Embed Size (px)
Citation preview

1
not-for-profitnot-for-profithttp://www.hwbf.orghttp://www.hwbf.org1313thth Annual Meeting Annual Meeting
McCormick Place E266McCormick Place E266Chicago, ILChicago, IL
March 23, 2005March 23, 2005
AGENDAAGENDA
Hippocrates, Winslow & Hippocrates, Winslow & Babbage HWB Babbage HWB
FoundationFoundationRichard Ghillani, M.D.Bradford Henley, M.D.David Karges, D.O.Henry Mankin, M.D.
Jeffrey Mast, M.D.Augusto Sarmiento, M.D.Marc Swiontkowski, M.D.Edward Yang, M.D.
Annual ReportAnnual Report Data CollectionData Collection Educational ArchivesEducational Archives MeetingsMeetings By-LawsBy-Laws CertificationCertification

2
Registries - Why?Registries - Why?
"Maintenance of an active registry "Maintenance of an active registry must be viewed as important as the must be viewed as important as the medical care rendered, if the right medical care rendered, if the right person is going to receive the right person is going to receive the right treatment in a timely fashion without treatment in a timely fashion without undue cost to society.“undue cost to society.“
Gillot et al, Development of a Statewide Gillot et al, Development of a Statewide Trauma Registry, J Trauma 29:1667, Trauma Registry, J Trauma 29:1667, 19891989

3
Registries - Why?Registries - Why?
““It is our professional responsibility It is our professional responsibility to try to continuously improve our to try to continuously improve our performance, which cannot be performance, which cannot be done without the collection of end done without the collection of end result information.“result information.“
Swiontkowski M, Why we should Swiontkowski M, Why we should collect outcomes data, JBJS 35A collect outcomes data, JBJS 35A Supplement 1:14 2003Supplement 1:14 2003

4
Data QualityData QualityPolitical FactorsPolitical Factors
Health Info Tech SuccessHealth Info Tech Success 80% dependent on political 80% dependent on political
factors factors 20% dependent on info 20% dependent on info
technologytechnology
Reed Gardner 1998 Reed Gardner 1998 Past President of AMIAPast President of AMIA
5
Data Collection - Why?Data Collection - Why?
"The future belongs to whoever best "The future belongs to whoever best measures quality of care and then measures quality of care and then markets it best. markets it best.
Whoever does will absolutely Whoever does will absolutely control the market, and everyone control the market, and everyone who doesn't will disappear."who doesn't will disappear."
Richard L. Scott, Esq, former CEO Richard L. Scott, Esq, former CEO Columbia/HCA HealthCare Corp.Columbia/HCA HealthCare Corp.
6
Data Collection - Why?Data Collection - Why?
"Tens of millions of dollars have been spent in "Tens of millions of dollars have been spent in the establishment of trauma databases over the establishment of trauma databases over the past 15 years. Much data is gleaned from the past 15 years. Much data is gleaned from ICD entriesICD entries into administrative databases. into administrative databases.
The emphasis here is for maximum The emphasis here is for maximum reimbursement. Because of the reimbursement. Because of the lack of lack of clinical detailclinical detail the data within these the data within these registries, the data is inadequate for registries, the data is inadequate for sophisticated research and outcome analysis. sophisticated research and outcome analysis. ""
Cushing, Champion - J TRAUMA 1995 Cushing, Champion - J TRAUMA 1995

