Embed Size (px)
Citation preview

1
Pediatric HIV Infection
HAIVNHarvard Medical School AIDS
Initiative in Vietnam

2
Learning Objectives
By the end of this session, participants should be able to:
Explain how to diagnose children with HIV
Describe WHO clinical staging for children
Explain when and how to initiate cotrimoxazole prophylaxis in children
List the 6 vaccines that are contraindicated in children with AIDS

3
Overview of Pediatric HIV
>90% of global pediatric HIV due to mother-to-child transmission (MTCT)• During pregnancy• During delivery
Most common time for infection
• After delivery Breastfeeding increases transmission risk by
5-20%

4
Overview of MTCT
What is the risk of transmission without intervention?
The overall MTCT rate is approximately 25-40% without intervention
However, with current prophylactic strategies, the risk of transmission can be reduced to less than 2%

5
Pregnancy 5-10%
Delivery 10-15%
Breastfeeding 5-20%
When Does MTCT Occur?
In an untreated breastfeeding population, the total transmission rate is 25-40%

6
Management of HIV-Exposed Infants and Children
Make diagnosis as soon as possible Give appropriate vaccines and
prophylaxis Start antiretroviral therapy when
indicated (for HIV-infected infants) Recognize and treat opportunistic
infections Support growth and development

7
Diagnosis of HIV Infection: > 18 Months
Confirmed by the same HIV antibody test used for adults
HIV infection is diagnosed when the serum gives 3 positive results in 3 tests with 3 different bioproducts
Only laboratories certified by MoH are authorized to confirm HIV positive test results before reporting
the result to patients
Guidelines for the Diagnosis and Treatment of HIV/AIDS. Ministry of Health, 2009.

8
Diagnosis of HIV Infection: < 18 months (1)
Because an infant up to 18 months of age may carry maternal HIV antibodies, regular HIV antibody test will be positive whether baby has HIV or not• Test will either be detecting baby’s
antibodies or mother’s• This leads to difficulties interpreting an
HIV antibody positive test result in children < 18 months

9
Diagnosis of HIV Infection: < 18 months (2)
Diagnosis is based on PCR for viral DNA or RNA• < 9 months: 2 positive PCR (performed
after 4-6 weeks of life)• 9 to 18 months: if HIV antibody test is
positive then need PCR to confirm (as for < 9 month old)
If breastfeeding, stop for 6-8 weeks before testing
Guidelines for the Diagnosis and Treatment of HIV/AIDS. Ministry of Health, 2009.

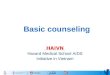
MOH 2009HIV exposed children(<9 months old)
PCR testingPCR testing not
available
PCR positive
PCR negative
No HIV infection
Breastfed within 6 weeks of PCR test?
Repeat PCR 6 weeks after last breastfeeding
Continued Care at HIV outpatient
clinic
2nd PCR
HIV infection confirmed
HIV antibody test at 18 months
NO
YES
POS
NEG
POS
NEG
HIV Diagnosis for HIV Exposed
Children <9 months

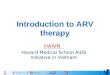
AntibodyAntibody
testingtesting
Antibody Antibody testing (+)testing (+)
AntibodyAntibody
testingtesting (-)(-)
PCRPCR testingtesting(as < 9 months (as < 9 months
old) old)
HIV exposed children(9-18 months old)
MOH 2009
NoNo HIVHIV infectioninfection
HIV Diagnosis for HIV
Exposed Children 9-18 months old

12
Clinical Diagnosis of Severe HIV/AIDS Disease in < 18 months
Stage 4 clinical disease • PCP• Toxoplasmosis• Cryptococcus• Wasting syndrome• Esophageal
candidiasis• EPTB (excluding
axillary LN – BCG disease)
At least 2 of the 3 findings:• Oral thrush (if >
1 month of age)• Severe bacterial
pneumonia• Severe sepsis
HIV Antibody test positive, plus:
OR

13
Staging of Pediatric HIV Infection

14
WHO Pediatric Clinical Staging
Clinical staging should be performed for infants and children with confirmed HIV infection
If HIV infection cannot be confirmed in infants <18 months, a presumptive diagnosis may be made in those with severe disease
Accurate staging is important for deciding when to start ART

15
WHO Pediatric Stages (1)
Stage 1 Child is asymptomatic May have persistent
generalized lymphadenopathy
Stage 2
Characterized by: Hepatosplenomegaly Recurrent or chronic
upper respiratory tract infections
Papular pruritic eruption
Herpes zoster

Linear gingival erythema
Stage 2 Diseases (1)
Zona

PPE: lower arms and legs, leaves scarring
after resolution
Stage 2 Diseases (2)

Bilateral parotid enlargement
Stage 2 Diseases (3)

19
WHO Pediatric Stages (2)
Stage 3
Characterized by: Unexplained moderate
malnutrition Unexplained diarrhea
>14 days Unexplained fever for
>1 month Pulmonary, lymph
node TB
Stage 4
Characterized by: Unexplained severe
wasting/malnutrition PCP Recurrent severe
bacterial infection Extrapulmonary TB HIV encephalopathy

Oral hairy leukoplakia:Side of tongue, can’t scrape off
Stage 3 Diseases (1)
Oral candidiasis

