Embed Size (px)
Citation preview

1
The June 1999 Draft BA/BE Guidance for Nasal Aerosols and Nasal Sprays:
History, Recommendations and Local Delivery Issues
Wallace P. Adams, Ph.D.
OPS/CDER/FDA
Orally Inhaled and Nasal Drug Products (OINDP) Subcommittee of Advisory Committee for
Pharmaceutical ScienceRockville, MD17 July 2001

2
NASAL AEROSOLS (MDIs) AND NASAL SPRAYS*
Corticosteroids
Anticholinergics
Antihistamines
Cromones*Draft FDA Guidance for Industry: BA and BE Studies for Nasal Aerosols
and Nasal Sprays for Local Action, June 1999

3
OUTLINE
• History
• Guidance Recommendations for BE– formulation and device– in vitro studies– in vivo studies
• Local Delivery BE Issues

4
History (a)
• Patent or exclusivity expiration dates– Beconase AQ (Glaxo)- 27 July 1990
• September 1993– GDAC with PADAC Representation meeting
– BE of nasal solution formulations may be established with in vitro testing only
• April 1995– CDER internal memo
• For BE of generic aqueous suspension nasal sprays
– Q1 and Q2 sameness
– comparative in vitro data
– multiple dose PK study

5
History (b)• December 1996 letter to FDA
– OGD requirements for BE of aqueous suspension nasal sprays do not require data on drug PSD, thus are inadequate to assure BE
– Drug PSD affects rate and extent of dissolution and absorption from aqueous suspension nasal sprays to sites of action
• May 1997– OINDP Technical Committee organized
• June 1999– Issuance of draft guidance, BA and BE Studies for
Nasal Aerosols and Nasal Sprays for Local Action
– AAPS Workshop on Regulatory Issues Related to Drug Products for Oral Inhalation and Nasal Delivery

6
History (c)
• November 1999– OINDP Expert Panel organizational meeting
• April 2000– OINDP Subcommittee of ACPS meeting
• November 2000– OINDP Subcommittee report to ACPS

7
METHODS FOR DOCUMENTATION OF BE*
• In vivo studies in humans comparing drug or active metabolite in an accessible biologic fluid
• In vivo studies in humans comparing a pharmacodynamic endpoint
• Comparative clinical trials to demonstrate bioequivalence
• Comparative in vitro studies• See 21 CFR 320.24 for details

8
APPLICATION OF BE STUDIES
• FOR NDA’s– To-be-marketed product comparable to
clinical trial product
• FOR ANDA’S– Generic product BE to innovator product
• FOR NDA’s and ANDA’s– Certain postapproval changes

9
BE RECOMMENDATIONSFormulation Equivalence
• Qualitative sameness (Q1)– identical active and inactive ingredients as in
the RLD
• Quantitative sameness (Q2)– inactive ingredients within ± 5% of the
concentrations in the RLD
10
BE RECOMMENDATIONSThe Device
• Assurance of equivalence:– is greatest when T uses the same brand and
model (particularly the metering valve or pump and actuator) as used in R.
– if not feasible, valve or pump, and actuator designs should be as close as possible in all critical dimensions (e.g., metering chamber volume, actuator orifice diameter)

11
BE RECOMMENDATIONS Comparable In Vitro Performance (a)
• Dose content uniformity through container life
• Droplet and particle size distribution

12
BE RECOMMENDATIONS: Comparable In Vitro Performance (b)
• Spray pattern
• Plume geometry
• Priming and repriming
• Tailoff characteristics

13
LOCAL DELIVERYClinical Endpoint in SAR Patients
• Dose-response– To document sensitivity
• Traditional treatment study
• Day(s) in the park study
• Environmental Exposure Unit (EEU) study

14
SYSTEMIC EXPOSURE STUDY (PK)
• Randomized, two-way crossover
• Healthy (non-SAR) subjects
• Single or multiple dose
• Multiple actuations per dose to achieve measurable plasma concentrations, if necessary– minimize drug loss from fluid drainage
• AUC and Cmax measures
• Two one-sided tests procedure (ANOVA)

15
SYSTEMIC ABSORPTION STUDY (PD)
• When PK study is not feasible - HPA axis suppression study for nasal corticosteroids– Healthy, nonallergic subjects– Randomized, placebo-controlled, parallel group
study– Conduct at maximum labeled dose for 14 days– 24-hr urinary free cortisol or 24-hr serum
cortisol, data baseline-adjusted

16
BE RECOMMENDATIONS(OVERVIEW)
• Q1 and Q2 sameness
• Device recommendations• Comparable in vitro performance• Comparable in vivo performance for local
delivery– suspension formulation nasal sprays and nasal
aerosols only • Comparable in vivo performance for systemic
exposure or absorption– suspension formulation nasal sprays and nasal
aerosols only

17
THE LOCAL DELIVERY ISSUES*• Clinical study may be crucial to establish
BE for local delivery
• Dose-response relationship– may not be possible to show– may not be consistently reproducible
• Clinical study should document sensitivity– between different doses– doses may differ by two to fourfold– minimum dose not less than one spray per
nostril daily• *Draft FDA Guidance for Industry: BA and BE Studies for Nasal Aerosols and Nasal
Sprays for Local Action, June 1999

18
DOSE-RESPONSE
Dose
% M
axim
um R
espo
nse
EfficacySafety
Red
uce
d
effi
cacy
Reduced safety
Res
pons
e E
quiv
alen
ce
Adapted from JN Pritchard, ANZSRS Annual Meeting, Brisbane, 16-19 Mar 2001

