Embed Size (px)
Citation preview
1
MS Patient CasesIran
May 2007Jack Burks, MD
Clinical Professor, NeurologistUniversity of Nevada School of Medicine
Reno, Nevada
Vice President/Chief Medical OfficerMultiple Sclerosis Association of America
PresidentMultiple Sclerosis Alliance

2
Important Issues in Treating MS: Illustrative Patient Cases
When to start therapy? How to decide on which therapy is the most
effective for a specific patient? How should patients be monitored to
determine good/poor Rx. responses? What is a poor response to treatment and
how should it be managed? How are side effects best managed? What is the future for current and emerging
therapies?

9
Patient 1:Deciding When to Initiate Treatment
10
Patient 1: Deciding When to Initiate Treatment
History 26-year-old secretary, mother of twins; no history of MS
or SLE Over 5-day period notices double vision, weakness in
the right arm and leg, unsteady gait, fatigue, and difficulty with memory when multitasking
Exam Diplopia on right gaze, mild right hemiparesis, and
wide-based, slightly ataxic gait Normal bedside mental status Husband stresses patient’s recent disorganization
11
Patient 1: Deciding When to Initiate Treatment
MRI 6 periventricular lesions, 1 pontine lesion, 1 high
cervical lesion on T2 MRI 4 GAD+ lesions
Lab work All negative Spinal tap not done

12
Neurologist’s Assessment
Patient had a CIS but does not meet the criteria for CDMS, could be ADEM
Steroids should be used in this patient, but a DMT is not appropriate at this stage
Is this the appropriate diagnosis? What goes into the decision process
to determine the appropriateness of utilizing a DMT?

