Embed Size (px)
Citation preview

1
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
Burnout and Compassion Fatigue Literature Review
Barbara J. Henry
Northern Kentucky University
2
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
Introduction
Burnout and compassion fatigue are conditions that occur in many professionals,
particularly nurses working in high trauma specialties such as oncology. The purpose of this
paper is to review the literature and briefly describe the conceptual framework for burnout and
compassion fatigue in oncology nurses. The literature search was conducted using CINAHL,
MEDLINE, and PSYCHInfo databases along with articles obtained from Really Simple
Syndication (RSS) feeds and hand selection using the search terms of “burnout.” “compassion
fatigue,” “burnout and compassion fatigue in nurses,” and “burnout and compassion fatigue in
oncology.” Findings were grounded in the literature from nursing, medicine, psychology, social
work, and palliative care professions. The literature review was limited to the past 10 years
except for older original works on burnout and compassion fatigue. Articles on related topics
were also reviewed. Articles selected for the literature review are directly urelated to the
research question: how does a therapeutic retreat effect burnout and compassion fatigue in
oncology nurses?
Background and Conceptual Framework
In Boyle’s review of literature, antecedents to burnout and compassion fatigue included
the following: 1.) exposure to traumatic care of cancer patients, 2.) vulnerable individual
personality traits and lack of coping skills, or 3.) lateral violence from others (2011). Bush, like
Boyle, is a nursing author who has written extensively on burnout and compassion fatigue in
oncology nurses. Bush noted that burnout and compassion fatigue occur when emotional
