Embed Size (px)
Citation preview
1
Navy Medicine Strategic Plan
Executive Medical Department Enlisted Course
05 February 2014Karen L. M. Sayers, MSOD
Office of Strategy Management/M5U.S. Navy Bureau of Medicine &
Surgery
World-Class Care…Anytime, Anywhere
Learning Objectives
2
• Overview of Strategic Planning Process • Navy Medicine’s Strategic Plan
• Cascading the Plan
• Executing & Reviewing Progress
World-Class Care…Anytime, Anywhere
3
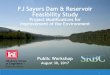
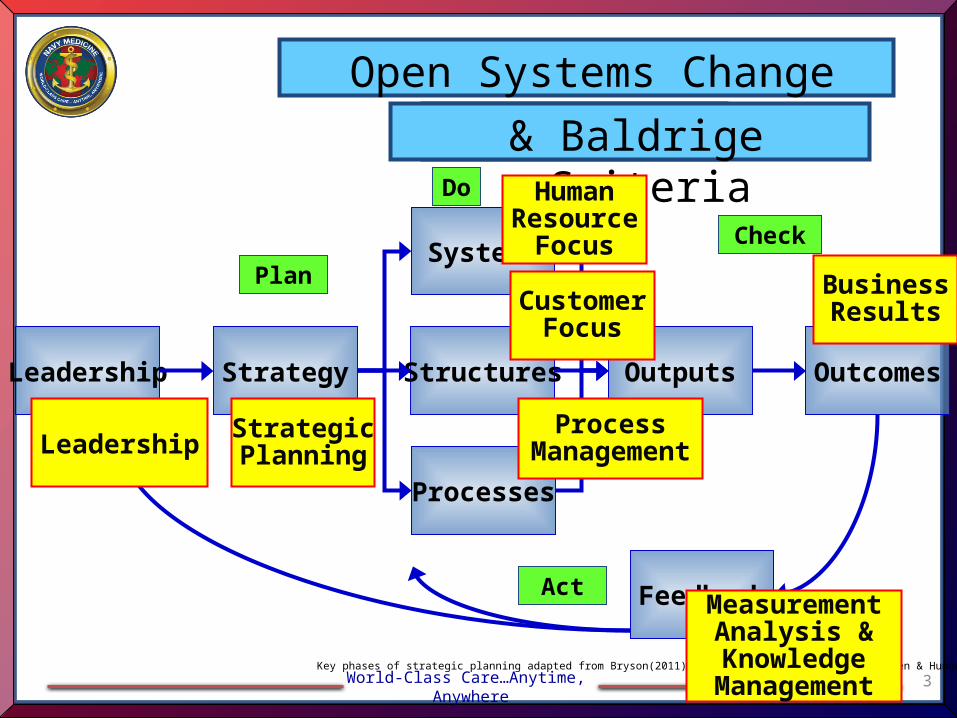
Leadership Strategy Structures
Systems
Processes
Outputs Outcomes
Feedback
Open Systems Change Model
Key phases of strategic planning adapted from Bryson(2011), Allison & Kaye(2005), and Wheelen & Hunger(2006)
Do
Check
Act
Plan
& PDCA& Baldrige Criteria
LeadershipStrategicPlanning
HumanResource
Focus
CustomerFocus
MeasurementAnalysis &Knowledge
Management
BusinessResults
ProcessManagement
World-Class Care…Anytime, Anywhere
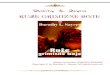
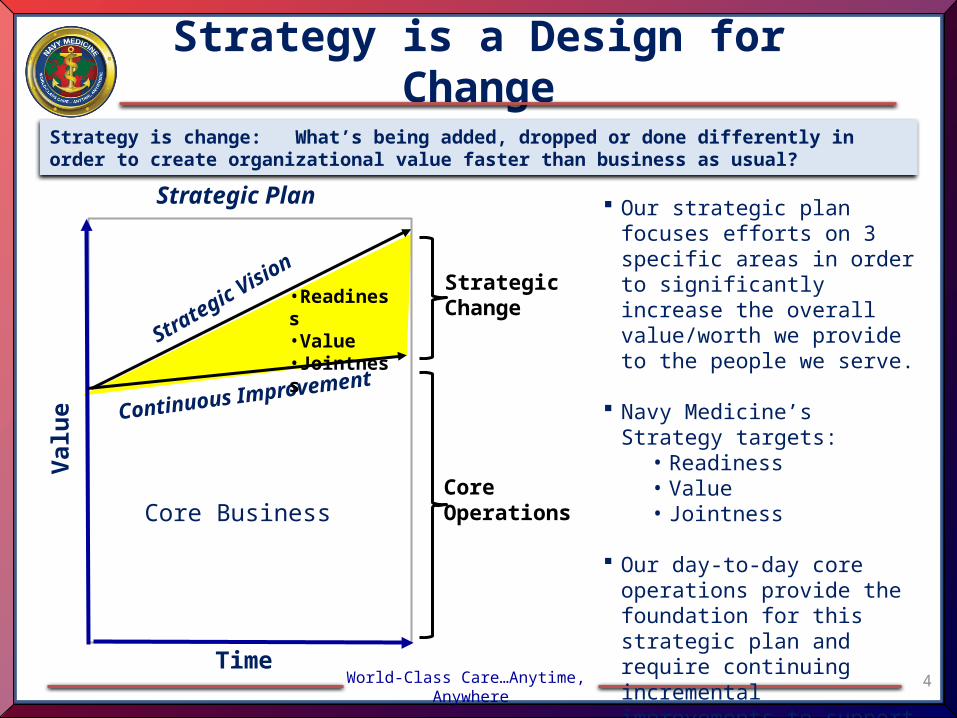
Strategy is a Design for Change
4Time
Our strategic plan focuses efforts on 3 specific areas in order to significantly increase the overall value/worth we provide to the people we serve.
Navy Medicine’s Strategy targets:
• Readiness • Value• Jointness
Our day-to-day core operations provide the foundation for this strategic plan and require continuing incremental improvements to support it.
Strategic Vision
Val
ue Continuous Improvement
Strategic Plan
StrategicChange
CoreOperationsCore Business
•Readiness•Value•Jointness
Strategy is change: What’s being added, dropped or done differently in order to create organizational value faster than business as usual?
5World-Class Care…Anytime, Anywhere
Navy Medicine
MissionWe enable readiness, wellness, and health care to Sailors, Marines, their families, and all others entrusted to us worldwide, be it on land or at sea.
VisionNavy Medicine is the pinnacle of excellence - answering the call across any dynamic - from kinetic operations to global engagement. Our health care is patient-centered and provides best value, preserves health, and maintains
readiness. Agility, professionalism, an ethos of care, and the ability to deploy to any environment or sea state are our hallmarks.
Guiding Principles Ship - Shipmate - Self
Strategic Priorities READINESS - VALUE - JOINTNESS
No Change
World-Class Care…Anytime, Anywhere
Navy Medicine Guiding Principles
6
Ship – Shipmate - Self
Ship ➢ Take care of the ship. The ship is the mission, the environment or command we operate in, our patients, and those we serve who seek care. It could be the Marines we are serving alongside or the vaccine we are trying to create. We must all consistently ask ourselves where we fit into the overall mission and priorities of not just our commands, but of the entire Navy Medicine enterprise. We must honor our proud heritage and perform the mission without fail.
Shipmate ➢ Take care of each other. Be vigilant to the needs and actions of your shipmates and watch out for one another. We must maintain an optimum level of professionalism at all times. We must remain on a path that supports our core values of honor, courage and commitment. When someone starts to veer off that course or starts to show signs of trouble, step between your shipmate and trouble and help them course correct. We all need one another to succeed. Leave no shipmate behind.
Self ➢ Take care of yourself. You cannot care for others if you are not caring for yourself. Asking for help is a sign of strength. We are all in this together. You must constantly reflect on your own needs and those of your family. Speak up so we can better equip you to meet the challenges you are facing. Self-reflection and awareness is also an important part of leadership and success.
No Change
World-Class Care…Anytime, Anywhere
Navy Medicine’s Strategic Goals
• We provide agile, adaptable, and scalable capabilities prepared to engage globally across the range of military operations within maritime and other domains in support of the national defense strategy.
Readiness
• We will provide exceptional value to those we serve by ensuring highest quality care through best health care practices, full and efficient utilization of our services, and lower care costs.
Value
• We lead Navy Medicine to jointness and improved interoperability by pursuing the most effective ways of mission accomplishment.
Jointness
7
• Strategic enabling objectives will help Navy Medicine achieve its mission and accomplish our Goals and Objectives.
STRATEGIC ENABLING OBJECTIVES
No Change
World-Class Care…Anytime, Anywhere
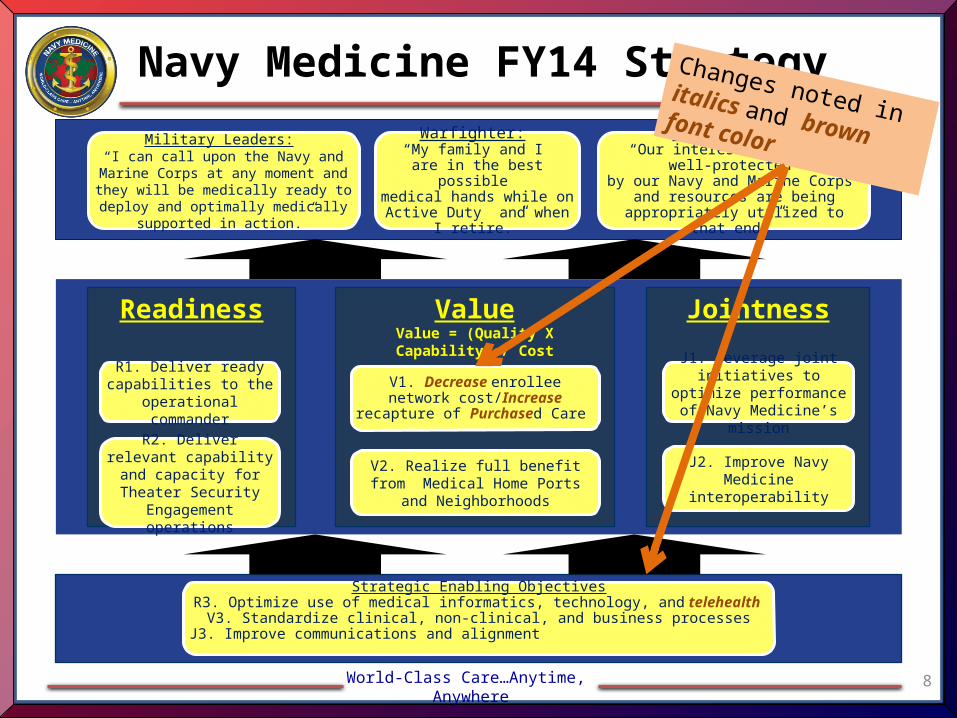
Readiness JointnessValueValue = (Quality X Capability) / Cost
R1. Deliver ready capabilities to the
operational commander
Military Leaders: “I can call upon the Navy and Marine Corps at any moment and they will be
medically ready to deploy and optimally medically supported in action.”
R2. Deliver relevant capability and capacity for
Theater Security Engagement operations
Strategic Enabling ObjectivesR3. Optimize use of medical informatics, technology, and telehealth
V3. Standardize clinical, non-clinical, and business processesJ3. Improve communications and alignment
Navy Medicine FY14 Strategy
8
Warfighter: “My family and I
are in the best possible medical hands while on Active Duty and when I
retire.”
J1. Leverage joint initiatives to optimize performance of Navy Medicine’s mission
U.S. Public: “Our interests are being well-protected
by our Navy and Marine Corps and resources are being appropriately
utilized to that end.”