7
Open Tibia Fracture = Open Tibia Fracture = ICD 823.3ICD 823.3
==
8
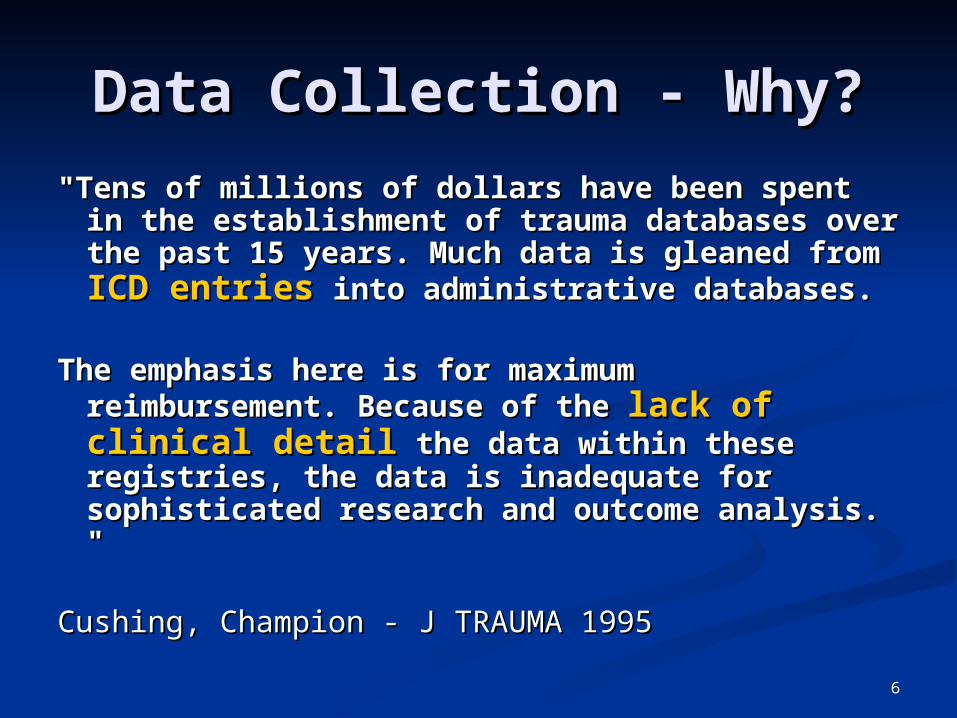
Practice ProfilingPractice Profiling
Pennsylvania Health Care Cost CPennsylvania Health Care Cost Containment Council ontainment Council
Maine Quality ForumMaine Quality ForumMedicare Hospital Quality InitiatMedicare Hospital Quality Initiativeive
Data Collection – by Data Collection – by DefaultDefault

9
Data Collection Data Collection – How?– How?UMC – HOSPITAL Records
Vanderbilt Medical Center 13,199Elmhurst Hospital Center 10,886Bellevue Hospital Center 6983Detroit Receiving Hospital 6636Hartford Hospital 4262Hennepin County Med Ctr 1043Norfolk & Norwich (UK) 633Southern Illinois University 456Denver General Hospital 450MIEMSS 168University of Geneva 46Rhode Island Hospital 0Maricopa County Hospital 0Grady Memorial 0Henry Ford Hospital 0
TOTAL 44,762

10
Data Collection – How?Data Collection – How?HWB Shortfall – Not UniqueHWB Shortfall – Not Unique
Electronic Medical RecordElectronic Medical Record - a - a cresting wave for 30 years - has cresting wave for 30 years - has not broken.not broken.
10% adoption10% adoption - Berner et al, - Berner et al,
JAMIA Feb 2005JAMIA Feb 2005 Katsushika Hokusai
wood engraving
"The Great Wave off Kanagawa"
- cerca 1830
11
Data Collection – How?Data Collection – How?President Bush – State of President Bush – State of
the Unionthe UnionProposes all Americans have an Proposes all Americans have an
EMR in 10 years to prevent EMR in 10 years to prevent medical errors and needless medical errors and needless costs.costs.
Spend $125 million Spend $125 million to get the job done. to get the job done.
http://www.jibjab.comhttp://www.jibjab.com
12
Data Collection – Failure - Data Collection – Failure - Causes Causes
JAMIA Feb 2005JAMIA Feb 2005
EMR Problems:EMR Problems:Malaligned IncentivesMalaligned IncentivesProduct ViabilityProduct ViabilityData QualityData QualityStandards - InteroperabilityStandards - Interoperability
13
Data Collection – Failure - Data Collection – Failure - Causes Causes
JAMIA Feb 2005JAMIA Feb 2005 Malaligned IncentivesMalaligned Incentives
Minimal Return On Investment Minimal Return On Investment with with
Information vs Imaging Information vs Imaging technology.technology.
CT study billable - not EMR data.CT study billable - not EMR data.