boundaries are blurred and the nurse absorbs distress, anxiety, fears, and trauma of the patient, (a
concept called countertransference in psychiatry), (2009). Collins & Long reported a
consequence of compassion fatigue and burnout is “unresolved emotional pain that caregivers
3
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
‘store away’” (2003 p 18). Difficulty balancing work and life outside work may be an
antecedent to or consequence of burnout and compassion fatigue as well.
Many articles define and describe the concepts of burnout and compassion fatigue. The
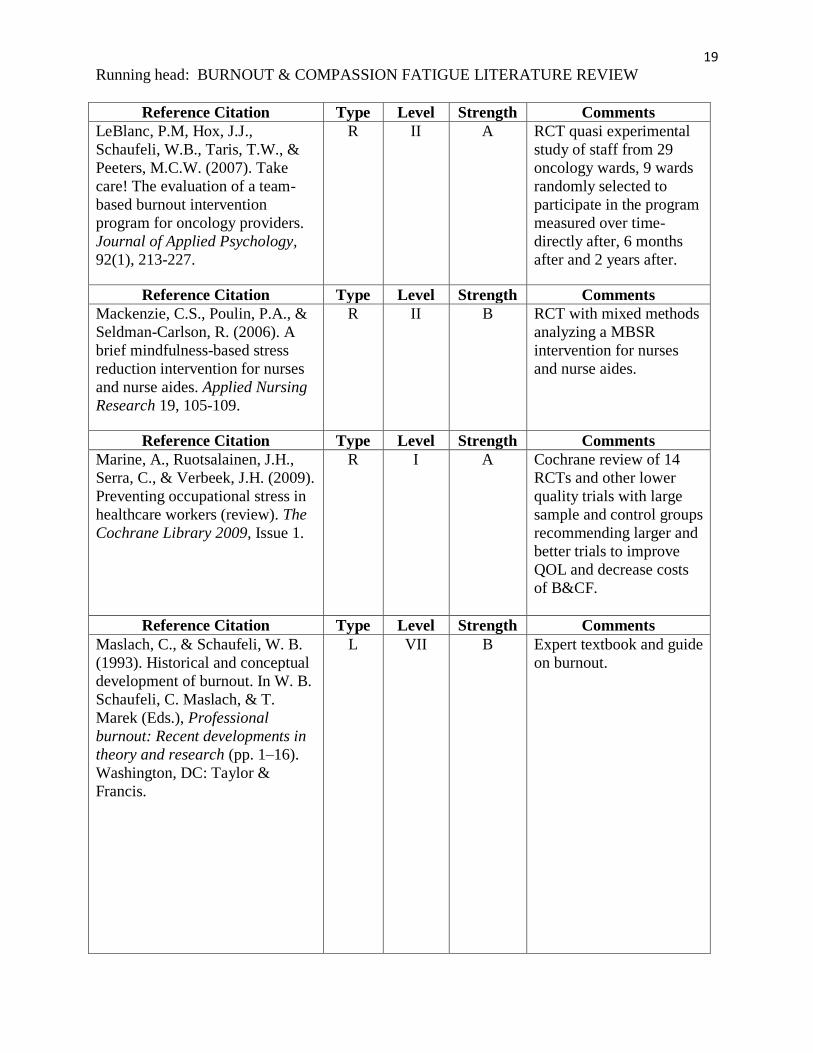
concept of burnout was first conceptualized by Christina Maslach who developed the Maslach
Burnout Inventory (MBI) tool to measure burnout in healthcare and other professional workers
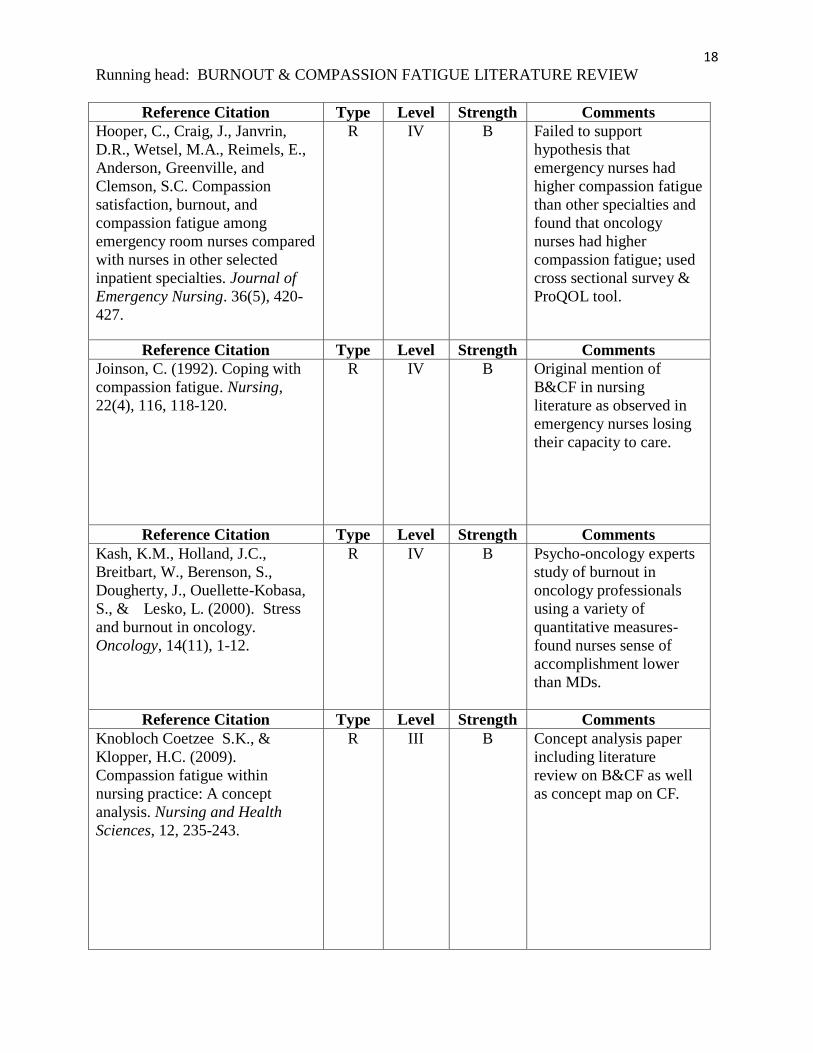
(Maslach,& Schaufeli, 1993). Compassion fatigue was first introduced by Joinson in 1992
during an investigation of burnout in emergency nurses. Joinson never formally defined
compassion fatigue and in 1995, it was adopted by psychologist Charles Figley as a term for
secondary traumatic stress disorder (Figley, 1995).
Pilkington suggested a conceptualization of burnout and compassion fatigue from the
perspective of the Neuman systems model (2008). Jean Watson’s seven assumptions of nurse
caring provide the theoretical underpinnings of potential for burnout and compassion fatigue
(Current Nursing, 2012).
Burnout, compassion fatigue, and related concepts have been topics of interest in nursing
literature, particularly in the past five years (Knobloch Coutzee & Klopper, 2005). The concept
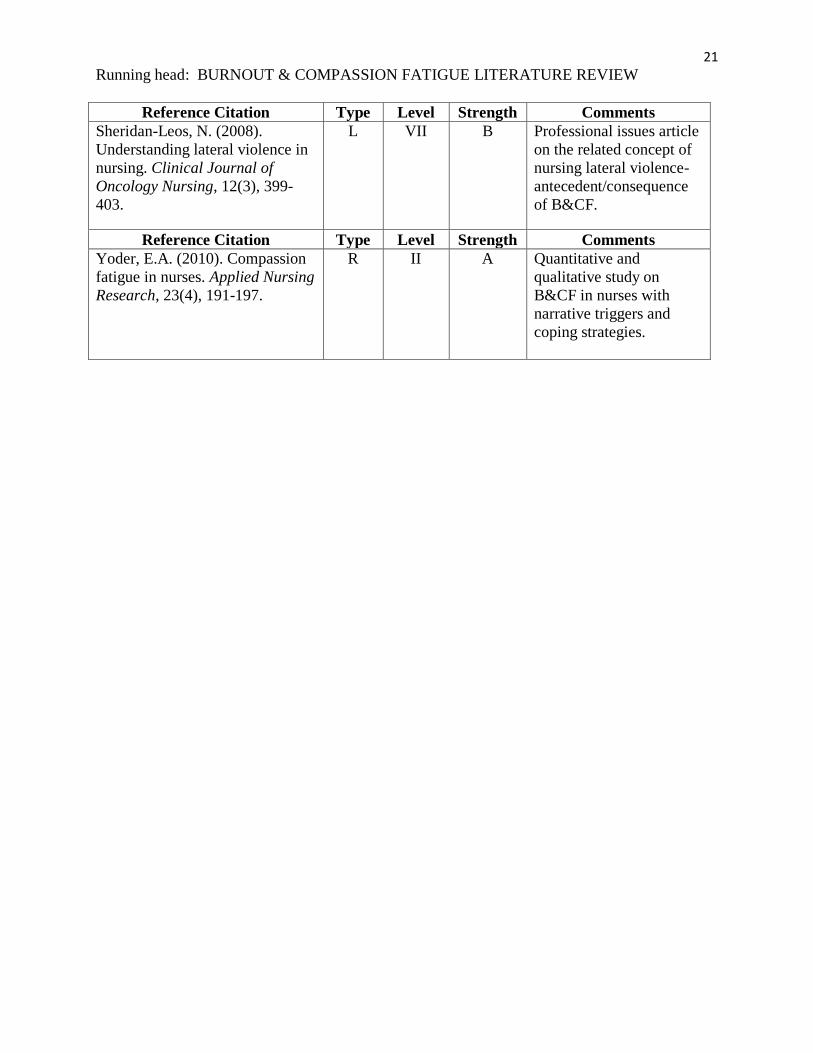
of lateral violence has emerged in the literature as both an antecedent and consequence of
burnout and compassion fatigue (Sheridan-Leos, 2008).
