Embed Size (px)
Citation preview

1
Should I give a medication…
Pharmacological Management of Behavioral Problems
Or just take one myself?Dr. Gordon ThomasGeriatric Psychiatrist
Royal Ottawa Mental Health Centre

Psychotropic drugs Part of the overall
approach• Psychotropic:
• Any drug capable of affecting the mind, emotions, and behavior
• Examples• Antidepressants• Antipsychotics• Anxiolytics/Sedatives• Mood stabilizers• Cognitive stabilizers
2

Psychotropic drugs Part of the overall
approach
Wandering / pacing Exit-seeking Sundowning Hoarding Rummaging Resistance to care Sexual disinhibition
Inappropriate dressing/disrobing
Inappropriate voiding/defecation
Swearing Screaming/repetitive
vocalizations Spitting
3
Behaviors that Do Not respond to Medication:

Psychotropic drugs Part of the overall
approach
Anxiety Depression Mania Psychosis Sleep disruption
Aggression Frontal disinhibition
General medical illness
Infections Medication side
effects Delirium Pain
Agitation
4
Causes of behaviors that May respond to Medication:
PHARMACOKINETICSHow the body handles drugs:
5

Psychotropic drugs Use in the
Elderly• Changes in how the body handles drugs
• Absorption• Distribution• Metabolism• Elimination
6

Psychotropic drugs Use in the
Elderly• Absorption
• Slower in elderly patients• Decreased motility and gastric pH
• No clinical significance without overt disease
• Can be delayed by other medications• Antacids• Aluminum containing cathartics• Calcium/Magnesium• Fibre
7

Psychotropic drugs Use in the
Elderly• Distribution (fat / water / protein bound)
• Higher fat:muscle and fat:water ratios• Lipid soluble medications stored and take longer to clear• Most psychotropics are lipid soluble
• Lower protein (albumin) levels• Not clinically significant by itself• Multiple medications bind protein and may compete
8

Psychotropic drugs Use in the
Elderly• Metabolism
• Phase I: oxidation before entering circulation• Decreased in elderly = more active drug in system
• Phase II: conjugation/glucuronidation• Relatively unaffected• Other changes decrease this process
• Reduced liver blood flow (40-45%)• Reduced liver mass
• Some activate or deactivate the process• Decrease or increase levels of active drug
9

Psychotropic drugs Use in the
Elderly• Elimination
• Decreased renal function with age• GFR decreases yearly from age 20• Calculated CrCl needed (eGFR is inaccurate)
• Decreased response to volume changes• More likely to have abnormal electrolytes (SIADH)
10

Psychotropic drugs Use in the
Elderly• Illnesses alter handling of drugs
• Gastric surgery• Heart failure• Liver disease• Renal disease• Malnutrition
11

PHARMACODYNAMICSHow the drugs affect the body:
12

Psychotropic drugs Use in the
Elderly• Changes in how drugs affect the body
• Increased sensitivity• Changes in receptor density• Decreased responsiveness of regulatory systems• Direct sensitivities (stroke, Parkinson’s, dementia)
13

Psychotropic drugs Use in the
Elderly• Different approach to using medications
• “Start low and go slow”• Overall therapeutic dose often unchanged
• Longer time to get a clinical response• Can be toxic at “therapeutic levels”• More vulnerable to some side effects
14

ANTIDEPRESSANTSThe happy pill…
15

Psychotropic drugs
Antidepressants• Antidepressant usage
• Depression treatment/prevention• Anxiety• Sleep disruption• Agitation• Frontal symptoms / Behaviors• Pain control
16
Psychotropic drugs
Antidepressants• SSRI (Selective Serotonin Reuptake
Inhibitor)• Celexa (citalopram): few drug interactions• Cipralex (escitalopram): few drug
interactions• Zoloft (sertraline): minor interactions• Luvox (fluvoxamine): more interactions,
sedating
• Effective and well tolerated• Depression/anxiety, agitation, behaviors
• Prozac (fluoxetine): half-life too long• Paxil (paroxetine): too anticholinergic
17

Psychotropic drugs
Antidepressants• SNRI (Serotonin Noradrenaline Reuptake
Inhibitor)• Effexor (venlafaxine)• Cymbalta (duloxetine)
• Effective and well tolerated• Depression/anxiety, (behaviors)• Neuropathic pain• Nociceptive pain (new indication)
18
Psychotropic drugs
Antidepressants• NaSSA (Noradrenergic and Selective Serotinergic
Antidepressant)
• Remeron (mirtazapine)
• Effective and well tolerated• Depression/anxiety, sleep disturbance,
appetite• (behavior), (pain)
19