14
Malaligned Incentives - Malaligned Incentives - RxRxIndirect ReductionIndirect Reduction
through Practice Management through Practice Management Integration Integration
BillingBilling ReportingReporting SchedulingScheduling TranscriptionTranscription ArchivingArchiving
Data Collection – Failure - Data Collection – Failure - Causes Causes
JAMIA Feb 2005JAMIA Feb 2005

15
Malaligned Incentives – Malaligned Incentives – Rx Rx
Indirect ReductionIndirect Reduction
through facilitation of:through facilitation of:
Risk Adjusted Practice ProfilingRisk Adjusted Practice Profiling Error Checking - Liability ReductionError Checking - Liability Reduction RRC CertificationRRC Certification Academic PromotionAcademic Promotion
Data Collection – Failure - Data Collection – Failure - Causes Causes
JAMIA Feb 2005JAMIA Feb 2005

16
Data Collection – Failure - Data Collection – Failure - CausesCauses
Leape, Massachusetts Plan, NPR Leape, Massachusetts Plan, NPR 02/04/0502/04/05Malaligned Incentives – RxMalaligned Incentives – Rx
33rdrd Party Payors to purchase MD EMR. Party Payors to purchase MD EMR.
EMR Cost @ $35,000/MD (EMR Cost @ $35,000/MD ($800 million$800 million))
33rdrd Party Savings ( Party Savings ($ 5 billion$ 5 billion) through:) through:
fewer errors and complicationsfewer errors and complications fewer inappropriate testsfewer inappropriate tests fewer inappropriate medsfewer inappropriate meds fewer billing errorsfewer billing errors
17
Data Collection – Failure - Data Collection – Failure - Causes Causes
JAMIA Feb 2005 JAMIA Feb 2005
EMR Problems:EMR Problems:MalalignedMalaligned IncentivesIncentivesProduct ViabilityProduct ViabilityData QualityData QualityStandards - InteroperabilityStandards - Interoperability
18
Database Production and Database Production and
MaintenanceMaintenance Engh et al. CORR 421 April 2004Engh et al. CORR 421 April 2004
Product ViabilityProduct Viability19771977
Starts porous coated THA stem. Starts porous coated THA stem.
Seeks documentation of outcomes. Seeks documentation of outcomes.
Data stored on paper forms in a Data stored on paper forms in a physical chart.physical chart.

19
Database Production and Database Production and
MaintenanceMaintenance Engh et al. CORR 421 April 2004 Engh et al. CORR 421 April 2004
Product ViabilityProduct Viability1983 – 19921983 – 1992
Starts electronic archiving - 1 data Starts electronic archiving - 1 data entry personentry person
dBASE II (Ashton-Tate)dBASE II (Ashton-Tate) dBASE IIIdBASE III dBASE IVdBASE IV

20
Database Production and Database Production and
MaintenanceMaintenance Engh et al. CORR 421 April 2004 Engh et al. CORR 421 April 2004
Product ViabilityProduct ViabilityEarly 1990'sEarly 1990's
Need:Need:
Automated data entry Automated data entry
Standardized classifications and Standardized classifications and outcomesoutcomes
dBASE IV to International dBASE IV to International Documentation and Evaluation Documentation and Evaluation System (IDES) migrationSystem (IDES) migration
21
Database Production and Database Production and
MaintenanceMaintenance Engh et al. CORR 421 April 2004 Engh et al. CORR 421 April 2004
Product ViabilityProduct Viability Mid 1990'sMid 1990's
IDES does not allowIDES does not allow local modification.local modification.
IDES to FoxPro 2.6 migration withIDES to FoxPro 2.6 migration with Customized scanable forms. Customized scanable forms. Codes for a comprehensive Orthopedic Codes for a comprehensive Orthopedic
Research Database (ORDB)Research Database (ORDB) Third-party applications to facilitate Third-party applications to facilitate
data entry, maintenance, and report data entry, maintenance, and report generation.generation.