Description and Critique of Scholarly Literature
There are very few randomized clinically controlled trials (RCTs) examining burnout and
compassion fatigue in oncology nurses or healthcare professionals. Most articles are reviews of
RCTs, review of literature, and qualitative studies.
A 2010 study utilized a two arm randomized controlled mixed methods trial using 65
medical personnel with direct patient contact as participants (Brooks, Bradt, Eyre, Hunt, &

4
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
Dileo, 2010). Results showed no statistically significant difference in change scores between the
control and experimental groups for self-reported burnout, sense of coherence, and job
satisfaction (Brooks, et al., 2010). Qualitative findings indicated that music imagery and creative
mandala drawings helped participants relax, rejuvenate, and refocus enabling them to complete
their shifts with renewed energy (Brooks, et al., 2010). A limitation of this study was the sample
size and that shortly after the study began a major restructuring at one of the hospitals resulted in
layoffs, increased shifts, and fear of termination for open admission of feeling burned-out during
the process, and many planned music-imagery sessions were cancelled affecting study findings
(Brooks, et al., 2010).
16 participants in a brief mindfulness intervention for nurses and nurse aids experienced
significant improvements in burnout symptoms, relaxation, and life satisfaction compared to 15
wait list control participants (Mackenzie, Poulin, & Seidman-Carlson, 2006). Each week,
participants from large urban geriatric teaching hospital attended one of 6 sessions held during
the day and evening shifts and received a CD of guided mindfulness exercises, which they were
instructed to practice for at least 10 minutes per day 5 days per week along with a manual
summarizing key points from the sessions and homework assignments (Mackenzie, et al., 2006).
Mackenzie and colleagues utilized the MBI, Smith Relaxation Dispositions Inventory, and
Intrinsic Job Satisfaction subscale from the Job Satisfaction Scale, Satisfaction with Life scale,
and 13 item version of the Orientation to Life Questionnaire to measure quantitative data (2006).
An obvious limitation of this study was the sample size, but results of the study support the
feasibility and potential effectiveness of brief mindfulness training in reducing burnout and
improving morale in nurses (Mackenzie, et al, 2006.)
5
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
Marine, Ruotsalainen, Serra, & Verbeek conducted a review of RCTs on interventions
aimed at prevention of psychological stress and burnout in healthcare workers (2009). Authors
presented a meta-analysis and qualitative synthesis of 14 RCTs, 3 cluster randomized trials, and
2 crossover trials with a total of 1,564 participants in intervention groups and 1,248 participants
in control groups (Marine, et al., 2009). The main limitation of these studies were that only two
of the trials were of high quality. Interventions were grouped into person-directed and work-
directed. One trial showed stress remained low a month after the intervention, another showed a
reduction in emotional exhaustion and in lack of personal accomplishment maintained up to two
years post-intervention with refresher sessions (Marine, et al., 2009). Two studies showed a
reduction in anxiety maintained up to a month post-intervention (Marine, et al., 2009). The
authors recommended larger and better quality trials and concluded that person-directed
interventions including cognitive behavioral approaches like coping skills training combined
with relaxation techniques can be effective in reducing burnout in healthcare workers compared
to no intervention (Marine, et al., 2009).
Najjar and colleagues reviewed 57 studies with healthcare workers and found a variety of
terminology used to describe burnout and compassion fatigue (Najjar, Davis, Beck-Coon, &
Carney Doebbling, 2009). The authors described 14 studies on compassion fatigue with various
healthcare professionals, the largest sample being 336 county child protection staff and one
clinical trial examining the treatment effectiveness of the Certified Compassion Fatigue
Specialists Training (CCFST) for mental health professionals (Najjar, et al., 2009). The authors
acknowledged that conceptual and methodological research on the problem is lacking, and
summarized personal, professional, and organizational strategies to manage and treat compassion
fatigue (Najjar, et al., 2009).

6
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
In a study on nurse practice environments and patient outcomes, Friese (2005) used a
large sample of 1956 registered nurses including 305 oncology nurses. The study was a
secondary analysis of survey data collected in 1998 using statistical analysis instruments
including logistic regression (Friese, 2005). Though the data was old, a limitation of the study,
the author found that oncology nurses had superior patient outcomes compared to non-oncology
nurses and that emotional exhaustion was significantly lower for nurses working in magnet
hospitals compared to those working in non-magnet hospitals (Friese, 2005). Friese’s key points
were that nurse concern with practice environments was reflected by their job dissatisfaction,
burnout, and perceived quality of care, and to improve outcomes, practice environments should
be assessed routinely to optimize the success of nursing interventions (2005).
Kash, Holland, Breitbart, Berensen, Dougherty, Ouellette-Kobasa, and Lesko identified
the concept of a hardy personality, social support, and relaxation methods as moderating
variables that may decrease burnout and compassion fatigue in oncology professionals (2000).
