Embed Size (px)
Citation preview

1
SERM’sIES Winter Conference 24.11.05
Iris Vered,
Sheba Medical Center
Tel Hashomer
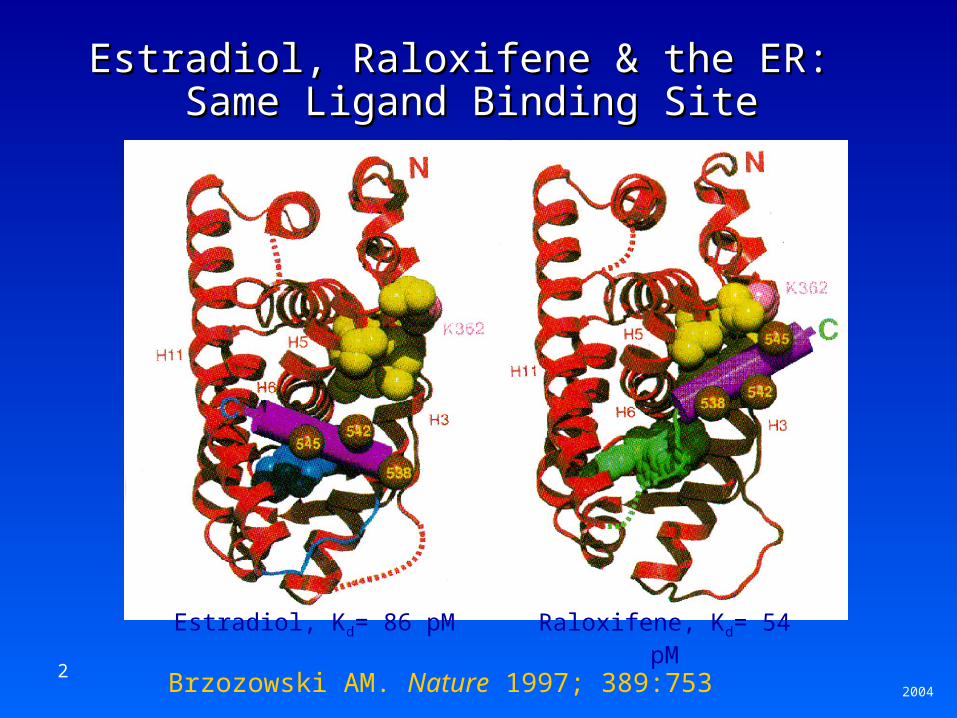
2 Brzozowski AM. Nature 1997; 389:753
Estradiol, Raloxifene & the ER: Estradiol, Raloxifene & the ER: Same Ligand Binding SiteSame Ligand Binding Site
2004
Estradiol, Kd= 86 pM Raloxifene, Kd= 54 pM
3
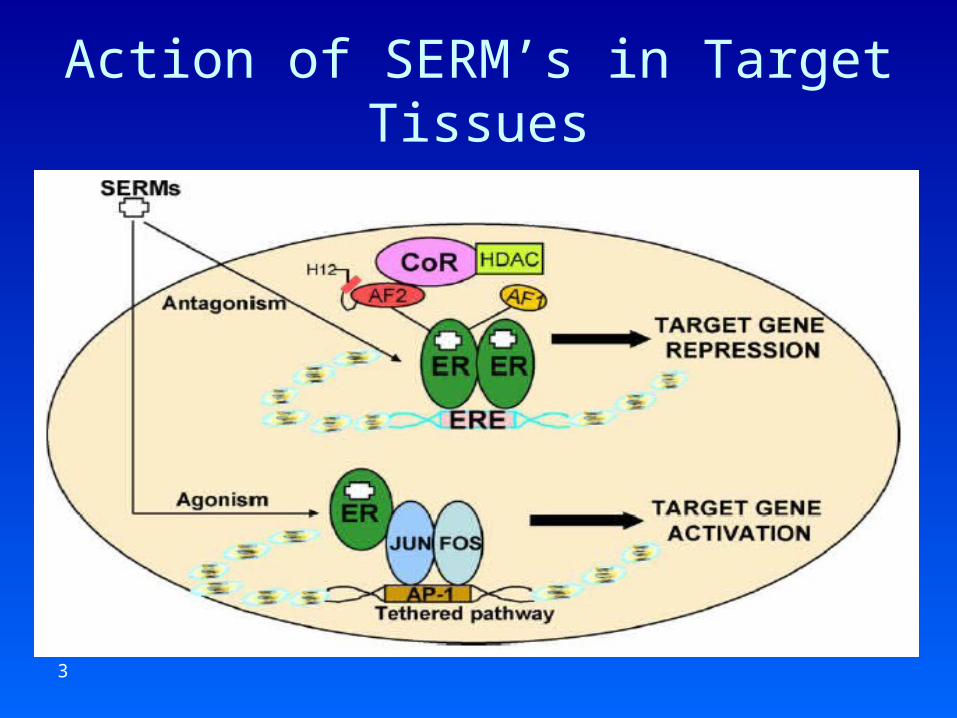
Action of SERM’s in Target Tissues
ER
4
SERM’s Developed for Osteporosis
• Raloxifene, Evista®, Eli Lilly. – FDA approved 01 Oct. 1999
• Idoxifene, BMS (failed phase III)• Lasofoxifene, Oporia®, Pfizer• Arzoxifene, Eli Lilly• Bazedoxifene, Wyeth
5
Multiple Outcomes of Raloxifene Evaluation (MORE) Trial Summary
• Randomized, double-blind, placebo-controlled osteoporosis treatment trial in postmenopausal women with osteoporosis (N=7705)
• 4 years of treatment• 3 treatment arms:
– Placebo (n=2576)– Raloxifene 60 mg/d (n=2557)– Raloxifene 120 mg/d (n=2572)
• 1ary endpoints: vertebral fracture, BMD, safety• 2ary endpoints: all osteoporotic fractures, cardiovascular
health, breast cancer, cognitive function
6
MORE Trial Results, 4 YearsPostmenopausal women with osteoporosistreated with raloxifene had:• A modest increase in lumbar spine & femoral
neck BMD• A decreased risk of new vertebral fractures • No reduction in risk for all non-vertebral
fractures• A decreased risk of new non-vertebral fractures
at 6 major sites*: clavicle, humerus, wrist, pelvis, hip, leg in women with prevalent vertebral fractures
• A lower incidence of breast cancer
7
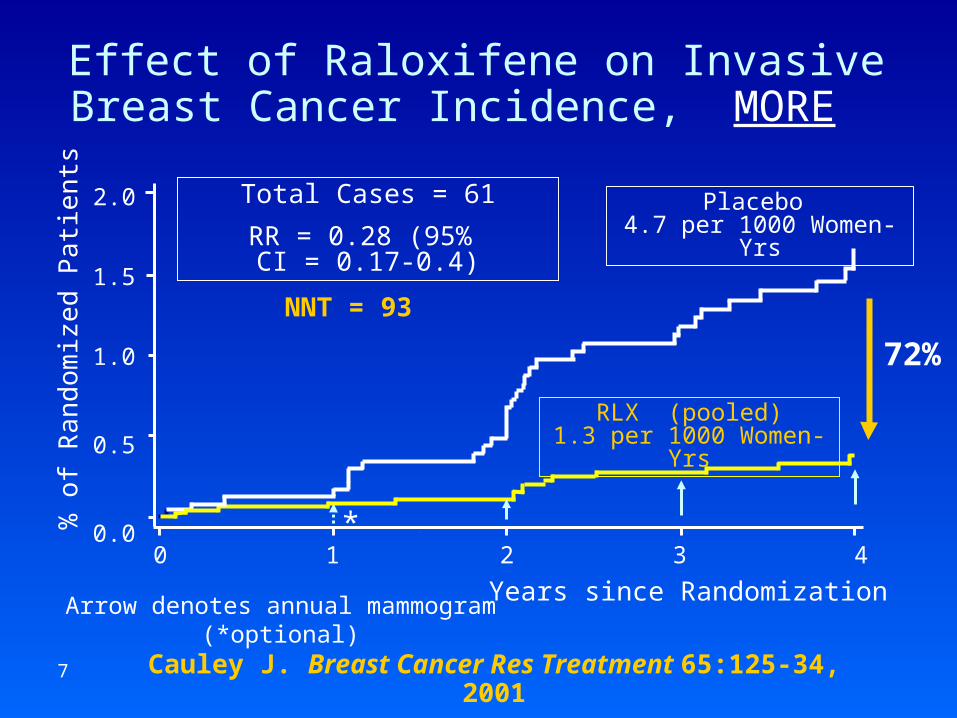
Effect of Raloxifene on Invasive Breast Cancer Incidence, MORE
Arrow denotes annual mammogram (*optional)
Cauley J. Breast Cancer Res Treatment 65:125-34, 2001
2.0
1.5
1.0
0.5
0.00 1 2 3 4
Years since Randomization
% o
f Ran
dom
ize
d P
atie
nts
72%
Total Cases = 61
RR = 0.28 (95% CI = 0.17-0.4)