V1. Decrease enrollee network cost/Increase recapture of
Purchased Care
V2. Realize full benefit from Medical Home Ports and Neighborhoods
J2. Improve Navy Medicine interoperability
Changes noted in italics and brown font color
World-Class Care…Anytime, Anywhere
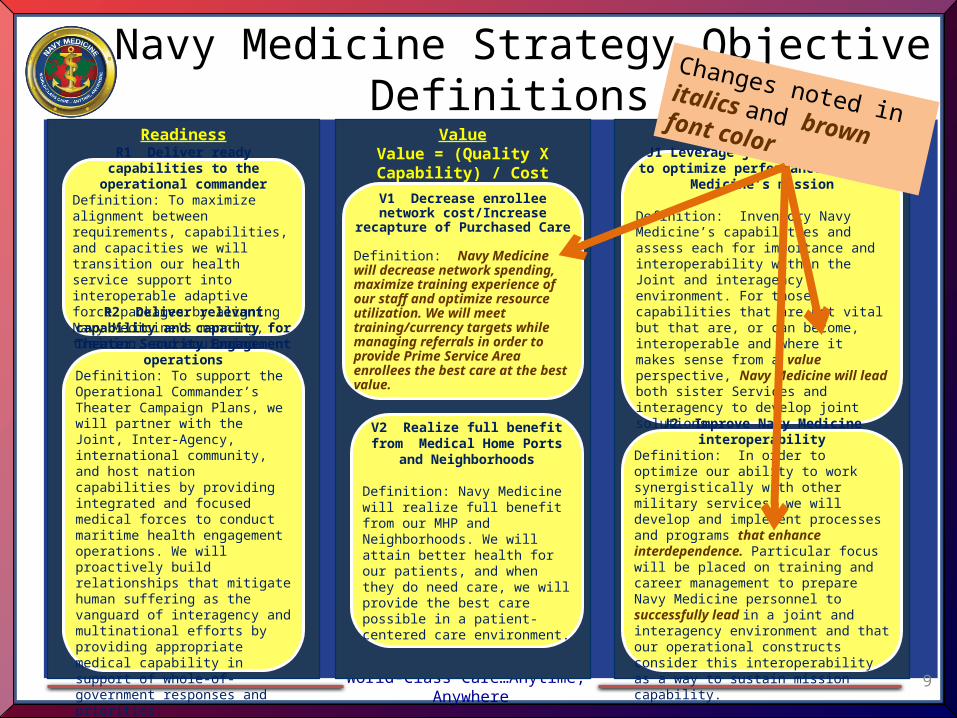
Readiness JointnessValueValue = (Quality X Capability) /
Cost
Navy Medicine Strategy Objective Definitions
R1 Deliver ready capabilities to the operational commander
Definition: To maximize alignment between requirements, capabilities, and capacities we will transition our health service support into interoperable adaptive force packages by aligning Navy Medicine's manning, training, and equipping.
R2 Deliver relevant capability and capacity for Theater Security
Engagement operationsDefinition: To support the Operational Commander’s Theater Campaign Plans, we will partner with the Joint, Inter-Agency, international community, and host nation capabilities by providing integrated and focused medical forces to conduct maritime health engagement operations. We will proactively build relationships that mitigate human suffering as the vanguard of interagency and multinational efforts by providing appropriate medical capability in support of whole-of-government responses and priorities.
9
J1 Leverage joint initiatives to optimize performance of Navy Medicine’s
mission
Definition: Inventory Navy Medicine’s capabilities and assess each for importance and interoperability within the Joint and interagency environment. For those capabilities that are not vital but that are, or can become, interoperable and where it makes sense from a value perspective, Navy Medicine will lead both sister Services and interagency to develop joint solutions.
V1 Decrease enrollee network cost/Increase recapture of
Purchased Care
Definition: Navy Medicine will decrease network spending, maximize training experience of our staff and optimize resource utilization. We will meet training/currency targets while managing referrals in order to provide Prime Service Area enrollees the best care at the best value.
V2 Realize full benefit from Medical Home Ports and
Neighborhoods
Definition: Navy Medicine will realize full benefit from our MHP and Neighborhoods. We will attain better health for our patients, and when they do need care, we will provide the best care possible in a patient-centered care environment.
J2 Improve Navy Medicine interoperability
Definition: In order to optimize our ability to work synergistically with other military services, we will develop and implement processes and programs that enhance interdependence. Particular focus will be placed on training and career management to prepare Navy Medicine personnel to successfully lead in a joint and interagency environment and that our operational constructs consider this interoperability as a way to sustain mission capability.
Changes noted in italics and brown font color
World-Class Care…Anytime, Anywhere
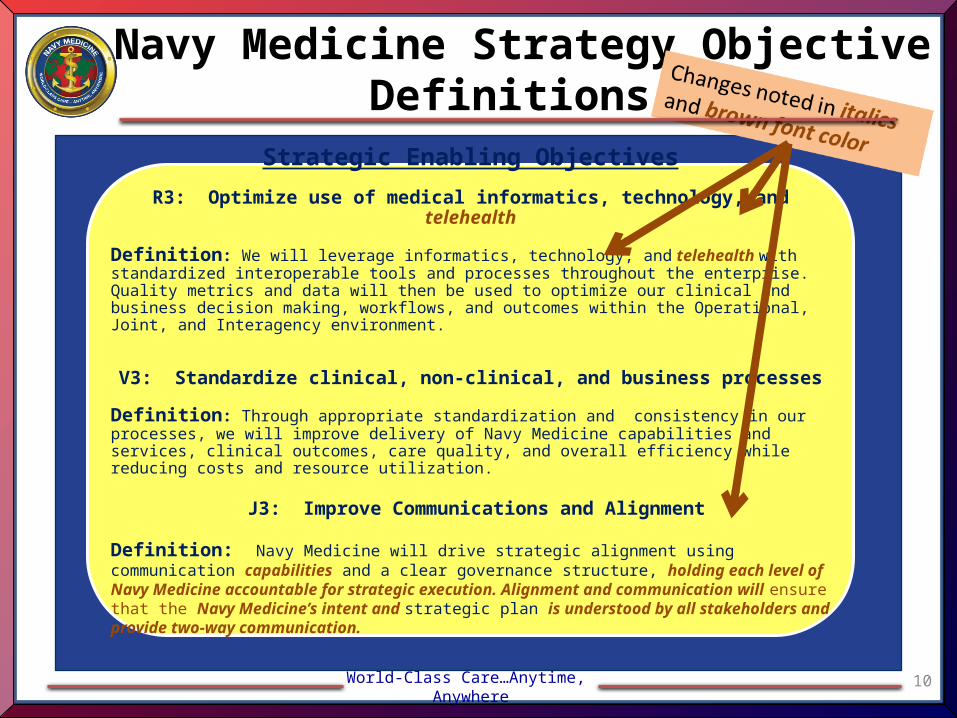
Strategic Enabling Objectives
R3: Optimize use of medical informatics, technology, and telehealth
Definition: We will leverage informatics, technology, and telehealth with standardized interoperable tools and processes throughout the enterprise. Quality metrics and data will then be used to optimize our clinical and business decision making, workflows, and outcomes within the Operational, Joint, and Interagency environment.
V3: Standardize clinical, non-clinical, and business processes
Definition: Through appropriate standardization and consistency in our processes, we will improve delivery of Navy Medicine capabilities and services, clinical outcomes, care quality, and overall efficiency while reducing costs and resource utilization.
J3: Improve Communications and Alignment
Definition: Navy Medicine will drive strategic alignment using communication capabilities and a clear governance structure, holding each level of Navy Medicine accountable for strategic execution. Alignment and communication will ensure that the Navy Medicine’s intent and strategic plan is understood by all stakeholders and provide two-way communication.
10
Navy Medicine Strategy Objective Definitions
World-Class Care…Anytime, Anywhere
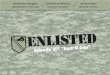
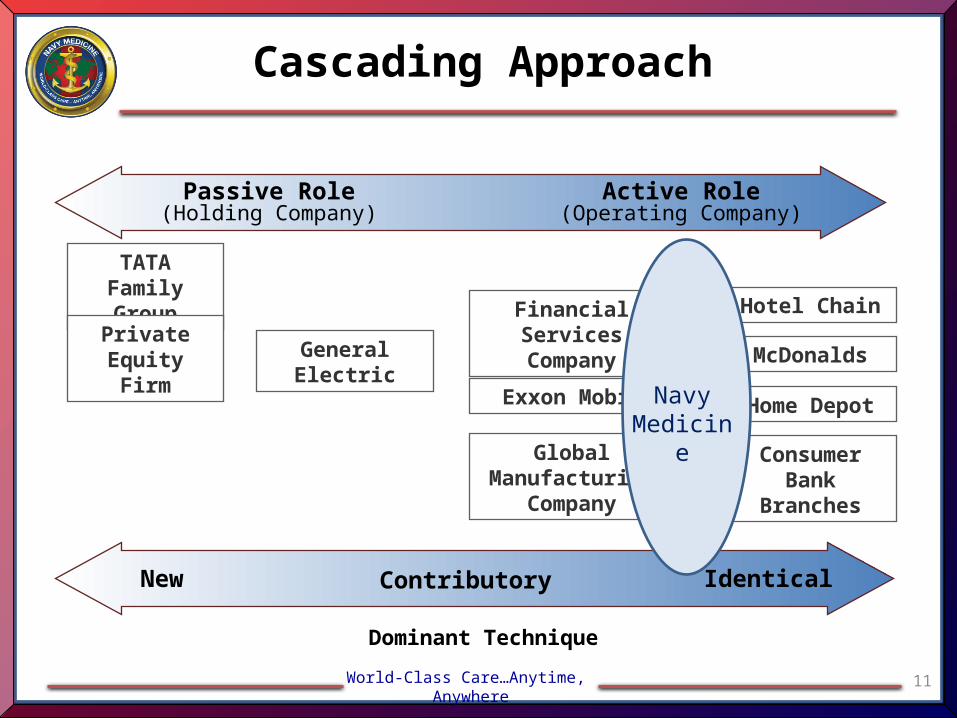
Cascading Approach
11
TATA Family Group
Private Equity Firm
GeneralElectric
Financial Services Company
Exxon Mobil
Hotel Chain
Global Manufacturing
Company
Home Depot
McDonalds
IdenticalContributory
Passive Role(Holding Company)
Active Role(Operating Company)
Dominant Technique
New
Consumer Bank
Branches
NavyMedicine
World-Class Care…Anytime, Anywhere
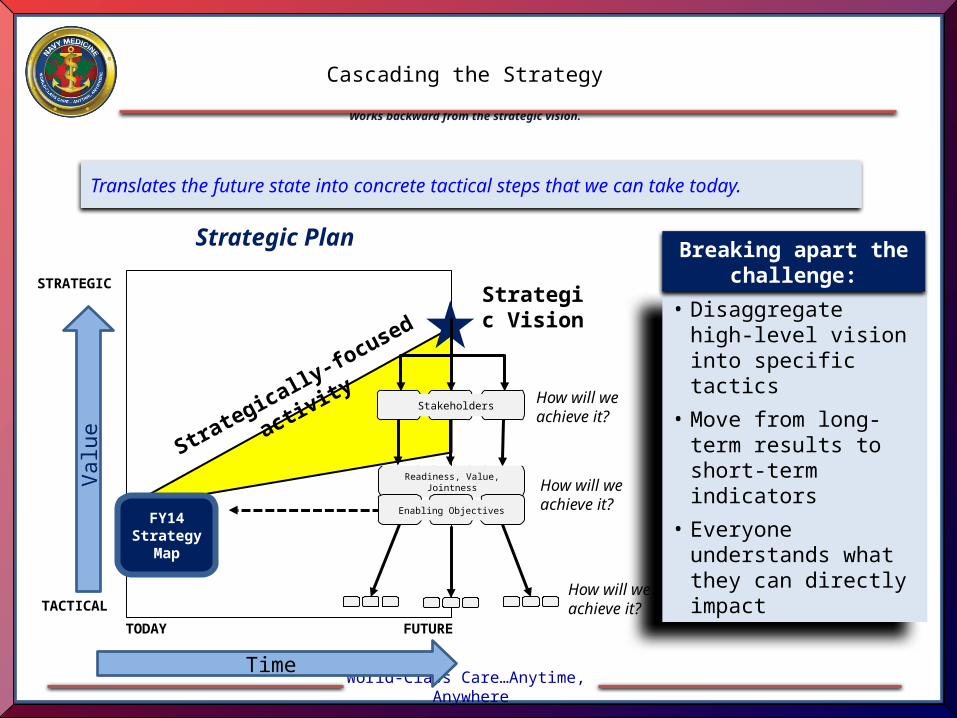
Cascading the Strategy
Works backward from the strategic vision.
