Embed Size (px)
Citation preview

1Pharmacy Regulatory Updates and an Introduction to Specialty Pharmacy
Mark Atalla, PharmD

2Disclosure
• I have no relevant financial relationships with commercial interests pertaining to the content presented in this program

3Objectives
• 3 Key Things to Walk Away With:– Understand what Specialty Pharmacy means– Understand Regulatory Landscape for Sterile Compounding– Discuss Pedigree and FDA Track and Trace Requirements

4
Renal Specialty Pharmacy
Specialty Regulatory Tie-in
• Renal Therapy Management• Integrating care among clinics and patients to deliver health outcomes
• Focus on value added pharmacy services• Right dose, right time• Counseling• Adherence• Adverse events
Breakdown of the medicine value chain by stakeholder – IMS illustrative

5
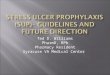
The Importance of Phosphate Management
*Urea Reduction RatioBlock GA et al. J Am Soc Nephrol 15: 2208-2218, 2004
Specialty Regulatory Tie-in

6
Renal Specialty Pharmacy
Specialty Regulatory Tie-in
Specific Goals of a Renal Specialty Pharmacy:• Create alignment with prescribers to improve medication compliance• Offer care and service to help our patients by providing convenient delivery
of medications in the most cost effective way• Be a valued resource to our staff to help improve patient outcomes
Breakdown of the medicine value chain by stakeholder – IMS illustrative

7
Renal Specialty Pharmacy
Specialty Regulatory Tie-in
• How to get there:• Clinical pharmacists that review lab values, compliance, and engage
patients• Pharmacists with certification in ESRD and co-morbidities• Focus on execution, collaboration, and experience
Breakdown of the medicine value chain by stakeholder – IMS illustrative

8
Specialty Pharmacy Overview
• Specialty Medications are:• CMS: medications that cost ≥$600 for a 30 day supply• Represent a limited number of drugs that are used by a small
proportion of beneficiaries • Have specific processing, handling, and administration requirements• May be a limited distribution network• Potential narrow, and narrowing, commercial networks
Alexion – Ultra-rare diseases
Specialty Regulatory Tie-in

9
Renal Specialty MedicationsIndication Medication Comments
Hyperphosphatemia Lanthanum carbonate (Fosrenol®)
Chewable or Powder
Hyperphosphatemia Sevelamer hydrochloride (Renagel®) -
Hyperphosphatemia Sucroferric oxyhydroxide (Velphoro®)
Chewable
Hyperphosphatemia Ferric citrate (Auryxia®) Potential increase in iron (ferritin)
Hyperphosphatemia Sevelamer carbonate (Renvela®)
Available in powder or tablet
Specialty Regulatory Tie-in

10
Renal Specialty MedicationsIndication Medication Comments
Anemia Darbepoetin alfa (Aranesp®)
Available in pre-filled syringes
Anemia Epoetin alfa(Epogen®)
Single and Multidose vials
Secondary hyperparathyroidism
Cinacalcet (Sensipar®)
Daily dosing – compliance is important
Specialty Regulatory Tie-in

11
Case Study
• ESRD patient with HIV • Common therapy for HIV is tenofovir (Viread)• Patient was taking Viread daily• Data and recommendations from manufacturer:
Intermittent hemodialysisTenofovir 300 mg PO every 7 days following routine dialysis; administer following completion of dialysis.
• Adverse reactions: hypertriglyceridemia, increased cholesterol, decreased bone mineral density, GI side effects
Key Take Away: Specialty pharmacies strive to deliver better outcomes through developing disease-state specific expertise
Specialty Regulatory Tie-in

12
Regulatory Environment
• Specialty pharmacies build expertise in specific disease states and the medications that affect those disease states
• The regulatory environment heavily governs pharmacy practice• State and Federal Regulations
• Three regulatory issues that affect practice and our patients:• CMS consent • Sterile Compounding• Pedigree and Track and Trace
Goal: Build awareness of the regulatory issues that impact pharmacy with leaders in ESRD care
Specialty Regulatory Tie-in

