Embed Size (px)
Citation preview

1
National Rural Health Mission:
Convergence with ICDS

2
National Rural Health Mission
• The Prime Minister launched a National Rural Health Mission on 12th April 2005.
• The Mission is for a period of 7 years (2005-12).
• The Outlay for NRHM for 2005-06 is over Rs.6700 crore.
• High focus on 18 States (8 EAG, 8 North East, Jammu & Kashmir and Himachal Pradesh)
• Reproductive and Child Health Programme (RCH-II) is an important component of NRHM

3
Reproductive Child Health Programme
RCH-II is the Flagship programme under NRHM. Its strategies include:
• Maternal Health – Institutional deliveries EmOC, BCC, Mobilization Strategies, improved coverage and quality of ANC, skilled care to Pregnant women, Post -partum care at Community level.
• Child health - UIP, IMNCI
• Population Stabilization – contraceptive choice, private sector intervention, stimulating demand for FP services
• Urban and tribal health – similar initiatives with special focus disadvantages

4
NRHM Goals • To provide effective health care to rural population
(especially for Women & Children).• Improve access to health care.• Enable community ownership and demand for
services.• Strengthen public health system for efficient service
delivery.• Enhance equity and accountability.• Promote decentralization.• Mainstream AYUSH.• Integration with other sectors (ICDS, Sanitation,
Drinking water )• Focus to change from Outlays to Outcomes.

5
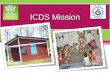
NRHM – The Concept
Health Health Determinants
RCH-II NDCP
AYUSH General Curative
Care
Nutrition Sanitation & Hygiene
Drinking Water Supply

6
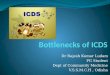
National Steering Group
Mission Steering Group
Empowered Programme Committee
State Health Mission
District Health Mission ------------Rogi Kalyan Samitis
Village Health Committee
Village Health Committee
Village Health Committee
Mission Directorate
Institutional Framework
Panchayat

7
Core Strategies • Train and enhance capacity of PRIs to own,
control and manage public health services.• Promote access to healthcare to household
through the female Accredited Social Health Activist (ASHA).
• Health Plan for each village.• Untied fund for Sub-centre.• Upgrading all CHCs to Indian Public Health
Standards.• Integrating relevant vertical Health and Family
Welfare programmes at National, State and District levels.
• Mainstreaming AYUSH. – revitalizing local health traditions.

8
Intersectoral Convergence under NRHM
1) Mission Steering Group chaired by Union Minister for Health and Family Welfare. Dy. Chairman, Planning Commission, Minster for HRD, PR & Rural Development members.
2) Empowered Programme Committee has representatives from cognate Ministries - DWCD,PR, RD, NE and AYUSH
3) Committee on Intersectoral Convergence constituted under Mission Director.
4) Preparation and Implementation of an inter-sectoral District Health Plan prepared by the District Health Mission, including drinking water, sanitation & hygiene and nutrition.
5) Theme Papers on Convergence shared with DWCD, PRI TSC, NACO
6) In-principle agreement on NRHM framework
7) Common strategy being evolved for IEC & Training among DWCD, DoHFW & PR

9
ASHA under NRHM
• Community based functionary - a change agent of health in a village.
• First port of call for any health related demand.
• Create awareness and provide information to the community.
• Counsel women on birth, safe delivery, breast feeding etc.

10
ASHA under NRHM (II)• Mobilize the community and facilitate health
related services.• Work with the village health and sanitation
committee of Gram Panchayat.• Arrange escort / accompany pregnant women
and children requiring any health services.• Provide primary medical care.• Will be equipped with Drug Kit• Promote construction of household toilets
under Total Sanitation Campaign.

11
Village Level Convergence under NRHM
1) Anganwari to be hub of mother and child care activity at village level
2) Village Health Team: ANM, AWW, ASHA, SHG etc. under Village Health & Sanitation Committee of the Gram Panchayati
3) Monthly Health Camp at Anganwari to promote ANC, PNC, Universal Immunisation, Nutrition, Micronutrient supplementation – ASHA to support AWW in mobilising pregnant women and infants.
4) AWW to be the Mentor for ASHA 5) AWW will be the depot holder for drug kits
and will be issuing them to ASHAs.

12
Micronutrient Deficiency
1) Micronutrients of Public Health significance: Iron, Iodine, Vitamin A & Zinc
2) Three strategies for correcting micronutrient deficiencies are:
* Supplementation
* Fortification
* Dietary diversification
3) Convergence between ICDS & Health and Family Welfare important for strategies on dietary diversification and supplementation.

13
Government Programmes for Nutrition Intervention
Integrated Child Development Scheme (ICDS) Mid Day Meal Programme (MDMP) Wheat Based Programme (WBP) Reproductive and Child Health Programme for
Iron Folic Acid and Vitamin ‘A’ supplementation. National Iodine Deficiency Disorders Control
Programme (NIDDCP) Pilot Programme against Micronutrient
Malnutrition for School children, adolescents etc introduced in 1995 - to assess levels of Iron, Vitamin A and Zinc deficiency.
Notification to ban sale of non-iodated salt issued on 27.5.2005

14
Micronutrient Programmes and Convergence under RCH & ICDS
• Vitamin ‘A’ Deficiency– The AWW / ASHA to bring children to
Anganwadi Centres or health Sub-centres for supplementation of Vitamin ‘A’ by ANM.
– ANM, ASHA and AWW to create awareness about vitamin ‘A’ deficiency.

15
IRON DEFICIENCY ANAEMIA
• AWW / ASHA & ANM to distribute iron folic acid tablets to pregnant and lactating mothers.
• Educate the consequences of anaemia.
• Awareness about regular consumption of fruits and vegetables.
• Promote good food habits.

16
IODINE DEFICIENCY DISORDERS
• AWW, ASHA / ANM to educate public about various iodine deficiency disorders.
• Promote regular consumption of iodated salt.
• Demonstrate qualitative testing of house hold salt.

17
OPPORTUNITIES OF CONVERGENCE WITH DWCD AND MOH&FW
• Mutual Institutional support by both the Ministries for Women and Child programme
• Capacity building of functionaries of both departments.
• Identification and training of village level community workers.
• Joint training of health and ICDS functionaries and usage of common facilities.
• Fixed health and nutrition days block level resource mapping organised jointly by AWW/ANM/ASHA
• Village Health Plan to include ICDS/Health components
• Community based monitoring system for ICDS and health programmes.

18
Immediate Action Points• Expression of general support for NRHM particularly the
ASHA to be mentored by the Anganwari system.• State level meeting between Secretary HFW and DWCD and
issuance of Guidelines on common goals for NRHM and National ICDS program
• Guidelines for Common Training Program• Setting up of State Level Task Force for Common IEC
Strategy.• Setting up Convergence Mechanism between Institutes of
Training of DWCD and HFW for development of common training material, programme, curriculum etc.
• Discussion about financial compensation to AWW for mentoring role.
• Physical infrastructure at Anganwari by Health Sector• Preparation of District Plan for Health and Nutrition• Quarterly Joint Review Mechanism to monitor progress at all
levels – Block, District, State and National

19
Medium Term Plan
• Health Data System including e-moding to be made available to ICDS
• Convergence of management of Stores, Training Institutions and Physical Infrastructure including residential colonies, fund flow, logistics and supplies for better efficiencies.

20
THANK YOU