Embed Size (px)
Citation preview

1
Presented by:Diana Knaebe, Heritage Behavioral Health Center
Macon County Initiative Integrating Behavioral Health and
Primary Care

2
Integration Partnership Background
1. Description/History of Partnerships
2. Rationale for involvement
3. Evolution of Partnerships and programs – services offered
4. Next Steps

3
Heritage Behavioral Health Center
Community Health Improvement Center

4
Integration Partnership Background
Description/History of PartnershipCommunity Health Improvement Center and
Heritage
Have had working relationship for the past fifteen years; initially, there were cooperative efforts with mutual referrals to assure that clients received needed primary care/mental health services.
Early on the entities worked cooperatively with a local pharmacy, and developed a system utilizing bubble cards containing daily prescribed dosages of medications for medical and psychiatric problems which could be taken by the client on a daily basis.

5
Integration Partnership Background
• In July 2006, the United Way funding allowed Heritage to provide an adult psychiatrist on-site at CHIC. This psychiatrist provided psychiatric care, support, and follow up to patients, and consultation to medical physicians 9 hours per month. The CHIC physicians were so pleased with the immediate psychiatric consultation available that the pediatric providers requested on-site psychiatric availability.
• Consequently, in April 2007, a child and adolescent psychiatrist was added. He provides mental health services to the primary heath center 4 hours per month, direct care to patients, and consultation and education to the medical physicians.

6
Integration Partnership Background
• United Way funding allowed CHIC to provide a APN as well as a liaison on-site at a Homeless Day Center operated by Heritage. This allowed access to health care by individuals many of whom had not received health care in years.
• Both organizations have attended the National Council’s Integrated Care Sessions for past 5 years.
Participated in National Council’s Integrated Collaborative Care Project in 2007
Participated in MHCA Integrated Healthcare Learning Community August 2009-November 2010

7
Rethinking the Format of Visions
M E D I C A L H O M E Primary Care Mental Health Clinic Center
U N I F I E D F U N D I N G
CORE COMPETENCIES
CORE PROGRAMS
INTERVENTIONS

8
Reasons/Rationale for Partnerships
Ultimately to Implement a patient centered medical home – true integration of care
Better Overall health outcomes.Improved access and retention of clients
Joint referral process and records access Clinical processes defined for collaboration and joint education for staff Nurse practitioners and/or Physician Assistants at both CHIC and
Heritage Clients only seen at one site for all needs – as much as possible unless
need specialty care Maximizing revenue (current and new services) Efficient/effective/efficacious care Non-duplication of care and services Education sharing component for staff and clients

9
Cultural Issues/differences
Term-language Differences How patients/clients are seen – length of time
for visit and follow upFunding Streams and Mechanisms often very
differentDetermination of “hand-offs” and/or referrals
Releases – Medical Records

10
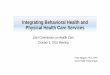
The Four Quadrant Clinical Integration Model For the Adult Population/ Heritage & CHIC Adaptation
Quadrant IIHigh Behavioral Health (BH)Low Physical Health (PH)Heritage is medical home. Care to be provided by or arranged by Heritage BH Counselor Criteria for placement in this quadrantMay have accessed services at CHIC or HBHEligible for 132 Services•Has low physical health risk/ complexityNeeds psychotropic medication provided by psychiatrist at HBHPhysical health care by PCP located at HBHMay have stigma issue about going to HeritageNeeds case management, housing, assistance with finances & or Heritage Payee servicesDual problems of S/A & MH (requires treatment for both)Inpatient Hospitalization in past or required now.Needs daily living skills trainingNeeds outreach services provided by HeritageActions to Be Taken :Clinician arranges case management services for housing and other community supportsArranges for S/A treatmentArranges for access to primary health care if enters @ HBH, and assures communication with Primary Care Physician (PCP)BH Clinician provides assessment, Psychiatrist provides and monitors needed medication
Quadrant IVHigh Behavioral Health (BH)High Physical Health (PH)Heritage is medical home with counseling and case management services provided at HeritageCriteria for placement in this quadrantAccesses services at Heritage in most casesPhysical health care by PCP located at HeritageEligible for 132 Services•Has complex and high risk physical problems, and requires regular physician visits, and or specialty physician care•Needs a BH case manager at HBH who provides assistance with housing, financial assistance•May have Dual problems of S/A and MH (requires treatment for both)•Needs inpatient hospitalization for either physical or mental health issuesActions to Be Taken:Primary Dr provides primary care and assures specialty physical health care when neededHeritage BH counselor assures collaboration between BH & PH BH clinician arranges for case management and other needed support servicesPsychiatrist provides and monitors needed medicationIf no Primary care physician at HBH, will receive primary care at CHIC
Quadrant ILow Behavioral HealthLow Physical HealthCHIC is medical home with on site CHIC BH clinicianCriteria For Placement in this quadrantMay have accessed services at CHIC or HBHLow physical health risk/complexitySlightly elevated health or BH riskClient may need BH and or S/A triage, assessment, and service planningBrief BH counseling or treatment or group therapyMay need referral to community and educational resourcesMay need health risk educationDrs only clients at HBH would be appropriate in this quadrantActions to Be Taken:PCP provides primary care and uses screening tools and guidelines to serve most individuals in Primary CareRefers to & collaborates with psychiatrist to assure coordinated careCHIC BH clinician provides formal and informal consultation to the PCPCHIC BH clinician provides brief counselingPsychiatric consultation provided to PCP if needed
Quadrant III High Physical Health Low Behavior HealthCHIC is medical home with on site CHIC BH clinician Criteria for Placement in this quadrantHas complex and high risk physical health problems, and requires regular physician visits, and or specialty physician careLow BH needs, but needs screening by PCP using screening tools May need BH triage or assessmentMay need consultation to the PCPMay need referral to community educational resourcesActions To Be Taken:•PCP provides primary care and assures specialty care when needed•PCP utilizes BH screening tools and guidelines to serve most individuals in Primary Care•BH clinician provides triage, assessment, & consultation with PCP