22
Database Production and Database Production and
MaintenanceMaintenance Engh et al. CORR 421 April 2004Engh et al. CORR 421 April 2004
Product ViabilityProduct Viability2004200433rdrd party apps party apps not compatiblenot compatible with new with new
FoxProFoxProFoxPro 2.6 FoxPro 2.6 no longer supportedno longer supported by Microsoft by Microsoft FoxPro 2.6 FoxPro 2.6 not compatiblenot compatible with Windows XP. with Windows XP.
Database Database not reflecting contemporarynot reflecting contemporary clinical concernsclinical concerns
Currently migrating to another database Currently migrating to another database application.application.

23
Database Production and Database Production and
MaintenanceMaintenance Engh et al. CORR 421 April 2004Engh et al. CORR 421 April 2004
Product ViabilityProduct ViabilitySummary:Summary:
7 major database changes in 21 years 7 major database changes in 21 years associated data corruption/lossassociated data corruption/loss
$50,000 - estimated annual data entry $50,000 - estimated annual data entry & maintenance cost ( does not include & maintenance cost ( does not include the surgeons’ time). the surgeons’ time).
New upgrades will substantially New upgrades will substantially increase annual cost.increase annual cost.
Consider Consider saving the papersaving the paper..

24
Database Production and Database Production and
MaintenanceMaintenance HWB Experience – Software Changes in 12 yearsHWB Experience – Software Changes in 12 years
Product ViabilityProduct Viability 5 major database changes in 12 years 5 major database changes in 12 years
Hypercard 1.0Hypercard 1.0 Fox Pro 2.5 Fox Pro 2.5 Visual Fox Pro 3.0Visual Fox Pro 3.0 FileMaker ProFileMaker Pro MySQL & PHPMySQL & PHP
4 major front-end changes in 12 years 4 major front-end changes in 12 years Hypercard 1.0Hypercard 1.0 Hypercard 2.0Hypercard 2.0 Metacard 2.5Metacard 2.5 HTMLHTML
25
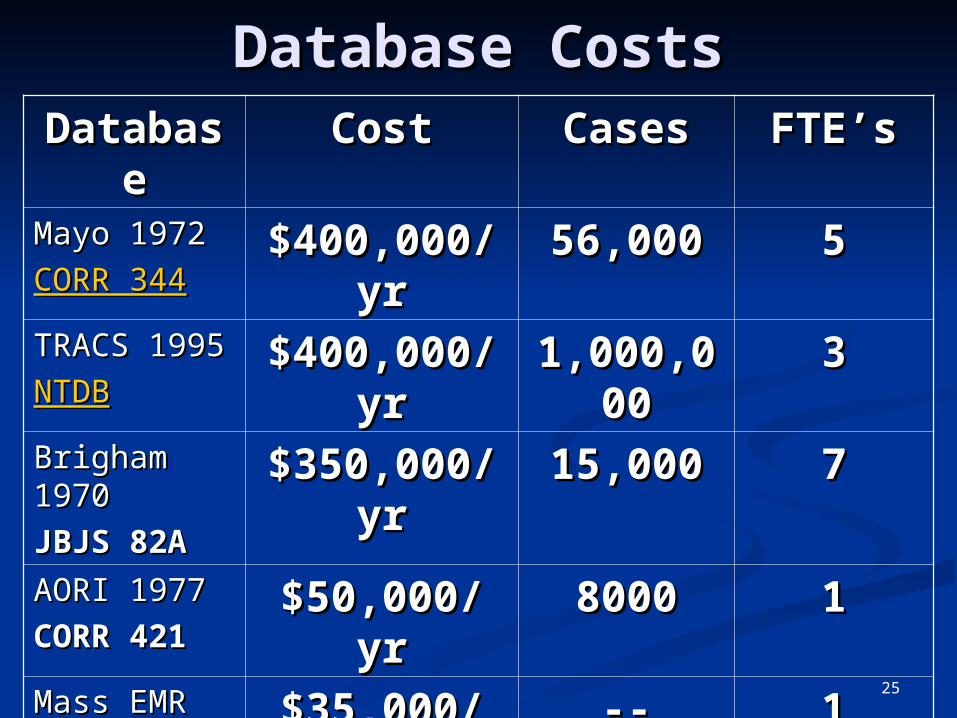
Database CostsDatabase CostsDatabasDatabas
eeCostCost CasesCases FTE’sFTE’s
Mayo 1972 Mayo 1972
CORR 344CORR 344$400,000/$400,000/
yryr56,00056,000 55
TRACS TRACS 19951995
NTDBNTDB
$400,000/$400,000/yryr
1,000,01,000,00000
33
Brigham Brigham 19701970
JBJS 82AJBJS 82A
$350,000/$350,000/yryr
15,00015,000 77
AORI 1977AORI 1977
CORR 421CORR 421$50,000/$50,000/
yryr80008000 11
Mass EMRMass EMR
NPR 02/04/NPR 02/04/0505
$35,000/$35,000/GPGP
---- 11
HWB 1993HWB 1993
www.hwbf.owww.hwbf.orgrg
$12,700/$12,700/yryr
45,00045,000 ----
26
