1 Operationalizing Peer Support through the Lens of Family Driven Care and Motivational Interviewing...
51
1 Operationalizing Peer Support through the Lens of Family Driven Care and Motivational Interviewing One hospital’s journey to implement Peer support on an inpatient behavioral health unit National Presentation for Families with Mental Illness, 2014 Kendra Crookston, LPCC-S, Coordinator of Parent Partners Regina Saunders, Parent Partner
1 Operationalizing Peer Support through the Lens of Family Driven Care and Motivational Interviewing One hospital’s journey to implement Peer support on
1 Operationalizing Peer Support through the Lens of Family
Driven Care and Motivational Interviewing One hospitals journey to
implement Peer support on an inpatient behavioral health unit
National Presentation for Families with Mental Illness, 2014 Kendra
Crookston, LPCC-S, Coordinator of Parent Partners Regina Saunders,
Parent Partner
Slide 2
2 Agenda Peer support Hospital System Family Driven Care
Motivational Interviewing Identifying stages of Change in
Caregivers HCIA background Parent Partner Case Manager Outcomes
Parent Partner Experience Questions
Slide 3
3 Aids in reducing stigma and isolation Promotes confidence and
hope while activating strengths Why Peer support?
Slide 4
4 Primary Goal= Provide support to parents and families coping
with children with behavioral problems. Secondary goals include
empower parent s in decision making normalize parent experience
educate on coping, self care, and crisis management assist parent
in identifying their own needs and concerns Integration of Peer
Support into a Hospital System
Slide 5
5 Family Driven Care is Treatment is individualized to the
specific patient and family Culturally competent and engaging
Builds knowledge and skills Solution focused Promotes advocacy from
caregiver to provider
Slide 6
6 Match to family ability and desired treatment Increased
likelihood that families will follow through with treatment
recommendations Improved outcomes and reduction in reuse of
emergent services Assures family voice is valued Assures that
family choice is identified Provides individualized support to
caregivers Why Employ Family Driven Care in a Pediatric Hospital
Setting?
Slide 7
7 Motivational interviewing (MI) is a person-centered, guiding
method of communication and counseling to elicit and strengthen
motivation for change Motivational Interviewing 2 nd Edition,
Miller & Rollnick, 2002, Guilford Press INTRODUCTION TO
MOTIVATIONAL INTERVIEWING
Slide 8
8 What is Motivational Interviewing (MI)? MI is a particular
kind of conversation about change (counseling, therapy,
consultation, method of communication) MI is collaborative
(person-- centered, partnership, honors autonomy, not expert--
recipient) MI is evocative (seeks to call forth the persons own
motivation and commitment) Motivational Interviewing is a
collaborative conversation to strengthen a persons own motivation
for and commitment to change. Rollnick S., & Miller, W.R.
(1995). What is motivational interviewing? Behavioural and
Cognitive Psychotherapy, 23, 325-334
Slide 9
9 Motivational Interviewing Techniques Used in Peer Support Ask
open ended questions Affirm person by shedding light on strengths
they have identified Reflect persons meaning and feeling Summarize
what you have heard from a Caregiver Focus on collaboration,
evocation, compassion and accepting of others. Focus on Caregiver
ambivalence
Slide 10
10 Using the Stages of Change Model to Assess for Parental
Readiness Not every parent is experiencing the same level of
readiness for treatment recommendations Importance of assessing
Parents for their specific ability to process information given by
clinicians Treatment recommendations are tailored to Parents
abilities
Slide 11
11 Precontemplation is the state in which people are not
considering changing or initiating a behavior. They may be unaware
that a problem exists. Contemplation is the stage characterized by
ambivalence about changing or initiating a behavior Preparation is
the stage characterized by reduced ambivalence and exploration of
options for change. Action is the stage characterized by the taking
of action in order to achieve change. Maintenance is the stage
characterized by seeking to integrate and maintain a behavior that
has been successfully changed or initiated. Relapse is the stage
characterized by a recurrence of the undesired behavior or
elimination of a desired behavior. (Prochaska and DiClemente, 1986,
1992) Stages of Change Model
Slide 12
12 HOW THE PROJECT WAS DEVELOPED, I.E., INTRODUCING PEER
SUPPORT IN A PEDIATRIC HOSPITAL SETTING
Slide 13
13 Akron Childrens Hospital received a 3-year, $13.3M