13
Treat Early! Diagnosis of MSin Clinical Isolated Syndrome (CIS)
Lesions in Time and Space
Clinical Presentation Space Time(Add’l Requirements) (Add’l Requirements)
2 attacks; 2 locations No No
2 attacks; 1 location MRI abnormal or No2 MRI lesions + CSF
1 attack; 2 locations No MRI 3 months or
second attack
1 attack; 1 location (CIS) MRI abnormal or MRI 3 months 2 MRI lesions + CSF or second attack
Ref: McDonald, I. Annals of Neurology 2002
14
McDonald MRI Criteria for Dissemination in Time
First scan 3 months after clinical event New Gadolinium lesion
• Must not be the same site No new Gadolinium lesion:
• Repeat MRI at ≥3 months New T2 or gadolinium lesion
McDonald WI et al. Ann Neurol. 2001;50:121-127.The exact relationship between MRI findings and clinical status of patients is not completely understood.
15..
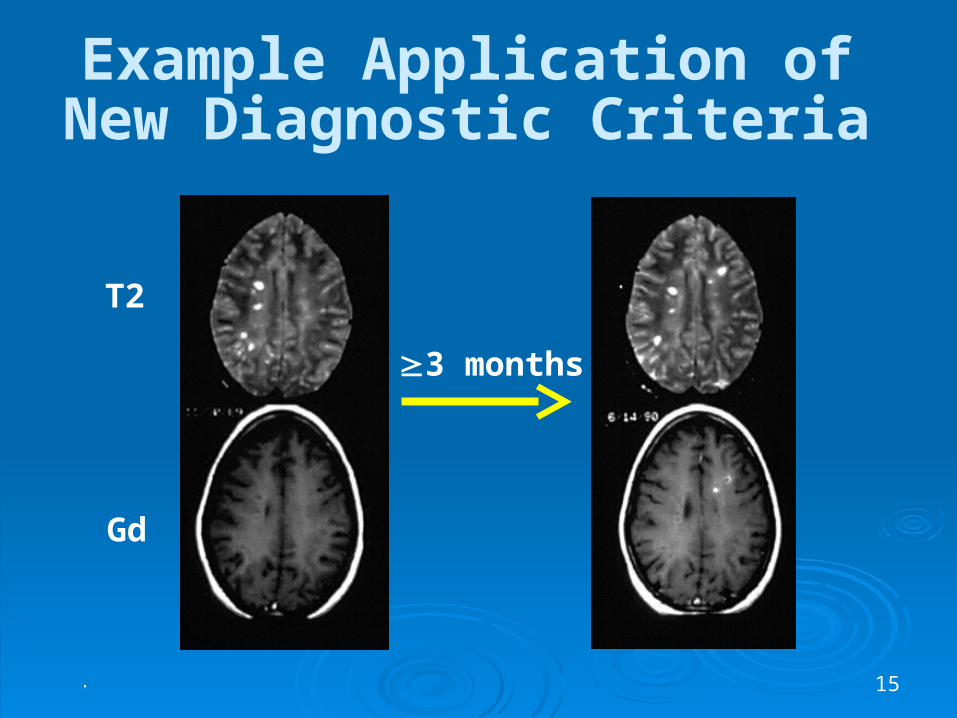
Example Application ofNew Diagnostic Criteria
3 months
T2
Gd
16
Polman Revision of McDonald Criteria (2005)
New T-2 MRI lesions at 1 month after CIS MRI (lesions in time)
Spinal cord lesions can be considered as a brain infratentorial and, if Gd-enhancing, can substitute for a brain Gd-enhancing lesion
Polman CH et al. Ann Neurol. 2005;58:840-846.
17
Patient 1: Follow-up After being treated with a course of IV
Solu-Medrol, the patient’s symptoms improved
At a 3-month follow-up visit: Clinical signs resolved Fatigue and memory problems less Neurology exam normal Previous GAD+ lesions had resolved 1 new GAD+ lesion and 2 new T2 lesions
18
Neurologist’s Assessment at Follow-up
Patient meets the McDonald criteria for CDMS/RRMS
The patient was started on treatment Do you agree with decision to treat? How do you decide which DMT to utilize in this
situation? Is there a difference or are they all the same? What do Evidence Based Medicine Analysis
and Class I Head to Head Trial indicate?
19
Patient was treated with IFNβ-1b
BENEFIT Trial
17 year follow-up data
AAN Treatment Guidelines
20Kappos L, Polman CH, Freedman MS, et al, for the BENEFIT Study Group. Treatment with interferon beta-1b delays conversion to clinically definite and McDonald MS in patients with clinically isolated syndromes. Neurology. 2006;67:1242-1249.
II. BENEFIT: Betaferon in CIS Objective:
To assess efficacy, safety, and tolerability of every-other-day (EOD) interferon beta-1b treatment in patients with a clinically isolated syndrome (CIS) suggestive of multiple sclerosis
Study design: Randomized, double-blind, placebo-controlled, parallel-group,
multicenter study with 468 patients Participants had experienced a first clinical demyelinating event, and
at least 2 clinically significant MRI-detected brain lesions Patients received Betaferon 250 µg or placebo SC EOD for 24 months
or until CDMS
Primary endpoints: Time to CDMS according to the modified Poser criteria Time to diagnosis of MS according to McDonald diagnostic criteria
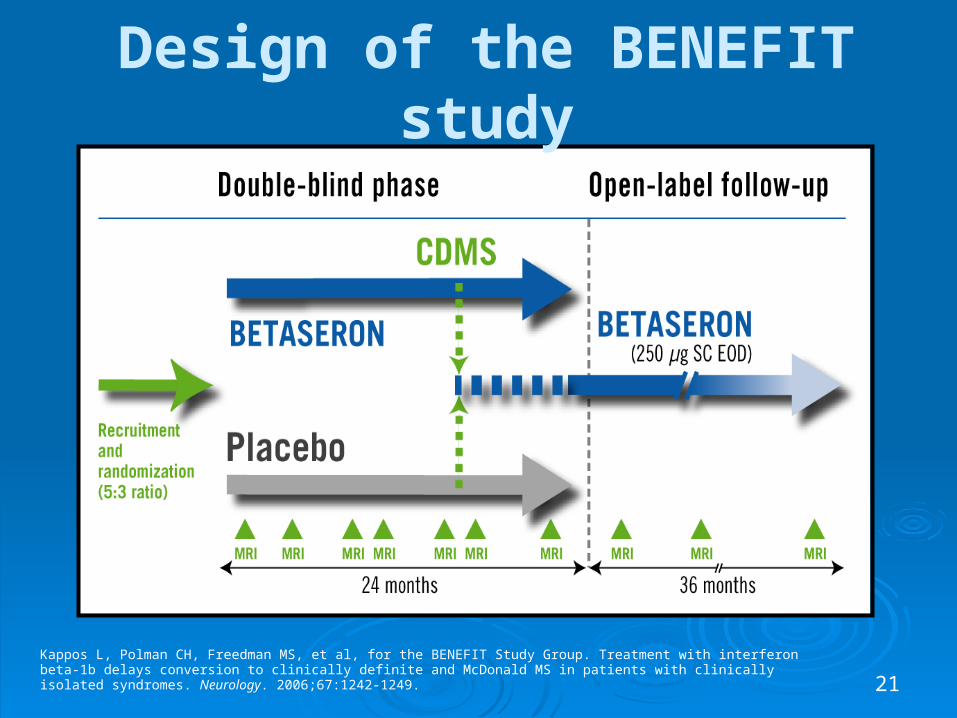
21Kappos L, Polman CH, Freedman MS, et al, for the BENEFIT Study Group. Treatment with interferon beta-1b delays conversion to clinically definite and McDonald MS in patients with clinically isolated syndromes. Neurology. 2006;67:1242-1249.
Design of the BENEFIT study
22
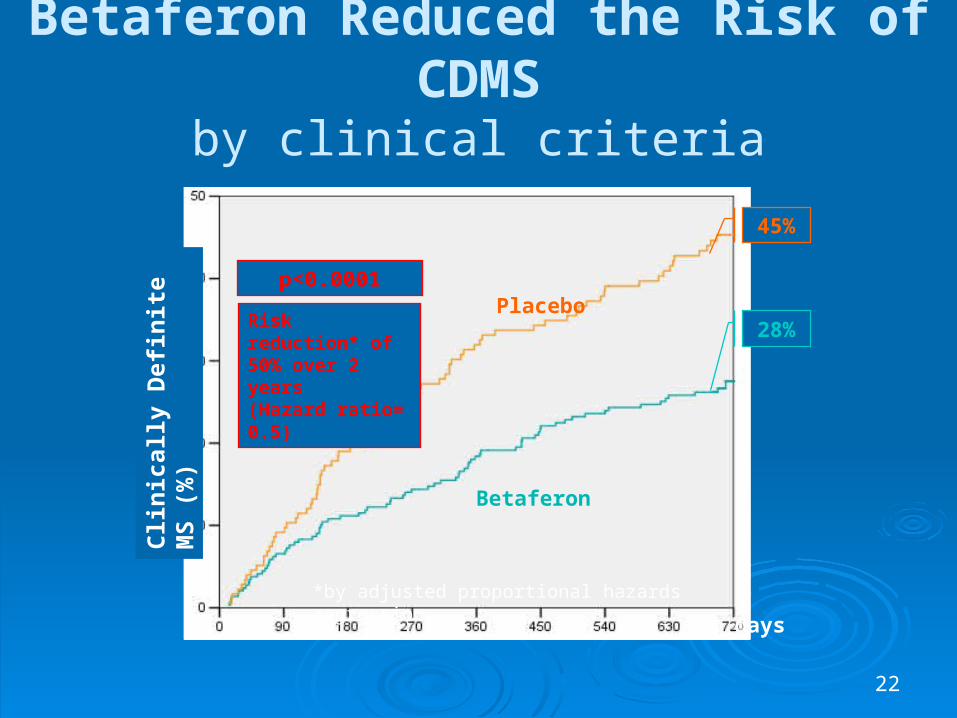
28%
45%
Placebo
Betaferon
Risk reduction* of 50% over 2 years(Hazard ratio= 0.5)
*by adjusted proportional hazards regression
days
p<0.0001
Betaferon Reduced the Risk of CDMSby clinical criteria
Cli
nic
ally
Def
init
e M
S (
%)
23
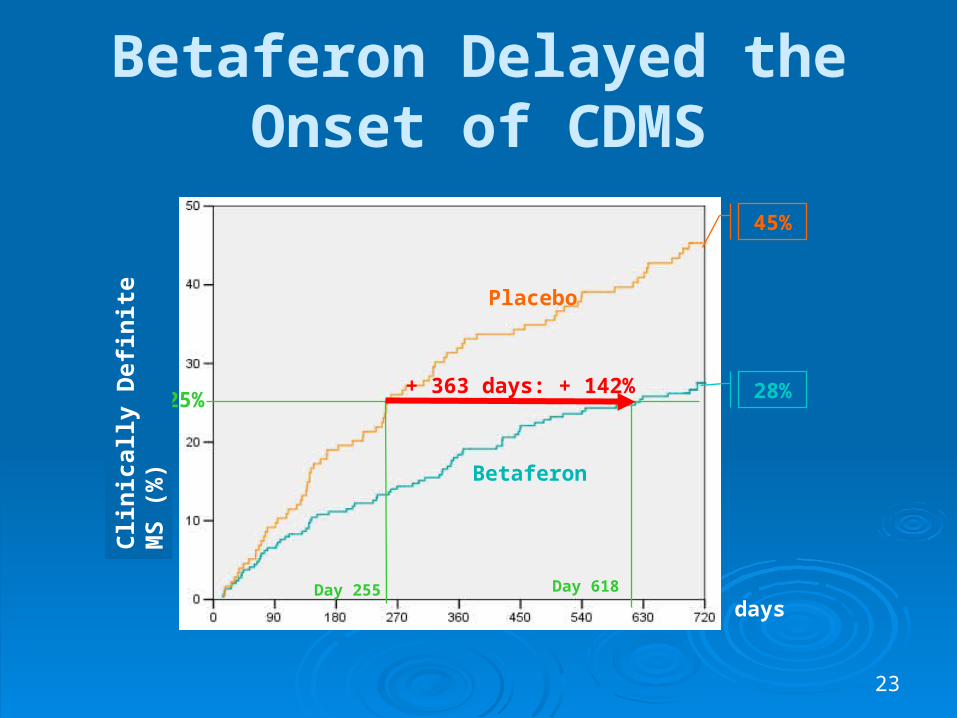
28%
45%
Placebo
Betaferon
25%+ 363 days: + 142%
Day 255 Day 618
Betaferon Delayed the Onset of CDMS
Cli
nic
ally
Def
init
e M
S (
%)
days
24
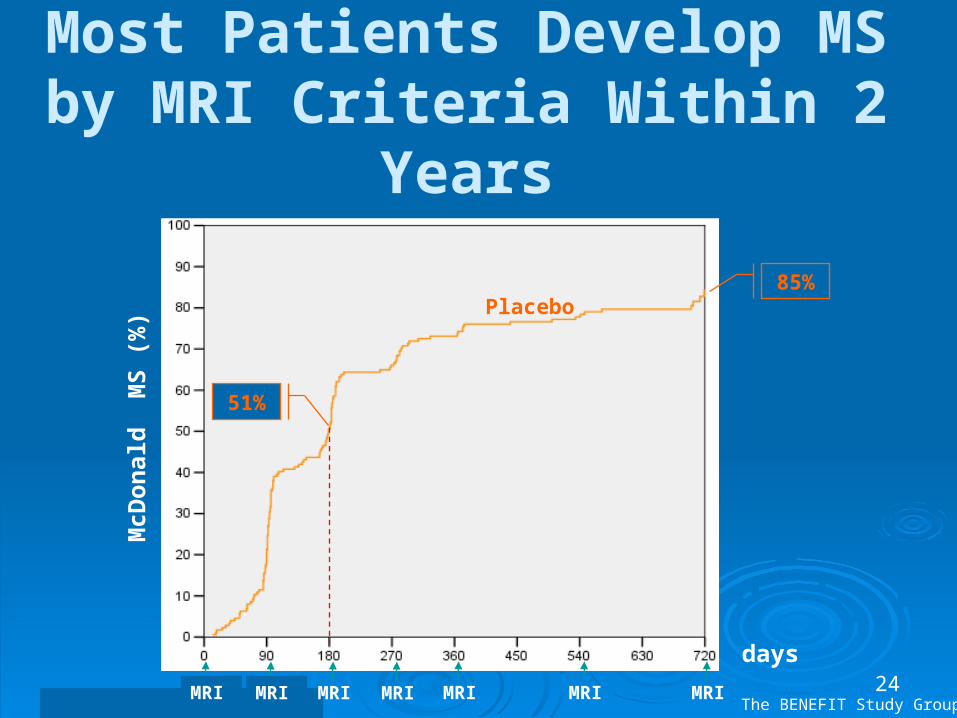
Most Patients Develop MS by MRI Criteria Within 2 Years
McD
on
ald
M
S (
%)
days
MRI MRI MRI MRI MRI MRIMRI
Placebo
51%
85%
The BENEFIT Study Group
25
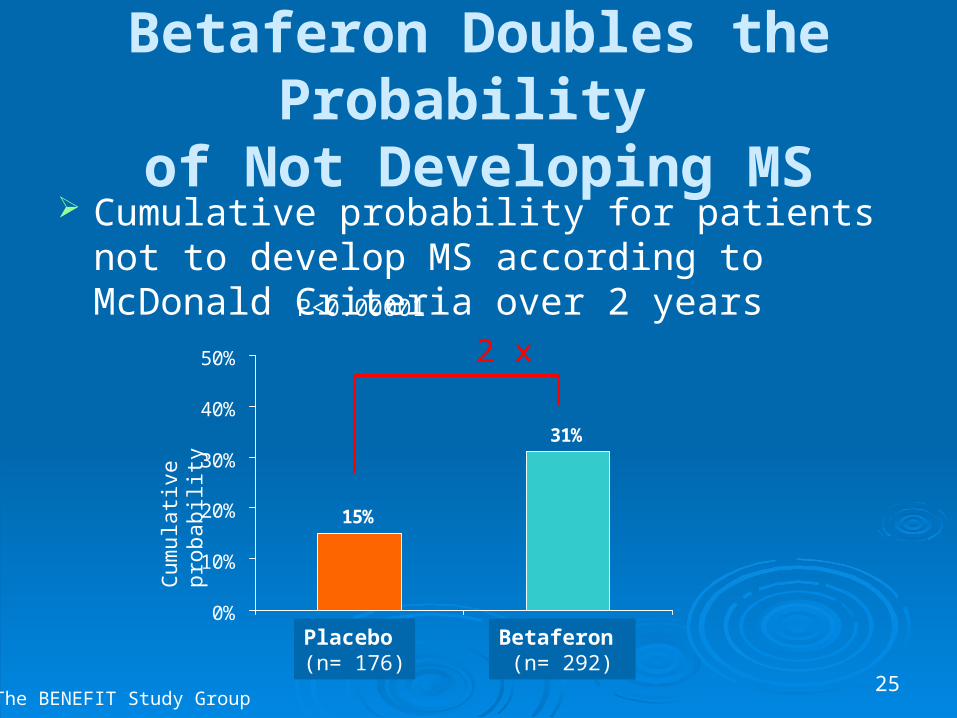
Betaferon Doubles the Probability of Not Developing MS
Cumulative probability for patients not to develop MS according to McDonald Criteria over 2 years
15%
31%
0%
10%
20%
30%
40%
50%
Placebo Betaferon
Cum
ulat
ive
prob
abili
ty
Placebo (n= 176)
Betaferon (n= 292)
2 x
The BENEFIT Study Group
P<0.00001
26
BENEFIT Trial: Early vs. Delayed Treatment: 3 year follow-up (2007)
Confirmed Progression (EDSS) Placebo then Betaferon 24% Betaferon from CIS 16% 40% decrease of confirmed progression with
early Betaferon treatment! (P=0.02)
No effect of NAbs on clinical outcomes