Stage 3 Diseases (2)
Pulmonary TB TB Lymphadenitis

22Lymphocytic interstitial pneumonitis:
Typical nodular infiltrates in mid and lower lungs
Stage 3 Diseases (3)

Stage 4 Diseases (1)
Herpes Simplex chronic infection (>1 month)

Penicillium Marneffei skin lesions:Flesh-color, umbilicated papules concentrating mainly on face
Stage 4 Diseases (2)

Quiz: Which stage?
Scenarios Stage ?
A 5 year old boy who has:•had an unexplained fever for over a month now•and also has a skin rash consistent with papular pruritic eruption (PPE)
A 1 year old girl who has TB meningitis
A 7 year old boy who with generalized lymphadenopathy but otherwise appears well with no other symptoms
3
4
1

26
Immunological Staging (1)
The degree of immunosuppression in HIV infected children is assessed by the percentage (%) of CD4 cells
CD4 percentage is used for children under 5 years of age, whereas CD4 number is used for children 5 years and older

27
Immunological Staging (2)
<11 months
12-35 months
36-59 months
≥ 5 yrs
Not significant
> 35% > 30% > 25% > 500 cells
Mild 30 – 35%
25 – 30%
20 – 25% 350−499 cells
Advanced 25 – 29%
20−24% 15−20% 200−349 cells
Severe <25%<1500 cells
<20%<750 cells
<15%<350 cells
<15% <200 cells

28
Overview on Care and Treatment of Children
with HIV/AIDS

29
Cotrimoxazole Prophylaxis for HIV-Exposed and -Infected Children
HIV-exposed children
Confirmed HIV-infected children
•Start 4–6 weeks after birth•Continue until exclusion of HIV infection
< 24 months
24 – 60 months > 60 months
All
Clinical stages 2, 3 and 4 regardless of CD4 count orCD4 < 25% or ≤ 750 cells/mm3 regardless of clinical stage
Clinical stage 3 or 4 regardless of CD4 count or CD4 ≤ 350 regardless of clinical stage

30
Immunization Children with HIV and C.S 4 should not be given live vaccines
Vaccine HIV-exposed infants, before diagnosis is known
HIV + with clinical stages I, II, III
HIV + with clinical stage IV
• Nationally-supported vaccines
BCG As scheduled DO NOT GIVE DO NOT GIVE
DPT As scheduled As scheduled As scheduled
Poliomyelitis oral
As scheduled As scheduled IM vaccine only
Hepatitis B As scheduled As scheduled As scheduled
Measles As scheduled As scheduled DO NOT GIVE
JE As scheduled As scheduled As scheduled
• Optional vaccines
HIB As scheduled As scheduled As scheduled
Varicella As scheduled As scheduled DO NOT GIVE
Mumps As scheduled As scheduled DO NOT GIVE
Rubella As scheduled As scheduled DO NOT GIVE

31
ARV Indications
Children with confirmed HIV infection:
Age Starting ART
< 24 monthsStart ART as soon as possible
(regardless of clinical stage or CD4)
24 - 60 months
Clinical stage 3 or 4 regardless of CD4 count
CD4% ≤ 25% or CD4 ≤ 750 cells/mm3 regardless of clinical stage
> 60 months Indications as per HIV-infected adults

32
Common Opportunistic Infections in HIV-infected
Children

33
Pneumocystis carinii Pneumonia (PCP)
Most common OI in young children
Interstitial, diffuse pneumonia
Characterized by:• Fever• Cough• Progressive dyspnea• Tachypnea• Hypoxia
Peaks at 2-8 months of age
Infant mortality after treatment up to 40%

34
AIDS-Defining Conditions by Age at Diagnosis for Perinatally-Acquired AIDS Cases
Reported through 1999, United States
Age in Months
Nu
mb
er
of
Cases
0
0
50
100
150
200
250
300
350
400
450
2 4 6 8 10 12 14 16 18 20 22 24
Other AIDS-defining
conditions
Pneumocystis jiroveci pneumonia

35
Tuberculosis
Diagnosis of TB in children in VN• High index of suspicion needed• Suspect in any child with prolonged cough,
low grade fevers, failure to thrive• BK smear, PPD (tuberculin skin test), CXR• Gastric aspirates used in small infants• Look for LN, peripheral and mediastinal• FNA to evaluate for lymph node infection
Differential Diagnosis: Lymphoid interstitial pneumonia, PCP, bacterial pneumonia

36
Support for Growth and Development
Growth High rates of growth
failure due to decreased intake and/or increased nutrient demands• Give multivitamins
containing Vitamin A• Treat iron-deficiency
anemia• Maximize caloric intake
Development Watch for spastic
limbs and gait, encephalopathy, other neurological deficits
Review developmental milestones
Delay or loss of developmental milestones indicate HIV encephalopathy

37
Key Points
Most children get HIV through mother-to child transmission• Children > 18 months are tested with
antibody test• Younger children may still carry mother’s
antibodies, need different testing strategy Use clinical and immunological staging
to determine ART eligibility Important to look closely at child’s
growth and development markers for clues about health

38
Thank you!
Questions?