Strategically-fo
cused activity
Strategic Vision
How will we achieve it?
STRATEGIC
TODAY
FY14 Strategy
Map
• Disaggregate high-level vision into specific tactics
• Move from long-term results to short-term indicators
• Everyone understands what they can directly impact
Breaking apart the challenge:
Translates the future state into concrete tactical steps that we can take today.
Stakeholders
Readiness, Value, Jointness
Enabling Objectives
How will we achieve it?
How will we achieve it?
Strategic Plan
Time
Val
ue
TACTICAL
FUTURE
World-Class Care…Anytime, Anywhere
Readiness JointnessValueValue = (Quality X Capability) /
Cost
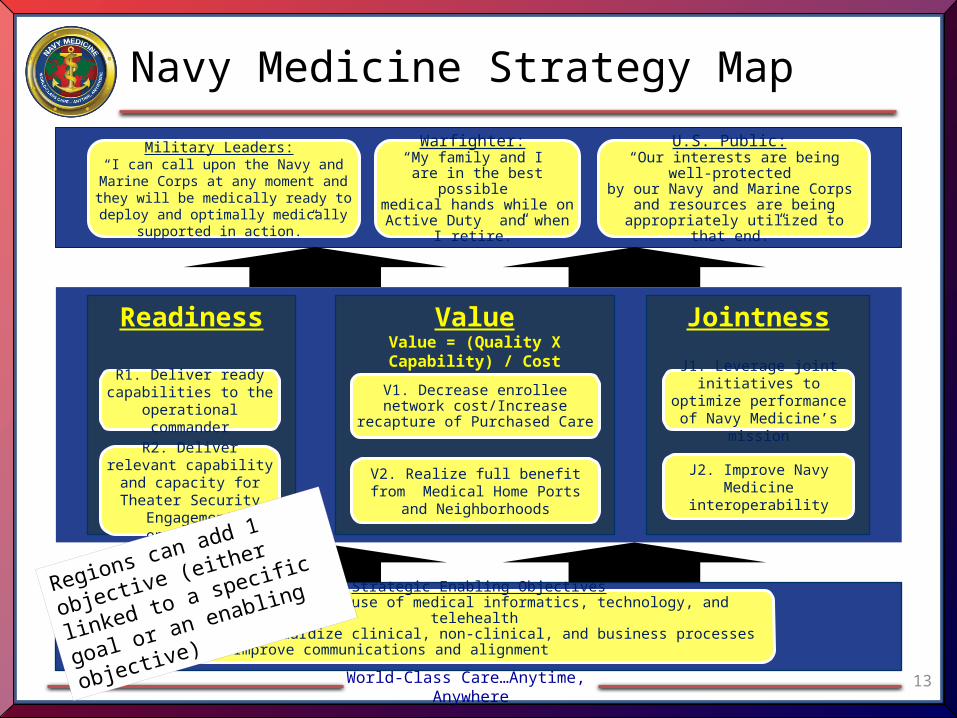
Navy Medicine Strategy Map
R1. Deliver ready capabilities to the
operational commander
Military Leaders: “I can call upon the Navy and Marine Corps at any moment and they will be
medically ready to deploy and optimally medically supported in action.”
R2. Deliver relevant capability and capacity for
Theater Security Engagement operations
Strategic Enabling ObjectivesEO1. Optimize use of medical informatics, technology, and telehealth
EO2. Standardize clinical, non-clinical, and business processesEO3. Improve communications and alignment
13
Warfighter: “My family and I
are in the best possible medical hands while on Active Duty and when I
retire.”
J1. Leverage joint initiatives to optimize performance of Navy Medicine’s mission
U.S. Public: “Our interests are being well-protected
by our Navy and Marine Corps and resources are being appropriately
utilized to that end.”
V1. Decrease enrollee network cost/Increase recapture of
Purchased Care
V2. Realize full benefit from Medical Home Ports and Neighborhoods
J2. Improve Navy Medicine interoperability
Regions can add 1 objective
(either linked to a specific
goal or an enabling
objective)
World-Class Care…Anytime, Anywhere
Readiness JointnessValueValue = (Quality X Capability) /
Cost
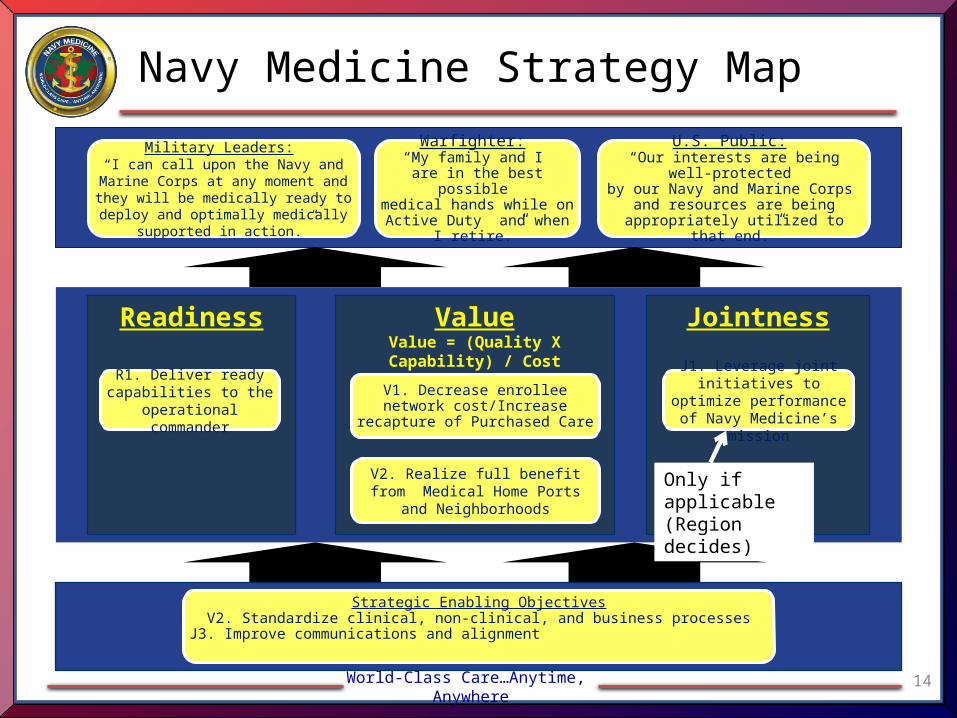
Navy Medicine Strategy Map
R1. Deliver ready capabilities to the
operational commander
Military Leaders: “I can call upon the Navy and Marine Corps at any moment and they will be
medically ready to deploy and optimally medically supported in action.”
Strategic Enabling ObjectivesV2. Standardize clinical, non-clinical, and business processes
J3. Improve communications and alignment
14
Warfighter: “My family and I
are in the best possible medical hands while on Active Duty and when I
retire.”
J1. Leverage joint initiatives to optimize performance of Navy Medicine’s mission
U.S. Public: “Our interests are being well-protected
by our Navy and Marine Corps and resources are being appropriately
utilized to that end.”
V1. Decrease enrollee network cost/Increase recapture of
Purchased Care
V2. Realize full benefit from Medical Home Ports and Neighborhoods
Only if applicable (Region decides)
World-Class Care…Anytime, Anywhere
Readiness JointnessValueValue = (Quality X Capability) /
Cost
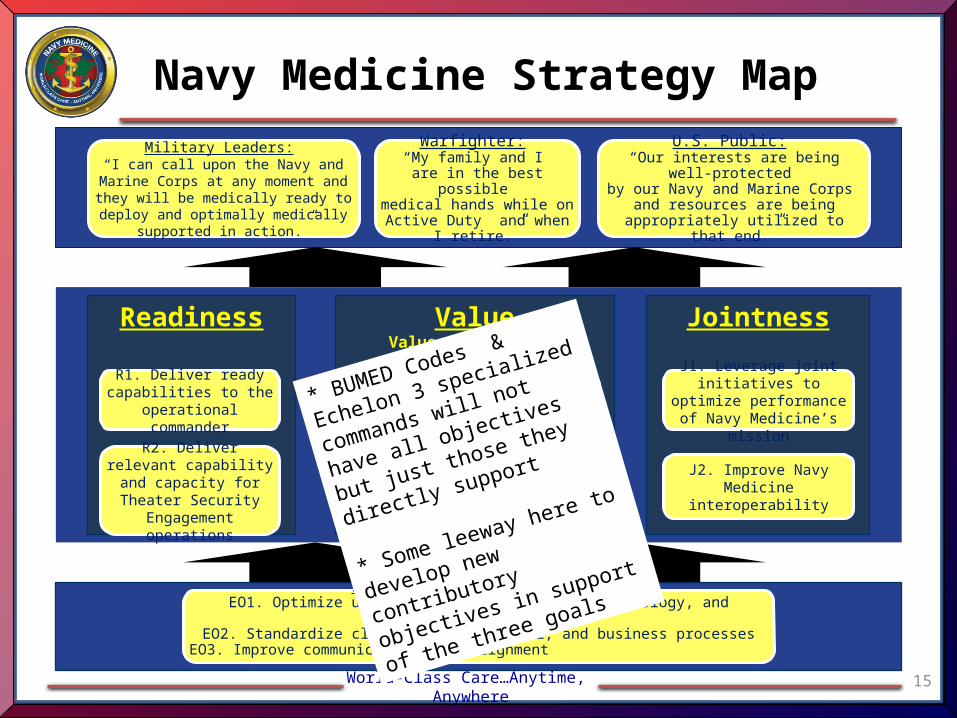
Navy Medicine Strategy Map
R1. Deliver ready capabilities to the
operational commander
Military Leaders: “I can call upon the Navy and Marine Corps at any moment and they will be
medically ready to deploy and optimally medically supported in action.”
R2. Deliver relevant capability and capacity for
Theater Security Engagement operations
Strategic Enabling ObjectivesEO1. Optimize use of medical informatics, technology, and telehealth
EO2. Standardize clinical, non-clinical, and business processesEO3. Improve communications and alignment
15
Warfighter: “My family and I
are in the best possible medical hands while on Active Duty and when I
retire.”
J1. Leverage joint initiatives to optimize performance of Navy Medicine’s mission
U.S. Public: “Our interests are being well-protected
by our Navy and Marine Corps and resources are being appropriately
utilized to that end.”