27The BENEFIT Study. Betaferon® in newly emerging multiple sclerosis for initial treatment: Clinical results [poster].
BENEFIT study: Discontinuation rates
Only 2.7% of Betaferon patients discontinued due to adverse events*
The majority of patients experienced no flu-like symptoms over 2 years
Factors for low rate of discontinuation include:
Dosage Titration
Analgesics: before injection
*From an analysis of patients who adhere to study protocol.
28
Lessons from BENEFIT Trial Placebo patients studied in BENEFIT had a high risk
of progressing to MS according to the McDonald criteria 85% within 2 years, 51% after 6 months
In the BENEFIT study, every-other-day Betaferon significantly Reduced the risk of progression to CDMS (by 50%) Prolonged the time to CDMS by 1 year (+142%)
(based on the 25th percentiles) Delayed EDSS disability scores at 3 years
Every-other-day Betaferon is well tolerated and well accepted in patients

29
17 year follow-up Rationale IFNB-1b was approved for the treatment of relapsing forms of
multiple sclerosis (MS) based on the results of a double-blind placebo-controlled study in which patients received placebo or IFNB-1b for 104 weeks and were followed up for up to 5 years
Results of this pivotal study showed IFNB-1b to be effective and well tolerated over this period
There are few data regarding the long-term benefit of IFNB treatment for more than 10 years. However, given that MS evolves over several decades, there is a need for longer-term data on treatment outcomes
This study assessed the long-term impact of IFNB-1b therapy in patients involved in the pivotal study
Ebers, George 2007
30
Credibility factors in Betaferon 17 year follow-up data
Positive: Independent analysis Intent to treat analysis: treated vs. placebo
• About 90% case ascertainment • Betaferon effective and safe for 17 years
Concerns: Unknown treatment modalities for some patients
after trial ended High rate of mortality in placebo group after trial
ended. Is untreated MS a potentially fatal disease?
31
*Versus patients on other DMTs or no treatment.
Goodin DS, Ebers G, Traboulsee A, et al, for the Betaferon® LTF Study group [poster]. American Neurological Association. October 8-11, 2006. Ebers G, Traboulsee A, Langdon D, Goodin D, Konieczny A, for the Betaferon®/Betaferon® LTF Study Group [poster]. American Academy of Neurology. April 1-8, 2006.
Long-term follow-up study: Betaferon significantly delayed disease progression over 17 years of treatment
Patients who continuously used Betaferon had nearly 60% more cane-free years from time of diagnosis*
Treatment with Betaferon delayed progression to SPMS by 6.6 years compared to other treatments or no treatment
After 17 years, the tolerability and safety profile of Betaferon remains excellent
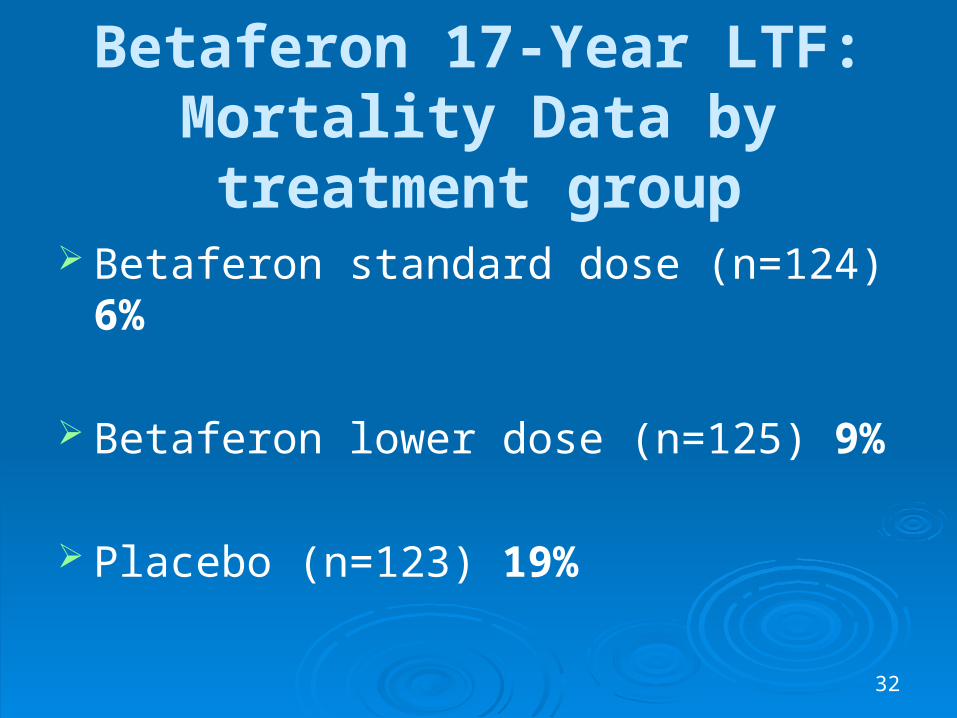
32
Betaferon 17-Year LTF:Mortality Data by treatment group
Betaferon standard dose (n=124) 6%
Betaferon lower dose (n=125) 9%
Placebo (n=123) 19%
33
Using Evidenced Based Medicine to Guide MS Therapy
AAN Guidelines
Cochrane Committee Reports
Head to Head Class I Trials

34Goodin DS, et al. Neurology. 2002;58:169-178.
Evidence-based Medicine: AAN Guidelines
35
AAN Guidelines on DMT’s 1) Relapses and MRI
• All better than placebo (A)
2) Disability Progression• Interferons: Probably Effective (B)• Copaxone: Possibly Effective (C)
3) IFNs: Higher Dose / frequency more effective (B)
4) NAb: Conflicting data (U)• Utility of measuring is uncertain• Did not recommend testing requirements
36
Patient 2: Evaluating the
Response to Disease Modifying Therapy
(DMT) in MS
37
Patient 2: Evaluating Response to DMT
Current complaint 28-year-old surgical resident with RRMS Recently developed fatigue and frustration
but without impairment of surgical skills, even during extended operations
She is considering changing her MS therapy
38
Patient 2: Evaluating Response to DMT (Cont.)
Past Neurological History 3.5 yrs ago: first symptom (unsteadiness of gait)
resolved without treatment or evaluation 3 years ago: bladder urgency, difficulty handwriting,
mild weakness in right leg• Brain MRI revealed 2 GAD+ lesions and 10 T2 lesions: locations
included periventricular areas, brain stem, cerebellum and corpus Callosum.
• CSF: + bands and IgG Synthesis: Other labs normal • Diagnosis of RRMS was made and treatment was I.V. Steroids
for 5 days. IFN B-1b was also begun. She recovered completely in one month
6 months later: mild blurred vision in left eye for two weeks with spontaneous recovery without steroids. No Evaluation

39
Patient 2: Evaluating Response to DMT (Cont.)
Current evaluation: Neuro Exam Normal: Possible depression? MRI: No GAD lesions: T2 lesions are
smaller. No black holes or atrophy NAb test: + (1:100 titer)
40
Neurologists Assessment Since IFN B-1b, this patient has had only
one episode of (likely) mild optic neuritis – shortly after beginning therapy 3 yrs ago
Neuro exam was normal MRI demonstrated improvement since
beginning therapy Patient does not have enough evidence to
diagnose “suboptimal response” to current therapy.
41
Neurologist’s Action Plan
Patient should remain on IFN B-1b Treat symptomatically for fatigue &
depression Patient and NAb status should be
reevaluated in 6 months
42
Questions
What is the utility of NAb testing in this clinically stable patient?
What will be the patient’s response to changing a treatment that is apparently working, especially if the change results in a treatment that may not work as well?