11
Integration Partnership - Expansion
The Administrative and Clinical Collaborative Committees continue to meet on the existing collaboration as well as expanding to additional behavioral health services on site at CHIC and with an intention of continuing to work towards the provision of primary health care in a behavioral health care setting. This project is the logical extension of efforts currently underway between Heritage and CHIC. Heritage and CHIC meet regularly to plan, coordinate, and implement our existing collaboration of integrating behavioral and primary health care. This collaboration is progressive and moving forward.
The MCMHB joined the Administrative Committee in late 2009 when we began a “pilot project” to add expertise, additional funds with Medicaid billing through them plus the matching local dollars.

12
Integration Partnership Background
Integration: Partnering Agencies 2011
The Community Health Improvement Center (CHIC), a primary health care center – Federally Qualified Health Center,
Heritage Behavioral Health Center (Heritage), a community behavioral health center – Mental Health, Substance Abuse, Homeless and Housing Services
The Macon County Mental Health Board (MCMHB), a public taxing body that funds MH/SA/DD services
The Macon County Health Department, public health department (MCHD)

13
Integration Partnership – Expansion TwoMacon County Health DepartmentMCHD entered into partnership with IDPA ABCD II
(Assuring Better Child Health and Development Initiative) project in 2005. State level partners included:
Illinois Chapter, American Academy of Pediatrics ( ICAAP) and Illinois Academy of Family Physicians
Ounce of Prevention Fund (OPF) Illinois Department of Human Services (IDHS) Office of Family Health (OFH) IDHS Office of Mental Health (OMH) Illinois Department of Children and Family Services Illinois Primary Health Care Association (IPHCA Local partners included: AOK Network FQHC: CHIC WIC/FCM Coordinator Pediatric/Family Practices: Early Intervention/CFC: Heritage Behavioral
I

14
Edinburgh Postnatal Depression Scale (EPDS)
Possible Depression is indicated at score of 10 or above. Referral provided for all scores of 10 or higher
INITIAL NUMBERS INDICATED HIGH RATE OF NEED !
Edinburgh’s Completed :
May 05 – September 05 = 434
Scores of 10 or higher = 100 Result=25% rate of at risk women in need of referral ! Current screening rates maintain average of 100 screens completed /month with 10-20%
rate of need for referral

15
Hopes & Screams from MCHDMCMHB Board Director enlisted local mental health providers to
provide counseling services for clients with positive screening scores
Referral rates outnumbered available resourcesMCMHB providers had long waiting times for client entrySome MCMHB providers were charging clients for services
against project agreement Some providers requested clients not be referred if in prenatal
stateSome OB providers declined to accept screening resultsMCHD staff expressed frustrations and concerns related to
referral inconsistencies

16
MCHD Request to MCMHB Fall 2010Invited MCMHB Director to Maternal Child Health staff meeting
to address staff concerns related to the counseling referral system
Staff relayed numbers of underserved clients
Gave examples of referral difficulties with MCMHB paid agencies
Requested on site services and to include home visits for clients with barriers such as daycare, transportation, work/school schedules
Goal= to achieve through partnership timely and adequate service delivery and follow up for at risk women and families