V1. Decrease enrollee network cost/Increase recapture of
Purchased Care
V2. Realize full benefit from Medical Home Ports and Neighborhoods
J2. Improve Navy Medicine interoperability
* BUMED Codes & Echelon
3 specialized commands will
not have all objectives but
just those they directly
support
* Some leeway here to
develop new contributory
objectives in support of the
three goals
World-Class Care…Anytime, Anywhere
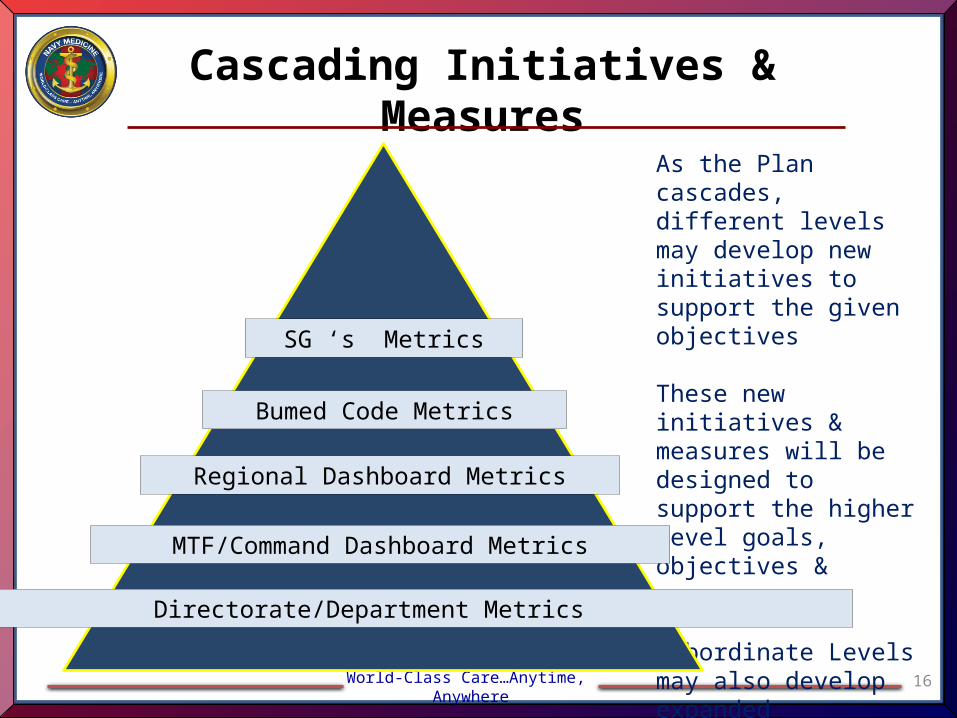
Cascading Initiatives & Measures
16
As the Plan cascades, different levels may develop new initiatives to support the given objectives
These new initiatives & measures will be designed to support the higher level goals, objectives & measures
Subordinate Levels may also develop expanded metrics/measures
SG ‘s Metrics
Regional Dashboard Metrics
Bumed Code Metrics
MTF/Command Dashboard Metrics
Directorate/Department Metrics
World-Class Care…Anytime, Anywhere
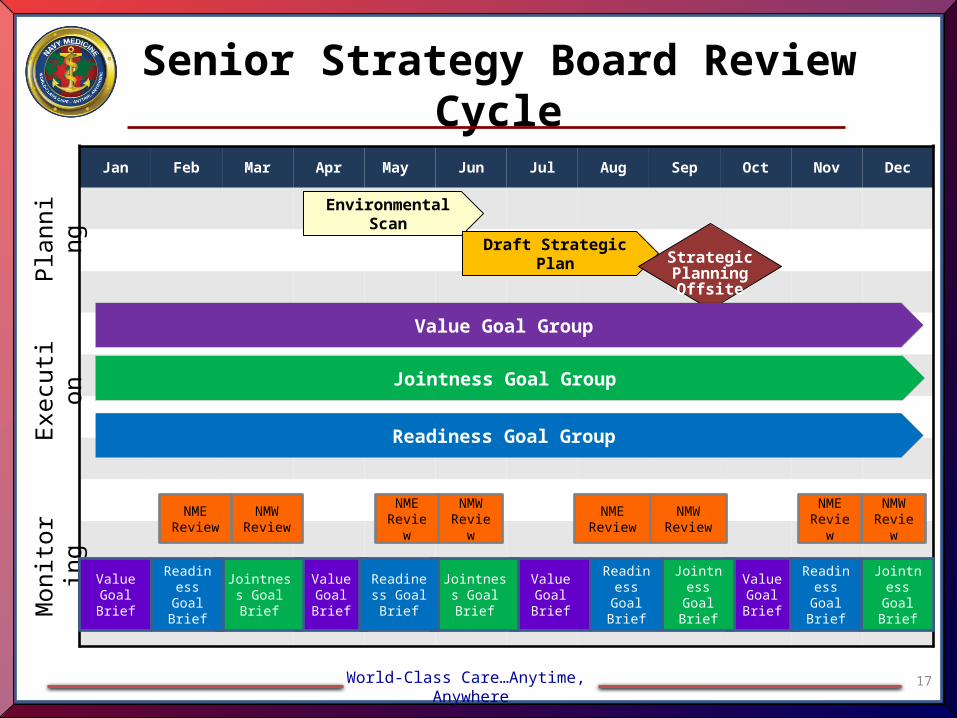
Senior Strategy Board Review Cycle
17
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Environmental Scan
Draft Strategic Plan StrategicPlanning Offsite
Value Goal Group
Jointness Goal Group
Readiness Goal Group
Pla
nnin
gE
xecu
tion
Mon
itorin
g
NMW Review
NME Review
NMW Review
NME Review
NMW Review
NME Review
NMW Review
NME Review
Value Goal Brief
Value Goal Brief
Value Goal Brief
Value Goal Brief
Jointness Goal Brief
Jointness Goal Brief
Jointness Goal Brief
Jointness Goal Brief
Readiness Goal Brief
Readiness Goal Brief
Readiness Goal Brief
Readiness Goal Brief
World-Class Care…Anytime, Anywhere
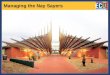
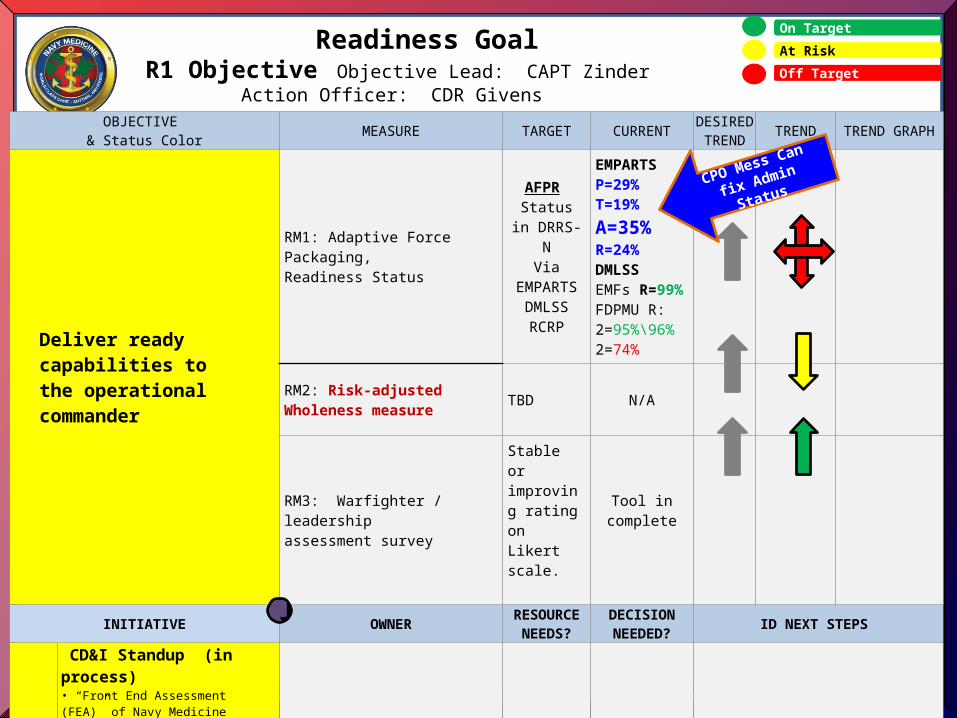
18
On Target
At Risk
Off Target
OBJECTIVE & Status Color MEASURE TARGET CURRENT DESIRED
TREND TREND TREND GRAPH
Deliver ready capabilities to the operational commander
RM1: Adaptive Force Packaging, Readiness Status
AFPR Status in DRRS-N
ViaEMPARTS
DMLSSRCRP
EMPARTSP=29%T=19%A=35%R=24%DMLSSEMFs R=99%FDPMU R:2=95%\96%2=74%
RM2: Risk-adjusted Wholeness measure TBD N/A
RM3: Warfighter / leadership assessment survey
Stable or improving rating on Likert scale.
Tool in complete
INITIATIVE OWNER RESOURCE NEEDS?
DECISION NEEDED? ID NEXT STEPS
RI11
CD&I Standup (in process)• “Front End Assessment (FEA)” of Navy Medicine readiness reporting. • DRRS-N reporting of NAVMED Sponsored & Supported Platforms • Develop & deploy tool to assess operational Commanders’ satisfaction with Navy Medicine’s readiness during all phases of deployment.
CD&I Pending Pending FTE Estimation
Readiness GoalR1 Objective Objective Lead: CAPT Zinder
Action Officer: CDR Givens
J
CPO Mess Can fix
Admin Status
World-Class Care…Anytime, Anywhere
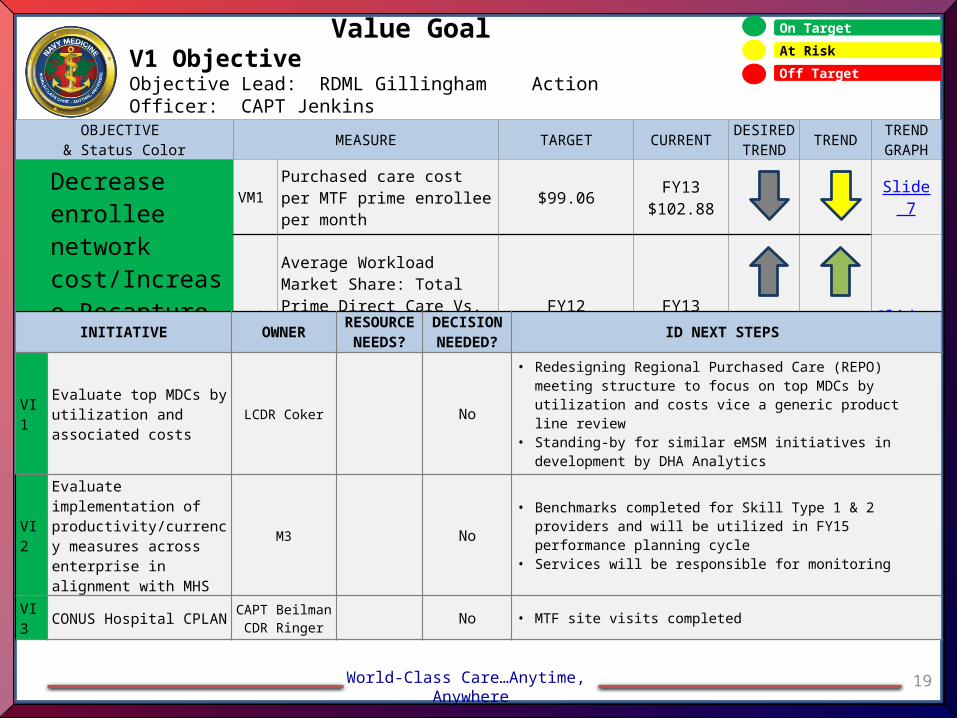
19
On Target
At Risk
Off Target
OBJECTIVE & Status Color MEASURE TARGET CURRENT DESIRED
TREND TREND TREND GRAPH
Decrease enrollee network cost/Increase Recapture of Purchased Care
VM1 Purchased care cost per MTF prime enrollee per month
$99.06FY13
$102.88Slide 7
VM2
Average Workload Market Share: Total Prime Direct Care Vs. Total Prime Care within a Prime Service Area
FY1247%
FY1350%
Slide 8
Value GoalV1 ObjectiveObjective Lead: RDML Gillingham Action Officer: CAPT Jenkins
INITIATIVE OWNER RESOURCE NEEDS?