Psychotropic drugs
Antidepressants• NDRI (Norepinephrine-Dopamine Reuptake
Inhibitor)• Wellbutrin (bupropion)
• Effective and well tolerated• Depression• May worsen anxiety
20

Psychotropic drugs
Antidepressants• TCA (Tri-Cyclic Antidepressant)
• Nortriptyline, Desipramine• Amitriptyline, Imipramine
• Effective but poorly tolerated• Cardiac effects (hypotension, tachycardia)• Increased fall risk• Anticholinergic effects
• Dry mouth, confusion, constipation, confusion, urinary retention, confusion, blurred vision, confusion
21

Psychotropic drugs
Antidepressants• MAOI (MonoAmine Oxidase Inhibitor)
• Parnate, Nardil• Poorly tolerated due to need for diet (yuck!)
• Mannerix (Moclobemide)• No need for diet• Less effective and poorly studied in elderly
22

Psychotropic drugs
Antidepressants• Trazodone
• Not used for depression (need high doses)• Used at low doses
• Sleep initiation• Anxiety• Agitation• Frontal symptoms
23
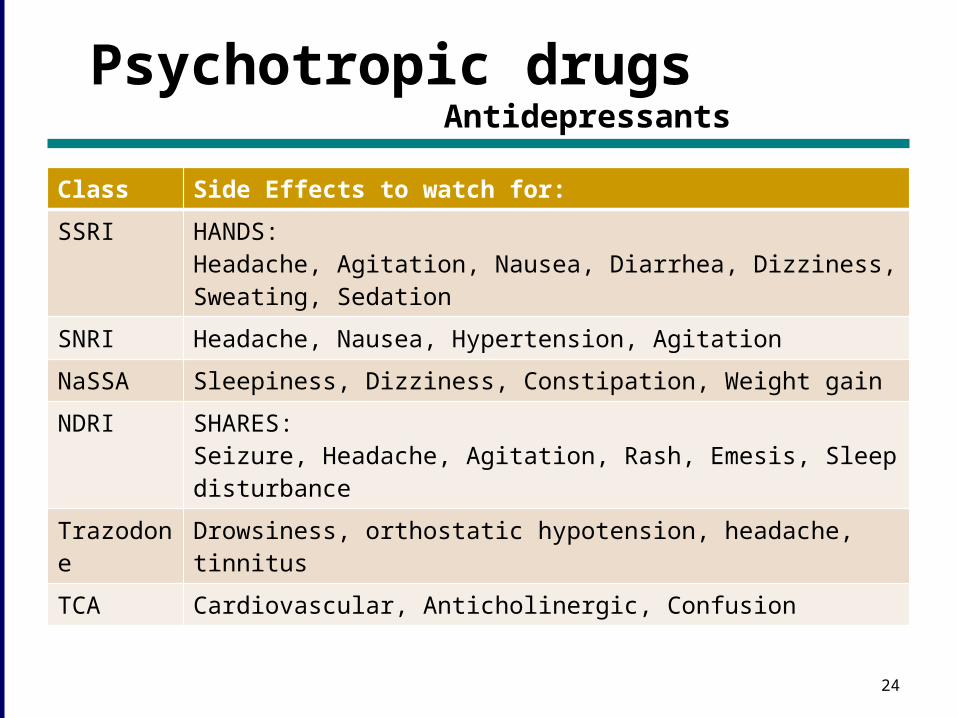
Psychotropic drugs
AntidepressantsClass Side Effects to watch for:
SSRI HANDS:Headache, Agitation, Nausea, Diarrhea, Dizziness, Sweating, Sedation
SNRI Headache, Nausea, Hypertension, Agitation
NaSSA Sleepiness, Dizziness, Constipation, Weight gain
NDRI SHARES:Seizure, Headache, Agitation, Rash, Emesis, Sleep disturbance
Trazodone
Drowsiness, orthostatic hypotension, headache, tinnitus
TCA Cardiovascular, Anticholinergic, Confusion
24

Psychotropic drugs
Antidepressants
25
Drug Typical initial doses
Typical dose range
Celexa (citalopram) 10 mg daily 20-40 mg daily
Cipralex (escitalopram) 5 mg daily 10-20 mg daily
Zoloft (sertraline) 25 mg daily 50-200 mg daily
Luvox (fluvoxamine) 25 mg qhs 50-200 mg qhs
Effexor XR (venlafaxine)
37.5 mg daily 150-300 mg daily
Cymbalta (duloxetine) 30 mg daily 60-120 mg daily
Remeron (mirtazepine) 15 mg qhs 30-45 mg qhs
Wellbutrin XL (bupropion)
150 mg daily 300-450 mg daily
Trazodone25-50 mg qhs12.5-25 mg tid12.5–25 mg q4h prn
25-200 mg qhs12.5-100 mg tid12.5-50 mg q4h prn