RLX (pooled)1.3 per 1000 Women-Yrs
Placebo 4.7 per 1000 Women-Yrs
*
NNT = 93
8
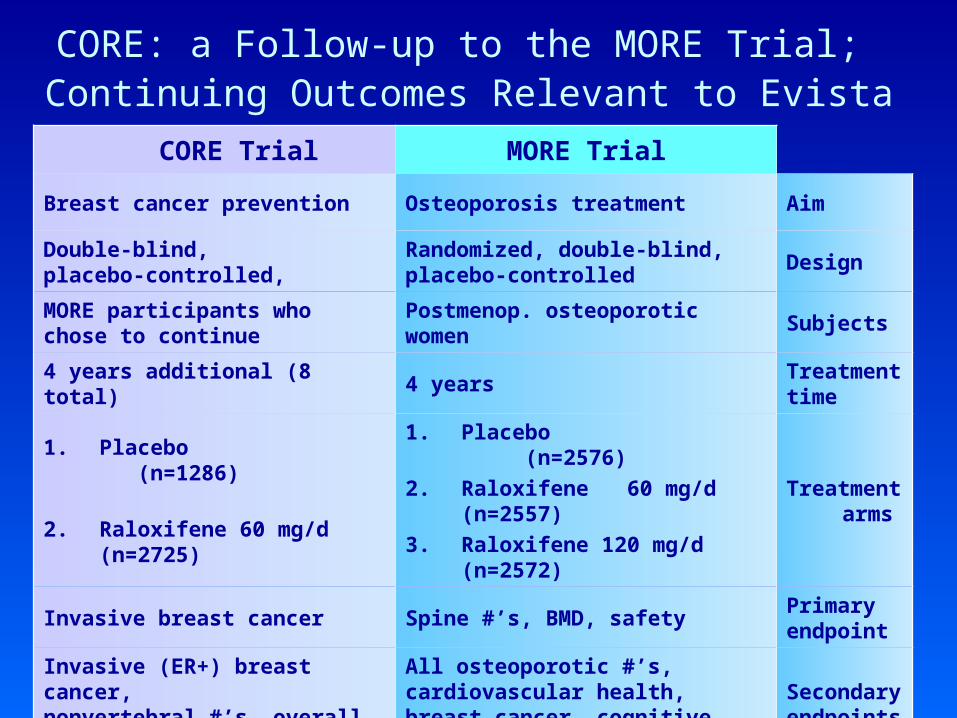
CORE: a Follow-up to the MORE Trial; Continuing Outcomes Relevant to Evista
MORE TrialCORE Trial
Aim Osteoporosis treatment Breast cancer prevention
Design Randomized, double-blind, placebo-controlled
Double-blind, placebo-controlled,
Subjects Postmenop. osteoporotic womenMORE participants who chose to continue
Treatment time
4 years4 years additional (8 total)
Treatment arms
1. Placebo (n=2576)
2. Raloxifene 60 mg/d (n=2557)
3. Raloxifene 120 mg/d (n=2572)
1. Placebo (n=1286)
2. Raloxifene 60 mg/d (n=2725)
Primary endpoint
Spine #’s, BMD, safetyInvasive breast cancer
Secondary endpoints
All osteoporotic #’s, cardiovascular health, breast cancer, cognitive function
Invasive (ER+) breast cancer, nonvertebral #’s, overall safety
9
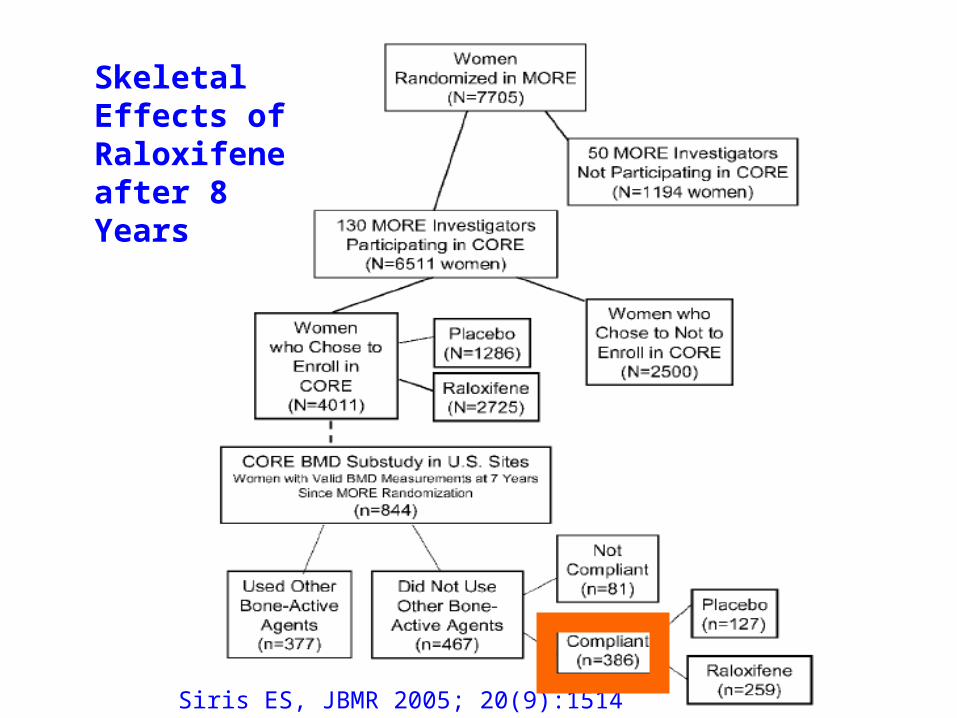
Skeletal Effects of Raloxifene after 8 Years: Strength & Limitations
• Strength: Placebo controlled for 8 years• Limitations:
– Differences between the women who did & did not enroll in CORE
– Disparities between the placebo & raloxifene groups in CORE
– A greater use of bone-active drugs in the placebo group after year 3
– 20% elected not to take the study drug
Siris ES, JBMR 2005, 20(9):1514
10
Siris ES, JBMR 2005; 20(9):1514
Skeletal Effects of Raloxifene after 8 Years
11
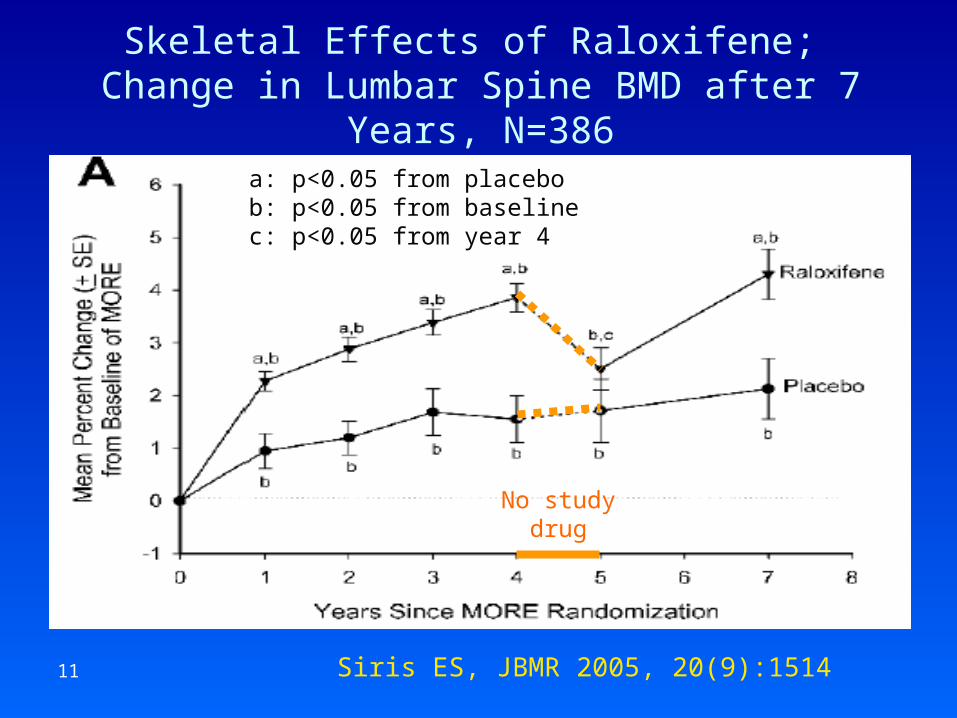
Skeletal Effects of Raloxifene; Change in Lumbar Spine BMD after 7 Years, N=386
Siris ES, JBMR 2005, 20(9):1514
a: p<0.05 from placebob: p<0.05 from baselinec: p<0.05 from year 4
No studydrug
12
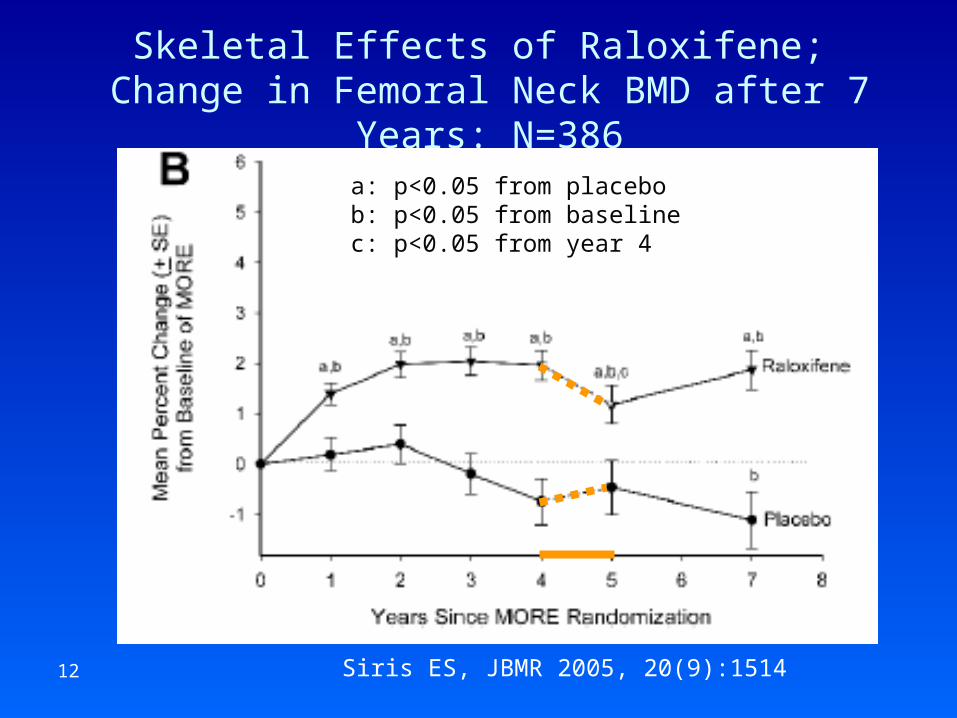
Skeletal Effects of Raloxifene; Change in Femoral Neck BMD after 7 Years: N=386
Siris ES, JBMR 2005, 20(9):1514
a: p<0.05 from placebob: p<0.05 from baselinec: p<0.05 from year 4
13
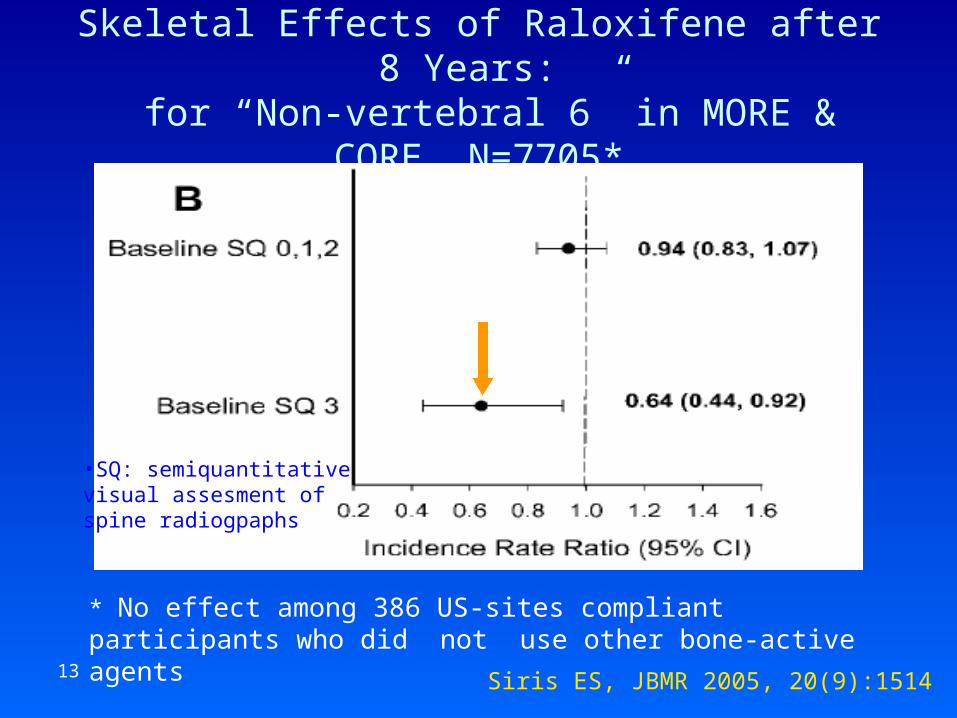