Data Collection – Failure - Data Collection – Failure - Causes Causes
JAMIA Feb 2005 JAMIA Feb 2005
EMR Problems:EMR Problems:MalalignedMalaligned IncentivesIncentivesProduct ViabilityProduct ViabilityData QualityData QualityStandards - InteroperabilityStandards - Interoperability
27
Data QualityData Quality
"It has become increasingly clear that "It has become increasingly clear that much of the clinical research that has much of the clinical research that has long been published and on which we long been published and on which we base much of our education and practice base much of our education and practice activity is, in fact, severely flawed."activity is, in fact, severely flawed."
Keller, SPINE 20 384 1995Keller, SPINE 20 384 1995
OTA Specialty Day Debate 1999OTA Specialty Day Debate 1999SwiontkowskiSwiontkowski
28
Data QualityData Quality Tang, Shortliffe et al, JAMIA Proc Tang, Shortliffe et al, JAMIA Proc
19941994An observational study of physicians An observational study of physicians
using 168 medical records in an using 168 medical records in an internal medicine outpatient clinic internal medicine outpatient clinic
81% of cases failure of chart to provide 81% of cases failure of chart to provide all information deemed necessary by all information deemed necessary by the physician for appropriate the physician for appropriate management of the patient. management of the patient.
38% of a clinic encounter is taken up 38% of a clinic encounter is taken up by chart review.by chart review.
29
Data QualityData QualityGIGOGIGO
What is written without pain is in What is written without pain is in general read without pleasuregeneral read without pleasure
– – Samuel Johnson 1709-1784Samuel Johnson 1709-1784
The quality of the data begins with The quality of the data begins with the diligence of those who generate the diligence of those who generate it. it.
– – Charles Engh - Charles Engh - CORR 421CORR 421

30
Data QualityData Quality Barrie, Marsh, Barrie, Marsh, BMJ. 1992BMJ. 1992
Manchester physician-entered Manchester physician-entered orthopaedic databaseorthopaedic database
Data Quality Data Quality
= = Completeness Completeness XX Accuracy Accuracy
62%62% 96% 96%
31
Data QualityData QualityPolitical FactorsPolitical Factors
Health Info Tech SuccessHealth Info Tech Success 80% dependent on political 80% dependent on political
factors factors 20% dependent on info 20% dependent on info
technologytechnology
Reed Gardner 1998 Reed Gardner 1998 Past President of AMIAPast President of AMIA