collaborative award with Nationwide Childrens Hospital Reduce COST:
prevent readmissions to the inpatient behavioral health unit
Improve CARE: provide family-driven care and parent
support/increase adherence to follow up mental health care Improve
HEALTH: support parents as they identify a reduction in their
childs negative behaviors Healthcare Innovation Award (HCIA)
Centers for Medicare and Medicaid Innovation June 2012- June
2015
Slide 14
14 CURRENT USE OF PARENT PARTNERS AND CASE MANAGER
Slide 15
15 Parent Partner A person with experience navigating the
mental health system with his/her own child Applied Peer Support
Provides a framework to parents for what to expect for a childs
admission to the inpatient Behavioral Health Unit 99% of families
accept the support of a Parent Partner when offered. Bridges the
gap between providers treatment recommendations and familys
willingness to follow through
Slide 16
16 Parent Partner A person with experience navigating the
mental health system with his/her own child Applied Peer Support
Continued.. Acts as a liaison between the clinician and family to
effectively tailor treatment planning Collaborates with clinical
staff to identify caregivers experience of the crisis Reinforces
family-driven care practices by viewing the family as
capable/expert Allows families to identify their own needs and
influence decisions regarding their childs care
Slide 17
17 Parent Partner family interaction
Slide 18
18 Parent Partners support, empower and activate
parents/caregivers at different touch points Parent Partner
Activities
Slide 19
19 Triage and assist families in need of services Assess for
fit of current services Remains with family until patient/family
engages in agreed upon services Introduction of a Case Manager into
the Peer Support System
Slide 20
20 The Case Manager Contacts each family: following discharge
prior to their first-follow up appointment after their first mental
health follow up visit Works intensively with Parent
Partner-identified, high acuity families to reduce barriers to
treatment ** Note: Limited to families receiving Medicaid based on
grant parameters
Slide 21
21 Case Manager (Continued)
Slide 22
22 OUTCOMES
Slide 23
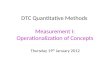
23 Mission: To decrease the incidence of avoidable inpatient
readmissions AIM Our goal is that 10% or less of our patients will
be readmitted within 60 days of their initial AIM Our goal is that
10% or less of our patients will be readmitted within 60 days of
their initial OUTCOME Our average re- admission rate over the last
12 months is 5.1%. This is a 50% reduction in readmissions to the
inpatient behavioral health unit.* OUTCOME Our average re-
admission rate over the last 12 months is 5.1%. This is a 50%
reduction in readmissions to the inpatient behavioral health unit.*
*Data reflects ACH data only
Slide 24
24 Readmission Rates Start of PP Intervention *Data reflects
ACH data only
Slide 25
25 Decreased Emergency Services Used Has the Parent Partner
Program contributed to a decrease of patients coming to PIRC after
their behavioral health inpatient discharge? 20112014% Change IP
Admissions (February-April)241263 Patients who came to PIRC after
IP discharge2212-45.5% % of patients who came to PIRC after IP
discharge9%5%-50.0% Data notes: 2014 data is available through Aug
16 th. Therefore, for 2011, a cutoff of August 16 th was also used
for PIRC returns. Some patients may have returned to PIRC more than
once, but only counted 1 visit (unique by patient) Includes all
payors Source system: Strata (with previous ADS and PIRC tracking
spreadsheet verification)
Slide 26
26 Inclusion in huddle process in multidisciplinary team rounds
Participation in unit transformation meetings to provide family
perspective Inclusion of Parent Partner in transitioning patients
from the Emergency Room to Inpatient Increased understanding of
parent perspective and challenges among all staff Request from
consult psychiatrist seeing patients on medical floors who will be
admitted to the inpatient behavioral health unit Integration of PP
into a Behavioral Health Inpatient Unit
Slide 27
27 Program Successes Inpatient Behavioral Health unit staff
comments: Parent Partners change the whole dynamic of comfort and
care. Not only does the patient feel satisfied but the families
feel confident and taken care of. (Survey Monkey of Inpatient staff
feedback) We cant imagine life without Parent Partners. (Inpatient
leadership) Many parents gave unsolicited positive feedback about
the care they received from the Parent Partners (Press Ganey survey
administered at time of discharge from Inpatient Behavioral Health
Unit)
