symptom(+)
Fatal pulmonary emboli

18
Venous stasis Parietal lesion Coagulation anomaly
Age > 60 yrs +
obesity + +
pregnancy + +
Immobilization or paralysis +
Orthopaedic surgery + + +
Trauma of lower limbs + + +
Cardiac insufficiency +
Myocardial infarction (acute phase)
+ +
Stroke + +
Cancer + +
General surgery + + +
Inherited or acquired haemostasis deficiencies
+
Venous insufficiency or varicosis
+ +
Previous history of DVT + + +

19
20
Primary risk factors for VTEPrimary risk factors for VTE
Major surgeryMajor surgery Acute MIAcute MI Major traumaMajor trauma Paralytic strokeParalytic stroke CancerCancer Spinal cord injurySpinal cord injury Pelvic fracturePelvic fracture
21
Secondary risk factors for VTE
Haematological Haematological disordersdisorders
Central venous Central venous cathethercathether
Varicose veinsVaricose veins PregnancyPregnancy Oestrogen treatmentOestrogen treatment HospitalizationHospitalization
Congestive heart Congestive heart failure failure
Previous VTEPrevious VTE ImmobilizationImmobilization ObesityObesity Chronic Chronic
respiratory failurerespiratory failure Increasing ageIncreasing age
22
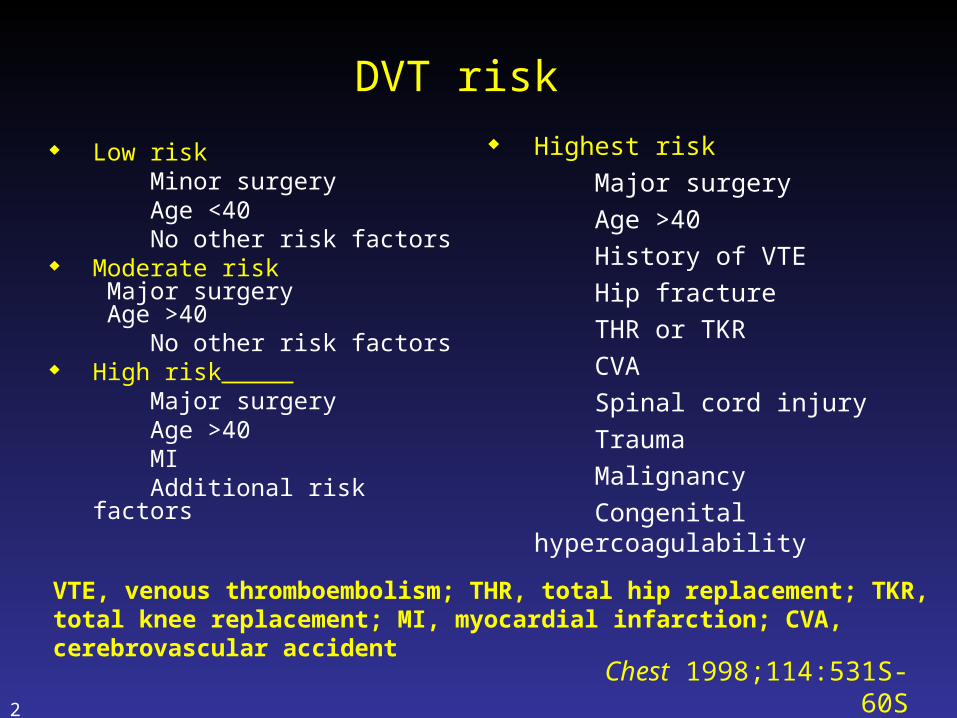
DVT risk