Skeletal Effects of Raloxifene after 8 Years: for “Non-vertebral 6” in MORE & CORE, N=7705*
Siris ES, JBMR 2005, 20(9):1514
•SQ: semiquantitative visual assesment of spine radiogpaphs
* No effect among 386 US-sites compliant participants who did not use other bone-active agents
14
EVA (Evista® Vs. Alendronate comparison trial)
• Head-to-head, double-blind, randomized trial for fracture risk reduction efficacy
• Original protocol: – 3000 postmenopausal women– age 50-80y– FN BMD T-score: -4.0 to -2.5– no prevalent spine fractures– no prior use of bone-active agents– duration: 5 y
• Early discontinuation due to slow enrollment, insufficient power to detect non-inferiority
Recker R, ASBMR 2005; s97
15
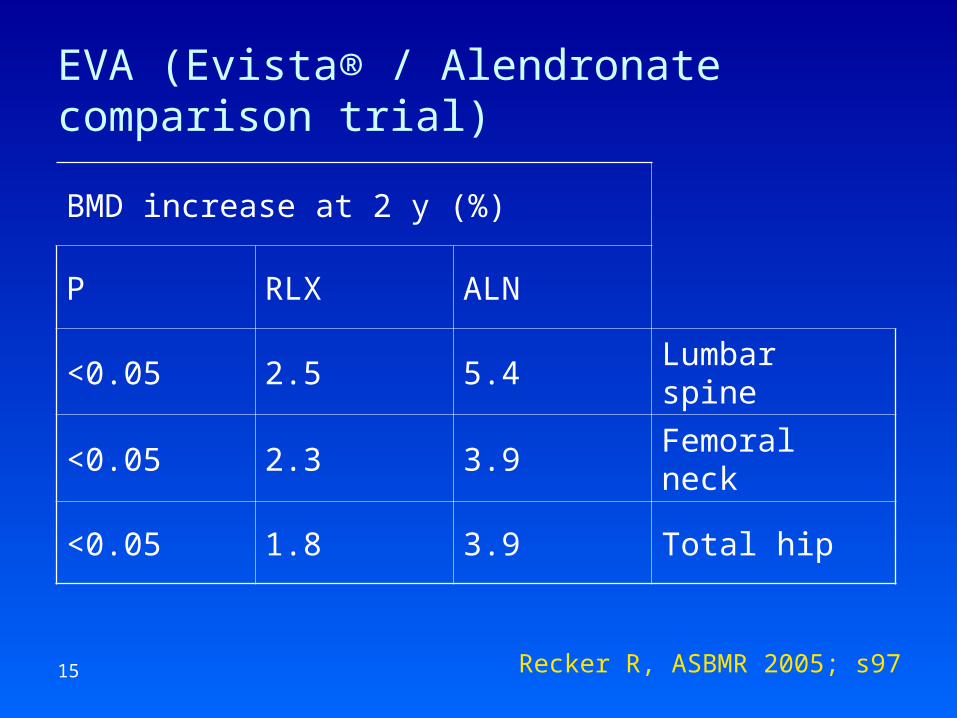
EVA (Evista® / Alendronate comparison trial)
Recker R, ASBMR 2005; s97
BMD increase at 2 y (%)
ALNRLXP
Lumbar spine5.42.5<0.05
Femoral neck3.92.3<0.05
Total hip3.91.8<0.05
16
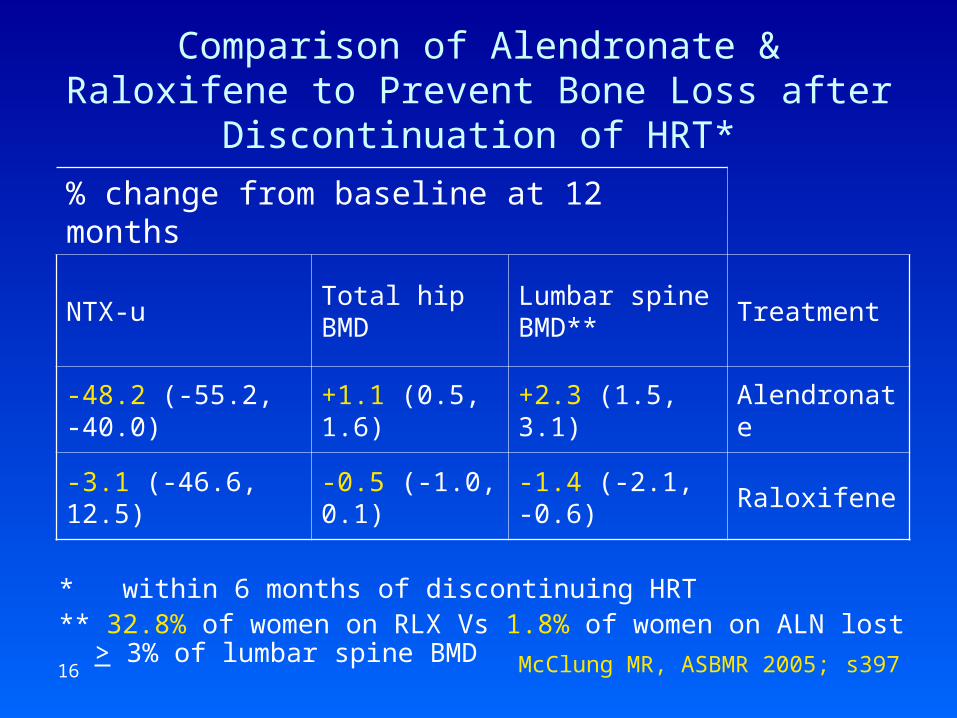
Comparison of Alendronate & Raloxifene to Prevent Bone Loss after Discontinuation of HRT*
* within 6 months of discontinuing HRT** 32.8% of women on RLX Vs 1.8% of women on ALN lost > 3% of
lumbar spine BMD
% change from baseline at 12 months
Treatment Lumbar spine BMD**
Total hip BMD
NTX-u
Alendronate +2.3 (1.5, 3.1)+1.1 (0.5, 1.6)-48.2 (-55.2, -40.0)
Raloxifene -1.4 (-2.1, -0.6)-0.5 (-1.0, 0.1)-3.1 (-46.6, 12.5)
McClung MR, ASBMR 2005; s397
17
Breast Cancer Objectives: CORE Trial
Primary endpoint• Determine the effect of raloxifene on incidence of
invasive breast cancer over a long-term period in postmenopausal women with osteoporosis 1
Secondary analyses• Incidence of invasive ER (+) breast cancer over 8 years 1
• Incidence of invasive breast cancer in postmenopausal women stratified by their 5-year predicted risk of developing breast cancer using the Gail model during the 4 years of the CORE trial 2