DECISION NEEDED? ID NEXT STEPS
VI1Evaluate top MDCs by utilization and associated costs
LCDR Coker No
• Redesigning Regional Purchased Care (REPO) meeting structure to focus on top MDCs by utilization and costs vice a generic product line review
• Standing-by for similar eMSM initiatives in development by DHA Analytics
VI2
Evaluate implementation of productivity/currency measures across enterprise in alignment with MHS
M3 No• Benchmarks completed for Skill Type 1 & 2 providers and will be
utilized in FY15 performance planning cycle• Services will be responsible for monitoring
VI3 CONUS Hospital CPLAN CAPT BeilmanCDR Ringer No • MTF site visits completed
World-Class Care…Anytime, Anywhere
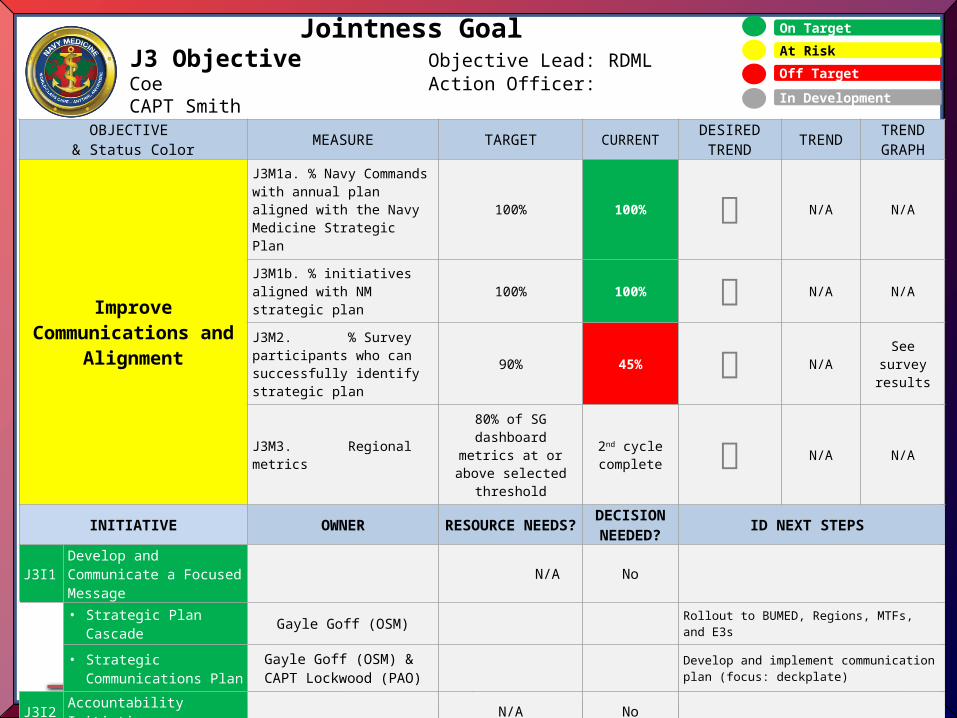
20
On Target
At Risk
Off Target
Jointness GoalJ3 Objective Objective Lead: RDML Coe
Action Officer: CAPT Smith
OBJECTIVE & Status Color MEASURE TARGET CURRENT
DESIRED TREND TREND TREND
GRAPH
Improve Communications and
Alignment
J3M1a. % Navy Commands with annual plan aligned with the Navy Medicine Strategic Plan
100% 100% N/A N/A
J3M1b. % initiatives aligned with NM strategic plan
100% 100% N/A N/A
J3M2. % Survey participants who can successfully identify strategic plan
90% 45% N/ASee survey
results
J3M3. Regional metrics
80% of SG dashboard metrics at or above selected threshold
2nd cycle complete N/A N/A
INITIATIVE OWNER RESOURCE NEEDS?
DECISION NEEDED? ID NEXT STEPS
J3I1 Develop and Communicate a Focused Message
N/A No
• Strategic Plan Cascade Gayle Goff (OSM) Rollout to BUMED, Regions, MTFs, and E3s
• Strategic Communications Plan
Gayle Goff (OSM) & CAPT Lockwood (PAO)
Develop and implement communication plan (focus: deckplate)
J3I2 Accountability Initiative N/A No
• Metrics Governing Board Gayle Goff (OSM) Continue to refine metrics; improve automation
• Regional Performance Review
COS Refreshed review reflects FY14 strategic changes; NME will undergo review in January
J3I3 BUMED Reinvention CAPT Hall None at this time
Single digits continue to define BUMED mission; ADCs will take vision and develop organizational constructs
In Development
World-Class Care…Anytime, Anywhere
21
Questions?
Ms. Karen L. M .Sayers, MSODOffice of Strategy Management/M5
Bureau of Medicine & Surgery7700 Arlington Blvd
Falls Church, VA 22042-5116Email: [email protected]
Com: 703-681-9034DSN: 761-9034
BB: 202-230-7496
22
Senior Strategy BoardReadiness Goal Brief
November 14, 2013
Goal Lead: RDML Stephen Pachuta
Vice Goal Lead: RDML Brian Pecha
We provide agile, adaptable, and scalable capabilities prepared to engage globally across the range of military
operations within maritime and other domains in support of the national defense strategy..
World-Class Care…Anytime, Anywhere
23
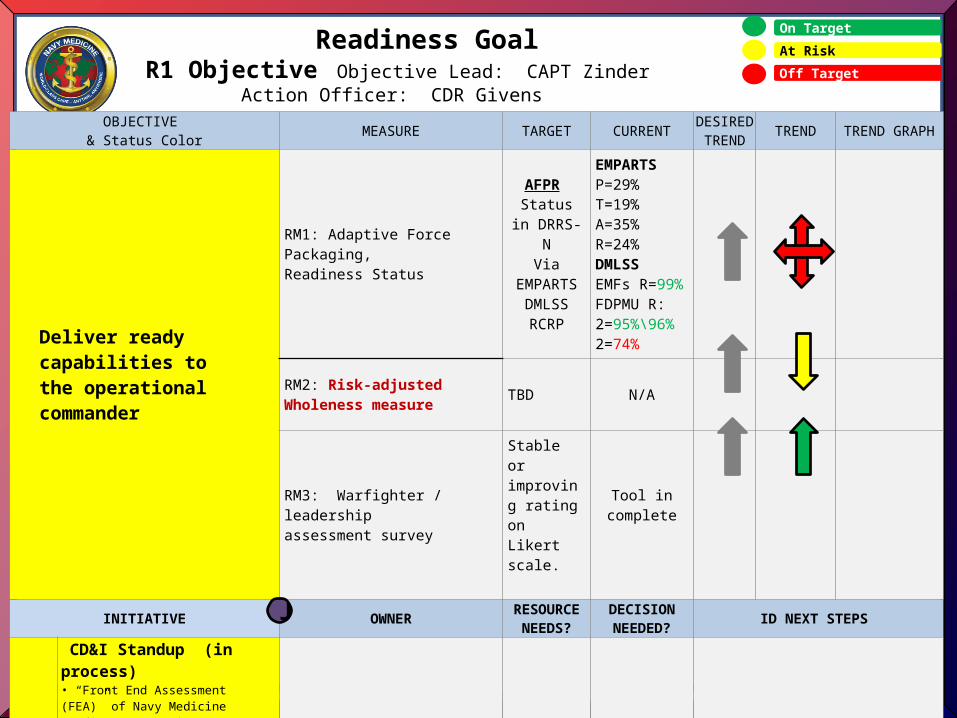
On Target
At Risk
Off Target
OBJECTIVE & Status Color MEASURE TARGET CURRENT DESIRED
TREND TREND TREND GRAPH
Deliver ready capabilities to the operational commander
RM1: Adaptive Force Packaging, Readiness Status
AFPR Status in DRRS-N
ViaEMPARTS
DMLSSRCRP
EMPARTSP=29%T=19%A=35%R=24%DMLSSEMFs R=99%FDPMU R:2=95%\96%2=74%
RM2: Risk-adjusted Wholeness measure TBD N/A
RM3: Warfighter / leadership assessment survey
Stable or improving rating on Likert scale.
Tool in complete
INITIATIVE OWNER RESOURCE NEEDS?
DECISION NEEDED? ID NEXT STEPS
RI11
CD&I Standup (in process)• “Front End Assessment (FEA)” of Navy Medicine readiness reporting. • DRRS-N reporting of NAVMED Sponsored & Supported Platforms • Develop & deploy tool to assess operational Commanders’ satisfaction with Navy Medicine’s readiness during all phases of deployment.
CD&I Pending Pending FTE Estimation
Readiness GoalR1 Objective Objective Lead: CAPT Zinder
Action Officer: CDR Givens
J
World-Class Care…Anytime, Anywhere
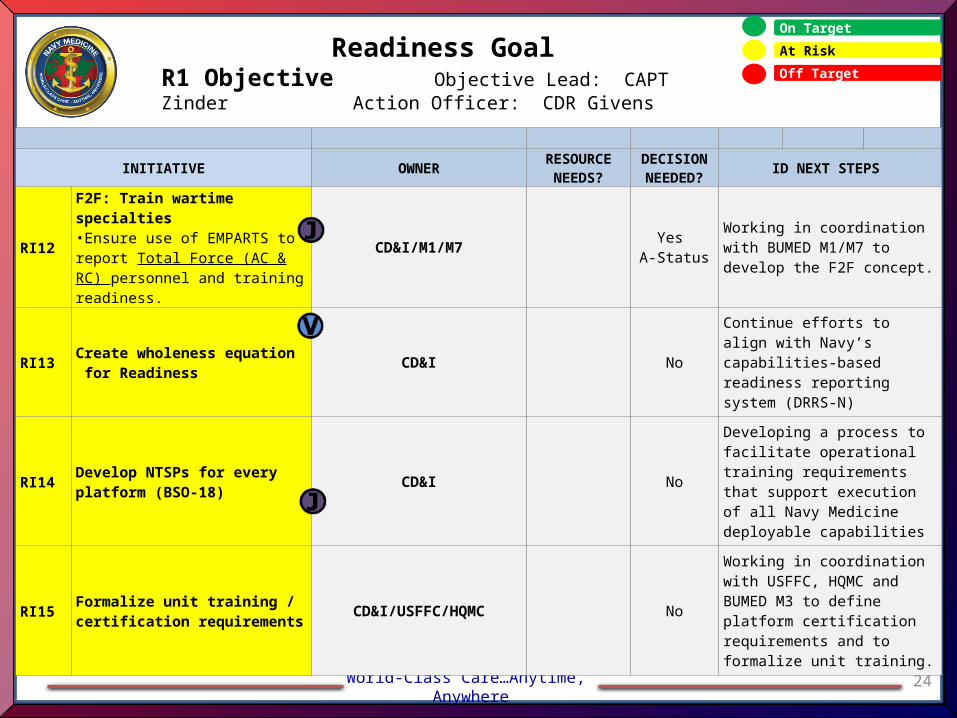
24
Readiness GoalR1 Objective Objective Lead: CAPT Zinder
Action Officer: CDR Givens
On Target
At Risk
Off Target
INITIATIVE OWNER RESOURCE NEEDS?
DECISION NEEDED? ID NEXT STEPS
RI12
F2F: Train wartime specialties•Ensure use of EMPARTS to report Total Force (AC & RC) personnel and training readiness.
CD&I/M1/M7 Yes A-Status
Working in coordination with BUMED M1/M7 to develop the F2F concept.
RI13 Create wholeness equation for Readiness
CD&I No
Continue efforts to align with Navy’s capabilities-based readiness reporting system (DRRS-N)
RI14 Develop NTSPs for every platform (BSO-18)
CD&I No
Developing a process to facilitate operational training requirements that support execution of all Navy Medicine deployable capabilities
RI15 Formalize unit training / certification requirements
CD&I/USFFC/HQMC No
Working in coordination with USFFC, HQMC and BUMED M3 to define platform certification requirements and to formalize unit training.