Low risk Minor surgery Age <40 No other risk factors Moderate risk
Major surgery Age >40
No other risk factors High risk Major surgery Age >40 MI Additional risk factors
Highest risk
Major surgery
Age >40
History of VTE
Hip fracture
THR or TKR
CVA
Spinal cord injury
Trauma
Malignancy
Congenital hypercoagulability
Chest 1998;114:531S-60S
VTE, venous thromboembolism; THR, total hip replacement; TKR, total knee replacement; MI, myocardial infarction; CVA, cerebrovascular accident
23
Pathogenesis : Triad Virchow
1. Vascular lesion/disruption
2. Blood component (coagulation imbalance)
3. Venous stasis
24
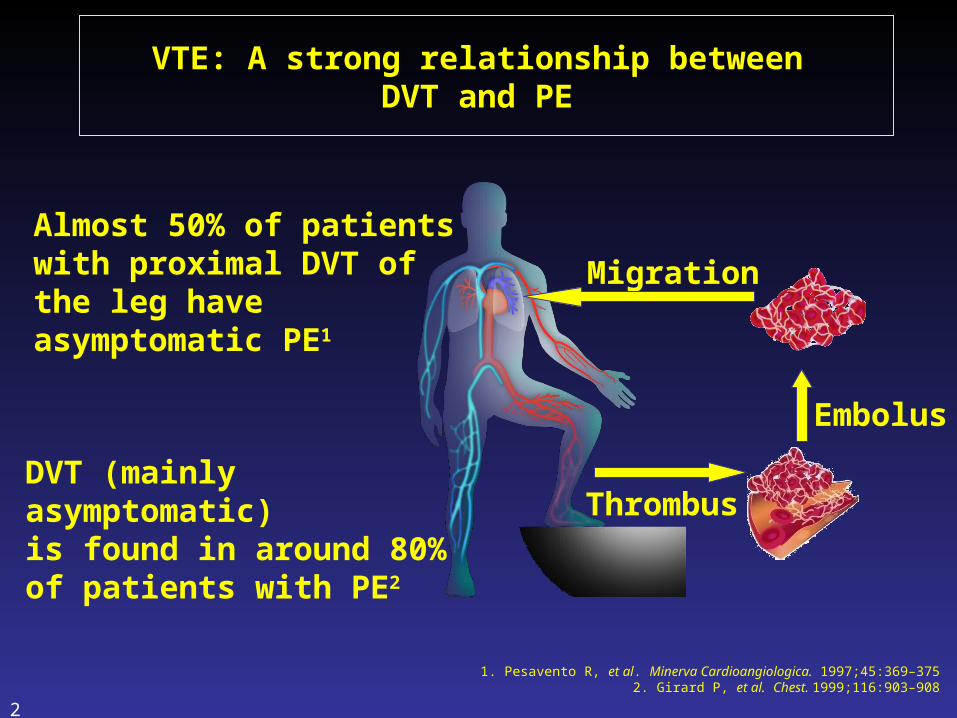
VTE: A strong relationship between DVT and PE
Almost 50% of patients with proximal DVT of the leg have asymptomatic PE1
DVT (mainly asymptomatic) is found in around 80% of patients with PE2
1. Pesavento R, et al. Minerva Cardioangiologica. 1997;45:369–3752. Girard P, et al. Chest. 1999;116:903–908
Embolus
Migration
Thrombus
DIAGNOSIS OF VTE: CLINICAL FINDINGS
DVT: Non specific Pain, tenderness, unilateral leg swelling,
superficial venous dilatation PE:
Dyspnea, pleuritic pain, cough, hemoptysis
Clinical prediction score for DVT/PE Laboratory test: D-dimer
Hypoxemia, hypocapnia (PE)