1. Martino S. J Nat Cancer Inst 2004, 96(23):17512. Cauley J, et al. Abst #1018, ASCO June 2004.
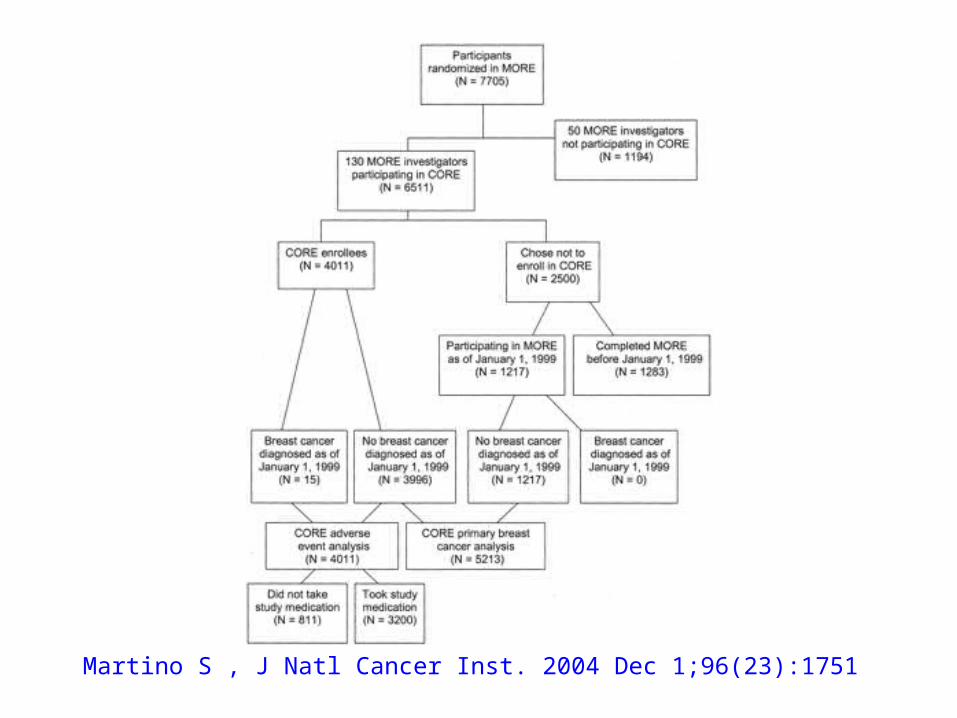
18 Martino S , J Natl Cancer Inst. 2004 Dec 1;96(23):1751
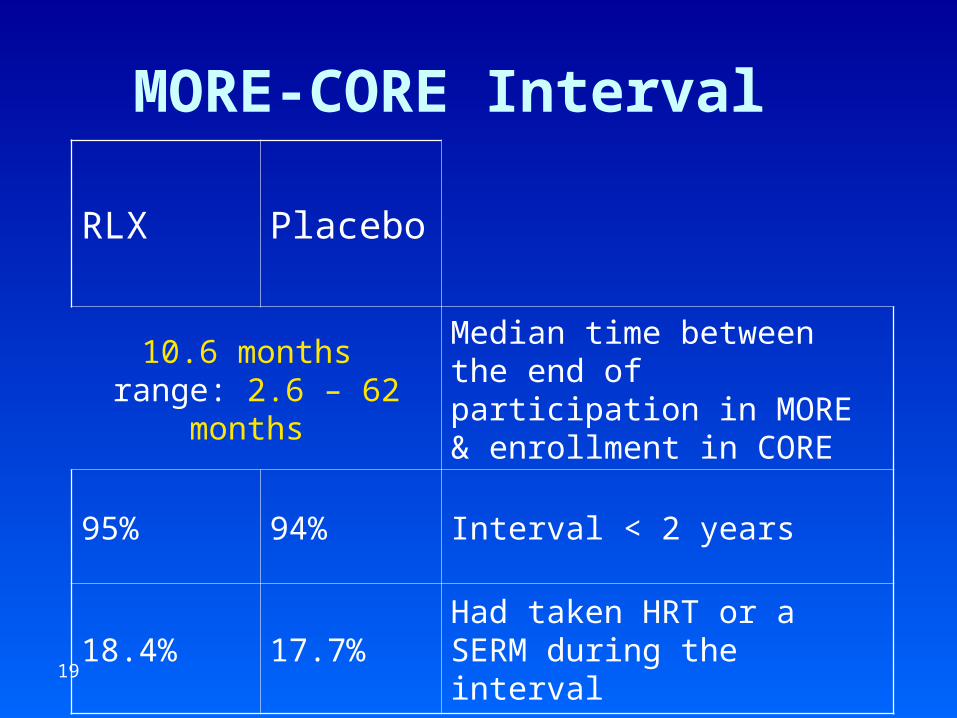
19
MORE-CORE Interval
Placebo RLX
Median time between the end of participation in MORE & enrollment in CORE
10.6 months range: 2.6 – 62 months
Interval < 2 years94%95%
Had taken HRT or a SERM during the interval
17.7%18.4%
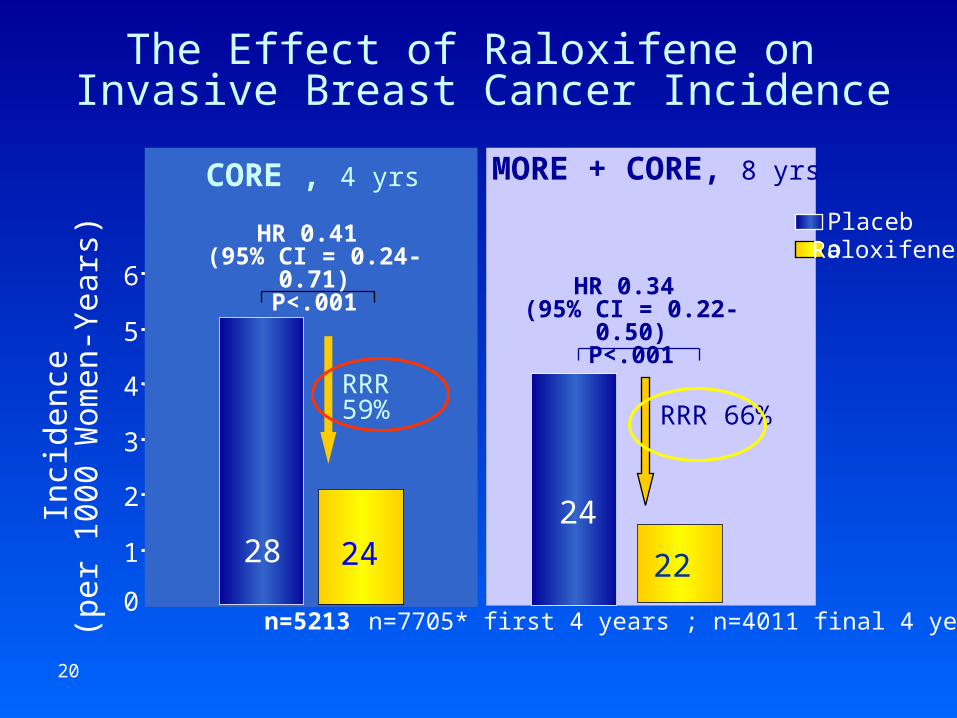
20
MORE + CORE, 8 yrs
HR 0.34 (95% CI = 0.22-0.50)
P<.001
n=7705* first 4 years ; n=4011 final 4 years
22
RaloxifenePlacebo
The Effect of Raloxifene on Invasive Breast Cancer Incidence
RRR 66%
n=5213
1
2
3
4
5
6
Inci
denc
e (
per
1000
Wom
en-Y
ears
)
0
28 24
CORE , 4 yrs
HR 0.41 (95% CI = 0.24-0.71)
P<.001
RRR 59%
24
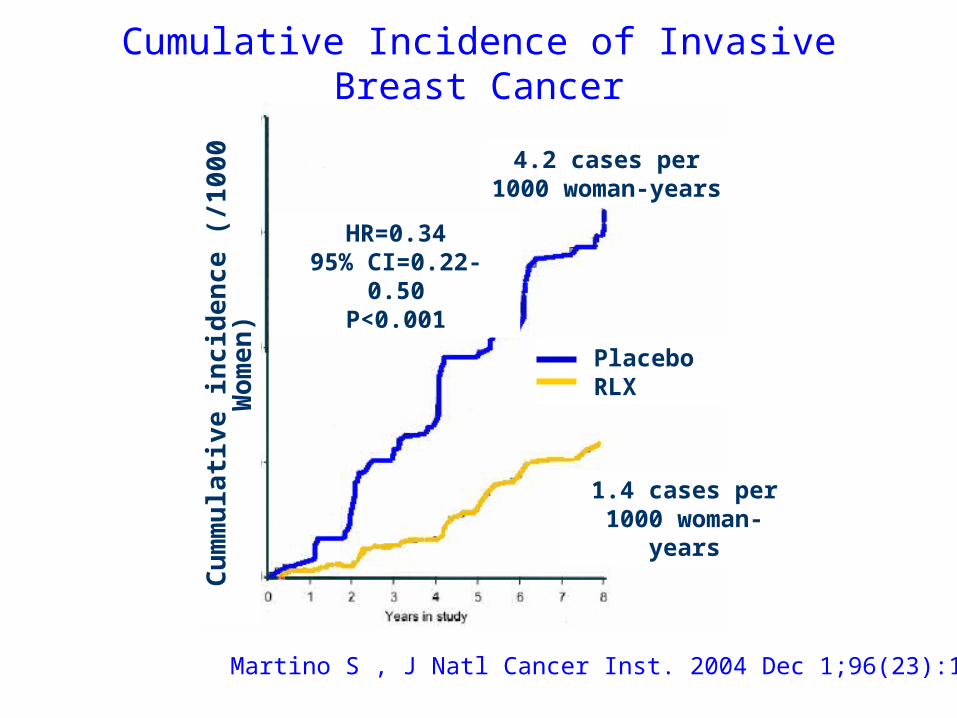
21
Cumulative Incidence of Invasive Breast Cancer
Cu
mm
ula
tiv
e in
cid
en
ce (
/10
00
Wo
me
n)
4.2 cases per1000 woman-years
1.4 cases per1000 woman-years
HR=0.3495% CI=0.22-0.50
P<0.001
PlaceboRLX
Martino S , J Natl Cancer Inst. 2004 Dec 1;96(23):1751
22
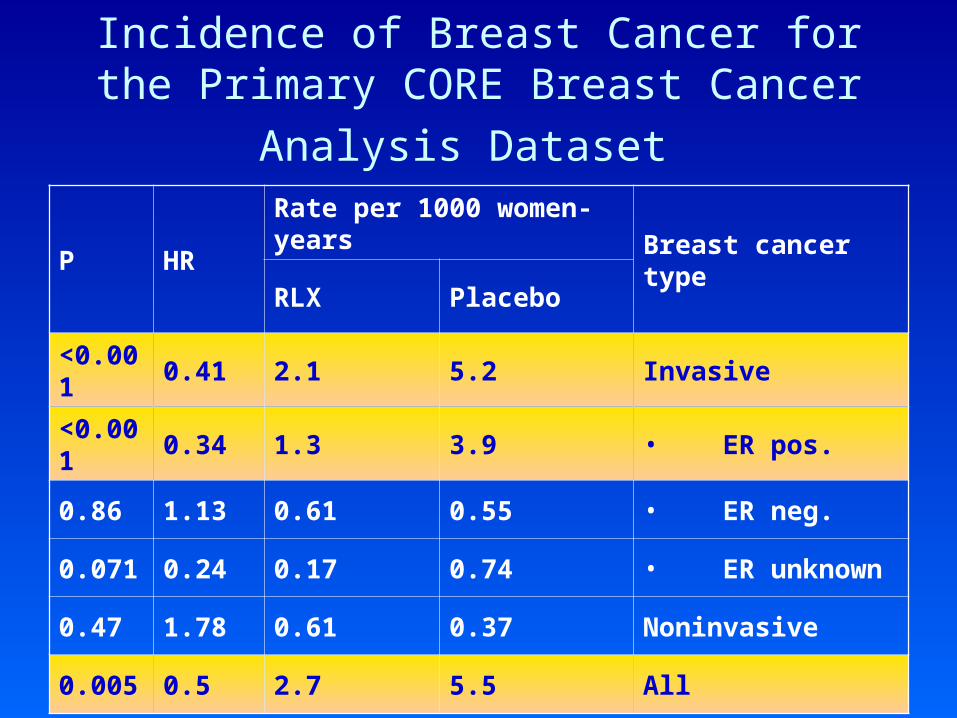
Incidence of Breast Cancer for the Primary
CORE Breast Cancer Analysis Dataset
Breast cancer type
Rate per 1000 women-yearsHRP
Placebo RLX
Invasive 5.22.10.41<0.001
• ER pos.3.91.30.34<0.001
• ER neg.0.550.611.130.86
• ER unknown0.740.170.240.071
Noninvasive 0.370.611.780.47
All 5.52.70.50.005
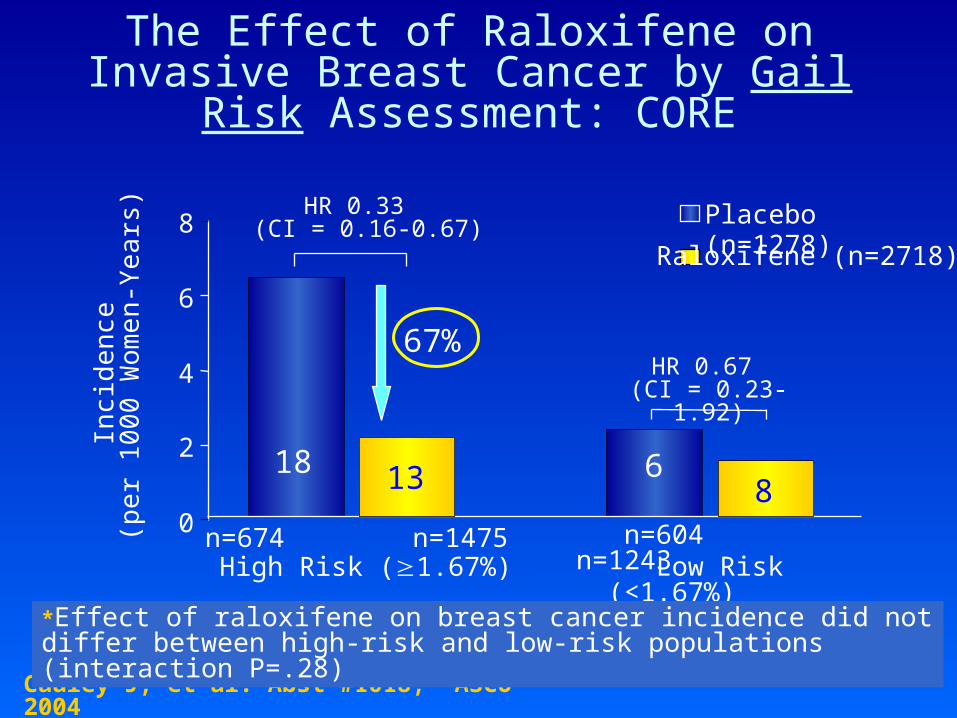
The Effect of Raloxifene on Invasive Breast Cancer by Gail Risk Assessment: CORE
0
2
4
6
8
Inci
den
ce (
per
10
00 W
ome
n-Y
ea
rs)
Low Risk (<1.67%)
HR 0.67 (CI = 0.23-1.92)
n=604 n=1243
HR 0.33 (CI = 0.16-0.67)
n=674 n=1475High Risk (1.67%)
Raloxifene (n=2718)*
Placebo (n=1278)
Cauley J, et al. Abst #1018, ASCO 2004
*Effect of raloxifene on breast cancer incidence did not differ between high-risk and low-risk populations (interaction P=.28)
18 13 68