Slide 28
28 Comments made by clinicians..
Slide 29
29 Program Volume Month Unique HCIA Program Participants Total
Touches September 2013169272 October 2013186304 November 2013153264
December 2013181270 January 2014157249 February 2014134194 March
2014135223 April 2014102177 May 201477119 June 201486176 July
201488141 August 201497178 Total1,5652,567
Slide 30
30 OUTCOMES: Vignette
Slide 31
31 Parent Partners and the Case Manager are an integral part of
the treatment team Parents easily build rapport with someone who
has had a shared experience Lack of program orientation to
non-grant staff Ever changing process requiring support and
collaboration Transition for Parent Partner staff into hospital
culture Parent Partners may need to take time off to support their
own childrens ongoing mental health needs Lessons Learned
Slide 32
32 HCIA grant dollars have provided the impetus for developing
a new model of care (Parent Partners), in preparation for an
Accountable Care model. ACH and Nationwide are the only two
hospitals in U.S. to implement peer support in a behavioral health
inpatient unit As risk is assumed, Parent Partners continue to be a
preventative intervention Well-trained, highly competent staff have
been hired/and trained, ready to provide family driven care (little
start-up cost) The Future As An Accountable Care Organization
Slide 33
33 Parent Partner/Case Manager Intervention has decreased the
readmission rate on 8100 by 50% Parent Partner/Case Manager
intervention in (PIRC) emergency service use has decreased by 50%
since the intervention Caregivers of children who suffer from
mental health issues are seen more regularly as expert and as
capable Abstract accepted by the National Federation of Families
for Childrens Mental Health 2014 conference, Washington, D.C.,
November, 2014, presentation Operationalizing Peer Support through
the Lens of Family Driven Care and Motivational Interviewing
Accomplishments
Slide 34
34 The Parent Partner Perspective
Slide 35
35 Being the Parent, the Professional and the lost. As if being
a mother wasnt enough I became the mother of a child with mental
illness. I began my journey working on the flip side of the coin,
not realizing how much I did not know. Now what were the things I
needed to know? Parent Partner Experience
Slide 36
36 Working As A Professional Having worked in Crisis
Intervention, I was trained and ready to help any where and any
time. I wanted to help and I am sure that given the opportunity I
can fix this for you. I am a professional fixer.
Slide 37
37 My Experience Parenting I realized that my child was
struggling What I began to notice in my own home, in my own child.
Am I truly being heard? But I am her mother, I am expert in my
child.
Slide 38
38 Watching My Child Be Admitted To An Inpatient Behavioral
Health Unit I was not prepared to have a child admitted to a mental
health unit. However, I believed the professionals such as myself
would wave the Magic Mental Health Wand and heal my child! I soon
learned that my journey was just in its infancy and I needed to
become my child's biggest advocate.
Slide 39
39 Things I did not know, that I did not know. How can I help
the professionals to understand my child. I am her mother and I am
a professional why am I not being understood? (what language was
missing between myself and the professionals?)
Slide 40
40 A Family Meeting On the Inpatient Behavioral Health Unit Now
we are getting somewhere! Today when I arrive, all of the
Professionals are prepared to help me with the child I am expert
on.
Slide 41
41 Learning the Nuances of Behavioral Health Jargon They said
it was a Family Session, Was this for my family or someone
else's?
Slide 42
42 Unanswered Questions Following My Childs Inpatient Admission
I had several questions and few answers They were very kind but
that did not help me to fix the way I was feeling. What did I
miss?
Slide 43
43 Okay, calling all of my IN NETWORK Professionals I decided
to talk with friends in the field. Was it helpful? I then thought I
would call other persons in the field that may help my child on an
outpatient basis. They will definitely understand me! Outcome
Slide 44
44 Myself the Helper, Professional and Know it All! I worked as
a Crisis Interventionist during this period of time. I am certain I
helped 90% of them, or did I ?
Slide 45
45 Fast-forwarding to Parent Partnership What is this Parent
Partner I hear of? Having been a Helper for many years I am certain
I can do this job. All I have to do is give these Parents my expert
advice, and my work is done, right?
Slide 46
46 Exploring the Parent Partner Job Opportunity I did not know
what I thought I knew about the position of a Parent Partner. I
learned much this day, and felt honored to even be considered for
my slight understanding of what this program could be.
Slide 47
47 Being Hired as a Parent Partner We definitely had our work
cut out for us.
Slide 48
48 A New Way of Thinking I began to hear many new words buzzing
about our trainings, conferences and meetings. Many new Ideas and
smart thoughts began to show themselves. We began to fumigate our
minds, replacing Professional think with memories of being the
parent of a mentally ill child only!
Slide 49
49 Setting the Parent Partner Program in Motion I was mentally
unprepared to handle what it would mean to bring a totally family
driven approach to the Medical Model method. Mama said there would
be days like this!
Slide 50
50 Parent Partners, We came, We learned, We conquered! What it
means to me to be a part of this movement. What I have learned by
helping to pioneer Parent Partnership. How we have maneuvered
collaboration with those holding fast to Medical Model Practice.
And what value we possess as Parent Partners in collaboration with
Parents.
Slide 51
51 In Closing, Smart Thoughts and Question Session Any
Questions or Comments Welcome at this Time. Lessons