Embed Size (px)
Citation preview

London (North West)
Haemoglobinopathy Registry
1
Process and Outcomes of a Process and Outcomes of a Multicentre Sickle Cell Disease Multicentre Sickle Cell Disease
Registry for Patient Management and Registry for Patient Management and ResearchResearch
44thth July 2006 July 2006
Annette Gilmore RN, MScHaematology Department, Central Middlesex Hospital, London.
www.europeanhbregistry.org.uk or www.hbregistry.org.uk

2
IntroductionIntroduction
The European Haemoglobinopathy Registry (EHR) is based in the Haematology Department, Central Middlesex Hospital, London, UK.
It collects longitudinal clinical and demographic information on sickle cell disease (SCD) patients to assist with their clinical management and for research.
Two national reports1 recommended the establishment of population based information systems as vital for improvement of services for SCD.1 National review of Haemoglobinopathy services: SMAC Report (1993) and Fair Shares for London (1997).

3
Inherited disease of red blood cells. Abnormal haemoglobin causes red blood cells to become stiff and
malformed, causing blockages insmall blood vessels.
Approximately 10,000 people with SCD in UK. Disease severity varies among individuals and during life cycle. Symptoms – pain episodes, chronic anaemia, severe infections and
damage to vital organs. Treatment aimed at symptom prevention & control. Minority cured by bone marrow transplant. Reduced life expectancy.
What is Sickle Cell Disease (SCD) ?What is Sickle Cell Disease (SCD) ?

4
AimsAims
Study the natural history of the Haemoglobinopathies.
Evaluation of treatments – Hydroxyurea, Blood Tx, Chelating Agents (Desferal & L1).
Management tool for improving patient care.
Accurate information for clinical practice, clinical governance & audit, and planning services.
Collaboration and information sharing.
Impact on future research.

5
EHR Research Ethics ProcessEHR Research Ethics Process
Data Protection Act Registration[Registration No. Z5730583].
MREC [Approval - MREC/99/2/4].
LREC [Approval - BEC 612].
Patient Information and Consent Forms.
Secure Access to Registry (PATS): Password Access. Encrypted Data Communications.

6
Sampling MethodSampling Method
Comprehensive list of all eligible patients created.
Inclusion criteria: All patients with SCD diagnosis (e.g. SS, SC, SBthal). Attends participating hospital as an outpatient or
inpatient.
Exclusion criteria: Failure to obtain consent.
All consecutive cases selected since November 1999.

7
Data Collection and ReportingData Collection and Reporting
Initial registration requires retrospective review of patients‘ medical records.
Follow-up proformas are completed annually.
Additional proformas are completed as required (e.g. Adverse Events, Hydroxyurea and Transfusion Therapy).
Automated data validation, processing and clinical reporting.
Web site for general public and members.
Data collection tools and reports available to members via secure website.

8

9

10

11

12

13

14
Achieving Reliability and ValidityAchieving Reliability and Validity
The quality of a database is assessed by its “coverage” and “accuracy”.
Robust sampling method. Data abstractors blinded to hypotheses. Standardized proformas. Glossary with definitions of clinical events. Guidelines for proforma completion. Consensus management of conflicting and 'difficult to interpret' data. Abstractors are health professionals or experienced heathcare employees. Abstractors receive training, ongoing supervision and support. Sample of data source (patient medical records) are second checked. Automated data validation and processing. Draft patient reports returned to abstractors for verification and completion of missing
and/or conflicting information. Intraobserver and interobserver reliability study of abstractors in progress. Assessing completeness of variables.

15
ResultsResults
626 patients out of 927 consented.
474 patients (216 males, 258 females) have data collected, totalling 4,515 patient years (yrs) of data.
Mean length of follow-up is 9.5 yrs(SD 9 yrs, range 0 mths - 42 yrs).
Mean age is 25.8 yrs(SD 15.8 yrs, range 0 yr - 74 yrs).
Patients on Hydroxyurea (HU) Treatment: 258 patient yrs of HU data has been collected on 70 patients. Mean length of follow-up is 3.7 yrs
(SD 3 yrs, range 0 mths - 11 yrs).

16
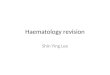
North West London & RegistryNorth West London & RegistryPopulation by Age GroupPopulation by Age Group

17
North West London & RegistryNorth West London & RegistryPopulation by Haemoglobinopathy TypePopulation by Haemoglobinopathy Type

18
Funding StructureFunding Structure
The registry has no formal long-term funding.
Funding to set-up and run the central registry at CMH and to set-up and collect data in the four local participating hospitals is approx. £575,000 over 6½ years. Cost per patient year of data is approx. £115.
Funded by: Research grants (DoH x 2, European sources). 3 year development project grant from local PCTs. Brent PCT funding – 3 years. Charitable monies.

19
How can you contact us?How can you contact us?
Email: [email protected]
By post:Annette GilmoreHaematology DepartmentCentral Middlesex HospitalActon LaneLondonNW10 7NS
Web site: www.europeanhbregistry.org.uk or www.hbregistry.org.uk
Telephone: +44-(0)20-8453 2135+44-(0)20-8453 2112/2113 (Haematology Office)
Fax: +44-(0)20-8965 1115