67%
24
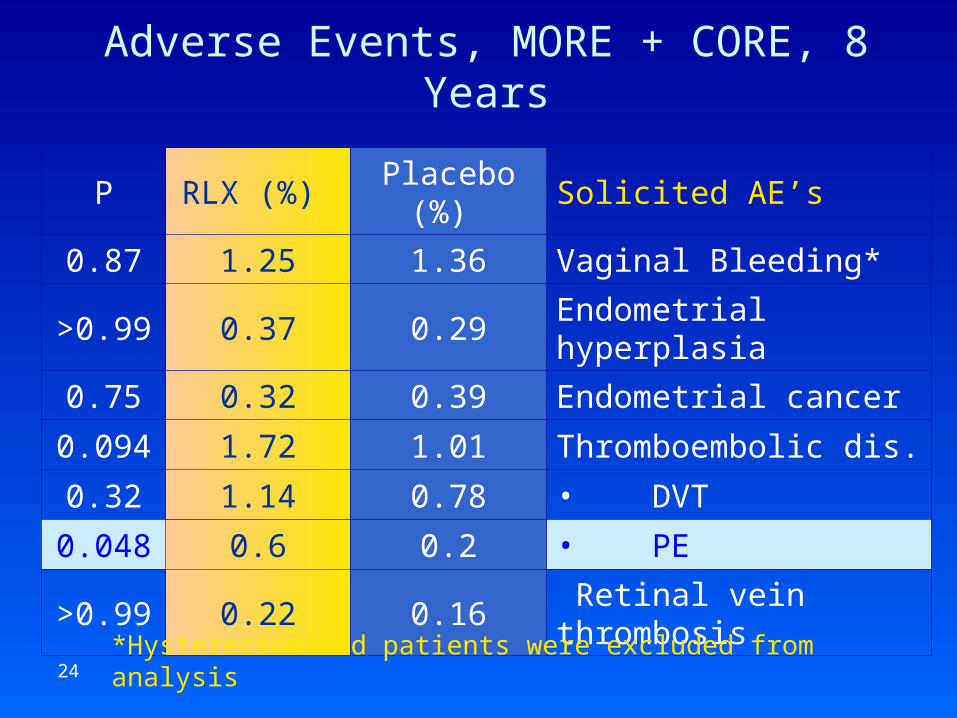
Adverse Events, MORE + CORE, 8 Years
Solicited AE’sPlacebo (%) RLX (%) P
Vaginal Bleeding*1.361.250.87
Endometrial hyperplasia0.290.37>0.99
Endometrial cancer0.390.320.75
Thromboembolic dis.1.011.720.094
• DVT0.781.140.32
• PE0.20.60.048
Retinal vein thrombosis0.160.22>0.99
*Hysterectomized patients were excluded from analysis
25
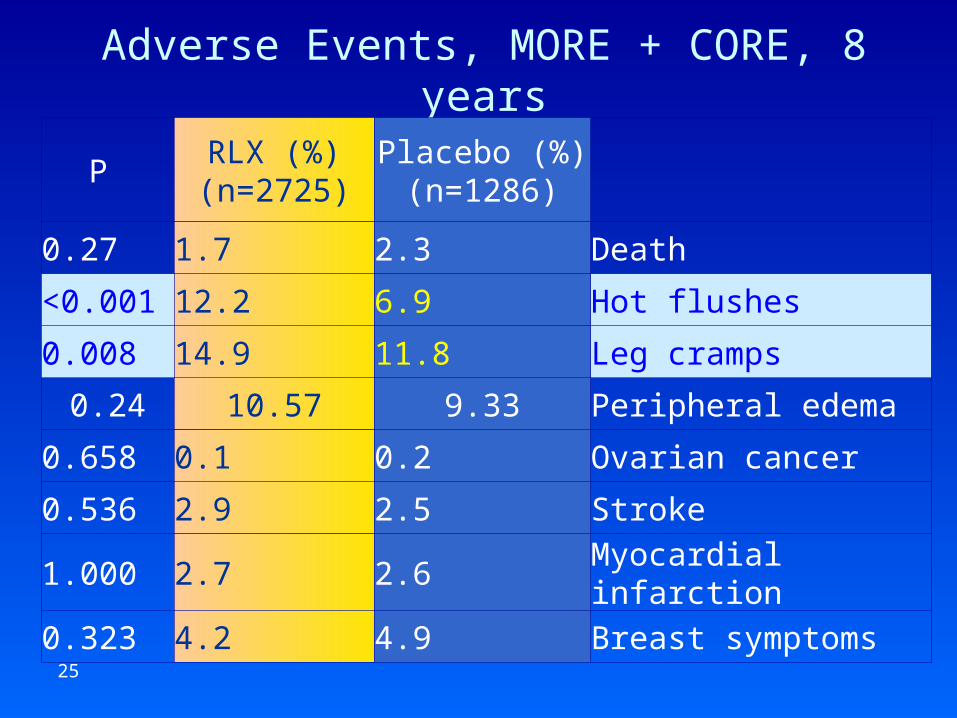
Adverse Events, MORE + CORE, 8 years
Placebo (%) (n=1286)
RLX (%) (n=2725)
P
Death2.31.70.27
Hot flushes6.912.2<0.001
Leg cramps11.814.90.008
Peripheral edema9.3310.570.24
Ovarian cancer0.20.10.658
Stroke2.52.90.536
Myocardial infarction2.62.71.000
Breast symptoms4.94.20.323
26
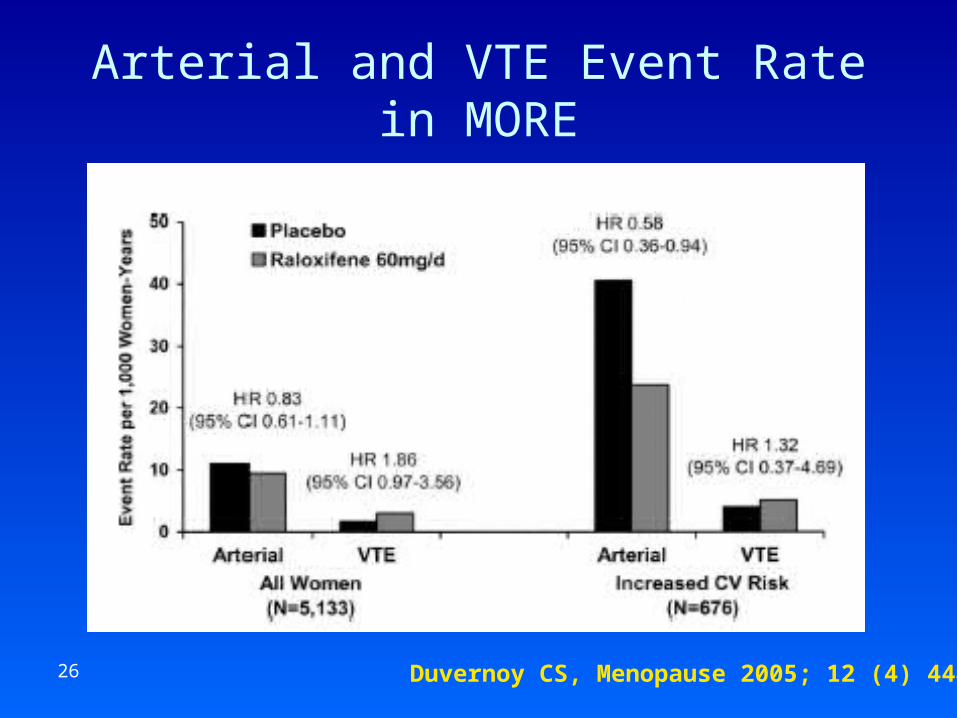
Arterial and VTE Event Rate in MORE
Duvernoy CS, Menopause 2005; 12 (4) 444
27
Effect of Raloxifene on Prevention of Dementia and Cognitive Impairment: MORE
• After 3 years, those who had clinical symptoms of dementia or scored in the lowest 10th percentile on cognitive screening were evaluated by a blinded dementia specialist and had brain scans and laboratory tests to evaluate dementia etiology– 5,153 / 5,386 (95.7%) cognitively normal– 181 (3.4%) mild cognitive impairment– 52 (1.0%) dementia, 36 Alzheimer's disease
Yaffe K. Am J Psychiatry. 2005;162(4):683
28
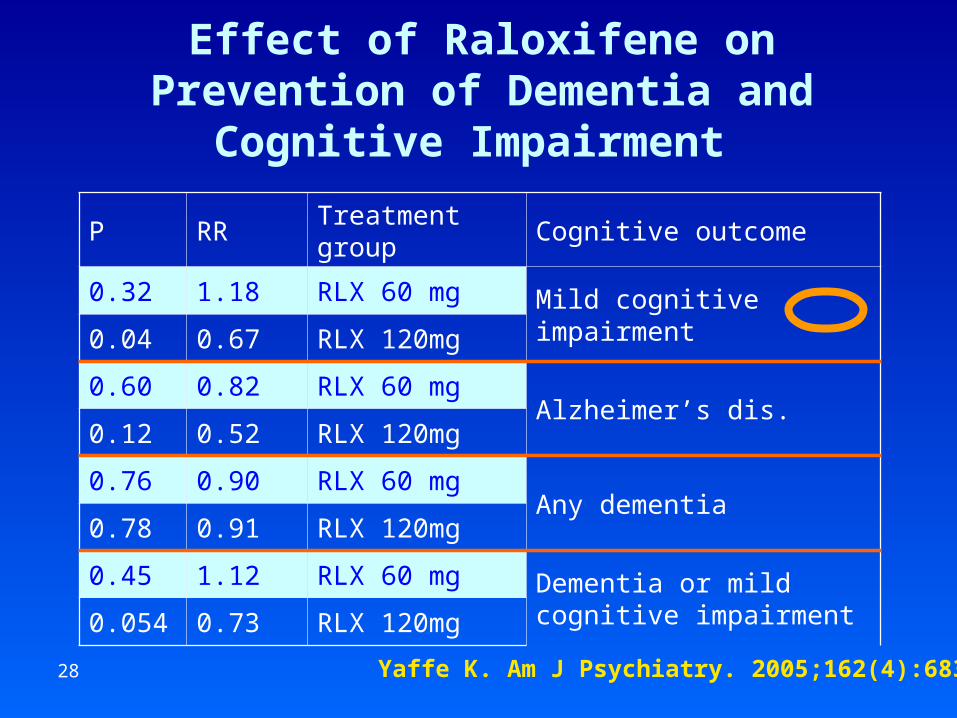
Effect of Raloxifene on Prevention of Dementia and Cognitive Impairment
Yaffe K. Am J Psychiatry. 2005;162(4):683
Cognitive outcome Treatment group RRP
Mild cognitive impairment RLX 60 mg1.180.32
RLX 120mg0.670.04
Alzheimer’s dis.RLX 60 mg0.820.60
RLX 120mg0.520.12
Any dementia RLX 60 mg0.900.76
RLX 120mg0.910.78
Dementia or mild cognitive impairment
RLX 60 mg1.120.45
RLX 120mg0.730.054
29
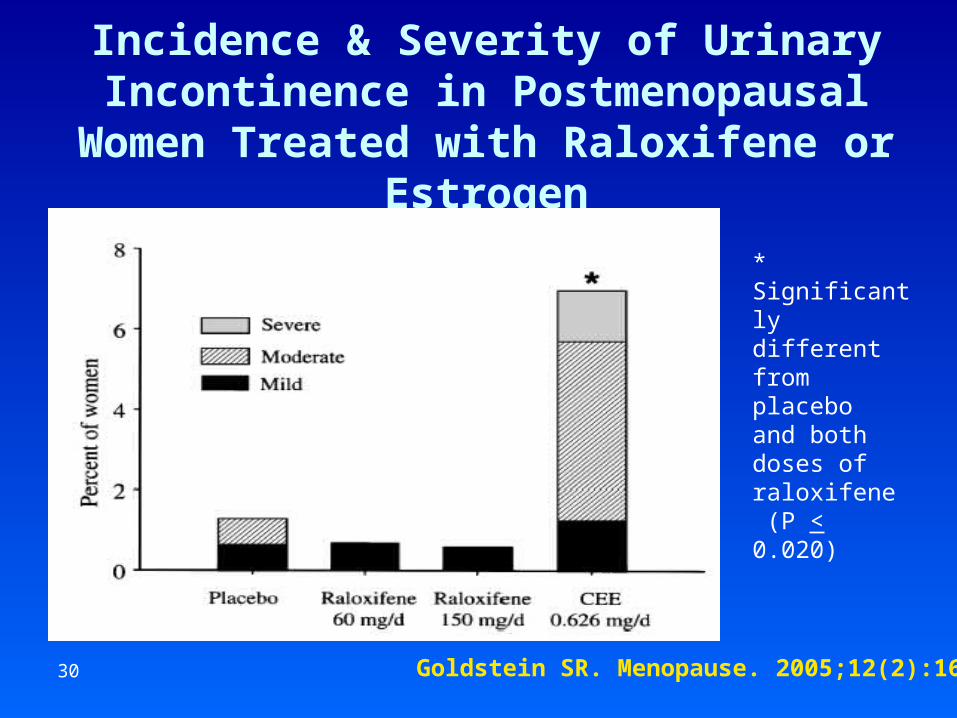
Urinary Incontinence in Postmenopausal
Women Treated with Raloxifene or Estrogen
• Based on adverse event data, in an osteoporosis prevention trial