43
Comments There remain differences of opinion regarding the
use NAb testing. 2007 AAN guidelines using EBM principles do not support routine NAb testing because
No class I EBM results on utility of NAb testing No standardized NAb test No established level of NAb relevance (?100-200) titer No EBM data on timing of NAb test No EBM data on clinical outcomes after changing therapy
based on + NAb test Recent data fails to correlate NAbs with poor
response to treatment.
44
Neutralizing Antibodies to Interferon B-1b are not
Associated with Disease Worsening in Multiple Sclerosis
Goodin DS., Hurwitz B., Noronha A. The Journal of International Medical Research, 2007; 35: 173-187
45
NAb Results:6698 Patients
Australia: All Patients on IFNβ-1b 37% NAb positive
North America: Suboptimal Responders 21.3 % NAb positive
Europe: Suboptimal Responders 27.6% NAb positive
Goodin, 2007
46
Conclusions:
Poor responders were less likely to have NAbs than responders
NAbs are not responsible for poor clinical responses and that NAb status is of little clinical value.
Goodin DS., Hurwitz B., Noronha A. The Journal of International Medical Research, 2007; 35: 173-187

47
Evaluating Response to DMT: Patient 2 Follow-up
6 months later she was NAb Θ on retest The patient has remained on IFN B-1b with no
new symptoms for the last 2 years Modafinil was added for fatigue: improvement SSRI taken for depression for one year. She is now a fully functioning surgeon
with no depression and minimal fatigue

48
Patient 4: Managing Side Effects of DMT's
49
Patient 4: Managing Side Effects of DMT’s
34 yr old RRMS patient has been on IFN B-1b for 4 months
Neurologically stable but experiences flu like side effects and redness/pain at injection sites. She is unable to work because she feels “sick”, agitated, and depressed. Although feeling better in the past 2 months, she still wants to stop or switch treatment.
Initially she was started on the full dose of IFN B-1b without titration or analgesia pre-injection medication. Her husband has been injecting the drugs at an angle “to avoid going too deep”.
Liver function and CBC tests are normalMRI is unchanged

50
Neurologist’s Assessment
Since beginning therapy she has had no relapses or new MRI lesions
Side effects are caused by lack of dose titration when starting treatment and improper injection technique (Intradermal injections).
Depression could be from learning of her diagnosis of MS or worry about drug side effects vs. a direct effect from drug.
51
Neurologist’s Actions
Drug holiday for one month Re-start IFN B-1b at ¼ dose and titrate to ½,
then ¾ and then full dose each 2-3 weeks Close supervision and counseling Take analgesics before each shot Inject at 90 degrees Evaluate for depression on each visit, but no
anti depression medication at this time
52
Patient 4: Outcome
At 1 year patient tolerated treatment well with very few side effects and no recurrence of depression symptoms.
No missed days from work

53
Patient : Discussion
Drug side effects may mimic worsening of MS
Proper initiation of therapy prevents most early side effects
Aggressive side effect management can often avoid terminating therapy
54
Patient 5:Evaluating Possible Treatment Failures
55
Patient 5: Deciding When Treatment Is Not Working
A 43-year-old patient seeks a second opinion 5-year history MS Treated for 3 years with IFNβ-1a IM weekly Clinical exam
Weakness in extremities (worst in left lower) Uses cane for balance (4 months) Bilateral extensor plantar responses decreased vibration and position sensation in both legs and left hand Dysmetria bilaterally on finger to nose, and rapid alternating
movements bilaterally; dysmetria on heel to shin Mild memory dysfunction
56
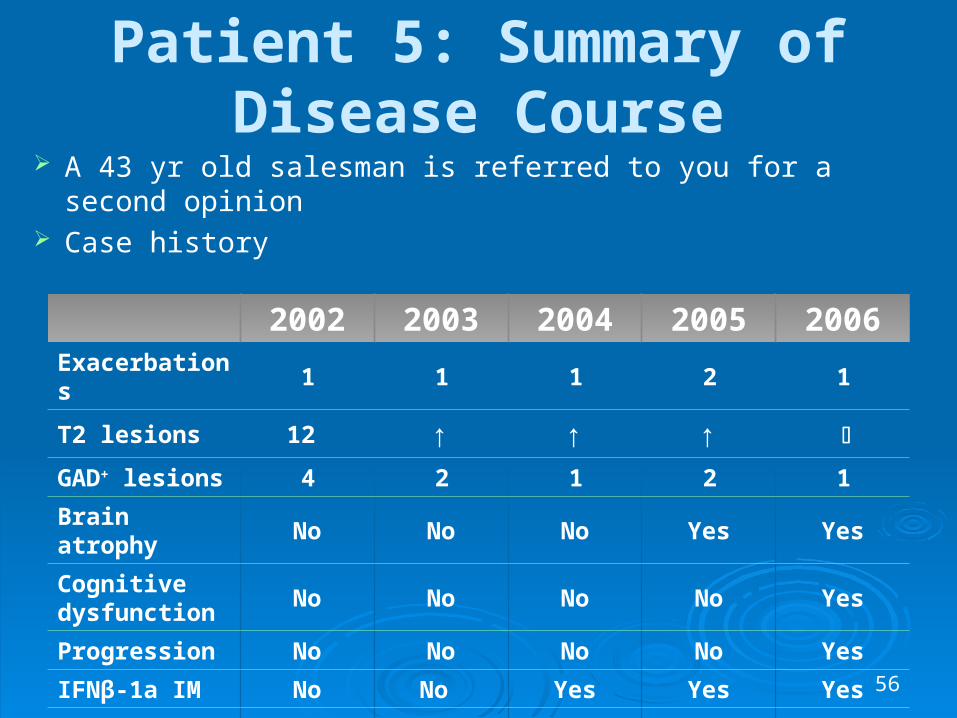
Patient 5: Summary of Disease Course
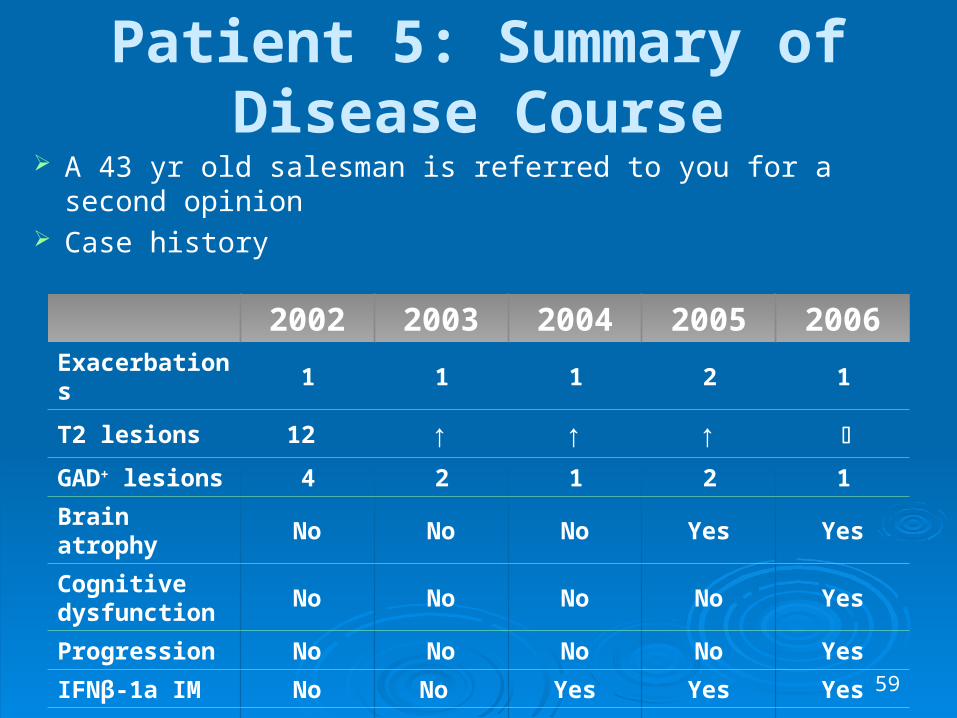
A 43 yr old salesman is referred to you for a second opinion Case history
2002 2003 2004 2005 2006Exacerbations 1 1 1 2 1
T2 lesions 12 ↑ ↑ ↑
GAD+ lesions 4 2 1 2 1
Brain atrophy No No No Yes Yes
Cognitive dysfunction
No No No No Yes
Progression No No No No Yes
IFNβ-1a IM No No Yes Yes Yes
NAb status ND ND Negative Negative Negative
57
Neurologist’s Assessment
The initial diagnosis of RRMS was correct The patient had 4 exacerbations during the
3 years on INF B-1a IM weekly The disease has transitioned from RRMS to
SPMS in the past 6 months Response to IFNB-1a has been suboptimal
in spite of negative NAb testing Therefore, treatment was switched to IFN
B-1b, 250 mcg god
58
Questions Raised by Patient 5
Was DMT started at the right time? What did his NAb test results mean? When did this patient’s disease become sub-
responsive to IFN B-1a IM? What criteria are most important for
determining when a patient has a suboptimal response to treatment?
When should natalizumab, and/or immunosuppressant drugs be considered?
59
Patient 5: Summary of Disease Course
A 43 yr old salesman is referred to you for a second opinion Case history
2002 2003 2004 2005 2006Exacerbations 1 1 1 2 1
T2 lesions 12 ↑ ↑ ↑
GAD+ lesions 4 2 1 2 1
Brain atrophy No No No Yes Yes
Cognitive dysfunction
No No No No Yes
Progression No No No No Yes
IFNβ-1a IM No No Yes Yes Yes
NAb status ND ND Negative Negative Negative