Three attributes of a hardy personality found to be buffers against stress were: commitment to
self and work, a sense of being able to control or influence events, and a sense of challenge in the
face of a changing environment (Kash, et al., 2000). The cross-sectional survey data from 83
nurses and 178 oncologists at Memorial Sloan Kettering Cancer Center (MSKCC) was studied
over a two year period (Kash, et al., 2000). The MBI, demoralization scale of the Psychiatric
Epidemiology Research Interview (PERI), somatization scale of the Hopkins Symptom
Checklist, Kobasa personality scale, peer cohesion subscale of the Work Environment Subscales,
perception of religious person scale, and a stress questionnaire were used to quantify results
(Kash, et al., 2000). Nurse sense of accomplishment was much lower than house oncology
medical staff, which the authors attributed to nurses seeing patients with cancer when they are
7
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
most ill, a sense of futility about cancer treatment, anger and cynicism about limited role of
nurses in the overall treatment trajectory (Kash, et al., 2000). Stressors that contributed most to
burnout and demoralization were negative work settings, high number of patient deaths, and
struggling over a DNR decision with another colleague or family member (Kash, et al., 2000).
These psycho-oncology expert authors concluded that cancer centers must explore means of
reducing work stress in order to emotionally equip professionals to effectively communicate and
provide support to patients (Kash, et al., 2000).
In a study of emergency nurses and nurses from three other specialty hospital units:
oncology, nephrology, and intensive care, the authors found a risk for higher risk for burnout and
compassion fatigue in oncology nurses (Hooper, Craig, Janvrin, Wetsel, Reimels, Anderson,
Greenville, & Clemson, 2010). Findings failed to support the hypothesis that emergency nurses
are at greater risk for burnout and compassion fatigue compared to nurses from other specialties
(Hooper, et al., 2010). Compassion satisfaction, burnout, and compassion fatigue scores were
measured using the Professional Quality of Life, Fourth Revision (ProQOL R-IV) instrument.
Limitations of the study were the small sample size of 109 respondents chosen from one 461 bed
acute care hospital in the Southeast measured at a single point in time. Despite study limitations,
authors concluded that raising the awareness of the emotional impact on nurses of caring for
patients will lead to the development of ongoing support programs for hospital nurses (Hooper,
et al., 2010).
Yoder also utilized the ProQOL scale to measure compassion fatigue, compassion
satisfaction, and burnout in nurses employed at a 123 bed Midwest Magnet community hospital
(2010). Yoder found that 15% of participants had ProQOL scores indicating risk for compassion
fatigue, 2010). In addition to the Pro-QOL scale, Yoder solicited qualitative data by asking
8
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
participants to “describe a situation where you experienced compassion fatigue and burnout and
what strategies did you use to deal with the situation?” (2010, p.193). 71 nurses completed the
narrative portion and described trigger situations for burnout and compassion fatigue: 1.) patient
condition/status, 3.) challenging behavior, 4.) futile care, 5.) workload, 6.) management
decisions, 7.) personal limits, and 8.) personal experiences (Yoder, 2010). Coping strategies
included: a.) change personal engagement, b.) change nature of work involvement, c.) debrief
informally, d.) take action to change/manage current situation, e.) develop ritual, f.) life outside
work, g.) spiritual or religious, h.) introspection, and i.) attitude modification (Yoder, 2010).
Yoder’s study limitations were small sample size from one hospital taken at one point in time.
Edmunds provided further detail on Yoder’s findings that compassion fatigue was triggered by
patient care situations in which the nurse 1.) believed their actions would not make a difference
or not be enough, 2.) had problems with the system-high census and acuity, heavy patient
assignments, overtime and extra work day(s), 3.) had personal issues such as inexperience or
inadequate energy, 4.) identified with the patients, or 5.) overlooked serious patient symptoms
(2010.)
Contrary to most studies, Barnard, Street, & Love found that there was no statistically
significant relationship between level of perceived work supports and level of burnout (2006).
Barnard, et al., 2006 surveyed 101 cancer nurses working at a specialist oncology metropolitan
Australian hospital. More than 50% of participants experienced a list of 50 stressors from an
amended version of the Stressor Scale for Pediatric Oncology Nurses and found that most work
support came from peers rather than supervisors or the organization (Barnard, et al., 2006). In
addition to the stressor scale, burnout was measured by the MBI. According to Barnard, et al.,
94% participants indicated that 2 items in particular were sources of stress: “when nurses and
9
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
doctors are not communicating well about patients,” and “feeling I can’t get all my work done”
(2006). Nurses were also given a free response comment section concerning support required
from the organization, which listed the following as the most important needs: 1.) further
nursing education, 2.) nursing administration/management support, 3.) recognition, rewards, and
support, 4.) regular staff counseling and debriefing, and 5.) services for staff (Barnard, et al.,
2006). The strength of this study is the use of two quantifiable and one qualitative tool, though a
weakness is the small sample size from one institution collected at one point in time.
There has been a great deal published about the prevalence of burnout and compassion
fatigue in oncology nursing, but less on interventions to decrease the problem. Compassion
fatigue is amenable to intervention; with therapeutic support programs and retreats, nurses may
continue to work in their chosen field (Sabo, 2011). Sabo’s extensive review of literature,
similar to that of Boyle (2011), presented a recommendation that more energy should be focused
on psychosocial health and well-being of nurses (2011).
In a quasi-experimental RCT among staff of 29 hospital oncology units in the
Netherlands, Le Blanc, Hex, Schaufeli, Tarsi and Pesters evaluated the effects of a team-based
burnout intervention program combining a staff support group with a participatory action
research approach. Nine oncology units were randomly selected to participate (2007). Before the
“Take Care” program started (Time 1), directly after the program ended (Time 2), and 6 months
later (Time 3), participants filled out a questionnaire on their work situation and well-being
(LeBlanc, et al., 2007). Staff who participated in the program experienced significantly less
emotional exhaustion at both Time 2 and Time 3 and less depersonalization at Time 2, compared
with staff who did not participate in the program (LeBlanc, et al., 2007). Often in the formal
training of oncology nurses, there is no solid basis of psychosocial awareness, knowledge, and
10
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
skills to facilitate coping (LeBlanc, et al., 2007). Participants in the “Take Care” program
experimental group felt significantly less exhausted than those in the control group immediately
after the program and again six months later (Le Blanc et al., 2007).
