Embed Size (px)
Citation preview

1
Medicare Part D Prescription Drug Benefit: Understanding Implications for Practices and Patients

2
Educational Objectives
• Provide an overview of the new Part D Medicare prescription drug benefit
• Review Part D eligibility guidelines and enrollment timelines
• Introduce Part D and Medicare Advantage regions
• Discuss the standard Part D benefit and alternative benefit structures
• Analyze assistance available for limited income beneficiaries
• Understand coverage for Part D drugs and formulary guidelines
• Discuss how Part D will impact practices and Medicare beneficiaries
• Review the Part D resources available to your practice and patients
2

3
Overview of Medicare Programs
Part A benefits provide coverage for inpatient services, such as hospitalizations, hospice care, skilled nursing
facility stays, and home health services.
Part A
Part B
Part B benefits provide reimbursement for outpatient services, durable medical equipment, home health
services, and drugs that are “not usually self-administered.”
Part CMedicare via managed care with all benefits of standard
Medicare plus additional benefits (formerly known as Medicare+Choice), now known as Medicare Advantage.
Part D
Beginning in 2006, the newly established Part D will provide an outpatient prescription drug benefit for
those drugs not currently covered by Medicare Part A or B.

4
Medicare Prescription Drug Coverage
• Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA)
•Signed by President Bush on December 8, 2003
• Prescription Drug Discount Card•Available to all Medicare beneficiaries June 1, 2004 – December 31, 2005
Estimated savings between 15% and 25% per prescription•Program ends December 31, 2005
Beneficiaries will need to enroll in Part D for drug coverage
• Medicare Part D Prescription Drug Benefit•Effective January 1, 2006 •Benefits include a standard plan and three levels of subsidy for limited income enrollees
4

5
Part D Covered Drugs
• For a drug to be covered under Medicare Part D, it must meet the following characteristics:
• Available only by prescription• Approved by FDA• Used for medically accepted indication• Used and sold in the US
• Covered Part D drugs include prescription drugs, biological products, insulin and vaccines
• Part A and B covered drugs may be included on some Part D plan formularies
• Currently covered Part B drugs will remain covered under Part B Oral anti-cancer prodrugs Oral anti-emetic drugs
• Wrap-around coverage provided by Part D when not covered by A or B• Part D will not cover co-insurance from Part A or B covered drugs
5

6
Administration of Part D Benefit
• The Part D benefit will be administered by risk-bearing private plans:
• Prescription Drug Plans (PDPs)• Traditional, fee-for-service Medicare, with access to private drug-only plans
• Medicare Advantage Prescription Drug Plans (MA-PDs)• Integrated plans that cover Medicare benefits and drugs• Parts A, B, and D in one product
• Plans began communicating to beneficiaries October 1, 2005
6

7
Part D Eligibility and Enrollment
• Beneficiaries currently eligible for Part A and/or Part B will be eligible for enrollment into Part D
• Enrollment into Part D is voluntary•Beneficiaries must elect to enroll in Part D•Dual eligibles and some limited income beneficiaries will be auto-enrolled
•Late enrollment penalties may apply
• Beneficiaries will have a variety of plans to choose from• Interested beneficiaries may enroll in a PDP or a MA-PD •National and regional PDP and MA-PD options exist •Plan enrollment is good for one year
7

8
Scenario 1: Beneficiary Enrolls Prior to January 1, 2006
If beneficiary enrolls in Part D before December 31, 2005, benefits are effective January 1, 2006, no late enrollment penalty
2006
Nov. 21
Patient enrolls in Part D
Jan. 1
Part D benefits are active
Jan. 20
MD prescribes patient Rx
treatment. Rx is covered by
Part D
2005

9
Scenario 2: Beneficiary Enrolls after January 1, 2006
If beneficiary enrolls in Part D after December 31, 2005, but before May 15, 2006, benefits are effective the first day of the following
month, no late enrollment penalty
2006
Mar. 3
MD prescribes Rx treatment
Mar. 4
Patient enrolls in Part D
Apr. 1
Part D benefits are active

10
Scenario 3: Beneficiary Enrolls after May 15, 2006
If beneficiary enrolls in Part D after May 15, 2006, benefits are effective the January 1, 2007, and beneficiary will be subject to a
late enrollment penalty
2007
Jun. 3
MD prescribes Rx treatment
Jun. 4
Patient enrolls in Part D
Jan. 1
Part D benefits are active
2006

11
Late Enrollment Penalty
• Part D is “insurance” and can be bought to either help with drug costs or to protect oneself from future drug costs
• Premiums are lower if beneficiaries enroll when first eligible
• Beneficiaries subject to a 1% premium increase per month past the enrollment deadline if beneficiary does not have creditable coverage
• Example calculation for beneficiary who enrolls in a plan eight months late, January 1, 2007
Late Enrollment Penalty Estimated Calculation
Beneficiary enrolls January 1, 2007
May 15, 2006 -
January 1, 20078 months late
Premium penalty of 1% of base beneficiary premium per month
1% x 8 months ($32.20 x 08%) = $2.58
Late enrollment premium
$32.20 + $2.58 $34.78
11

12
Creditable Coverage
• Definition: Coverage through a source other than Medicare (eg., retiree plan) that is at least as good as the standard Part D benefit
• Medicare beneficiaries with creditable coverage can remain in their plan without a late enrollment penalty
•Some retiree plans are considered creditable
• Medicare beneficiaries who have coverage that is not “creditable” or as good as the standard benefit will be subject to a late enrollment penalty
•Medigap prescription coverage currently does not offer coverage as good as the standard Part D benefit and, therefore, would not be creditable coverage
• Plan sponsors are required to mail letters to all Medicare patients indicating if their coverage is creditable or not
12