World-Class Care…Anytime, Anywhere
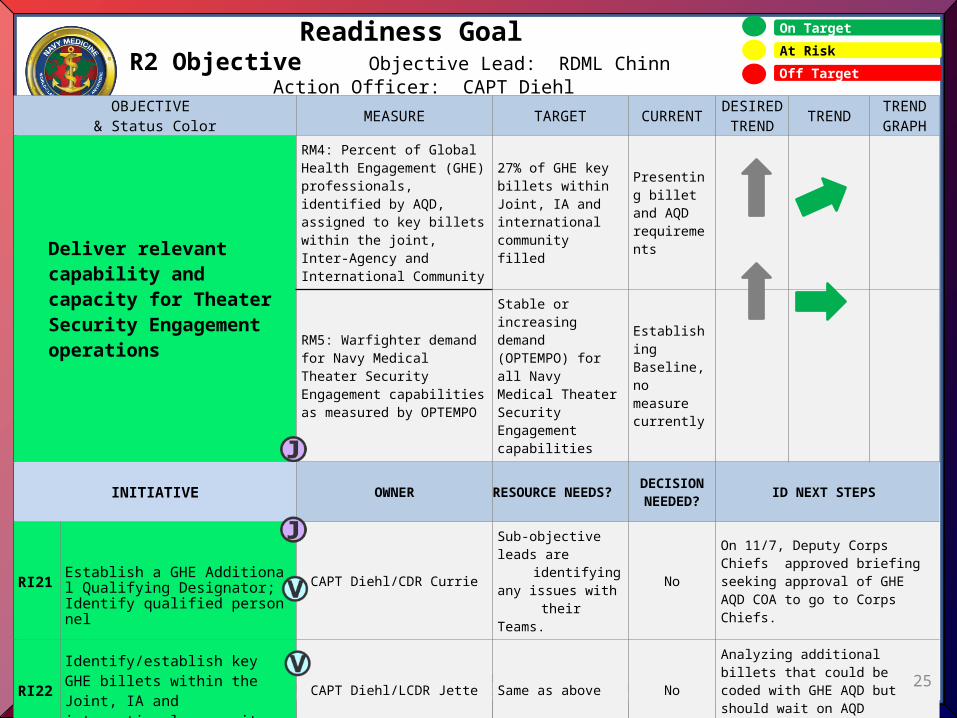
OBJECTIVE & Status Color MEASURE TARGET CURRENT DESIRED
TREND TREND TREND GRAPH
Deliver relevant capability and capacity for Theater Security Engagement operations
RM4: Percent of Global Health Engagement (GHE) professionals, identified by AQD, assigned to key billets within the joint, Inter-Agency and International Community
27% of GHE key billets within Joint, IA and international community filled
Presenting billet and AQD requirements
RM5: Warfighter demand for Navy Medical Theater Security Engagement capabilities as measured by OPTEMPO
Stable or increasing demand (OPTEMPO) for all Navy Medical Theater Security Engagement capabilities
Establishing Baseline, no measure currently
INITIATIVE OWNER RESOURCE NEEDS?DECISION NEEDED?
ID NEXT STEPS
RI21 Establish a GHE Additional Qualifying Designator; Identify qualified personnel.
CAPT Diehl/CDR Currie
Sub-objective leads are identifying any issues with their Teams.
No
On 11/7, Deputy Corps Chiefs approved briefing seeking approval of GHE AQD COA to go to Corps Chiefs.
RI22Identify/establish key GHE billets within the Joint, IA and international community.
CAPT Diehl/LCDR Jette Same as above NoAnalyzing additional billets that could be coded with GHE AQD but should wait on AQD approval.
RI23Identify/establish Navy Medical Theater Security Engagement capabilities by UTC.
CAPT Diehl/CDR ColemanSame as above
NoWorking in coordination with USFFC and BUMED M5/M3 to define GHE Adaptive Force Packages.
RI24
Establish an algorithm for measuring and comparing historical OPTEMPO to current year OPTEMPO.
CAPT Diehl/LCDR Wicker Same as above. No
Developing collection process to establish baseline for OPTEMPO algorithm. Establishing contact and Fellow(LNO ) at Defense Security Cooperation Agency (DSCA). 25
On Target
At Risk
Off Target
Readiness GoalR2 Objective Objective Lead: RDML Chinn
Action Officer: CAPT Diehl
World-Class Care…Anytime, Anywhere
OBJECTIVE & Status Color MEASURE TARGET CURRENT
DESIRED TREND TREND TREND
GRAPH
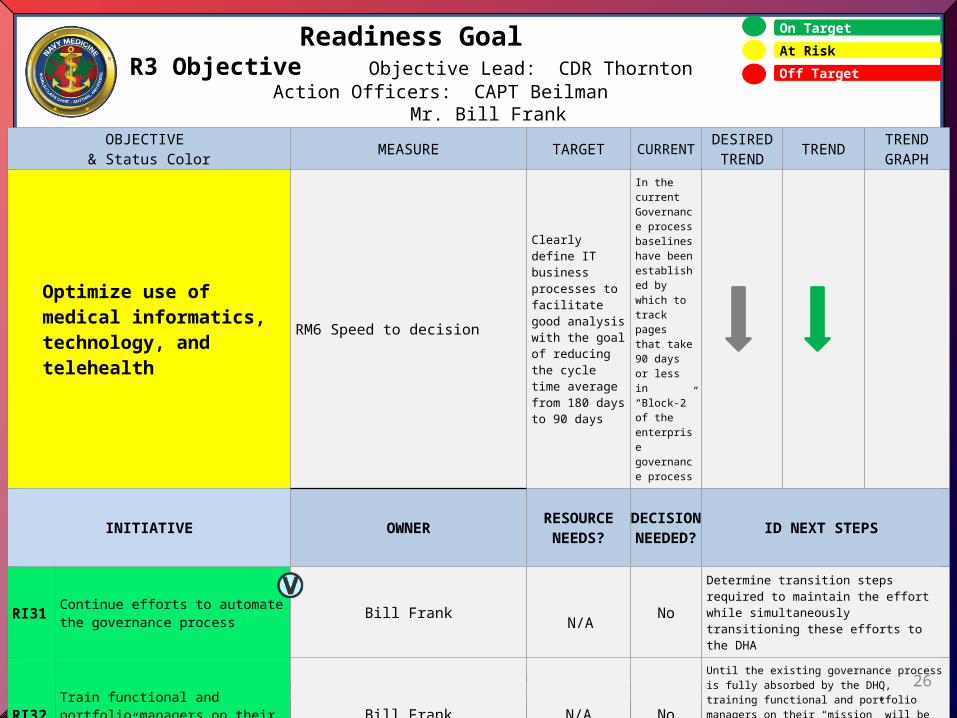
Optimize use of medical informatics, technology, and telehealth
RM6 Speed to decision
Clearly define IT business processes to facilitate good analysis with the goal of reducing the cycle time average from 180 days to 90 days
In the current Governance process baselines have been established by which to track pages that take 90 days or less in “Block-2” of the enterprise governance process
INITIATIVE OWNER RESOURCE NEEDS?
DECISION NEEDED? ID NEXT STEPS
RI31 Continue efforts to automate the governance process Bill Frank N/A No
Determine transition steps required to maintain the effort while simultaneously transitioning these efforts to the DHA
RI32 Train functional and portfolio managers on their “mission” Bill Frank N/A No
Until the existing governance process is fully absorbed by the DHQ, training functional and portfolio managers on their “mission” will be crucial to the process of fielding IT solutions throughout the BSO-18 enterprise.
26
On Target
At Risk
Off Target
Readiness GoalR3 Objective Objective Lead: CDR Thornton
Action Officers: CAPT Beilman Mr. Bill Frank
World-Class Care…Anytime, Anywhere
27
On Target
At Risk
Off Target
OBJECTIVE & Status Color MEASURE TARGET CURRENT
DESIRED TREND TREND TREND
GRAPH
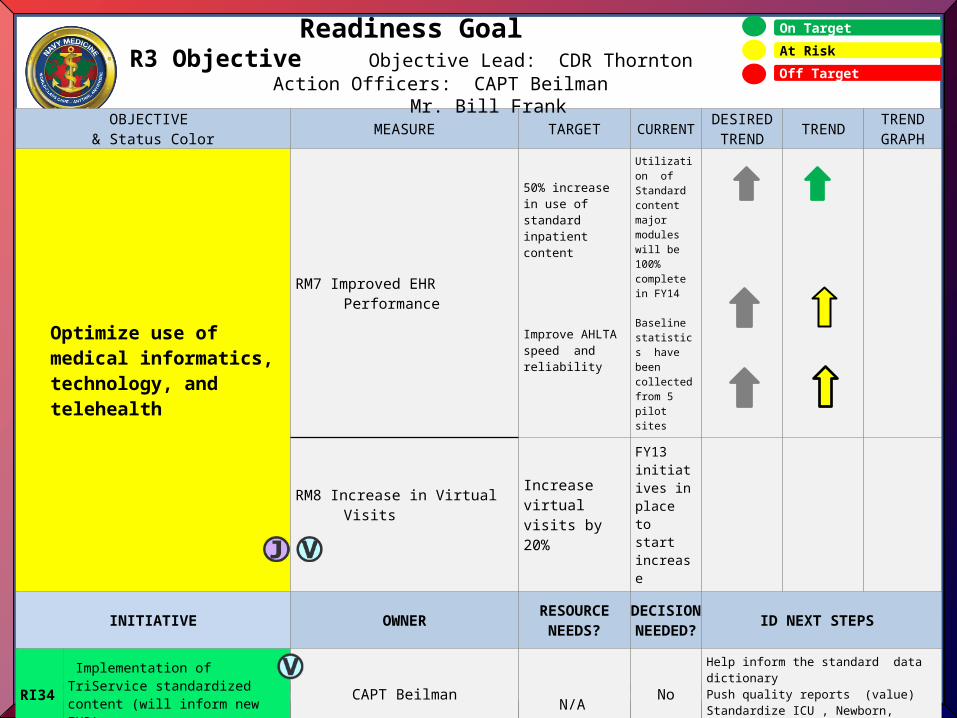
Optimize use of medical informatics, technology, and telehealth
RM7 Improved EHR Performance
50% increase in use of standard inpatient content
Improve AHLTA speed and reliability
Utilization of Standard content major modules will be 100% complete in FY14
Baseline statistics have been collected from 5 pilot sites
RM8 Increase in Virtual Visits Increase virtual visits by 20%
FY13 initiatives in place to start increase
INITIATIVE OWNER RESOURCE NEEDS?
DECISION NEEDED? ID NEXT STEPS
RI34 Implementation of TriService standardized content (will inform new EHR)
CAPT Beilman N/A No
Help inform the standard data dictionaryPush quality reports (value)Standardize ICU , Newborn, Pediatric content
RI35 Spotlight on AHLTA speed and reliability CAPT Beilman N/A No
Baseline established, piloting reports at 5 sites, working on automated report using E2E tool.
RI36 Increase Use of TH Modality CAPT Mitton N/A NoCommunicate strategic direction to Regions ; Seat on MHS Telehealth IPT; ID initial service lines for Navy
Readiness GoalR3 Objective Objective Lead: CDR Thornton
Action Officers: CAPT Beilman Mr. Bill Frank
World-Class Care…Anytime, Anywhere
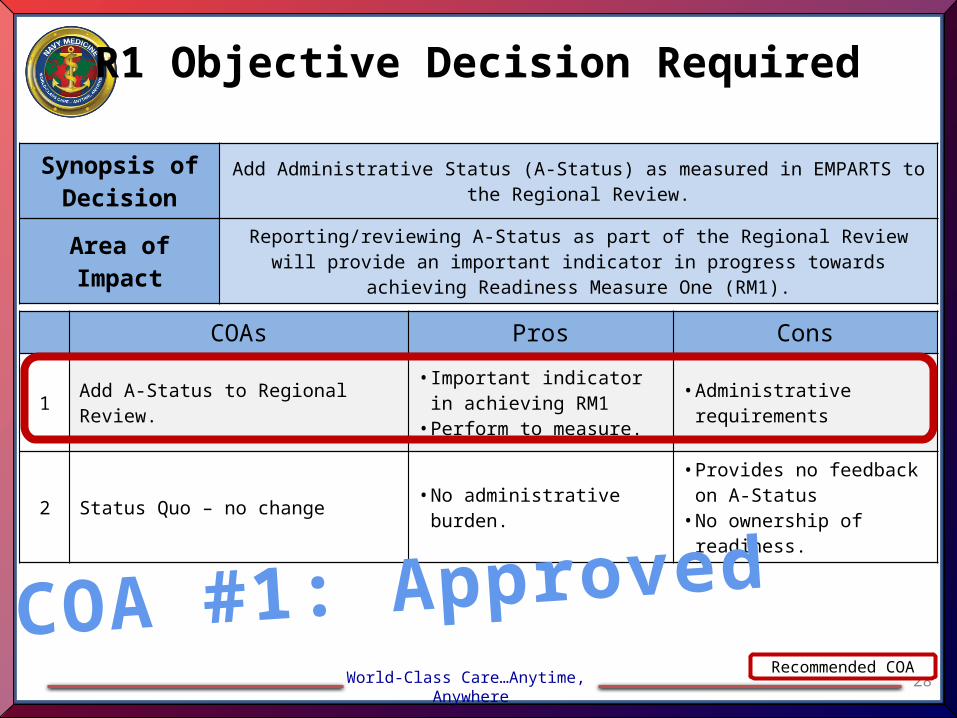
R1 Objective Decision Required
28
COAs Pros Cons
1 Add A-Status to Regional Review.• Important indicator in
achieving RM1• Perform to measure.