Medland, Howard-Rubin, and Whitaker (2004) identified psychosocial wellness and the
avoidance of burnout as key to retention of oncology nurses, and described a program to enhance
oncology nurse coping skills. Turnover rates on the oncology units was greater than 40%
compared to a hospital average of 14.2%, which lead to the study (Medland, et al., 2004). Five
full day “Circle of Care” retreats with 150 oncology staff members were held away from the
clinical area in a relaxed setting in a large Midwest cancer center (Medland, et al., 2004). The
retreats offered interactive and informal presentations on wellness, bereavement, developing
stress management skills like relaxation, journaling, cultivating team effectiveness, and art
making activities (Medland, et al. 2004). Participants viewed a videotape on a positive
management philosophy and discussed the “CARES” philosophy, a framework for incorporating
stress management and self-care into practice (Medland, et al. 2004). Practice changes to
decrease burnout and increase ongoing focus on staff support at the facility were implemented
based on ideas generated at the retreats (Medland, et al. 2004). Though the study and
intervention provided valuable data on a burnout and compassion fatigue intervention, the
authors did not utilize any quantitative data or tools to measure the effects.
Adcock and Boyle examined existing interventions to manage compassion fatigue in
oncology nurses (2009). They surveyed 231 Oncology Nursing Society chapter presidents in
2007 and received 103 responses. 22% or fewer respondents had on-site resources such as:
employee assistance programs (EAPs), pastoral care, counselor or psychologist, psychiatric
clinical nurse specialist, and support group (Adcock & Boyle, 2009). The authors found that
11
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
those with EAPs have three free visits available per year with discount for ongoing services, and
that a barrier to obtaining other counseling services was the lag time between request and
scheduled time available for an appointment (Adcock & Boyle, 2009). Only 5% of respondents
reported exposure to staff support groups and that the groups were rarely continued over time
(Adcock & Boyle, 2009). Though off-site retreats to promote renewal were experienced by only
a few respondents, qualitative data reflects the value of these retreats to participants (Adcock &
Boyle, 2009). A weakness in this study is that no quantitative data or measures were obtained.
Hayes and colleagues wrote about retention strategies implemented at large Eastern U.S.
cancer centers that decrease burnout and increase support for oncology nurses (Hayes, Reid
Ponte, Oakley, Stanhellini, Gross, Perryman, Hanley, Hickey, & Somerville, 2005). Strategies
included: a New Graduate Development Program, Support Mentorship and Respect Together in
Nursing (SMaRT) a mentoring program designed to support minority nurses entering oncology,
Oncology Nursing Leadership Advisory Group with cross institutional participation, oncology
nursing grand rounds and educational programs, Spirit Rounds, Reflective Practice rounds,
narratives for individual reflection on practice, ambulatory nursing retreats for reflection and
renewal, and individual meetings with a psychiatric clinical nurse specialist for new graduates,
all with favorable outcomes despite some initial implementation difficulties (Hayes et al., 2005).
This study reported qualitative but not quantitative data.
Bauer Wu and colleagues facilitated overnight staff renewal retreats with oncology
nurses from a large Eastern U.S. cancer center in 2005 (2005). Goals of the retreats included
bringing staff together outside the work setting to relax, have fun, revisit self-care and self-
reflection as well as rekindling spirit in order to feel rejuvenated and professionally re-inspired
(Bauer Wu, 2005). The retreat theme was “Creating Balance and Peace in a Life of Blessings
12
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
and Losses,” with participant choice of four experiential break-out sessions: “Keeping the
Hope” using art, imagery, and story to restore hopefulness as a self-care practice, “Coming
Home to Your Body,” using therapeutic movement, “Being Peace” using mindfulness meditation
to foster peace and balance in everyday life, and “What Matters Most” for self-reflection and
expression through collage and writing (Bauer-Wu, 2005). Though no quantitative evaluation
tools were used, the author reported that participants acknowledged appreciation for the unique
experience of fun, personal growth, and knowledge (Bauer Wu, 2005).
Potter and colleagues studied prevalence of burnout in a large Midwest U.S. cancer
center, and an intervention based on the needs of the center that did not have an existing program
in place. Staff facilitators were trained to meet the unique needs of the staff and presented a
series of four 90-minute training sessions and a four hour retreat designed to help RNs gain skills
to reduce burnout (Potter, et al., 2010). The ProQOL R-IV was administered pre and post-
intervention, along with qualitative measures reflecting positive outcomes for program
participants. There was no wait list control group.
An 8-week mindfulness-based stress reduction program was offered to 25 nurses at an
Eastern U.S. hospital and health network funded by the organization and the senior VP for
clinical services who was one of the study investigators (Cohen-Katz, Wiley, Capuano, Baker,
Deitrick, & Shapiro, 2005). Qualitative and quantitative data from the study found the
intervention to be effective in improving relaxation, self-care, work and family relationships,
though the process at times generated challenges like restlessness, pain, and dealing with
difficult emotions (Cohen, et al, 2005).
13
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
Inferences for Future Research
Further research is needed to develop a theory of compassion fatigue for nursing practice
(Knobloch Coutzee & Klopper, 2010). Additional research may determine factors that
contribute to the progression from compassion discomfort to compassion stress, and compassion
fatigue, and determine time line involved in this process (Knobloch Coutzee & Klopper, 2010).