60
Deciding When Treatment Is Not Working: Discussion
To provide optimal, care one must be prepared to change treatment if the course of the disease changes
Worsening neurological status (including cognition) with or without relapses are the most important criteria for deciding if a patient is progressing
61
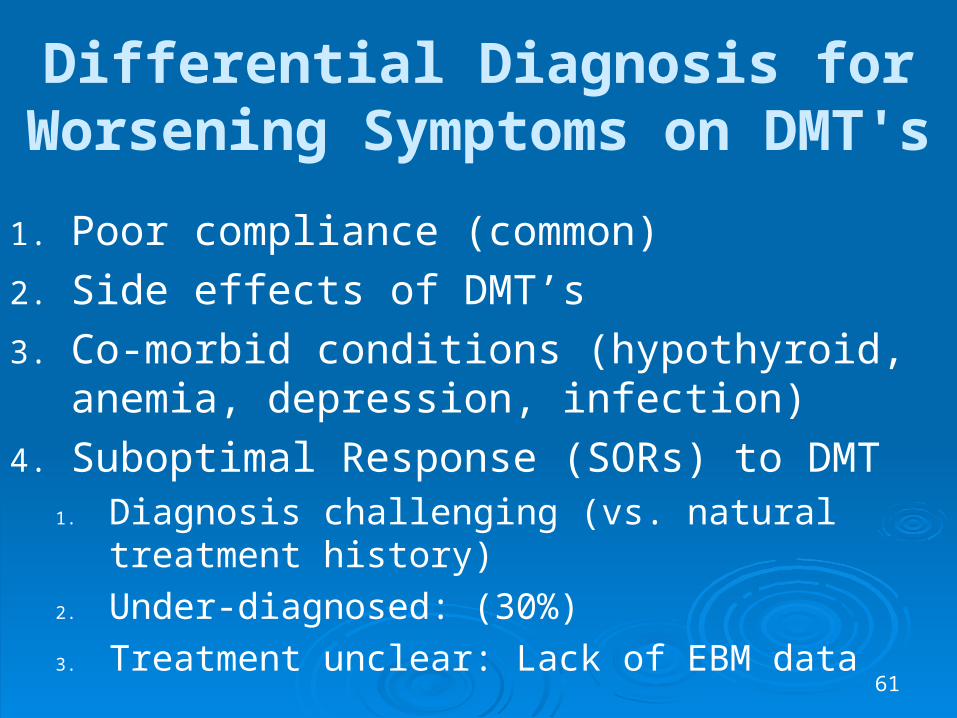
Differential Diagnosis for Worsening Symptoms on DMT's
1. Poor compliance (common)
2. Side effects of DMT’s
3. Co-morbid conditions (hypothyroid, anemia, depression, infection)
4. Suboptimal Response (SORs) to DMT1. Diagnosis challenging (vs. natural treatment
history)
2. Under-diagnosed: (30%)
3. Treatment unclear: Lack of EBM data
62
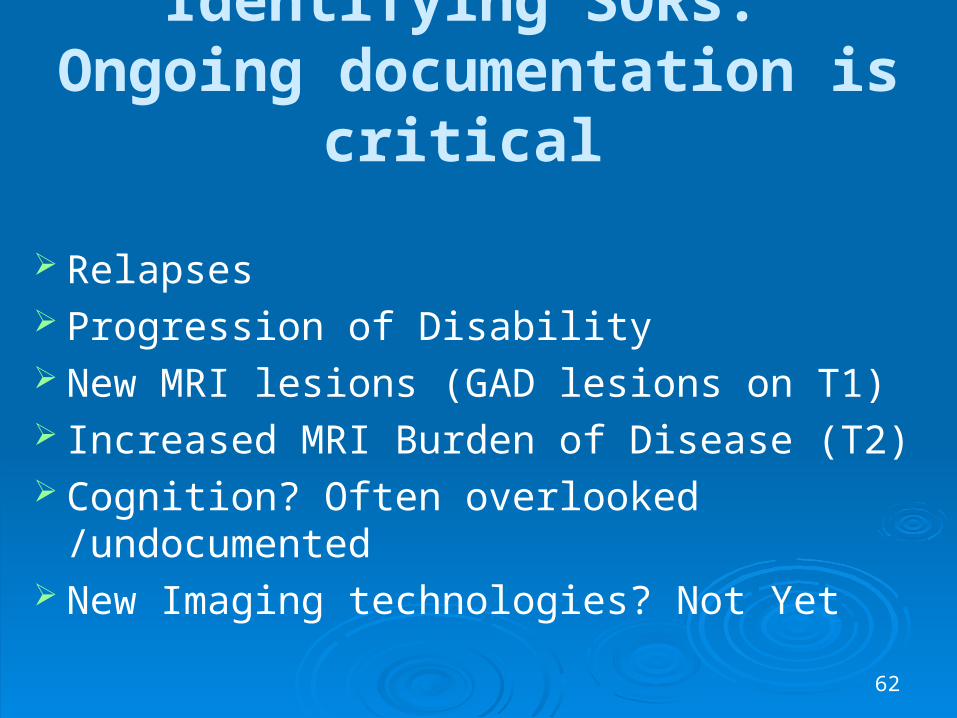
Identifying SORs: Ongoing documentation is critical
Relapses Progression of Disability New MRI lesions (GAD lesions on T1) Increased MRI Burden of Disease (T2) Cognition? Often overlooked /undocumented New Imaging technologies? Not Yet
63
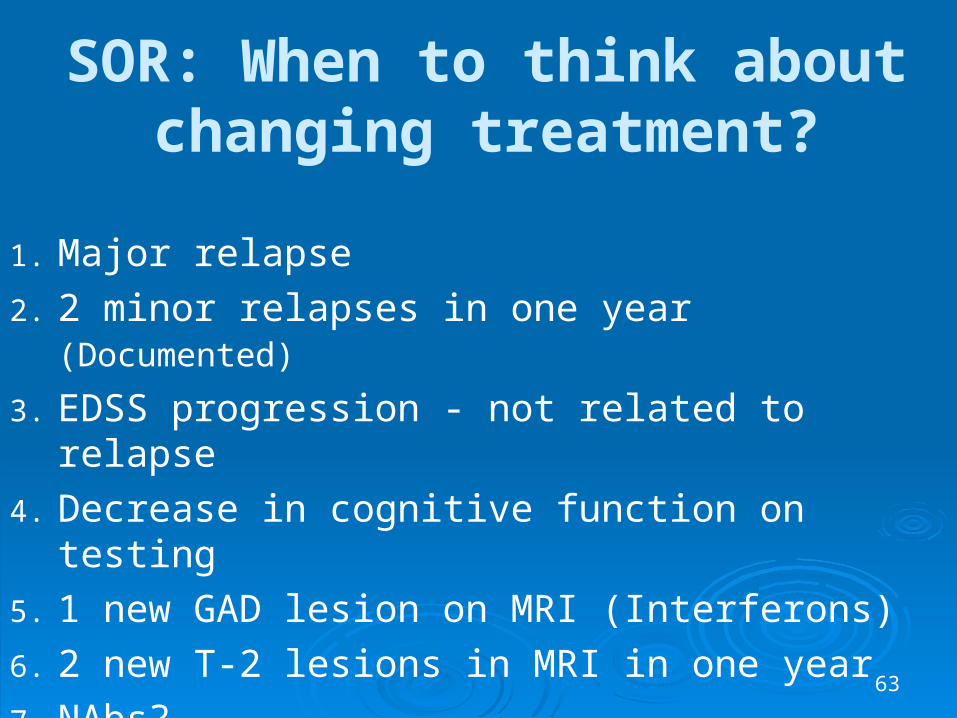
SOR: When to think about changing treatment?
1. Major relapse
2. 2 minor relapses in one year (Documented)
3. EDSS progression - not related to relapse
4. Decrease in cognitive function on testing
5. 1 new GAD lesion on MRI (Interferons)
6. 2 new T-2 lesions in MRI in one year
7. NAbs?