32
Data QualityData QualityPolitical FactorsPolitical Factors
2% surgeons over 55 have a 2% surgeons over 55 have a major interest in orthopaedic major interest in orthopaedic trauma. trauma.
As it is these surgeons who tend As it is these surgeons who tend to be politically influential it is to be politically influential it is clear that orthopaedic trauma clear that orthopaedic trauma is considerably disadvantaged.is considerably disadvantaged.
JBJS 1997 79B:1, Court-Brown, JBJS 1997 79B:1, Court-Brown, McQueen McQueen Editorial: Trauma management in the Editorial: Trauma management in the UKUK
33
Data QualityData Quality Prospective vs. Prospective vs. RetrospectiveRetrospective
Do clinical databases give Do clinical databases give rise torise to
retrospective paper retrospective paper mills ?mills ?

34
Data QualityData Quality Random vs. Non-Random Random vs. Non-Random
Prospective randomized trials are Prospective randomized trials are well-proven for evaluating well-proven for evaluating pharmaceuticals. pharmaceuticals.
Different hands administering a Different hands administering a pill, however, have less influence pill, however, have less influence on the result than different hands on the result than different hands performing a surgical procedure. performing a surgical procedure.
Matta JOT August 2001Matta JOT August 2001

35
Prospective vs. Prospective vs. RetrospectiveRetrospective
Swiontkowski, JOT 2001 AugSwiontkowski, JOT 2001 Aug Because of the difficulty with Because of the difficulty with
performing high-quality control trials, performing high-quality control trials, observational studies are often the observational studies are often the best evidence we have. best evidence we have.
HoweverHowever When orthopaedists rely on these When orthopaedists rely on these
weaker forms of evidence, they must weaker forms of evidence, they must acknowledge the risk of utilizing a acknowledge the risk of utilizing a suboptimal or potentially even suboptimal or potentially even detrimental intervention for patients.detrimental intervention for patients.

36
Prospective vs. Prospective vs. RetrospectiveRetrospective
Benson et al, Benson et al, NEJMNEJM - June 22, 2000 - June 22, 2000Observational study advantages over PRCT:Observational study advantages over PRCT:
lower costlower cost greater timelinessgreater timeliness a broader range of patientsa broader range of patients
HoweverHoweverBias is a problemBias is a problem
Some say:Some say: observational studies are not reliable.observational studies are not reliable. observational studies should not be funded.observational studies should not be funded. observational studies should not be observational studies should not be
published. published.

37
Prospective vs. Prospective vs. RetrospectiveRetrospective
Bhandari et al, Bhandari et al, Arch Arch OrthopOrthop Trauma Trauma
SurgSurg. 2004 Jan. 2004 Jan Femoral Neck Fx Femoral Neck Fx
THA vs ORIF THA vs ORIF
14 randomized vs 14 randomized vs
13 13 non-randomizednon-randomized
THATHA RandoRandomm
Non-Non-RanRan
MortMort 1.04 1.04 1.441.44
Rev Rev RednRedn
0.380.38 0.230.23
Non-randomized studiesNon-randomized studies:: Over estimated THA risk - mortality 40%Over estimated THA risk - mortality 40% Under estimated THA benefit - revision Under estimated THA benefit - revision reduction 20%reduction 20%

