Embed Size (px)
Citation preview

1
Statistical ReviewDRAFT
Barbara Krasnicka, Ph.D.
FDA, CDRH
Division of Biostatistics

2
Objective of the Submission
To present the effectiveness and safety of the Cardica® PAS-Port Proximal Anastomosis System use in patients requiring CABG

3
Studies of Interest Submission was based on (utilized results
of) 4 studies The Pivotal Study Conducted under the
Investigational Plan CP2001-01; Study 1 A prospective, nonrandomized, multi-center
follow-up study (CP 2004-03) carried out to evaluate long-term health status of patients from study CP2001-01
The C-Port Study Conducted under the Investigational Plan CP2002-02; Study 2
A prospective, nonrandomized, multi-center follow-up study to evaluate long-term (about 1 year) health status of C-Port patients

4
Pivotal Study –General Characteristics
Conducted under the Investigational Plan CP2001-01 Prospective, non-randomized, one-arm Conducted in 2 German and 1 Swiss clinical sites
from June 2002 to March 2003 Objective: Assess ease of PAS-Port device use,
identify any procedural failure, and evaluate safety and efficacy of the PAS-Port System
Undefined hypothesesCarried out without IDE

5
Pivotal Study – Plan of Evaluations
Four main evaluations:pre-operative (coronary angiography)
at discharge from hospital (coronary angiography)
three month post-operative assessment
six month post-operative (coronary angiography)

6
Primary Effectiveness Endpoint (post-hoc process)
Primary endpoint: Patency of a PAS-Port graft at 6 months assessed by angiographyPatency: stenosis < 50% in the proximal
anastomosis related to a PAS-Port graft The PAS-Port graft patency rate at 6 months is
to be compared to the fixed OPC (OPC: Objective Performance Criterion) number equal 80%
The historical control rate was 85% with lower confidence limit (LCL) of 95% CI equal 80%.

7
Other Effectiveness and Safety Endpoints (post-hoc process)
Patency of a proximal anastomosis of a PAS-Port graft at 12 months as assessed by stress ECG
Occurrence and Frequency of MACE (myocardial infarction, mortality and revascularization) at one year estimated in connection with stress ECG
Any adverse event –safety endpoint

8
Patient Disposition – CP2001-01
Sixty patients signed consent form Five patients were eliminated based on the intra-
operative screening process. 55 patients finally enrolled in the study (ITT
population) Implantations of the PAS-Port for 47 (85%) patients
were successful Devices were not implanted successfully for 8 (15%)
patients (10 attempts , 10 technical device failures) 6 month evaluation was performed for only 80%
(44/55) of enrolled patients

9
Primary Effectiveness Endpoint Main Results
Observed patency rate (based on the angiography at 6 months) is 0.86 (36/42), 95% CI (0.71,0.95)
With patency imputed based on MRI, the patency rate is 0.87 (41/47), 95% CI (0.74, 0.95)

10
Primary Effectiveness EndpointSensitivity Analysis
For the ITT population, when considering all technical failures, all grafts in deceased patients and grafts without additional clinical information indicating patency as occluded, the patency rate is 0.72 (43/60), with 95% CI (0.59, 0.83)

11
Primary Effectiveness EndpointSummary
Point estimates
Lower confidence limits of the 95% CI for the patency rates for different methods of assessment are all below the recommended 80% level

12
MACE Frequencies
Kaplan Meier estimate of MACE frequency rates
MACE is defined as: myocardial infarction, mortality, and revascularization related to the PAS-Port device

13
Problems with MACE Evaluations
MACE rate at 6 month +15 days is 13% i.e., much higher than 4.4%
Only 39 (71%) of 55 patients were evaluated at 6 months by angiography
Lack of question on adverse event occurrence history in the so-called ’12 month’ Case Report Form.
7 patients who withdrew at the baseline were re-enrolled for the 2 year evaluation. But only 4 of them received the stress ECG test. Despite that, the sponsor qualified all 7 patients as MACE free during 2 years after procedure

14
Safety Endpoint - Results
Summary of Adverse Events

15
Safety Endpoint - Problems
Two patients died during the follow-up period between the 6th and 24th month visits
10 technical failures (8 patients) of the device use were not included in the adverse events analysis

16
Limitations of Analyses
The effectiveness endpoint was not met either for ITT, or for the per protocol or for the observed populations.
Point estimates, endpoints of confidence intervals may be biased
Post-hoc analyses
Small data set, only 55 patients (60 grafts)
Missing information (only 42 (70%) grafts were evaluated by angiography)
Study was carried out without IDE

17
Limitations of Analyses
Procedures performed in only 3 sites outside US
Comparison of 12 month MACE rates for the pivotal study with the CABG historical data is inadequate.