64
SOR: When to think “Why should I NOT Change treatment?”
1. 2 major relapses in one year2. Documented further EDSS progression on 2
exams 6 months apart3. Documented further decline of cognition on 2
exams 6 months apart. 4. 2 or more GAD lesions in 2 years (interferons)5. 3 or more new T-2 lesion in 2 years6. Considerable increase in brain atrophy,
permanent black holes
65
Management of SOR
Data is incomplete: Little EBM data:
“Therapeutic Window” is closing
Increase dose/frequency within class of drug
Change class of treatment
Add drug/combination therapy
66
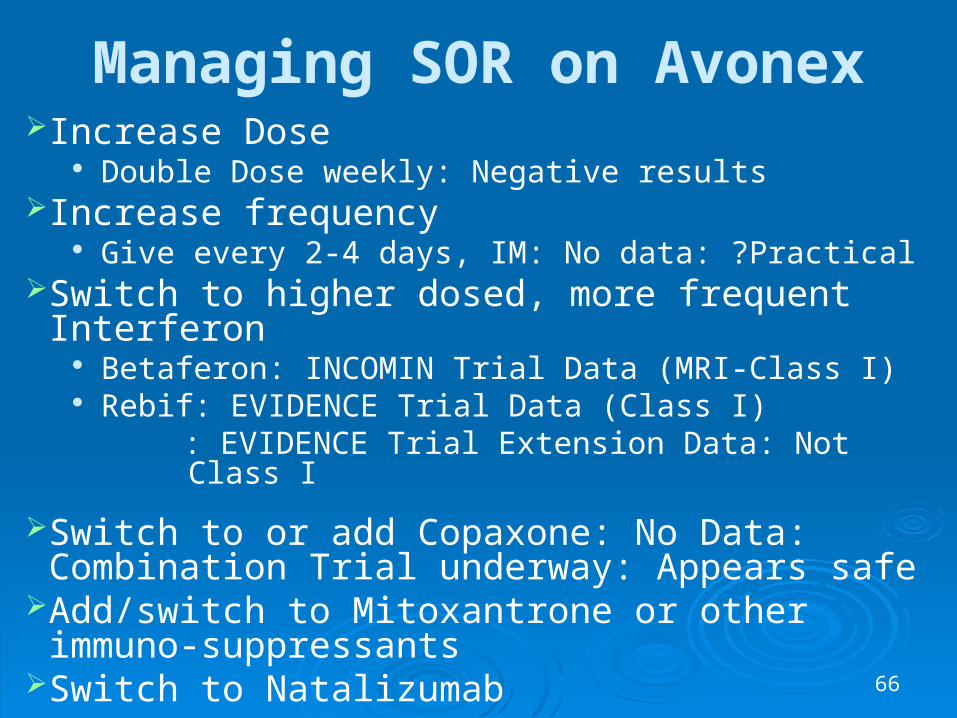
Managing SOR on AvonexIncrease Dose
Double Dose weekly: Negative resultsIncrease frequency
Give every 2-4 days, IM: No data: ?PracticalSwitch to higher dosed, more frequent Interferon
Betaferon: INCOMIN Trial Data (MRI-Class I) Rebif: EVIDENCE Trial Data (Class I)
: EVIDENCE Trial Extension Data: Not Class I
Switch to or add Copaxone: No Data: Combination Trial underway: Appears safe
Add/switch to Mitoxantrone or other immuno-suppressants
Switch to Natalizumab

67
INdependent COMparison of INterferon (INCOMIN)
Trial Study Group
Durelli et al. Lancet 2002, 359:1453-60Durelli et al. Lancet 2002, 359:1453-60
A Multicenter Trial Comparing Clinical and
MRI Efficacy of Betaferon® and Avonex® in RRMS

68
Betaferon vs. AvonexThe INCOMIN Trial
Results: First 24 Months
Betaferon vs. AvonexThe INCOMIN Trial
Results: First 24 Months Avonex Betaferon
(n=92) (n=96) % p Avonex Betaferon
(n=92) (n=96) % p
T2 Lesion Free (0-24 mo) 19 (26%) 42 (55%) +53% 0.0003
% Change Lesion Load +11.7% -2.8% >100 0.0001
EDSS progression (0-24 mo) 28 (30%) 13 (14%) -46 0.005
New T2 lesions (6-12 mo) 33 (45%) 16 (21%) -52 0.002
Gd+ lesions (6-12 mo) 16 (22%) 7 (9%) -56 0.03
Gd Lesion Free (0-24 mo) 18 (25%) 39 (51%) +51 0.0008
Relapse-free (0-24 mo) 30 (33%) 46 (48%) +35 0.036
NAbs did not effect outcomes
69
The EVIDENCE Trial
Head-to-head, randomized, open label, evaluator-blinded comparison of Rebif (44 mcg tiw SC) with Avonex (30 mcg qw IM) in patients with RRMS
Neurology. 2002;59:1496-1506
EV idence of Interferon Dose-response:European North American Comparative
Efficacy Trial
EV idence of Interferon Dose-response:European North American Comparative
Efficacy Trial
Panitch H. Neurology 59: 1496-1503 (2004)
70
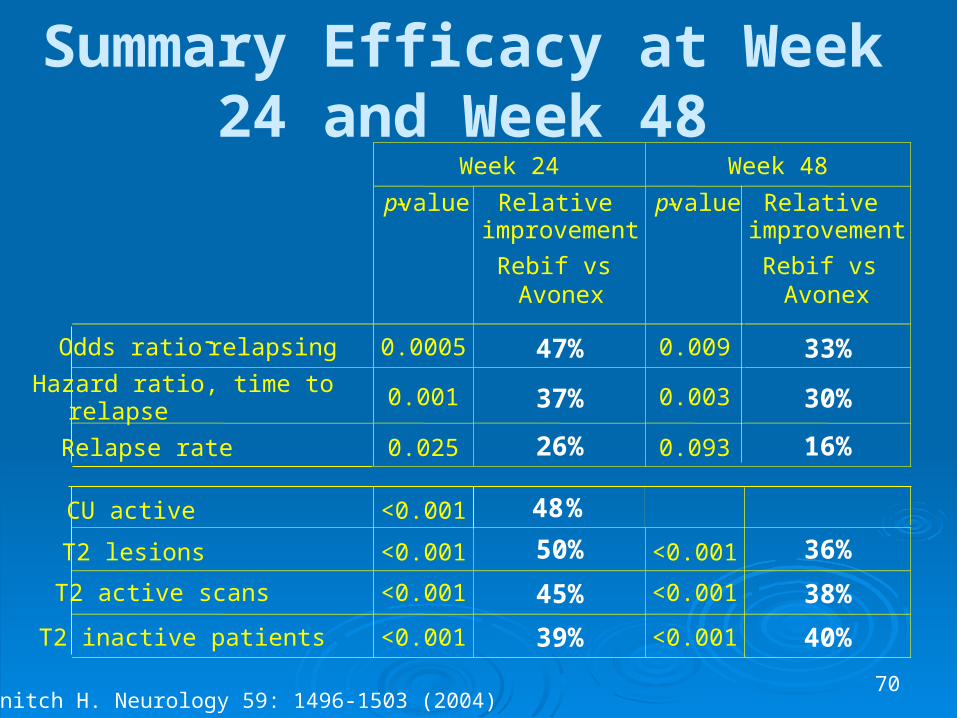
Summary Efficacy at Week 24 and Week 48
Week 24 Week 48
p-value Relative improvement
p-value Relative improvement
Odds ratio - relapsing 0.0005 47% 0.009 33%
Hazard ratio, time to relapse
0.001 37% 0.003
30%
Relapse rate 0.025 26% 0.093 16%
CU active
<0.001
48%
T2 lesions <0.001 50% <0.001 36%
T2 active scans <0.001 45% <0.001 38%
T2 inactive patients <0.001 39% <0.001 40%
Rebif vs Avonex
Rebif vs Avonex
Panitch H. Neurology 59: 1496-1503 (2004)