More studies are needed that evaluate interventions for preventing and reducing nursing burnout
compassion fatigue as well (Knoblach Coutzee & Klopper, 2010).
Randomized clinical trials conducted at multiple sites on the effect of therapeutic
interventions on oncology nurse burnout and compassion fatigue are needed to establish
empirical data on solving the problem. Studies show that the effects of these interventions may
last 6 months to 2 years (Marine, et al., 2009) demonstrating cost savings to healthcare
organizations providing regular burnout and compassion fatigue interventions to recruit and
retain nurses and improve patient outcomes.
Conclusions
Fatigue, stress, sadness, decrease in morale, and poor work performance, are all
influenced by psychosocial factors that have often been ignored by nurses and healthcare
administration (Boyle, 2012). Klobach Coutzee & Klopper (2010) believed that increased
knowledge of compassion fatigue and its manifestations may enable nurses to become aware of
others who might be suffering and facilitate the development of a peer support network, making
it possible for nurses to seek assistance in dealing with the detrimental effects of compassion
fatigue. An employee assistance program should be established in every health-care institution,
with free counseling and life skills education services allowing nurses to seek assistance in
dealing with the emotional burden of their work (Klobach Coutzee & Klopper, 2010).
14
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
Burnout and compassion fatigue impact recruitment and retention of oncology nurses and
may influence patient satisfaction and patient safety (Potter et al., 2005). Encouraging self-care
strategies and offering interventions within and outside the workplace address a key distinction
of nursing practice, namely that of holistic care for patients and nurses (Boyle, 2011).
With experience, self-care, and support from peers and healthcare organizations,
competent oncology nurses learn to establish appropriate boundaries that are more semi-
permeable than other clinical specialties. Because of the semi-permeable boundaries unique to
oncology nursing and high risk of developing burnout and compassion fatigue, oncology nurses
need annual therapeutic programs in addition to more frequent support outlets. Compassionate
nurses are an essential and dwindling resource in today’s healthcare system, and nurses must be
supported and cared for by providing nurses with time to share feelings and develop coping
strategies (Edmunds, 2010).

15
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
References
Graded references are listed according to the following legend from O’Neil, Dluhy,
Fortier, & Michael (2004) and Polit (2012) :
Legend Type: R= Research L= Literature N= National Guideline
Levels: I= Systematic Review of RCT, Systematic Review of Non-Randomized Trial
II=Single RCT, Single Non-Randomized Trial
III= Systematic Review of Correlational or RCT, Observational Studies
IV= Single Correlational or Observational Study
V=Systematic Review of Descriptive/Qualitative/Physiologic Studies
VI=Single Descriptive/Qualitative/Physiologic Study
VII=Opinion of Authorities, expert committees
Strength: A= Good evidence to support a recommendation
B= Moderate evidence to support a recommendation
C= Poor evidence to support a recommendation
O'Neill, E.S., Dluhy, N.M., Fortier, P.J., & Michael, H.E. (2004). Knowledge acquisition,
synthesis, and validation: A model for decision support systems.
Journal of Advanced Nursing, 47 (2), 134-142.
Polit, D. F. (2012). Evidence-based nursing: Translating research evidence into practice. In D. F.
Polit, Nursing Research: Generating and Assessing Evidence for Nursing Practice (pp.
25-47). Philadelphia, PA: J. B. Lippincott Company.
Reference Citation Type Level Strength Comments
Aycock, N. & Boyle, D. (2010).
Interventions to manage
compassion fatigue. Clinical
Journal of Oncology Nursing,
13(2), 183-191.
R IV A National survey to
determine resources
available to oncology
nurses for dealing with
burnout and compassion
fatigue (B&CF).
Reference Citation Type Level Strength Comments
Barnard, D., Street, A., & Love,
A. (2006). Relationships between
stressors, work supports, and
burnout among cancer nurses.
Cancer Nursing. 29(4), 338-345.
R IV B Pilot study of 101
Australian oncology
nurses using self-report
questionnaires and
Maslach Burnout
Inventory, moderate to
low burnout results.

16
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
Reference Citation Type Level Strength Comments
Bauer-Wu, S. (2005). Seeds of
hope, blossoms of meaning.
Oncology Nursing Forum, 32(5),
927-933.
R VI B Summary of B&CF
programs for oncology
nurses.
Reference Citation Type Level Strength Comments
Brooks, D.M., Bradt, J., Eyre, L.,
Hunt, A., & Dileo, C. (2010).
Creative approaches for reducing
burnout in medical personnel.
The Arts in Psychotherapy, 37,
255-263.
R II B RCT using music and art
therapy to reduce burnout
in 65 medical
professionals at an urban
hospital.
Reference Citation Type Level Strength Comments
Boyle, D. (2011). Countering
compassion fatigue: A requisite
nursing agenda. Online Journal of
Issues in Nursing, 13(1).
R I A Review of current
literature and research and
need for B&CF.
Reference Citation Type Level Strength Comments
Bush, N.J. (2009). Compassion
fatigue: Are you at risk?
Oncology Nursing Forum, 36(1),
24-28.
R VII B Case studies on B&CF,
differences/similarities
between B & CF, and
self-care.
Reference Citation Type Level Strength Comments
Cohen-Katz, J., Wiley, S.,
Capuano, T., Baker, D., Deitrick,
L., & Shapiro, S. (2005). The
effects of mindfulness-based
stress reduction on nurse stress
and burnout a qualitative and
quantitative study, part III.
Holistic Nursing Practice.