13
Patient Consent
• Automatic refills -> potential for waste• Patient complaints; consistent with decreasing fraud, waste, and
abuse• 2014 CMS – Part D sponsors to require pharmacies obtain patient
consent prior to each delivery • Goal: Decrease unintended waste, accumulation, costs
What does that mean for you or our patients?• Pharmacies must obtain patient consent prior to each delivery • Patients have a right to put a prescription on hold or refuse
treatment
Specialty Regulatory Tie-in

14
Sterile Compounding
• September 2012 – multistate outbreak of fungal meningitis• 751 patients affected in total, 25 in Florida (meningitis, stroke, spinal
infections)• 64 patients died, 7 in Florida
Previous Background• April 2002 – FDA issues Form 483 with findings• February 2003 – FDA issues Form 483 with findings
“…the potential for serious public health consequences if compounding practices are not improved…so long as a pharmacy’s operations fall within the scope of the practice of pharmacy, FDA will generally continue to defer to state authorities for regulatory oversight.”
• January 2007 – FDA Warning Letter• October 2012 – FDA Form 483
FDA New England Compounding Center: http://www.fda.gov/AboutFDA/CentersOffices/OfficeofGlobalRegulatoryOperationsandPolicy/ORA/ORAElectronicReadingRoom/ucm325828.htm
Specialty Regulatory Tie-in

15
FDA Guidance
• 2013 - Drug Quality and Security Act and Compounding Quality Act • Establishes 503B outsourcing facilities• Drugs must be compounded in compliance with cGMP
• 2013/2014 -• Section 503A –Requirements for exemption for licensed pharmacists or
licensed physicians compounding small quantities• Section 503B – outsourcing facilities – must follow current good
manufacturing practices• “Inordinate amounts of compounded drug products interstate”
Positive changes and guidance from the FDA to help guide sterile compounding
Specialty Regulatory Tie-in

16
State of Florida
• 2007 - Standards of practice for compounding sterile preparations• 2013/2014 – New Standards of Practice
• Adoption of USP Standards • Sterile Compounding Permit Required – in- and out-of-state
• Pharmacy inspections – new inspectors; significantly different form • Consultant pharmacist: provide guidance for Class IIb permit (eg. immediate
use, beyond-use dating)
Key Take Away: Significant Federal and State changes require that all pharmacies that supply CSPs must be permitted by the State of Florida and
follow USP or cGMP guidelines for sterile compounding
Specialty Regulatory Tie-in

17
Pedigree
• Counterfeit medications: Less than 1% in the US (WHO; FDA)• Proactive FDA approach – as specialty items increase, greater economic
incentives for counterfeiting
FDA - Counterfeit Version of Botox Found in the United States. http://www.fda.gov/Drugs/DrugSafety/ucm443217.htm
Specialty Regulatory Tie-in

18
Pedigree
• 2013 - Drug Supply Chain Security Act – Track and trace• Goal is building an electronic, interoperable system over next 10 years• Trading partners (manufacturers, wholesale distributors, and re-
packagers) provide transaction documentation to dispensers• Transaction information, transaction history, and transaction
statements • Trading partners maintain for ≥ 6 years after transaction
Key Take Away: The pharmaceutical supply chain is becoming more regulated with eventual greater transparency and tracking of medications
Specialty Regulatory Tie-in

19
Conclusions
• Pharmacies should be seen as a partner that can offer value added services for the patients we all treat
• Specialty Pharmacy refers to the clinical and practical expertise needed to dispense the range of medications that fit specific criteria
• Significant Federal and State changes require that all pharmacies that supply CSPs must be permitted by the State of Florida and follow USP or cGMP guidelines for sterile compounding
• The pharmaceutical supply chain is becoming more regulated with Track and Trace.
Specialty Regulatory Tie-in

20
Thank you