71
Avonex to Rebif Switch TrialAnnualized Relapse Rate
Final Comparative Phase vs Posttransition Phase
Panitch H. Neurology 59: 1496-1503 (2004)
Rebif 44 mcg tiw f 44 mcg tiw final comparative phase
Avonex 30 mcg qw final comparative phase
Rebif 44 mcg tiw posttransition 44 mcg tiw posttransitionfrom Rebif/Avonexfrom Rebif/Avonex
26%
0
0.2
0.4
0.6
0.8
An
nu
aliz
ed r
elap
se r
ate
(mea
n)
Avonex to Rebif (n=223)
P< 0.001
P=0.028
50%
Rebif to Rebif (n=272)
0.46
0.34
0.64
0.32
72
Managing SOR on Avonex Increase Dose
Double Dose weekly: Negative results Increase frequency
Give every 2-4 days, IM: No data: ?Practical Switch to higher dosed, more frequent Interferon
Betaferon: INCOMIN Trial Data Rebif: EVIDENCE Trial Data
: EVINDENCE Trial Extension Data Switch to Copaxone: No EBM data: Safe Add Copaxone: No Data: Combination Trial
underway: Appears safe Add/switch to Mitoxantrone or others Switch to Natalizumab
73
Managing SOR on Betaferon Increase Dose: Reasonable Pilot data: Well tolerated
OPTIMS Trial BEYOND Trial
Switch to Rebif: No data: Switch to Avonex:
No: INCOMIN Dose Reduction study Switch to Copaxone: Safe, No EBM data Add Copaxone: No data Add/Switch to Mitoxantrone or other
immunosuppression Switch to Natalizumab
74
INdependent COMparison of INterferon (INCOMIN)
Trial Study Group
Durelli et al. Lancet 2002, 359:1453-60Durelli et al. Lancet 2002, 359:1453-60
A Multicenter Trial Comparing Clinical and
MRI Efficacy of Betaferon® and Avonex® in RRMS
75
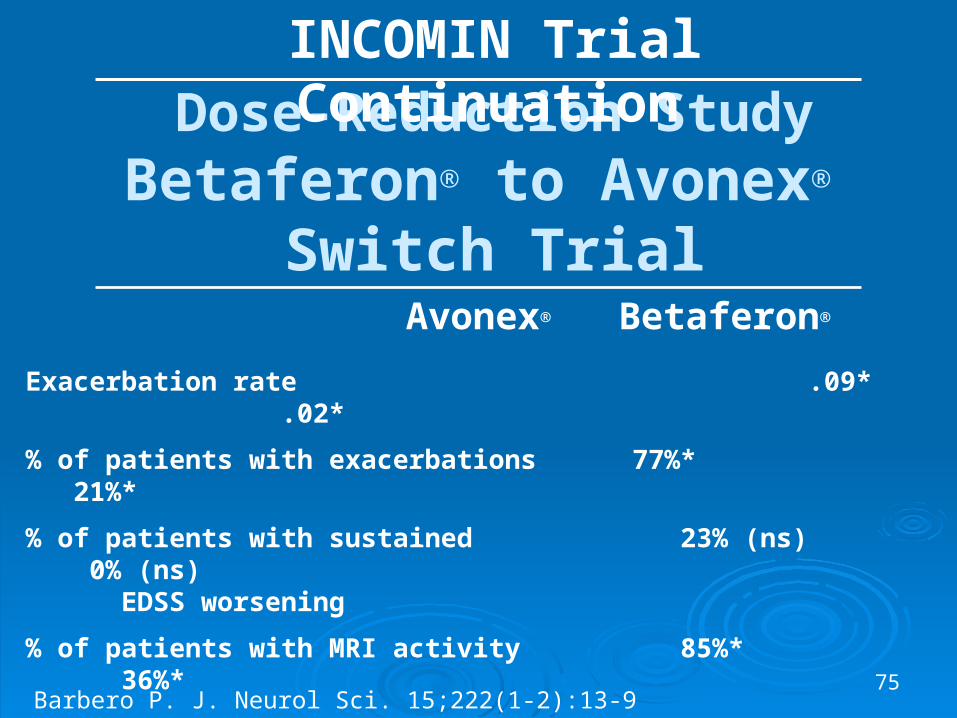
Dose-Reduction StudyBetaferon® to Avonex®
Switch TrialAvonex® Betaferon®
Exacerbation rate .09* .02*
% of patients with exacerbations 77%* 21%*
% of patients with sustained 23% (ns) 0% (ns) EDSS worsening
% of patients with MRI activity 85%* 36%*
* Statistically significant p<0.05
INCOMIN Trial Continuation
Barbero P. J. Neurol Sci. 15;222(1-2):13-9 (2004)
76
Managing SOR on Betaferon Increase Dose: Reasonable Pilot data: Well tolerated
OPTIMS Trial BEYOND Trial
Switch to Rebif: No data Switch to Avonex: No: INCOMIN Dose Reduction
study Switch to Copaxone: Safe, No EBM data Add Copaxone: No data Add/Switch to Mitoxantrone or other
immunosuppression Switch to Natalizumab
77
Managing SOR on Rebif
Increase Dose: No data: Not very practical Switch to Betaferon: No data: Maybe easier
to give even higher dose Switch to or add Copaxone : No data. Safe Add/Switch to Mitoxantrone or other
immunosuppression Switch to Natalizumab
78
Managing SOR on Copaxone
Increase dose? Double dose: positive PILOT data
Switch to Interferon: No EBM data: Most popular option: safe
Add Interferon: Combination Trial underway: safe
Add/switch to Mitoxantrone or others

79
Other SORs Treatment OptionsImmunosuppression:
Mitoxantrone (Novantrone) For worsening MS (RRMS and SPMS) Approved by FDA Popular for SOR treatment of ABCR drugs Relatively well tolerated Issues:
1. Occasional permanent amenorrhea
2. Cardiotoxicity: Dose dependent (2-3) years
3. Uncommon Risk of Leukemia (1 in 500?)
80
Other SOR Options
Pulses Methylprednisolone (I.V., monthly) Methotrexate (oral, weekly) Azathioprine (Imuran) (oral, daily) Cyclophosphamide (Cytoxan) Micophenolate (Cell Cept) IVIG Tysabri (Natalizumab): DO NOT ADD! Natalizumab (Tysabri) switch

81
Summary & Conclusions: SOR Diagnosis
SORs are common (30% or greater) but are under diagnosed
Is patient Compliant with drug? Regular documentation of MS course is
crucial: Relapses, MRI lesions, disability progression, ? Cognition
Rule out other causes of worsening MS : co-morbid conditions, pseudo exacerbations, depression, UTI, thyroid dysfunction
82
Summary & Conclusions: SOR Treatment
Little EBM data but therapeutic window closing: Options include:
1. Increase dose/frequency within class
2. Change class of treatment
3. Add different class of therapy (not natalizumab)
83
What is New?
Current and Emerging Therapies
84
A. Betaferon
1. BENEFIT Trial in CIS
2. 17 Year Follow up data
3. Betaferon vs. Double Dose Betaferon vs. Copaxone
85
B. Rebif
1. Reformulated Rebif
2. Rebif vs. Copaxone
3. Rebif in CIS
4. Cladribine Induction before Rebif
5. Rebif vs. Betaferon tolerability study
86
C. Copaxone
1. Copaxone in Primary Progressive MS: Discouraging
2. Double Dose Copaxone in RRMS: Encouraging
3. Copaxone in CIS (in progress)
4. Copaxone vs. Betaferon (in progress)
5. Copaxone vs. Rebif (data being analyzed)
87
D. Natalizumab (Tysabri)
1. Natalizumab vs. Placebo in RRMS
2. Natalizumab vs. Avonex
3. The PML issue
88
Oral Therapies
May improve convenience and compliance in MS therapy
Oral therapies now in phase 3 trials may be available in late 2010 Fingolimod (FTY720) Teriflunomide Cladribine Laquinimod
89
Monoclonal Antibodies (MAbs): Background
MAbs offer more favorable dosing regimens compared with current MS therapies (less frequent)
MAbs currently in use appear to be associated with specific side effects, eg, PML, Graves disease, ITP
Clinical trials of MAbs in MS are less advanced than those of oral therapies
Possible that no MAb currently in development will enter MS market before 2010
90
MAbs: Conclusions
Some striking efficacy results with MAbs in MS
Safety concerns must be allayed before MAbs are widely used in MS

91
Other Emerging Treatments
Fingolimod (oral) Campath (yearly) MBP82-98 (6 months) Rituximab (B-cell AB) (? PML) Cladribine (oral) Fumarate (BG-12) (oral) Teriflunomide (oral) Statins (oral): blocks IFNs Minocycline (oral Estriol (oral) Laguinimod (oral)
Fampridine-SR (Ambulation) NeuroVax (T-cell vaccine) Tovarin (anti T-cell) Bone Marrow Transplant IVIG Stem Cell Transplant Marijuana (symptomatic) Testosterone (Cognitive) Small Molecules CellCept (mycophenolate)