March/April, 78-86.
R IV B 8 week MBSR program
for 25 nurses improved
relaxation, work & family
relationships, caused
restlessness, emotional
pain dealing with difficult
emotions in group
discussions.
17
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
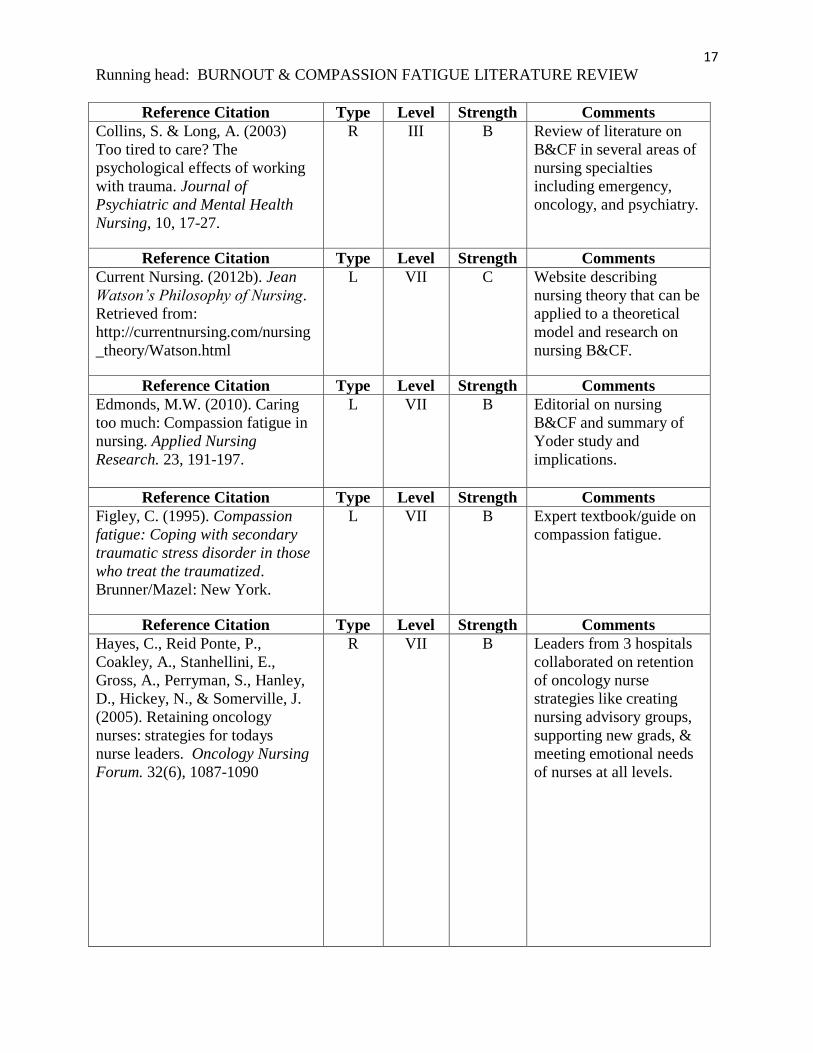
Reference Citation Type Level Strength Comments
Collins, S. & Long, A. (2003)
Too tired to care? The
psychological effects of working
with trauma. Journal of
Psychiatric and Mental Health
Nursing, 10, 17-27.
R III B Review of literature on
B&CF in several areas of
nursing specialties
including emergency,
oncology, and psychiatry.
Reference Citation Type Level Strength Comments
Current Nursing. (2012b). Jean
Watson’s Philosophy of Nursing.
Retrieved from:
http://currentnursing.com/nursing
_theory/Watson.html
L VII C Website describing
nursing theory that can be
applied to a theoretical
model and research on
nursing B&CF.
Reference Citation Type Level Strength Comments
Edmonds, M.W. (2010). Caring
too much: Compassion fatigue in
nursing. Applied Nursing
Research. 23, 191-197.
L VII B Editorial on nursing
B&CF and summary of
Yoder study and
implications.
Reference Citation Type Level Strength Comments
Figley, C. (1995). Compassion
fatigue: Coping with secondary
traumatic stress disorder in those
who treat the traumatized.
Brunner/Mazel: New York.
L VII B Expert textbook/guide on
compassion fatigue.
Reference Citation Type Level Strength Comments
Hayes, C., Reid Ponte, P.,
Coakley, A., Stanhellini, E.,
Gross, A., Perryman, S., Hanley,
D., Hickey, N., & Somerville, J.
(2005). Retaining oncology
nurses: strategies for todays
nurse leaders. Oncology Nursing
Forum. 32(6), 1087-1090
R VII B Leaders from 3 hospitals
collaborated on retention
of oncology nurse
strategies like creating
nursing advisory groups,
supporting new grads, &
meeting emotional needs
of nurses at all levels.
18
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
Reference Citation Type Level Strength Comments
Hooper, C., Craig, J., Janvrin,
D.R., Wetsel, M.A., Reimels, E.,
Anderson, Greenville, and
Clemson, S.C. Compassion
satisfaction, burnout, and
compassion fatigue among
emergency room nurses compared
with nurses in other selected
inpatient specialties. Journal of
Emergency Nursing. 36(5), 420-
427.
R IV B Failed to support
hypothesis that
emergency nurses had
higher compassion fatigue
than other specialties and
found that oncology
nurses had higher
compassion fatigue; used
cross sectional survey &
ProQOL tool.
Reference Citation Type Level Strength Comments
Joinson, C. (1992). Coping with
compassion fatigue. Nursing,
22(4), 116, 118-120.