38
Prospective vs. Prospective vs. RetrospectiveRetrospective
Benson et al, NEJM - June 22, 2000Benson et al, NEJM - June 22, 2000 136 reports about 19 diverse 136 reports about 19 diverse
treatmentstreatments
We found little evidence that We found little evidence that estimates of treatment effects in estimates of treatment effects in observational studies reported after observational studies reported after 1984 are either consistently larger 1984 are either consistently larger than or qualitatively different from than or qualitatively different from those obtained in randomized, those obtained in randomized, controlled trialscontrolled trials
39
Prospective vs. Prospective vs. RetrospectiveRetrospective
Concato et al, NEJM - June 22, 2000Concato et al, NEJM - June 22, 2000 99 reports about 5 clinical topics99 reports about 5 clinical topics
The results of well-designed The results of well-designed observational studies (with either a observational studies (with either a cohort or a case-control design) do cohort or a case-control design) do not systematically overestimate the not systematically overestimate the magnitude of the effects of treatment magnitude of the effects of treatment as compared with those in as compared with those in randomized, controlled trials on the randomized, controlled trials on the same topic.same topic.
40
Prospective vs. Prospective vs. RetrospectiveRetrospective
Tornetta et al, OTA 2000Tornetta et al, OTA 2000 Randomized trials are subject to Randomized trials are subject to Beta Beta
(Type II) error(Type II) error - - insufficient sample insufficient sample size. size.
Beta (Type II) error is the probability Beta (Type II) error is the probability of concluding that no difference of concluding that no difference between treatment groups exists, between treatment groups exists, when, in fact, there is a difference.when, in fact, there is a difference.
The beta (Type II) error rate for The beta (Type II) error rate for randomized trials in orthopaedic randomized trials in orthopaedic trauma is exceedingly high, averaging trauma is exceedingly high, averaging 90%.90%.

41
Prospective vs. Prospective vs. RetrospectiveRetrospective
Sarmiento, JOT 2001 AugSarmiento, JOT 2001 Aug There is not a system today, and there There is not a system today, and there
will not be a system tomorrow, that will not be a system tomorrow, that will guarantee the elimination of will guarantee the elimination of intended or unintended bias or intended or unintended bias or prejudice from the medical literature. prejudice from the medical literature.
That being the case, let us accept That being the case, let us accept outcome studies as well as traditional outcome studies as well as traditional retrospective ones.retrospective ones.

42
Data QualityData Quality End User Impact End User Impact

43
Data QualityData QualityEMR Design - Embi, JAMIA April 2004EMR Design - Embi, JAMIA April 2004
End User Impact End User Impact
Portland VAHPortland VAH
Documentation Availability Documentation Availability Work Processes and CommunicationWork Processes and Communication Alterations in Document Structure and Alterations in Document Structure and
ContentContent Mistakes, Concerns, and Decreased Mistakes, Concerns, and Decreased
Confidence Confidence
44
Data QualityData QualityPatel, JAMIA November 2000Patel, JAMIA November 2000
End User ImpactEnd User Impact EMR use changes physician EMR use changes physician
information gathering and reasoning information gathering and reasoning strategies. strategies.
Technology has a profound influence Technology has a profound influence in shaping cognitive behavior.in shaping cognitive behavior.
Effects on cognition by technology Effects on cognition by technology design needs to be explored. design needs to be explored.

45
Data QualityData QualityAMNews Feb. 17, 2003AMNews Feb. 17, 2003
End User ImpactEnd User ImpactEMR Rejection - EMR Rejection - Cedars Sinai RevoltCedars Sinai Revolt
"They "They poorly designed the systempoorly designed the system, poorly sold it , poorly sold it and then and then jammed it down our throatsjammed it down our throats and had and had the audacity to say everybody loves it and that the audacity to say everybody loves it and that it's a great system.“it's a great system.“
Cedars-Sinai Medical Center in Los Angeles has Cedars-Sinai Medical Center in Los Angeles has
indefinitely suspended use of its computerized indefinitely suspended use of its computerized physician order entry (CPOE) system, after physician order entry (CPOE) system, after hundreds of doctors complained hundreds of doctors complained it was it was difficult to use and compromised patient difficult to use and compromised patient safetysafety
Los Angeles TimesLos Angeles Times
46
Data Collection – Failure - Data Collection – Failure - Causes Causes
JAMIA Feb 2005 JAMIA Feb 2005
EMR Problems:EMR Problems:MalalignedMalaligned IncentivesIncentivesProduct ViabilityProduct ViabilityData QualityData QualityStandards - InteroperabilityStandards - Interoperability
47
Standards & InteroperabilityStandards & Interoperability Open SourceOpen Source
?? Solution ?? - ?? Solution ?? - Open Source SoftwareOpen Source Software – e.g. Linux– e.g. Linux
PROSPROS Low Cost - FreeLow Cost - Free StableStable Could provide essential infrastructure Could provide essential infrastructure
US Interstate Highways SystemUS Interstate Highways System Internet Transmission Control Protocol / Internet Internet Transmission Control Protocol / Internet
ProtocolProtocol Public Library of program componentsPublic Library of program components
CONSCONS Difficult to program and obtain local supportDifficult to program and obtain local support Microsoft buys IT lunch – Significant kickbacks Microsoft buys IT lunch – Significant kickbacks
barriersbarriers