• Administrative requirements
2 Status Quo – no change • No administrative burden.• Provides no feedback on A-
Status• No ownership of readiness.
Recommended COA
Synopsis of Decision
Add Administrative Status (A-Status) as measured in EMPARTS to the Regional Review.
Area of Impact Reporting/reviewing A-Status as part of the Regional Review will provide an important indicator in progress towards achieving Readiness Measure One (RM1).
COA #1: Approved

RDML Terry J. Moulton, MSC, USN
RDML Kenneth J. Iverson, MC, USN
23 January 2014
29
Navy Medicine
Strategic Goal:
ValueIn executing Navy Medicine’s mission, we will provide
exceptional value to those we serve by ensuring full and efficient utilization of our services, highest quality care
through best healthcare practices, and lower care costs.
Informational Brief
World-Class Care…Anytime, Anywhere
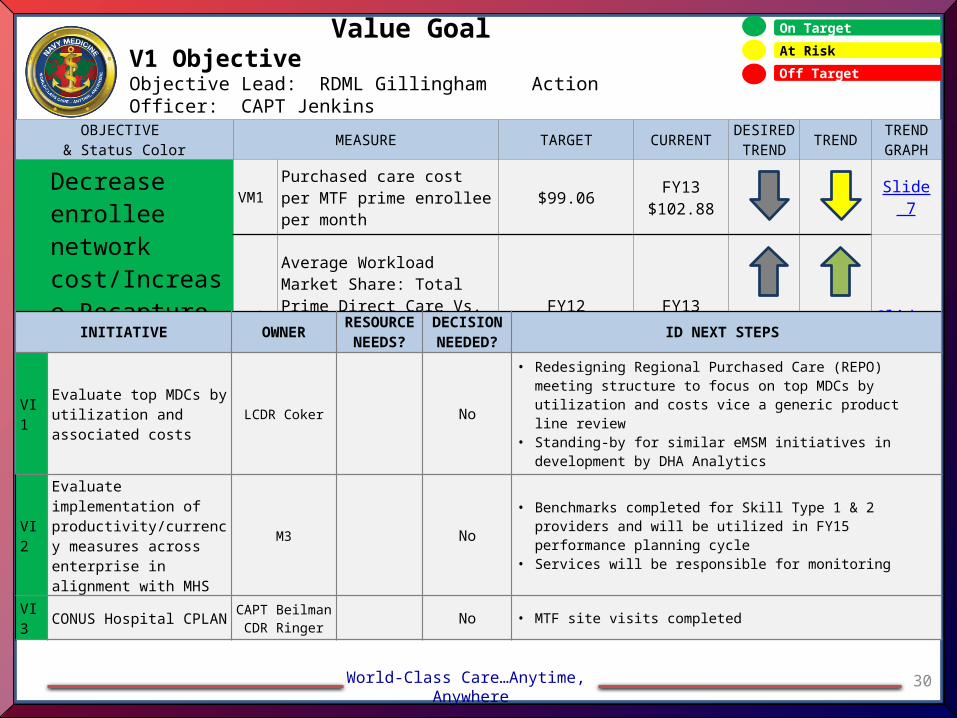
30
On Target
At Risk
Off Target
OBJECTIVE & Status Color MEASURE TARGET CURRENT DESIRED
TREND TREND TREND GRAPH
Decrease enrollee network cost/Increase Recapture of Purchased Care
VM1 Purchased care cost per MTF prime enrollee per month
$99.06FY13
$102.88Slide 7
VM2
Average Workload Market Share: Total Prime Direct Care Vs. Total Prime Care within a Prime Service Area
FY1247%
FY1350%
Slide 8
Value GoalV1 ObjectiveObjective Lead: RDML Gillingham Action Officer: CAPT Jenkins
INITIATIVE OWNER RESOURCE NEEDS?
DECISION NEEDED? ID NEXT STEPS
VI1Evaluate top MDCs by utilization and associated costs
LCDR Coker No
• Redesigning Regional Purchased Care (REPO) meeting structure to focus on top MDCs by utilization and costs vice a generic product line review
• Standing-by for similar eMSM initiatives in development by DHA Analytics
VI2
Evaluate implementation of productivity/currency measures across enterprise in alignment with MHS
M3 No• Benchmarks completed for Skill Type 1 & 2 providers and will be
utilized in FY15 performance planning cycle• Services will be responsible for monitoring
VI3 CONUS Hospital CPLAN CAPT BeilmanCDR Ringer No • MTF site visits completed
World-Class Care…Anytime, Anywhere
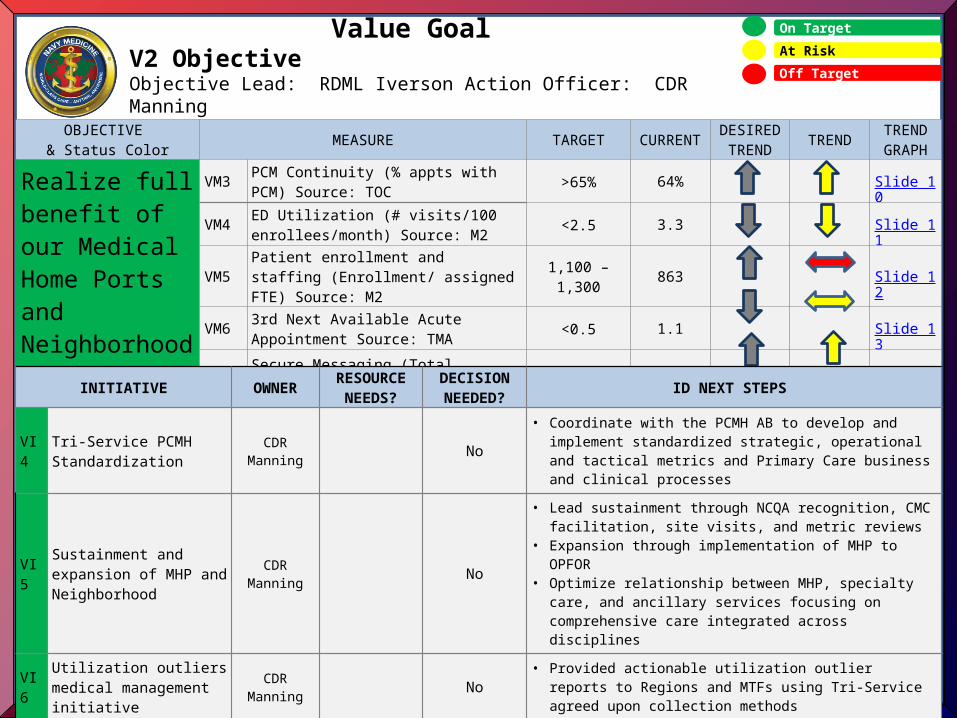
31
On Target
At Risk
Off Target
OBJECTIVE & Status Color MEASURE TARGET CURRENT DESIRED
TREND TREND TREND GRAPH
Realize full benefit of our Medical Home Ports andNeighborhoods
VM3 PCM Continuity (% appts with PCM) Source: TOC >65% 64% Slide 10
VM4 ED Utilization (# visits/100 enrollees/month) Source: M2 <2.5 3.3 Slide 11
VM5 Patient enrollment and staffing (Enrollment/ assigned FTE) Source: M2 1,100 – 1,300 863 Slide 12
VM6 3rd Next Available Acute Appointment Source: TMA <0.5 1.1 Slide 13
VM7 Secure Messaging (Total Connected / Total Enrolled) 40% 27% Slide 14
Value GoalV2 ObjectiveObjective Lead: RDML Iverson Action Officer: CDR Manning
INITIATIVE OWNER RESOURCE NEEDS?
DECISION NEEDED? ID NEXT STEPS
VI4 Tri-Service PCMH Standardization
CDR Manning No
• Coordinate with the PCMH AB to develop and implement standardized strategic, operational and tactical metrics and Primary Care business and clinical processes
VI5Sustainment and expansion of MHP and Neighborhood
CDR Manning No
• Lead sustainment through NCQA recognition, CMC facilitation, site visits, and metric reviews
• Expansion through implementation of MHP to OPFOR• Optimize relationship between MHP, specialty care, and
ancillary services focusing on comprehensive care integrated across disciplines
VI6 Utilization outliers medical management initiative
CDR Manning No • Provided actionable utilization outlier reports to Regions and
MTFs using Tri-Service agreed upon collection methods
VI7 Effective implementation of Nurse Advice line
CDR Manning No • Successfully implement NAL by April, 2014
World-Class Care…Anytime, Anywhere
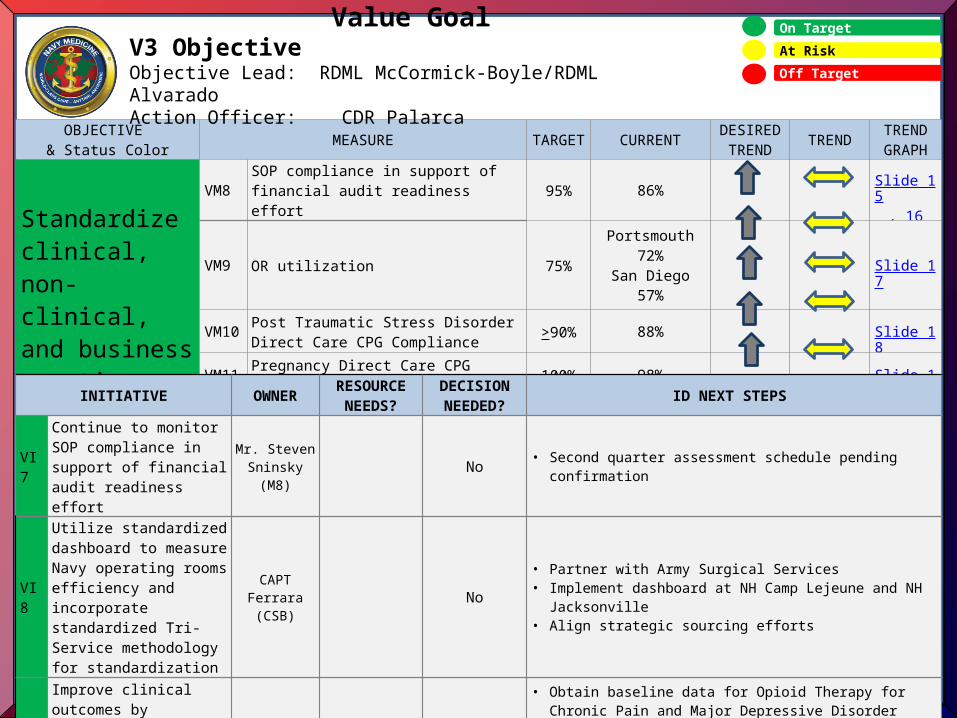
32
On Target
At Risk
Off Target
OBJECTIVE & Status Color MEASURE TARGET CURRENT DESIRED
TREND TREND TREND GRAPH
Standardize clinical, non-clinical, and business practices
VM8 SOP compliance in support of financial audit readiness effort 95% 86% Slide 15,
16
VM9 OR utilization 75%Portsmouth 72%San Diego 57% Slide 17
VM10 Post Traumatic Stress Disorder Direct Care CPG Compliance >90% 88% Slide 18
VM11 Pregnancy Direct Care CPG Compliance 100% 98% Slide 19
VM12 Low Back Pain CPG Compliance TBD 77% Slide 20
Value GoalV3 ObjectiveObjective Lead: RDML McCormick-Boyle/RDML AlvaradoAction Officer: CDR Palarca
INITIATIVE OWNER RESOURCE NEEDS?