• 619 hysterectomized women, age 40-60 y• Randomized to placebo, raloxifene 60 or 150
mg/d, or CEE 0.625 mg/d• Followed for up to 3 years
• Urinary incontinence was self-reported and rated by participants
Goldstein SR. Menopause. 2005;12(2):160
30
Incidence & Severity of Urinary Incontinence in Postmenopausal Women
Treated with Raloxifene or Estrogen
Goldstein SR. Menopause. 2005;12(2):160
* Significantly different from placebo and both doses of raloxifene (P < 0.020)
31
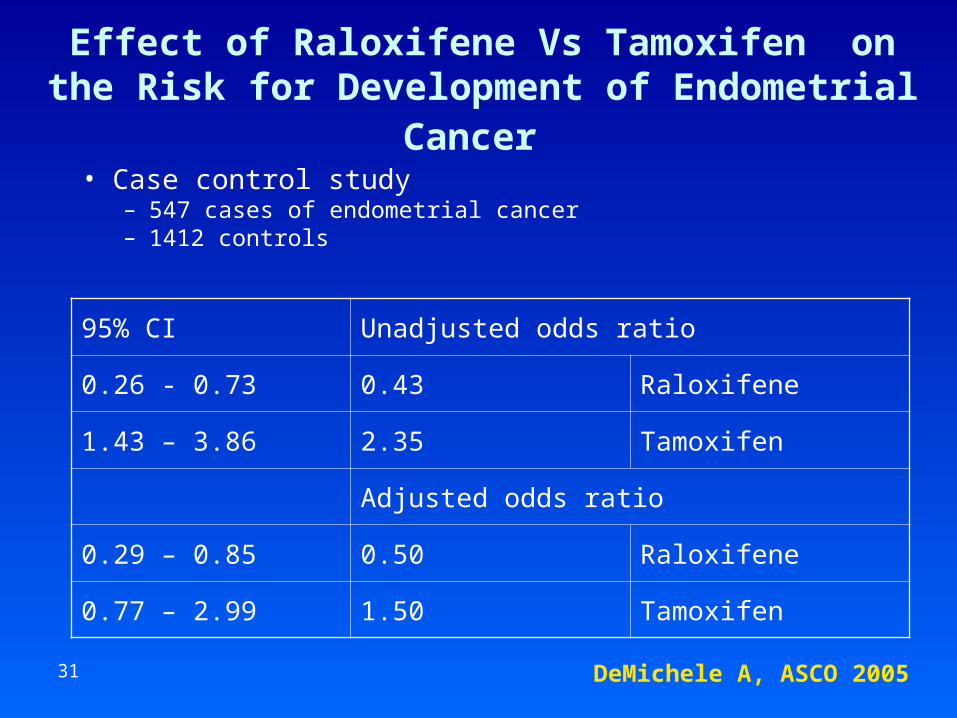
Effect of Raloxifene Vs Tamoxifen on the Risk for Development of Endometrial Cancer
• Case control study– 547 cases of endometrial cancer– 1412 controls
DeMichele A, ASCO 2005
Unadjusted odds ratio95% CI
Raloxifene 0.430.26 - 0.73
Tamoxifen 2.351.43 – 3.86
Adjusted odds ratio
Raloxifene 0.500.29 – 0.85
Tamoxifen 1.500.77 – 2.99
32
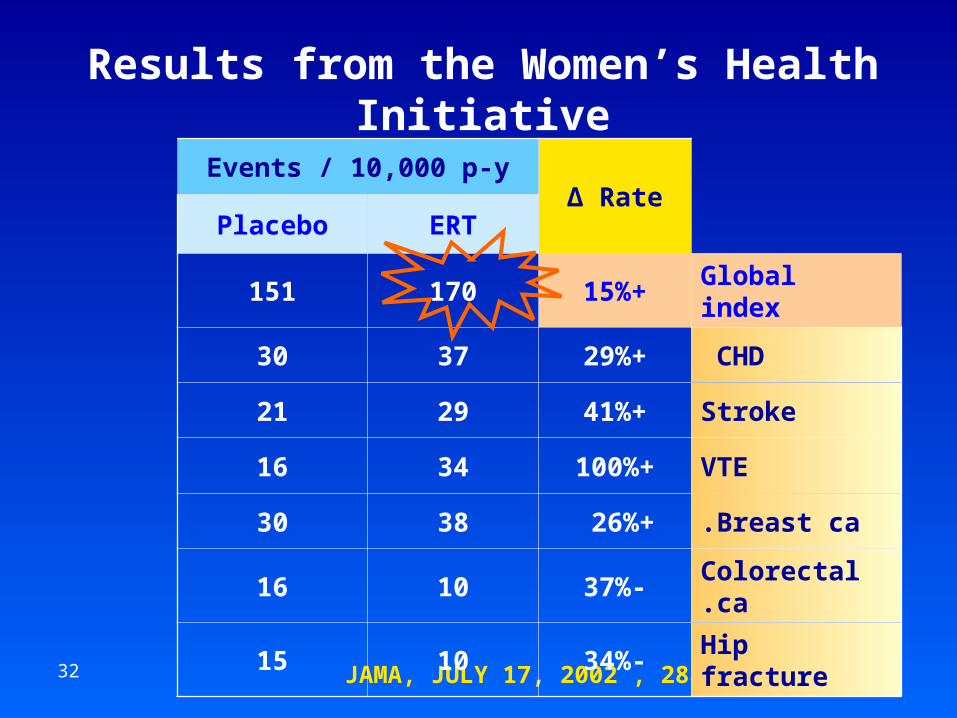
Results from the Women’s Health Initiative
JAMA, JULY 17, 2002 , 288:321
Δ RateEvents / 10,000 p-y
ERTPlacebo
Global index+15%170151
CHD +29%3730
Stroke+41%2921
VTE+100%3416
Breast ca.+26% 3830
Colorectal ca.-37%1016
Hip fracture-34%1015
33
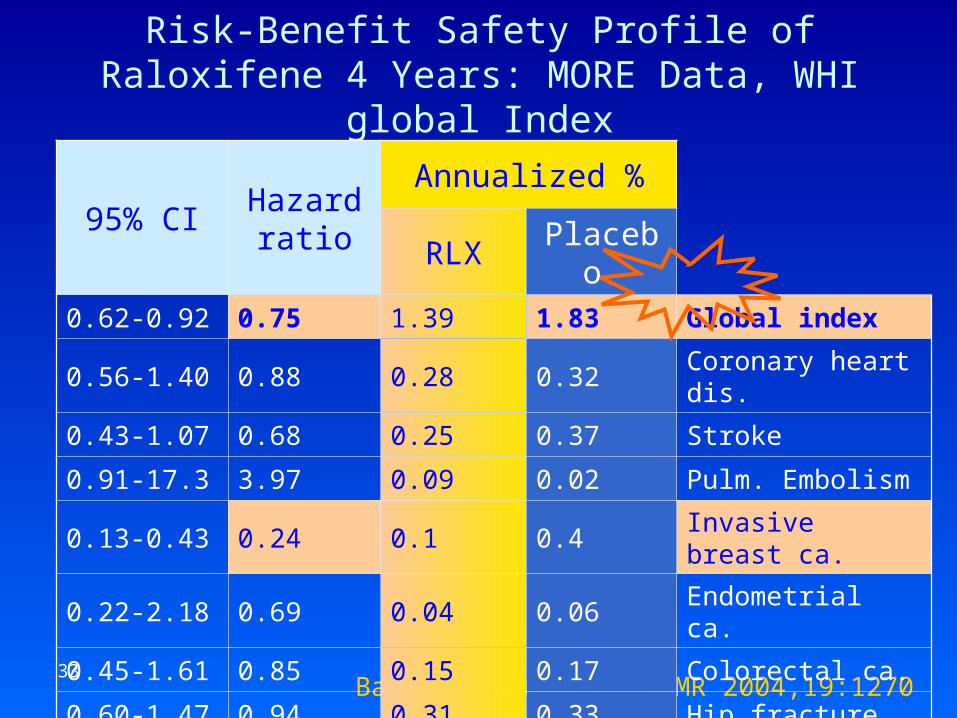
Risk-Benefit Safety Profile of Raloxifene 4 Years: MORE Data, WHI global Index
Barrett-Connor E. JBMR 2004,19:1270
Annualized %Hazard
ratio95% CI
Placebo RLX
Global index1.831.390.750.62-0.92
Coronary heart dis.0.320.280.880.56-1.40
Stroke 0.370.250.680.43-1.07
Pulm. Embolism0.020.093.970.91-17.3
Invasive breast ca.0.40.10.240.13-0.43
Endometrial ca.0.060.040.690.22-2.18
Colorectal ca.0.170.150.850.45-1.61
Hip fracture0.330.310.940.60-1.47
Total mortality0.410.350.850.56-1.28
34
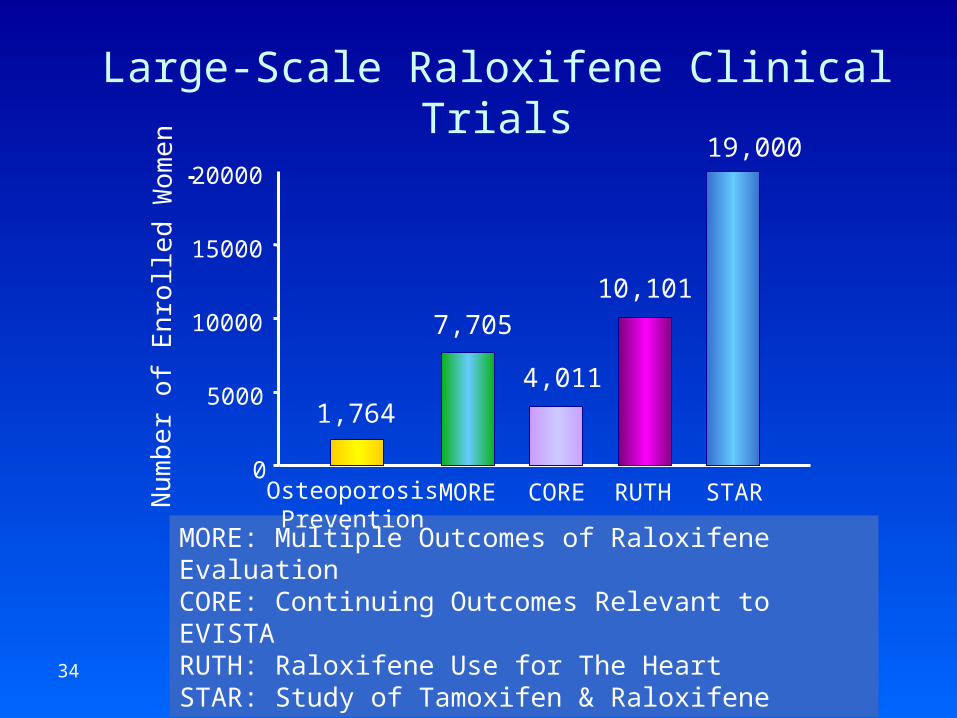
MORE: Multiple Outcomes of Raloxifene EvaluationCORE: Continuing Outcomes Relevant to EVISTA RUTH: Raloxifene Use for The HeartSTAR: Study of Tamoxifen & Raloxifene
Large-Scale Raloxifene Clinical Trials
0
5000
10000
15000
20000
7,705
4,011
10,101
19,000N
um
be
r of