48
Standards & InteroperabilityStandards & Interoperability Open SourceOpen Source
?? Solution ?? - ?? Solution ?? - Open Source SoftwareOpen Source Software – e.g. Linux – e.g. Linux
PROSPROS Low Cost - FreeLow Cost - Free StableStable Could provide essential infrastructure Could provide essential infrastructure
US Interstate Highways SystemUS Interstate Highways System Internet Transmission Control Protocol / Internet Internet Transmission Control Protocol / Internet
ProtocolProtocol Public Library of program componentsPublic Library of program components
CONSCONS Difficult to program and obtain local supportDifficult to program and obtain local support Microsoft buys IT lunch – Significant kickbacks Microsoft buys IT lunch – Significant kickbacks
barriersbarriers

49
SummarySummary EMR PotentialEMR Potential
benefitsbenefits risksrisksAvailabilityAvailabilityWorkflow Workflow integrationintegrationCognitive Cognitive enhancementenhancementLegibilityLegibilityConnectivityConnectivityRemote AccessRemote AccessError checkingError checking
ExpirationExpirationWorkflow Workflow disruptiondisruptionCognitive Cognitive impairmentimpairmentData fogData fogDiminished privacy Diminished privacy Cultural demiseCultural demiseError propagationError propagation

50
Data Collection – How?Data Collection – How?UMC – HOSPITAL Records
Vanderbilt Medical Center 13,199Elmhurst Hospital Center 10,886Bellevue Hospital Center 6983Detroit Receiving Hospital 6636Hartford Hospital 4262Hennepin County Med Ctr 1043Norfolk & Norwich (UK) 633Southern Illinois University 456Denver General Hospital 450MIEMSS 168University of Geneva 46Rhode Island Hospital 0Maricopa County Hospital 0Grady Memorial 0Henry Ford Hospital 0
TOTAL 44,762

51
ConclusionConclusion Hill, NEJM 1953Hill, NEJM 1953
""One must go seek more facts, One must go seek more facts, paying less attention to paying less attention to technique of handling the technique of handling the data and far more to the data and far more to the development and perfection development and perfection of the method for obtaining of the method for obtaining them."them."

52
Revised HWB Mission Revised HWB Mission StatementStatement
The mission of the HWB foundation The mission of the HWB foundation is is to find methodsto find methods to routinely to routinely collect well-specified, structured collect well-specified, structured and privacy-protected clinical data and privacy-protected clinical data from reliable sources and make from reliable sources and make that data, in quantities of statistical that data, in quantities of statistical significance, available in the public significance, available in the public domain where it may be interpreted domain where it may be interpreted from all points of view. from all points of view.




















![[Hippocrates] Hippocrates - Of the Epidemics(BookZZ.org)](https://img.pdfslide.us/doc/110x75/577cc3461a28aba711957d65/hippocrates-hippocrates-of-the-epidemicsbookzzorg.jpg)
![The Winslow mail. (Winslow, Ariz.) 1926-05-28 [p PAGE FOUR]](https://img.pdfslide.us/doc/110x75/621058d8c7683c59fe60e913/the-winslow-mail-winslow-ariz-1926-05-28-p-page-four.jpg)