92
Other Treatment Approaches
Stem cells (bone marrow and embryonic)
Remyelinating agents
Neuroprotective agents
93
Patient 5A: Management of
Suboptimal Responders to both low and high
Dose Interferons
94
Patient 5A
39 year old male with very active RRMS for 3 years. He averages 2 attacks per year for all three years with only partial response to IV steroids. He was started on INFβ1-a I.M. (Avonex) weekly for the next two years. He was then switched to Rebif 44 TIW for the past year. He had 2 attacks during that last year with incomplete recovery with steroids.
95
Patient 5A
He is stable between attacks, but ongoing MRI activity is present. His exam reveals a bilateral intramuscular opthalmoplegia; right hemiparesis and ataxic gait requiring a cane to walk (EDSS=6).
96
Patient 5A What is your best treatment option
1. Keep on Rebif but double the dose2. Get an NAb test and stop Rebif if positive3. Switch to IFNβ-1b at double dose (500 ug)4. Add or Switch to Mitoxantrone5. Add or switch to Azathioprine6. Add or switch to cyclophosphide 7. IVIG8. Add Natalizumab (No!)9. Switch to Natalizumab10. Other options?
97
Patient 5B A 36 year old lady from Sari with
severe MS wants a child 36 year old, married11 years, MS started 9
years after Mother died in her arms Initial Symptoms 9 years ago: Fatigue,
legs weak, falling. After 3 months Neurologist diagnosed MS
by symptoms, exam and MRI with multiple lesions. She does remember an CSF.
Treated with IV steroids and improved
98
Sari MS patient Relapse after 4 months, Treated with IV steroids and
improved back to “normal” Treated with Betaferon in 2000 and did well until 2004
when she stopped treatment to try “magic” therapy with alternative medicines, herbs and acupuncture.
Much worse symptoms until 2004 when saw a Neurologist and got Methetrexate followed by Betaferon. Her MS became more stable.
In 2006 stopped Betaferon to become pregnant. She had a miscarriage at 3 months and now wants to become Pregnant again. She fears her may leave her if she doesnot have a child.
3 weeks ago she became paraplegic with decreased feelings in both legs. She is considering Novantrone.
99
36 year old Sari patient
Brief Exam reveals tearful lady with only slight movement in legs in a wheelchair
Spasticity in legs with sustained clonus at the ankles
Mild to moderate weakness in arms - L. more than R side
Ataxia and tremor - L more than R Marked decrease in position sense in legs Cranial nerves OK

100
36 year old Sari patient
Meds include
Numerous vitamins
Baclofen
St John wort
Amantadine
MRI : 2003 Many T2 lesions
: 2005 More lesions with brain atrophy

101
Issues for Sari patient
Early Treatment value Problems with Adherence to Betaferon Chemotherapy in lady who wants kids “Alternative” medicine versus Betaferon Pregnancy desires versus treatment desires Acute treatment and long term treatment options Rehab, Depression and family issues

102
36 Year old Sari patient:My thoughts on Treatment
Must treat relapse immediately with IV steroids! If failure, try plasma phoresis or IVIG. Since she has done well on Betaferon in past, restart
with dose escalation ASAP – with IV steroids Treat with Betaferon for one year and re-evaluate. If sub
optimal response, try double dose of Betaferon if available data and positive by then. Or consider Novantrone or Tysabri. If she continues to do badly, consider Rituxamab in future – or other new med
Rehab, depression Rx and family counseling ASAP Consider adoption and not delay treatment for MS
103
Patient 6:The Dilemma of
“Asymptomatic” MS
104
Patient 624 year old female with bitemporal throbbing “migraine” headaches associated with nausea, vomiting for 4 years associated with menstrual periods. Headaches last 2-6 hours and are helped with sumatriptan (Imitrex) if taken early in the course of the headache. She denies any fevers or chills. She is otherwise healthy with no family history of Neurological disease. No history of previous head injury.
105
Patient 6
Her neurological exam was normal. MRI was done to rule out Meningioma, Aneurysm, or Arterial-venous malformation (AVM). Her T-2 weighted MRI revealed 6 white matter lesions ranging from 3-8mm, mainly periventricular. Radiologist conclusion “Multiple lesions, consistent with multiple sclerosis”.
106
Patient 6
She comes to you for a second opinion:
1. Does she have MS? (or something else?)
2. Should she have an L.P., another MRI (GAD?), Evoked Potential testing, other workups?
3. Should she be treated with steroids or specific MS therapies
107
Patient 6
What is your Differential Diagnosis?
How would you work up and treat this patient?

108
Patient 6Differential Diagnosis
Collagen vascular disease (SLE)
CADASIL Thyroid disease Hypoglycemia Vitamin deficiencies Sjögren syndrome Behçet’s disease Myasthenia gravis Spino-cerebellar Degeneration
Adrenoleukodystrophies Lyme disease Syphilis TB & other CNS infections Sarcoidosis CNS malignancy CNS embolic disease AIDS PML
109
Patient 6 Evaluation for MS:
Diagnosis and Progression Clinical history and exam best Ancillary tests
MRI CSF Evoked potentials Urological testing Cognitive tests EDSS, MSFC scale, Scripps scale
110
Patient 6
Her evoked potential tests, ANA, Sed Rate, thyroid screen, VDRL, and other screening tests are normal. She has no GAD lesions or new T-2 lesions on repeat MRI done 2 weeks later. CSF is normal
111
Patient 6
Would you diagnose MS? Would you treat with Steroids? Would you treat with Interferons? Would you treat with both Steroids &
Interferons?
112
Patient 6
She was not given the diagnosis of MS and was not treated

113
Patient 6
If she had an identical twin with MS, would that change your opinion?
Identical twins have a 30% concordance rate for MS
114
Patient 6
One year later, she remained asymptomatic with a normal exam, but a repeat MRI showed 2 new T-2 lesions, but no GAD + lesions.
Does she now have MS?
Would you treat?

115
Patient 6
She was not diagnosed as MS and was not treated
116
Patient 6 One year later she had an episode of numbness on
left arm and leg along with fatigue and ataxia. Her MRI revealed 4 new T-2 lesions and 2 GAD + lesions
Would you diagnose MS? Would you treat with Steroids? Would you treat with Interferons? Would you treat with both Steroids & Interferons?
117
Patient 6 She was diagnosed as MS and treated with
steroids and Interferon β-1b with no further attacks in 5 years of follow-up.
Her MRI revealed no new T-2 or GAD lesions.
Would you stop her Interferon Treatment?
118
Patient 7: Differentiating MS,
Neuromyelitis Optica (DEVIC’s), and Asian
Optica-spinal MS
119
Patient 7
18 year old Asian male presented with decreased vision in right eye over 3 days with pain on eye movement: ophthalmologist diagnosed “optic neuritis” and treated with IV steroids with good results. Four months later he developed numbness and weakness in his legs with difficulty walking over a one week time period. His examination showed optic palor on right, decreased sensation below umbilicus and decreased strength in both legs.
120
Patient 7
Babinski test was positive bilaterally, DTR’s were very active with transient clonus at At ankles. CSF tests were negative, except for 15 WBCs, MRI of spine showed a patchy longitudinal lesion from L1-4. Brain MRI showed 2 periventricular T-2 lesions. Extensive work up for other diseases was negative but acquaporin-4 antibody test was positive.
121
Patient 7
What is the most likely diagnosis?1. Classical MS
2. Asian MS (optic-spinal MS)
3. Neuro myelitis optica (NMO or Devics Disease)
4. CNS lymphoma or metastatic cancer
5. Other
122
Neuromyelitis Optica Optic-Spinal MSRecurrent Optic
Neuritis Recurrent Myelitis
123
Spectrum of MS:Neuromyelitis Optica (DEVIC's)
NMO Gender predilection: Female to Male ~10:1 Onset in all ages Ethnic predilection: No clear ethnic predilection
• May be present in all areas of the world at very low prevalence• In areas with high prevalence of MS, may be misdiagnosed as atypical
MS• In areas with low MS prevalence, differentiation from classic MS
becomes easier
Investigation Spinal cord–longitudinally extensive, central necrotic lesions Brain–some lesions now permitted CSF–pleocytosis (>50 white cells/μL), polymorphonuclear cells,
oligoclonal band negative NMO Antibody (Aquaporin 4) found in 70%

124
Spectrum of MS:Optic-Spinal Multiple Sclerosis
OSMS (Asia) Gender predilection: Female to Male ~3:1 or more Ethnic predilection: Far-east Asian, Japanese, Latin
American
Investigation Brain–generally normal, but typical MS-like lesions
can be observed Spinal cord–multiple cord lesions of variable lengths CSF–Oligoclonal bands in about 30% of cases NMO Antibody found in >50% if long cord lesions (?NMO)
125
Spectrum of MSRecurrent Optic Neuritis
If Brain and Spinal cord MRI normal
CDMS less likely BUT may convert to CDMS years later Treat with IV steroids, not DMT's
126
Spectrum of MSRecurrent Myelitis
If brain MRI normal, unlikely CDMS
If NMO Antibodies +, may be NMO
Treat with IV Steroids and Immunosuppressants
127
Patient 7
Patient was diagnosed as DEVIC’S (NMO)
He was treated with IV steroids only. He recovered considerable function but not completely.

128
Patient 7
Eight months later has another episode with decreased vision in left eye and numbness from his mid chest to his legs. Thoracic MRI revealed a new thoracic lesion covering 3 segments
129
Patient 7 How would you treat him?
1. No treatment
2. IV Steroids
3. Interferon
4. Azathioprine
5. Mitoxantrone
6. Rituximab
7. Cyclophosphamide
8. IVIG
9. Natalizumab
10. Other drugs
130
Patient 7
He was treated with IVMP and Aziathiaprine. He had 2 more attacks within the next 18 months, which left him blind in his left eye and he required a cane to walk. He was switched to IVIG and had another attack in 3 months. He was switched to Rituximab and has had no further attacks in 1 year of follow up