17
MCMHB Reasons for Involvement
New Medicaid by billing through the MCMHB – directly to DHFSLocal Funds Initiative - matching Medicaid with County dollars
means more money for the communityQuicker access to behavioral health servicesCaptive Audience at CHIC – linkage & need from MCHDEligibility – changes in eligibility over the years in mostly only target
population defined by DHS-OMH – this allows an Expansion of eligibility wider range of individuals than current and potentialStill meeting medically necessity
More holistic care - hopefully better clinical outcomes/people improving/getting better

18
Integration Partnership – Expansion Two Continued
Administrative Team established and meeting to work through challenges, barriers, referral processes, medical record – computer
Members from MCHD, MCMHB, Heritage
Clinical Teams also providing feedback through their supervisors – funnels up to Administrative Team and back to clinical teams/supervisors to smooth the processes

19
MCHD, “Happy Days Are Here!”
January 2011-Part time MCMHB funded Heritage Counselor begins accepting onsite referrals at MCHD and completing home visits.
40 referrals received in the first month! Whew!Initially ,frustration expressed regarding delayed contact
time vs referral numbers …However …Counselor provides assistance with multiple scenariosClients and staff express 100% satisfaction with follow up
services

20
Next Steps MCHD Expansion into Seniors
Plan to use Geriatric Depression Screen
One full-time mental health staff beginning July 2011 might expand to another part-time assigned to the MCHD clients/patients

21
Specific Changes Implemented in the Last Year
Lost the psychiatrist that worked so well for both organizations as a result have added Psychiatric Nurse Practitioner to FQHC
Added Mental Health Therapist to the FQHC site with MCMHC Board Funding
Screening to determine who can be better served at the FQHC as primary – Medical Home
Have received SAMHSA Integrated Primary Care Grant which will allow us to emphasize wellness with SPMI population added Physical PA on site at the Mental Health Center.
MCHD has become 2nd site funded by MCMHB for therapists to see identified by MCHD staff in need of services – primarily an outreach, in-home model though which is different than that at CHIC

22
Lessons Learned – things to Consider when establishing Collaborations for Integration of Care
Can take much more time to work through because our systems are often actually complicated
Are the right people at the table for discussions?Licensure of Sites – Scope of Practice ChangesWritten Agreements
Joint Contracts for purchasing of staff or servicesWho is billing for what?

23
SAMHSA Program Goals
Heritage Behavioral Health Center received a SAMHSA Grant in
September 2010 for its Primary and Behavioral Health Care
Integration (PBHCI) program. Our project focuses on:
individuals with Serious Mental Illness who are on antipsychotic medications and….
have co-occurring metabolic syndrome or a chronic medical condition
Establishment of a primary care clinic at Heritage Behavioral Health Center
Provision of wellness activities/programs Working with 500 SMI adults by the end of the 4th year

24
SAMHSA Program Goals
Health and Illness Background Information Used both as a screening and as a means of documenting
diagnoses (PH and BH) as well as important medical/health history variables SF-36 (short form)
Person Centered Healthcare Home Fidelity Scales and Protocols Developed by our evaluator, TriWest
Based on the conceptual work of Barbara Mauer and collaborators 2-day collaborative assessment process

25
Accomplishments
In 5 months, established a Health & Wellness Suite, including a Primary Care Office at Heritage
Contracted with CHIC Primary Care Clinic to place a Primary Care Physician/Assistant on site
Developed a Clinical Registry
Admitted 57 clients to Health and Wellness Program since Mid March 2011

26
Accomplishments
Received 87 referrals to the program since program began in February 2011
Success Stories: In one month, one client lost 20#, another lost 11#, a third
lost 14#. No one enrolled in the program has gained weight.
Two partially immobile clients are now mobile and
continuing to improve

27
Health and Wellness Activities
Food Pyramid Education weeklyHealthy Cooking Classes weeklyChair Zumba twice per weekModified Yoga weeklyDaily Walking ActivityHealthy Food Shopping As Needed1:1 Food Counseling and Review of Food Tracker as
neededWeekly Off Site Exercise

28
Plans for The Future
Expand hours and responsibilities of P/A to provide all primary care for individuals in the program
Provide fully certified smoking cessation classes to clients
Staff will become certified in smoking cessation, diabetes education, yoga, and zumba
Provide physical illness management education to case managers
Add Peer Support/Mentors to programWellness Model throughout organization

29
Key Contact Person(s) and Contact Information:
Julie Aubert, MCHD, [email protected] 217-423-6988 ext 1105
Barbara Dunn, CHIC, [email protected] 217-877-6111
Dennis Crowley, MCMHB, [email protected] 423-6199 X 108
Diana Knaebe, Heritage, [email protected]
217-420-4702
Karen Shiflett, MCHD, [email protected] 217-423-6988 ext 1343