Psychotropic drugs
Antidepressants
26
• Common questions• When should the dose increase?• When should the drug stop?• How long does it take to work?• What if it doesn’t work?• What other options are there?• What about ECT?
Psychotropic drugs
Antidepressants
27
• Common Uses• Depression and Anxiety• Pain (Effexor & Cymbalta)• Sleep (Remeron & Trazodone)• Frontal Disinhibition• Smoking Cessation (Wellbutrin)

ANTIPSYCHOTICSThe crazy pill…
28

Psychotropic drugs
Antipsychotics• Antipsychotic usage
• Schizophrenia / Delusional disorders• Psychotic depression• Delirium• Dementia with behavioral problems
These are not first choice medications
29

Psychotropic drugs
Antipsychotics• Atypicals (newer medications)
• Risperidone (Risperdal)• Olanzapine (Zyprexa)• Seroquel (Quetiapine)• Zeldox (Ziprazidone)• Abilify (Aripiprazole)
• Fewer side effects than older medications• Still need to be used cautiously• Sedation, weight gain, risk of falls, risk of stroke• Small increase in mortality
30

Psychotropic drugs
Antipsychotics• Typicals (older drugs)
• Haldol, Perphenazine, Nozinan, Loxapine, Chlorpromazine, others…
• More side effects, higher risks• Parkinsonian symptoms
• Tremor, rigidity, bradykinesia, restlessness, falls
• Cognitive blunting• Tardive dyskinesia• Increased mortality
31
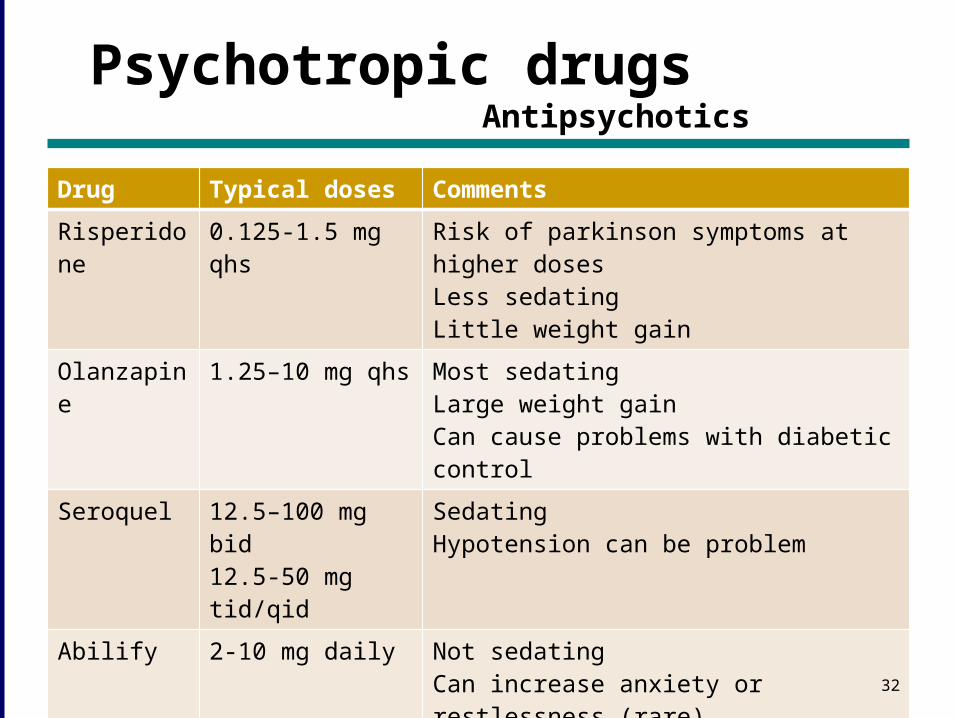
Psychotropic drugs
AntipsychoticsDrug Typical doses Comments
Risperidone
0.125-1.5 mg qhs
Risk of parkinson symptoms at higher dosesLess sedatingLittle weight gain
Olanzapine
1.25–10 mg qhs Most sedatingLarge weight gainCan cause problems with diabetic control
Seroquel 12.5–100 mg bid12.5-50 mg tid/qid
SedatingHypotension can be problem
Abilify 2-10 mg daily Not sedatingCan increase anxiety or restlessness (rare)Seems to work well for mood symptoms
Always need to use the lowest possible dose and review frequentlyMost patients need these medications only for short periods (few months)
32

Psychotropic drugs
Antipsychotics
33
• Common questions• When should the dose increase?• When should the drug stop?• How long does it take to work?• What if it doesn’t work?• What other options are there?• When should they not be used?