Enr
olle
d W
om
en
OsteoporosisPrevention
MORE CORE RUTH STAR
1,764
35
STAR• Objectives:
– Compare Raloxifene Vs Tamoxifen for reduction of the incidence rate of invasive breast cancer in postmenopausal women
– Compare the effects on the incidence of• Intraductal / lobular carcinoma in-situ • Endometrial cancer • Ischemic heart disease,• Fractures (hip, spine, or Colles’)
– Safety of these regimens– Quality of life
• N = 19,000• Length : 5 years• Primary results are expected in 2006
36
Raloxifene Use for The HeartTrial Design
• Double-blind, placebo-controlled, long-term coronary & breast cancer outcomes trial in postmenopausal women at risk of acute coronary events
• Combination of secondary and primary prevention (women with documented CAD and / or risk factors)
• Started in 1998 (enrollment complete 8/2000)
• N=10,101
• Length: up to 7.5 y
Mosca LM et al., Am J Cardiol 2001;88:392-395
37
NICE Recommendation on Raloxifene; 10/2005 Draft
• Not recommended as a treatment option for primary prevention of fractures– The breast cancer benefit should not be a
driver of any positive recommendation– The cost effectiveness of fracture prevention
is unfavorable relative to bisphosphonates & strontium
38
NICE Recommendation on Raloxifene; 10/2005 Draft
• For secondary prevention of osteoporotic fractures:– Raloxifene was not as effective or cost-effective as
bisphosphonates or strontium for treating osteoporosis
– The effect on prevention of breast cancer has not been assessed by the regulatory authorities
– The long-term risks beyond 8 years are uncertain
• Raloxifene should be recommended as a treatment option when bisphosphonates or strontium are contraindicated / impractical / ineffective
39
Cost-effectiveness of Raloxifene
• Examining the health economic implications of raloxifene treatment for 5 years, followed by no treatment for 5 years
• In a UK setting
• Based on the results of MORE
• Compared to no treatment