R IV B Original mention of
B&CF in nursing
literature as observed in
emergency nurses losing
their capacity to care.
Reference Citation Type Level Strength Comments
Kash, K.M., Holland, J.C.,
Breitbart, W., Berenson, S.,
Dougherty, J., Ouellette-Kobasa,
S., & Lesko, L. (2000). Stress
and burnout in oncology.
Oncology, 14(11), 1-12.
R IV B Psycho-oncology experts
study of burnout in
oncology professionals
using a variety of
quantitative measures-
found nurses sense of
accomplishment lower
than MDs.
Reference Citation Type Level Strength Comments
Knobloch Coetzee S.K., &
Klopper, H.C. (2009).
Compassion fatigue within
nursing practice: A concept
analysis. Nursing and Health
Sciences, 12, 235-243.
R III B Concept analysis paper
including literature
review on B&CF as well
as concept map on CF.
19
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
Reference Citation Type Level Strength Comments
LeBlanc, P.M, Hox, J.J.,
Schaufeli, W.B., Taris, T.W., &
Peeters, M.C.W. (2007). Take
care! The evaluation of a team-
based burnout intervention
program for oncology providers.
Journal of Applied Psychology,
92(1), 213-227.
R II A RCT quasi experimental
study of staff from 29
oncology wards, 9 wards
randomly selected to
participate in the program
measured over time-
directly after, 6 months
after and 2 years after.
Reference Citation Type Level Strength Comments
Mackenzie, C.S., Poulin, P.A., &
Seldman-Carlson, R. (2006). A
brief mindfulness-based stress
reduction intervention for nurses
and nurse aides. Applied Nursing
Research 19, 105-109.
R II B RCT with mixed methods
analyzing a MBSR
intervention for nurses
and nurse aides.
Reference Citation Type Level Strength Comments
Marine, A., Ruotsalainen, J.H.,
Serra, C., & Verbeek, J.H. (2009).
Preventing occupational stress in
healthcare workers (review). The
Cochrane Library 2009, Issue 1.
R I A Cochrane review of 14
RCTs and other lower
quality trials with large
sample and control groups
recommending larger and
better trials to improve
QOL and decrease costs
of B&CF.
Reference Citation Type Level Strength Comments
Maslach, C., & Schaufeli, W. B.
(1993). Historical and conceptual
development of burnout. In W. B.
Schaufeli, C. Maslach, & T.
Marek (Eds.), Professional
burnout: Recent developments in
theory and research (pp. 1–16).
Washington, DC: Taylor &
Francis.
L VII B Expert textbook and guide
on burnout.

20
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
Reference Citation Type Level Strength Comments
Medland, J., Howard-Ruben, J., &
Whitaker, E (2004). Fostering
psychosocial wellness in
oncology nurses: Addressing
burnout and social support in the
workplace. Oncology Nursing
Forum, 31(1), 47-54.
R IV B Qualitative evaluation of
a program developed
because of high turnover
rate in the oncology unit
compared to the rest of
the hospital.
Reference Citation Type Level Strength Comments
Najjar, N., Davis, L.W., Beck-
Coon, K., & Doebbeling, C.C.
(2009). Compassion fatigue: A
review of the research to date and
relevance to cancer-care
providers. Journal of Health
Psychology, 14(2), 267-277.
R I B Review of 57 studies
identifying prevalence of
compassion fatigue in
oncology providers,
instruments, and
prevention and treatment.
Reference Citation Type Level Strength Comments
Pilkington, F.B. (2009).
Theorizing the concept of burnout
in nursing. Nursing Science
Quarterly, 22, 199.
L VII B Editorial and introduction
to B&CF articles,
suggested developing
nursing model based on
Neuman.
Reference Citation Type Level Strength Comments
Potter, P., Deshields, T,
Divanbeigi, J., Berger, J.,
Cipriano, D., Norris, L., & Olsen,
S. (2010). Compassion fatigue
and burnout: Prevalence among
oncology nurses. Clinical Journal
of Oncology Nursing. 14(5):E56-
E62.
R IV B Descriptive cross
sectional survey with
moderate evidence to
support the
recommendations based
on the outcomes. The
main author is an expert
on the topic.
Reference Citation Type Level Strength Comments
Sabo, B.M. (2011). Reflecting on
the concept of compassion
fatigue. , Online Journal of Issues
in Nursing, 16(1), 1-19.
R V B Review of literature with
case scenarios, suggesting
lack of theoretical clarity
and need for quantitative
and qualitative research
on nurse B&CF.
21
Running head: BURNOUT & COMPASSION FATIGUE LITERATURE REVIEW
Reference Citation Type Level Strength Comments
Sheridan-Leos, N. (2008).
Understanding lateral violence in
nursing. Clinical Journal of
Oncology Nursing, 12(3), 399-
403.
L VII B Professional issues article
on the related concept of
nursing lateral violence-
antecedent/consequence
of B&CF.
Reference Citation Type Level Strength Comments
Yoder, E.A. (2010). Compassion
fatigue in nurses. Applied Nursing
Research, 23(4), 191-197.
R II A Quantitative and
qualitative study on
B&CF in nurses with
narrative triggers and
coping strategies.














![Compassion Fatigue, Burnout and Work Related- Stress …3)15/11.pdf · compassion fatigue in nursing literature was two Compassion fatigue evolves from a state of decades ago [2]](https://img.pdfslide.us/doc/110x75/5ab1e8c97f8b9ac66c8d09f2/compassion-fatigue-burnout-and-work-related-stress-31511pdfcompassion-fatigue.jpg)