25
DIAGNOSIS OF VTE: RADIOIMAGING
DVT: Venography/phlebography (gold standard) Compression ultrasonography (CUS) Venous Doppler/duplex scanning
PE: CXR: cardiomegaly, pleural effusion, atelectasis,
elevated hemidiaphragm Pulmonary angiography (gold standard) Ventilation-perfusion lung scintigraphy Spiral CT
26
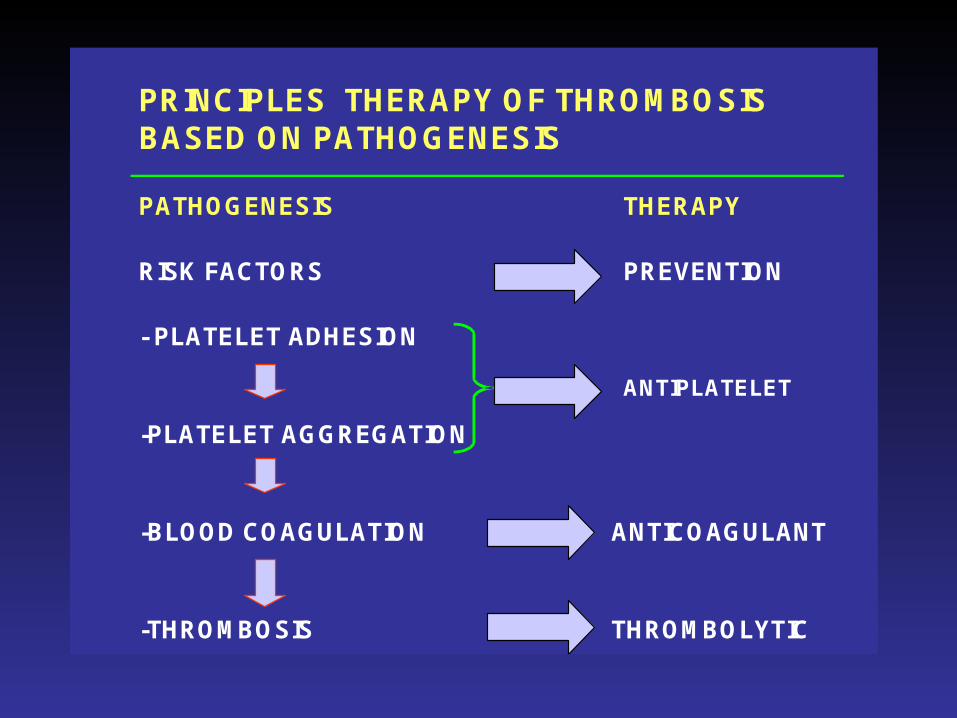
PRINCIPLES THERAPY OF THROMBOSIS BASED ON PATHOGENESIS
PATHOGENESIS THERAPY
RISK FACTORS PREVENTION
- PLATELET ADHESION
-PLATELET AGGREGATION
-BLOOD COAGULATION ANTICOAGULANT
-THROMBOSIS THROMBOLYTIC
ANTIPLATELET
28
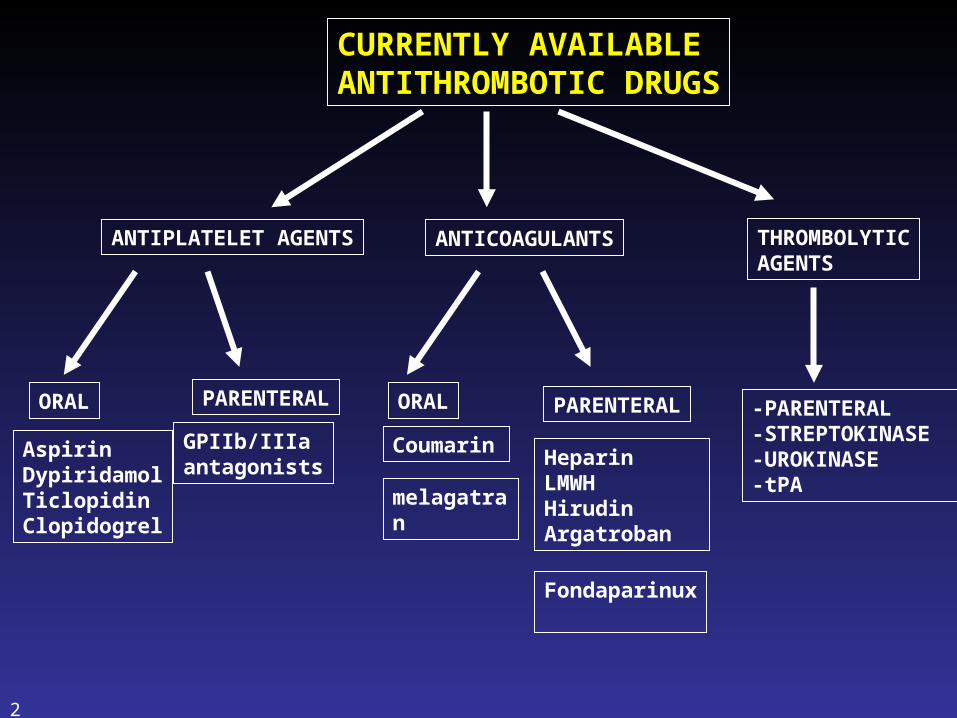
CURRENTLY AVAILABLEANTITHROMBOTIC DRUGS
ANTIPLATELET AGENTS ANTICOAGULANTS
ORAL PARENTERAL ORAL PARENTERAL
AspirinDypiridamolTiclopidinClopidogrel
GPIIb/IIIaantagonists
CoumarinHeparinLMWHHirudinArgatroban
melagatran
THROMBOLYTICAGENTS
-PARENTERAL-STREPTOKINASE-UROKINASE-tPA
Fondaparinux

29
Complications ofDeep Vein Thrombosis
• Permanent vascular damage to lower limb
• Post thrombotic venous insufficiency
• Postphlebitic syndrome
• Pulmonary embolism (PE)
• Pulmonary hypertension

32
POST THROMBO-PHLEBITIC SYNDROME

VTE PROPHYLAXIS
33
34
Thank you
35





