18
CP2002-02 Study – General Characteristics
Prospective, non-randomized, multi-center (4 in Germany and 1 in Switzerland) study
Objective was to assess safety and effectiveness of the C-Port Distal Anastomosis System
Some patients (52/118 = 44%) with multiple vein grafts received the PAS-Port device
The PAS-Port placement was based on surgeons’ discretion and was determined by aorta disease state and preferred grafting sequence.

19
Cohort 2 - Characteristics A subset of the CP2002-2 data used as a
complementary data set for the pivotal study Not a separate clinical study Data set on the PAS-Port system for Cohort 2
was created without stringent clinical rules normally imposed on device clinical studies
Data extracted from a broader data set collected for other purposes
Biases embedded in the data impossible to estimate .

20
Comparisons of Studies Evaluation of the PAS-Port system in Cohort 2 was
retrospective in conjunction with evaluation of another not approved by the FDA anastomosis system
The PAS-Port systems used in pivotal study and Study 2 were not exactly the same; the PAS-Port System was improved during and after pivotal study
Populations of two studies were different with respect to patients’ pre-operative variables (e.g., angina, age, CCS class) and intra-operative covariates (e.g., duration of surgery)

21
Comparisons of Studies-Propensity Score
The sponsor presented justification of pool-ability of the two data sets using the propensity score method
Propensity score may be used to some extent as a diagnostic tool to show comparability between the pivotal study cohort and Cohort 2
If two groups overlap well enough in terms of propensity scores, then it is possible to check the influence of ‘cohort effect’ on the outcome variable adjusted for baseline differences.

22
Propensity Score
The propensity score for a patient can be defined as a conditional probability of patient being assigned to Cohort 2, given the patient’s covariates
Can be used to balance the covariate differences of two groups
Can be seriously degraded if important covariates have not been collected or not taken into account in the analysis
Most of the observed covariates should be considered in the analysis.

23
Sponsor’s Propensity Score Analysis
The propensity score analysis was carried out in two steps: 1. predictors of angiographic patency (diabetes,
smoking history, vessel disease) were found2. the propensity scores were calculated for each
patient based on patency predictors Based on the propensity scores, the sponsor
grouped patients into three sub-groups and compared the outcome variable adjusted for baseline differences (p=0.22)
The sponsor claimed that the pool-ability of two data sets was justified.

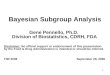
24
Distribution of Sponsor’s Propensity Score

25
Limitation of the Sponsor’s Analysis
Sponsor’s propensity score analysis could not provide statistical justification that results from two cohorts were poolable because:Propensity scores were based only on three
covariates which were predictors of patencySome important covariates (e.g., duration of
operation..) were not included in the analysisData set was very small

26
Propensity Score Analysis Model Building
A logistic regression model with a stepwise selection was utilized to build the propensity score model
The final propensity score model included the following covariates: Age, Angina, CCS, Gender, Hyperlipidemia, Vessel disease, NYHA, # of proximal anastomosis, Use of aspirin within 5 days of operation

27
Model Building
The entire population (109 pts) was divided into propensity score third-tiles, with 36 patients in each third-tile
One patient was excluded because she/he did not have CCS
Most patients from Cohort 2 was in the in 3rd and 2nd third-tiles (36 and 16 patients, respectively)

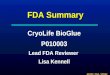
28
Propensity Score Distribution

29
Conclusion of Propensity Score Analysis
Propensity score distributions for the pivotal study and Cohort 2 do not overlap at all and do not support the sponsor’s pool-ability conclusion

30
Final Conclusions
No statistical support for combining two data sets (Pivotal Study and Cohort 2) does exist. Therefore, no statistical analysis for the combined data will be presented
A subset of the CP2002-2 data ( Cohort 2) is not a separate clinical study

31
Final Conclusions
Pivotal Study alone did not supply evidence of effectivness and safety of the PAS-Port System
Point estimates for the effectiveness and safety endpoints may be biased due to:
Post-hoc analyses
A lot of missing information (in some cases, the imputed patency is questionable).
Small data set