• The threshold of cost effectiveness used by NICE* for starting treatment between age 50-80y 30,000 £
*National Institute of Clinical Excellence
Kanis J. Osteoporos. Int. 2005;16:15
40
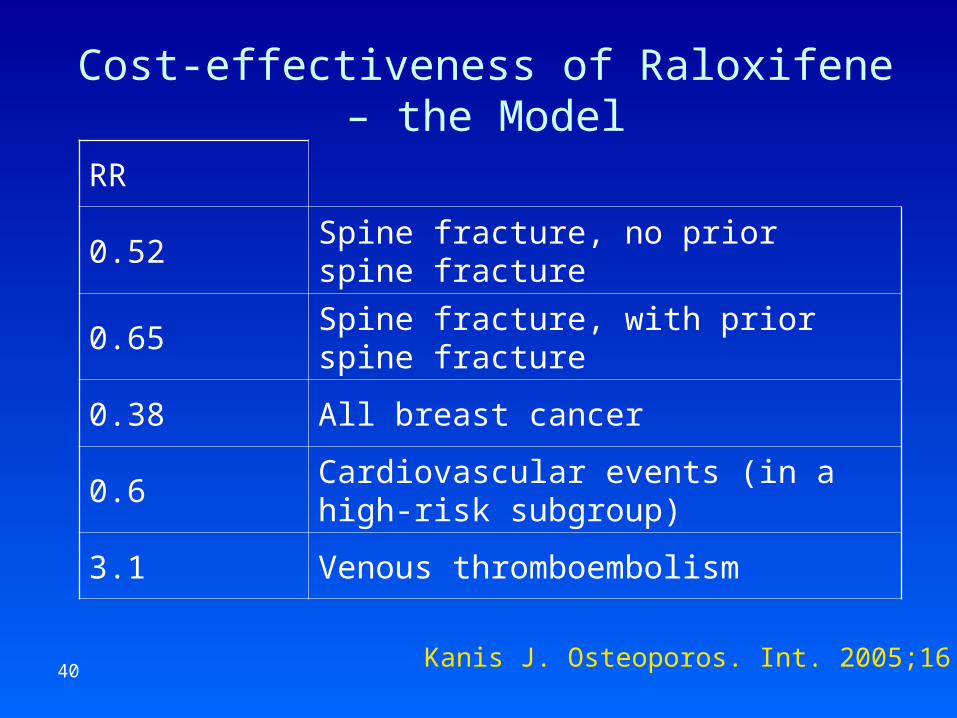
Cost-effectiveness of Raloxifene – the Model
Kanis J. Osteoporos. Int. 2005;16:15
RR
Spine fracture, no prior spine fracture0.52
Spine fracture, with prior spine fracture0.65
All breast cancer 0.38
Cardiovascular events (in a high-risk subgroup)
0.6
Venous thromboembolism3.1

41
Cost-effectiveness of Raloxifene - UK
Kanis J. Osteoporos. Int. 2005;16:15
Cost per year gained (£)
No prior spine fractureWith prior spine fracture
Age QALYLife-yearQALYLife-year
5018,00018,00018,00018,000
6023,00024,00024,00024,000
7018,00019,00018,00019,000
8021,00021,00020,00021,000

42
True Cost of Medications in Israel is the Best Kept Secret
Feasibility of Cost-effectiveness Analysis in Israel ?
43
Summary & Unanswered Questions
• Raloxifene is an alternative for bisphosphonates for treatment / prevention of osteoporosis when hip fracture risk is estimated to be low
• Raloxifene is less effective than bisphosphonates in preventing bone loss in postmenopausal women
• Raloxifene reduces the risk of invasive ER+ breast cancer– What is the best drug for prevention of breast cancer?– Who should be treated? – The optimal duration of preventive therapy?– Is there a survival benefit?– Should postmenopausal women at increased risk of breast cancer
receive raloxifene ?• If they are taking other anti-osteoporotic agents?• If they do not have osteoporosis?
– Can SERM’s be combined with HRT?



![arXiv:1707.06053v2 [cs.CV] 20 Jul 2017 · 2 Sheba Medical Center, Diagnostic Imaging Department, Tel Hashomer, Israel 3 Engineering Faculty, Bar-Ilan University, Israel Abstract](https://img.pdfslide.us/doc/110x75/5f4b78873807d920b93030e7/arxiv170706053v2-cscv-20-jul-2017-2-sheba-medical-center-diagnostic-imaging.jpg)

