19
PROPOSAL FOR BE STUDYNASAL SUSPENSION AEROSOLS AND SPRAYS
• Formulation recommendations
• Device recommendations
• In vitro studies
• In vivo studies– rhinitis study (lowest active dose)
– PK study (high dose)• alternate: PD study

20
ACKNOWLEDGMENTS
FDA/CDER OINDP Technical CommitteeHelen WinkleAjaz Hussain, Ph.D.Roger Williams, M.D.

21
BCC and CMC CCLocally Acting Drug Products
ComparativeClinical
Pharmacodynamic
In VitroBioavailability/Bioequivalence
Inhalation DrugProducts*
Comparability of Inactive Ingredients
Comparative SystemicAbsorption (Safety) Study
Working GroupsOral Inhalation and Nasal Drug Products
Wallace Adams (Chair)Badrul Chowdhury Mary FanningLydia Gilbert-McClain Robert Meyer
Gur Jai Pal Singh (Chair)Wallace Adams Dale ConnerStella Machado Robert MeyerDonald Schuirmann Sandra SuarezEugene Sullivan
Wallace Adams (Chair)James Allgire Charles BrownellDale Conner Moheb NasrRabindra Patnaik Pradeep SatheGur Jai Pal Singh Yi Tsong
Guirag Poochikian (Chair)Craig Bertha Timothy McGovernRobert Meyer Michael Smela
Donald Hare
Debra Birenbaum Tien-Mien (Albert) ChenYoung Moon Choi Dale ConnerRobert Meyer Gur Jai Pal SinghSandra Suarez
23 April 2001* A CMC CC Working Group

22
THE END

23
PROPOSED BE CRITERION FOR NONPROFILE DATA
• Evaluates– mean performance of T and R products– variability of R product– variability of T product
• Based on– difference between T and R means– difference between T and R variances– scaling of BE boundaries to RLD variance
• Uses one-sided 95% upper confidence bound– alpha = 0.05

24
PROPOSED BE CRITERION FOR NONPROFILE DATA:In Vitro Population BE Criterion
and BE Limit
limit (upper) BE vitroin
deviation standard stage life betweencanister Rand T within,
variancesbatch-between includes
scale); (log deviations standard Rand Tcanister between,
scale) (log means Rand T ,
CT
222T
222R
T
LRLT
CR
LTCT
LRCR
R
2
222
R
RTRT
25
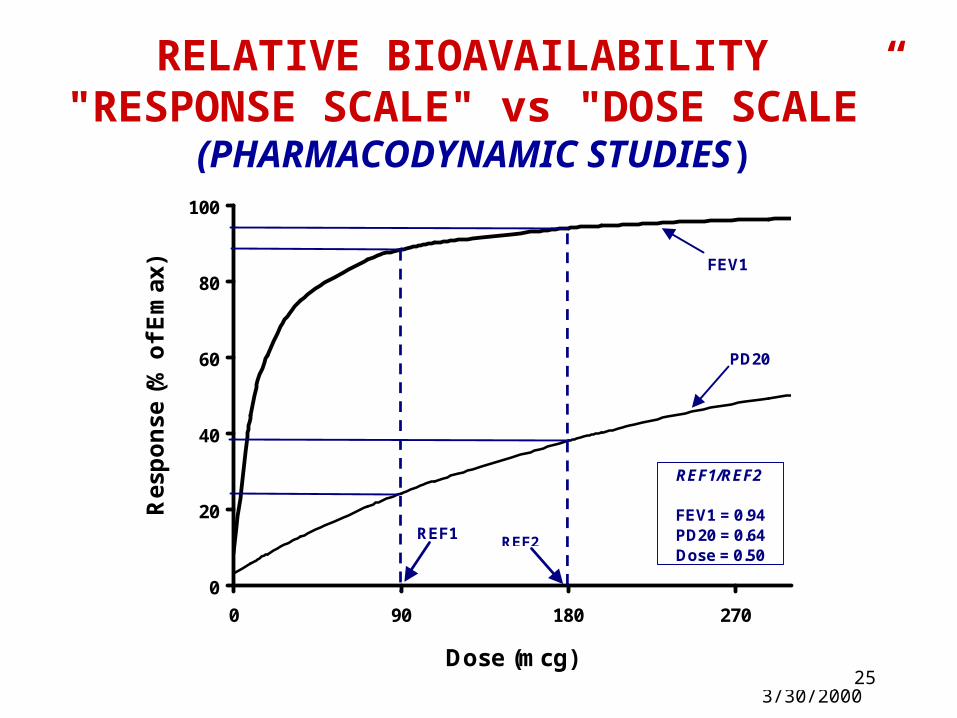
RELATIVE BIOAVAILABILITY "RESPONSE SCALE" vs "DOSE SCALE”
(PHARMACODYNAMIC STUDIES)
GJPS 3/30/2000
Dose09
18367290
108180198288576
90/180
0
20
40
60
80
100
0 90 180 270
Dose (mcg)
Res
po
nse
(%
of
Em
ax) FEV1
PD20
REF1REF2
REF1/REF2
FEV1 = 0.94PD20 = 0.64Dose = 0.50

26
DATA ANALYSIS
• Clinical Study (Rhinitis)– Under discussion
• Change from baseline data have continuous and noncontinuous (categorical) aspects
• HPA Suppression Study (PD)– To be drafted
• Systemic Exposure Study (PK)– Two one-sided tests procedure (ANOVA)
GJPS 3/30/2000





