ANXIOLYTIC / SEDATIVE HYPNOTICS
The sleepy pill…
34

Psychotropic drugs
Anxiolytics
35
• Anxiolytics / Sedative Hypnotic use• Use is controversial in elderly patients• Sleep• Anxiety• Behavioral management• Alcohol withdrawal

Psychotropic drugs
Anxiolytics• Benzodiazepines
• Alprazolam (Xanax)• Diazepam (Valium)• Flurazepam
(Dalmane)• Clonazepam
(Rivotril)
• Non-benzodiazepines• Zopiclone (Imovane)• Zolpidem (Ambien)• Zaleplon (Starnoc)
• Lorazepam (Ativan)• Oxazepam (Serax)• Temazepam
(Restoril)
36

Psychotropic drugs
Anxiolytics• Side effects
• Drowsiness / fatigue• Memory impairment / confusion
• Chronic use can meet criteria for dementia
• Weakness• Incoordination / ataxia• Depression• Disinhibition / behavior problems• Paradoxial reactions• Decreased sleep quality and worsened apnea• Tolerance and withdrawal symptoms
• Elderly (especially with dementia) are more sensitive
37

MOOD STABILIZERSThe steady pill…
38

Psychotropic drugs Mood
Stabilizers
• Mood stabilizer use• Bipolar disorder (mania & depression)• Augmentation of antidepressants
39

Psychotropic drugs Mood
Stabilizers
• Lithium• Effective for mania and depression• Effective in lower doses for
augmentation• Water soluble and cleared by kidneys• Serum levels must be monitored
• 0.4 – 0.7 mmol/L (not 0.8 – 1.5 mmol/L)• Lower levels for augmentation (0.3 - 0.6 mmol/L)
40

Psychotropic drugs Mood
Stabilizers
• Lithium side effects• nausea, anorexia, diarrhoea,vomiting• weight gain, sedation• subjective memory loss and slowing• tremor, parkinsonism, ataxia
• High serum levels are toxic• Increased side effects, delirium• Hold and check level if losing fluid
41

Psychotropic drugs Mood
Stabilizers
• Anticonvulsants• Valproic acid (Epival)
• GI upset, somnolence, alopecia, tremor, weakness, increased liver enzymes, gait instability
• Lamotragine (Lamictal)• Gabapentin (Neurontin)• Carbamazepine (Tegretol)
• some evidence of cognitive impairment caused by these drugs
42

COGNITIVE STABILIZERSThe memory pill…
43

Psychotropic drugs Cognitive
Stabilizers
• Cognitive Stabilizer use• Stabilizers not Enhancers
• Preservation of Abilities• Management of Behaviors• Stabilization of Cognitive function• Decrease caregiver time• Delay Entry into LTC setting
44

Psychotropic drugs Cognitive
Stabilizers
• Cholinergic agents• Aricept (donepezil)• Reminyl (galantamine)• Exelon (rivastigmine)
• Effective for Mild to Severe dementias• Stabilize cognition for 1-2 years
• Still some benefits even when decline resumes
45

Psychotropic drugs Cognitive
Stabilizers
• Cholinergic agents• Side Effects (MIND)
• Muscle cramps• Insomnia / nightmares• Nausea ***• Diarrhea
• Caution with:• COPD, heart block, seizures, ulcers
46

Psychotropic drugs Cognitive
Stabilizers
• Glutaminergic agents• Ebixa (memantine)
• Effective for Moderate to Severe dementias
• Stabilize cognition for 1-2 years• Small number have some improvement• Small number get more confused
• Not covered by ODB ($120 per month)
47

Psychotropic drugs Cognitive
Stabilizers
• Glutaminergic agents• Side Effects (CHECK)
• Confusion• Headache• Equilibrium (dizziness)• Constipation• Kidney function
• Dosage depends on CrCl (eGFR is not adequate)
48

Psychotropic drugs Cognitive
Stabilizers
• Who might benefit?• Alzheimer’s dementia• Vascular dementia • Mixed Dementia• Lewy-Body Dementia• Other neuropsychiatric disorders
• i.e. Parkinsons-related Dementia
Fronto-temporal dementia can get worse
49

Psychotropic drugs Cognitive
StabilizersDrug Starting dose Treatment dose
Aricept (donepezil) 5 mg qam 5 or 10 mg qam
Reminyl ER (galantamine)
8 mg qam 16-24 mg qam
Exelon (rivastigmine) 1.5 mg bid 3-6 mg bid
Exelon patch Patch 5 daily Patch 10 daily
Ebixa (memantine) 5 mg qam 5 or 10 mg bid
50

Psychotropic drugs Cognitive
Stabilizers
• Common Questions• Which medication?• When and how to switch medications?• How to monitor?• Are combinations useful?• When should they be stopped?
51