DECISION NEEDED? ID NEXT STEPS
VI7
Continue to monitor SOP compliance in support of financial audit readiness effort
Mr. Steven Sninsky (M8) No • Second quarter assessment schedule pending confirmation
VI8
Utilize standardized dashboard to measure Navy operating rooms efficiency and incorporate standardized Tri-Service methodology for standardization
CAPT Ferrara (CSB)
No
• Partner with Army Surgical Services• Implement dashboard at NH Camp Lejeune and NH
Jacksonville• Align strategic sourcing efforts
VI9
Improve clinical outcomes by minimizing practice variation through adherence to evidence-based care
CAPT Ferrara No
• Obtain baseline data for Opioid Therapy for Chronic Pain and Major Depressive Disorder CPGs
• Finalize targets and outcome measures for PTSD, Pregnancy and Low Back Pain CPGs
• Execute CPG Communications Plan
Classification: FOUO
Senior Strategy BoardDecision Brief
Goal Lead: RDML Raquel Bono, MC, USN
Vice Goal Lead: RADM Bruce Doll, DC, USN
December 18, 2013
33
JointnessWe lead Navy Medicine to jointness and improved
interoperability by pursuing the most effective ways of mission accomplishment.
World-Class Care…Anytime, Anywhere
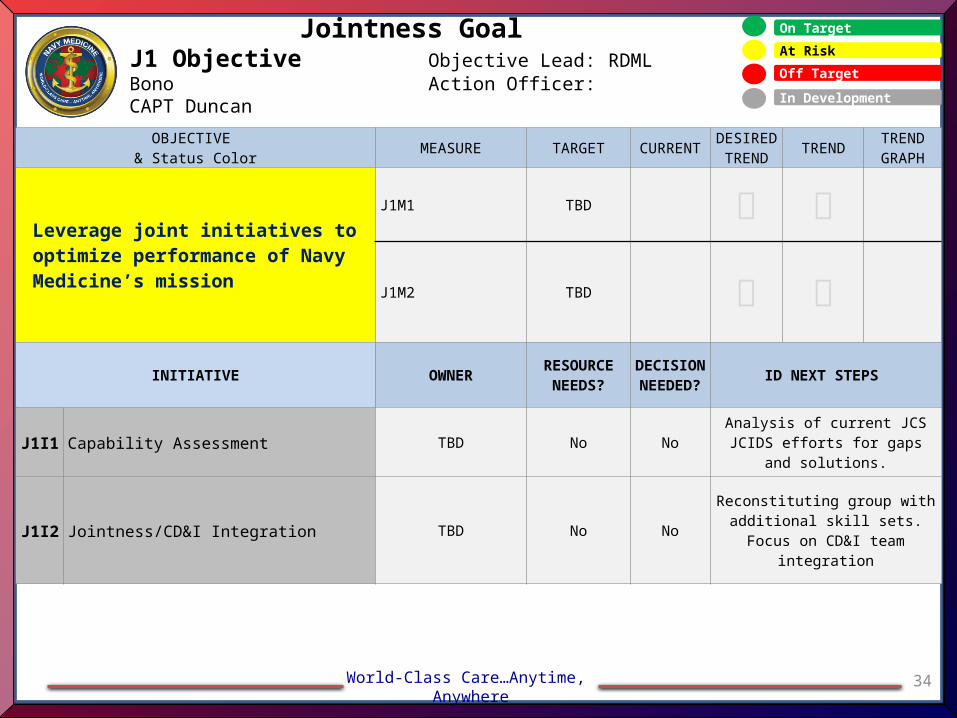
34
On Target
At Risk
Off Target
OBJECTIVE & Status Color MEASURE TARGET CURRENT DESIRED
TREND TREND TREND GRAPH
Leverage joint initiatives to optimize performance of Navy Medicine’s mission
J1M1 TBD
J1M2 TBD
INITIATIVE OWNER RESOURCE NEEDS?
DECISION NEEDED? ID NEXT STEPS
J1I1 Capability Assessment TBD No No Analysis of current JCS JCIDS efforts for gaps and solutions.
J1I2 Jointness/CD&I Integration TBD No NoReconstituting group with
additional skill sets. Focus on CD&I team integration
Jointness GoalJ1 Objective Objective Lead: RDML Bono
Action Officer: CAPT Duncan In Development
World-Class Care…Anytime, Anywhere
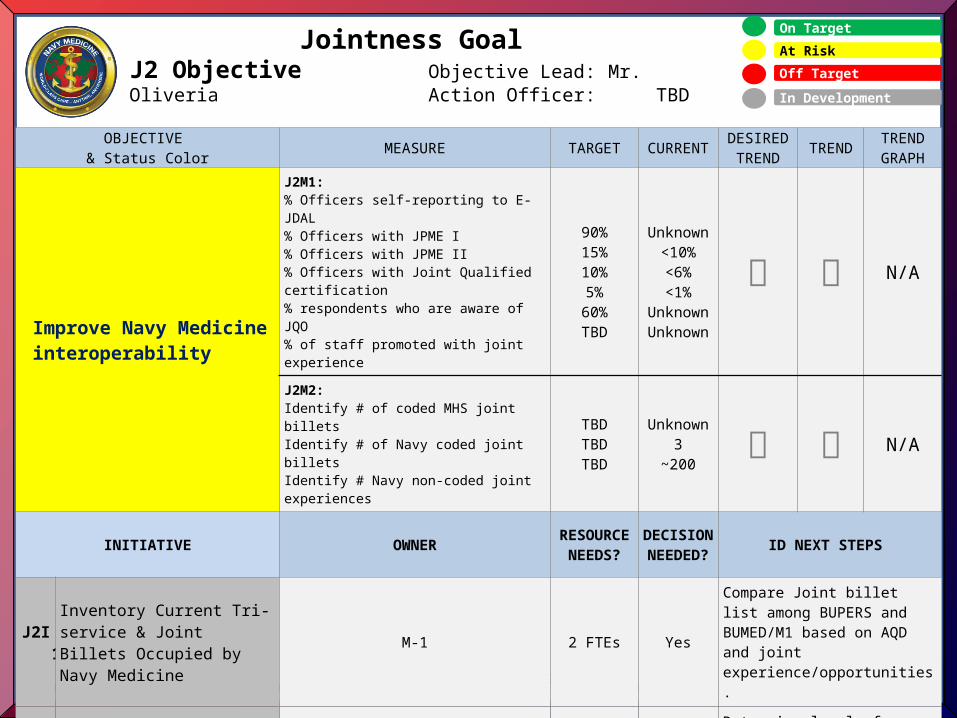
35
On Target
At Risk
Off Target
Jointness GoalJ2 Objective Objective Lead: Mr. Oliveria
Action Officer: TBD
OBJECTIVE & Status Color MEASURE TARGET CURRENT DESIRED
TREND TREND TREND GRAPH
Improve Navy Medicine interoperability
J2M1:% Officers self-reporting to E-JDAL% Officers with JPME I% Officers with JPME II% Officers with Joint Qualified certification% respondents who are aware of JQO% of staff promoted with joint experience
90%15%10%5%
60%TBD
Unknown<10%<6%<1%
UnknownUnknown
N/A
J2M2:Identify # of coded MHS joint billetsIdentify # of Navy coded joint billetsIdentify # Navy non-coded joint experiences
TBDTBDTBD
Unknown3
~200 N/A
INITIATIVE OWNER RESOURCE NEEDS?
DECISION NEEDED? ID NEXT STEPS
J2I1Inventory Current Tri-service & Joint Billets Occupied by Navy Medicine
M-1 2 FTEs Yes
Compare Joint billet list among BUPERS and BUMED/M1 based on AQD and joint experience/opportunities.
J2I2Determine Desired Joint Billets to Fill M-00C 1 FTE Yes
Determine level of interest in pursuing Joint billets.Identify a Navy LNO to cooperate with Army/AF/DHA about Joint billets.
In Development
World-Class Care…Anytime, Anywhere
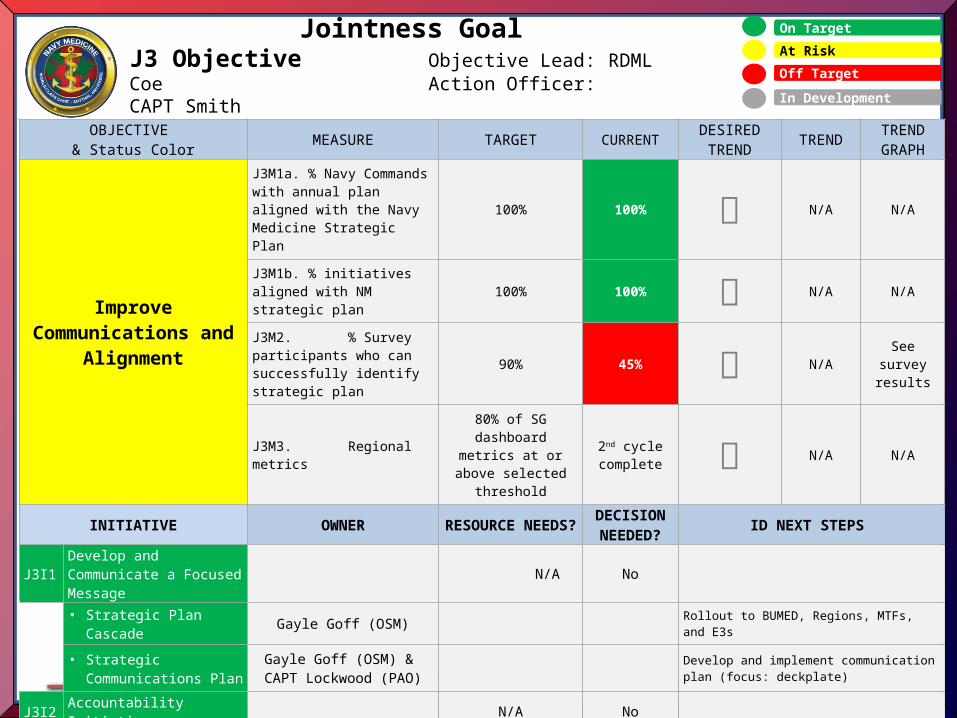
36
On Target
At Risk
Off Target
Jointness GoalJ3 Objective Objective Lead: RDML Coe
Action Officer: CAPT Smith
OBJECTIVE & Status Color MEASURE TARGET CURRENT
DESIRED TREND TREND TREND
GRAPH
Improve Communications and
Alignment
J3M1a. % Navy Commands with annual plan aligned with the Navy Medicine Strategic Plan
100% 100% N/A N/A
J3M1b. % initiatives aligned with NM strategic plan
100% 100% N/A N/A
J3M2. % Survey participants who can successfully identify strategic plan
90% 45% N/ASee survey
results
J3M3. Regional metrics
80% of SG dashboard metrics at or above selected threshold
2nd cycle complete N/A N/A
INITIATIVE OWNER RESOURCE NEEDS?
DECISION NEEDED? ID NEXT STEPS
J3I1 Develop and Communicate a Focused Message
N/A No
• Strategic Plan Cascade Gayle Goff (OSM) Rollout to BUMED, Regions, MTFs, and E3s
• Strategic Communications Plan
Gayle Goff (OSM) & CAPT Lockwood (PAO)
Develop and implement communication plan (focus: deckplate)
J3I2 Accountability Initiative N/A No
• Metrics Governing Board Gayle Goff (OSM) Continue to refine metrics; improve automation
• Regional Performance Review
COS Refreshed review reflects FY14 strategic changes; NME will undergo review in January
J3I3 BUMED Reinvention CAPT Hall None at this time
Single digits continue to define BUMED mission; ADCs will take vision and develop organizational constructs
In Development