13
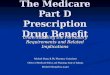
Prescription Drug Plan (PDP) Regions• Number of plans per region varies from 27 - 52
ME
VT
NHMA
RICT
NY
PA NJ
DEMDDCVA
NC
SC
GA
FL
ALMS
LATX
NMAZOK
AR
TN
KY
OH
WV
MI
INIL
WIMN
IA
MOKS
NE
SD
NDMT
WY
CO
UTNV
CA
ID
WA
OR
AK
HI
43
47 39
38
414343
47
44
43 40 41
43
40
41
44
4752
41
38
41
42
4242
45
42
45
44
27
29
40
46
4441
DE
DC
47MD
44
44
13

14
WA
OR
ID
MT
WY
CA
NV
AZ
UT
ND
SD
CO
NE
KS
OKNM
TX
MN
IA
MO
AR
LA
WI
IL IN
KY
TN
MS AL
MI
OH
AK
HI
FL
GA
SC
NC
VAWV
PA
NY
ME
NH VT
NJ
DE
DC
MD
CT
RI
MA
21
0
44 12
11332
164
17
257
34
14
12
53 17
20
14 14
24
4
22
49
3922
12
30
6
1116
1
35
21
164
15
7
54
13
28
25
8
1041
58
10
0
23
25
11
237
Medicare Advantage (MA-PD) Regions• Number of MA-PD plans varies from 0 to 257
14

15
Coverage under the Standard Benefit
• The total True Out of Pocket (TrOOP) costs incurred by a standard benefit enrollee prior to reaching catastrophic coverage is $3,600
• Monthly premiums do NOT count towards TrOOP
• The Kaiser Family Foundation estimates that the average beneficiary incurs annual prescription costs of $3,160
15
$32 premium$250 deductible
25%Co-insurance up to $2,250
5%Co-insurance
for $5,100 and beyond
Donut Hole Patientpays 100% cost ofdrug from $2,251
to $5,100
TrOOP = $250
TrOOP = $500
TrOOP = depends
ondrug costs
TrOOP = $2,850
* TrOOP = True Out of Pocket costs for the patient

16
Sample Medicare Benefit Designs (PDPs)
* Total drug costs
*** Members may obtain up to a 90 days supply at retail for incremental copays (1-30 = 1 copay; 31-60 = 2 copays; 61-90 = 3 copays
Plan Name Rx Type
Rx Costs
$0-$250 $250-$2250 Over $2250Over $3600 TrOOP
Humana PDP Standard
Generic
100% 25% 100% 5%Preferred
Non-preferred
Specialty
Humana PDP Enhanced
Generic $0 $7
100% 5%Preferred $30 $30
Non-preferred $60 $60
Specialty 25% 25%
Humana PDP Complete
Generic $0 $7 $7
5%Preferred $30 $30 $30
Non-preferred $60 $60 $60
Specialty 25% 25% 25%
Source: Humana benefit designs from https://www.humana-medicare.com

17
Patient spending for a course of therapy of $25,100
*Assumes that a course of therapy costs $25,100, that therapy is administered within one year, and that patient uses no other drugs
•$1233•$1046 •$1046
•$429•$209 •$209
•Humana PDP Complete
•25% coinsurance in donut hole
•Total spend: $4135•Month 1 •Month 2 •Month 3 •Month 4 •Month 5 •Month 6
Coinsurance benefit reduces the initial spending but total spend is only reduced by about 10% because catastrophic coverage is
delayed
•$2683
•$1080
•$209 •$209 •$209 •$209
•Part D Standard Benefit
•Total spend: $4600
•Month 1 •Month 2 •Month 3 •Month 4 •Month 5 •Month 6
Patient Spending with Coverage through Donut Hole
17

18
Part D Benefit Based on Patient Income Level
Income < 100% FPL <135% FPL <150% FPL Standard
Asset Test None$6,000 single
$9,000 couple
$10,000 single
$20,000 coupleNone
Premium Fully subsidized Fully subsidized Sliding scale $32.20
Deductible Fully subsidized Fully subsidized $50 $250
Patient co-payment/ coinsurance
$1 generic
$3 brand
$2 generic
$5 brand
15% up to catastrophic limit
25% up to $2,250 in drug expense
Gap in coverage
None None NoneBetween $2,250 and $5,100 in drug expense
Catastrophic coverage (>$3,601)
No cost sharing No cost sharing
$3 generic
$5 brand copay above limit
95% after $3,600 in OOP
18

19
Estimated OOPs for Beneficiaries of Different Income Levels, Assuming Drug Costs of $1,000 to $5,000
• Depending on the beneficiary’s ability to qualify for the low-income subsidy, the out-of-pocket expenses will vary greatly
• Assuming monthly drug costs between $1,000/mo to $5,000/mo the annual out-of-pocket expenses are displayed in the following table*
• For the beneficiary who qualifies for the full or partial subsidy, drug cost sharing under Part B may be greater than Part DGroup
Standard Benefit
<100% FPL <135% FPL <150 % FPL
$1,000 per month drug cost
$4,331 $36 $60 $2,229
$2,000 per month drug cost
$4,931 $36 $60 $3,991
$4,000 per month drug cost
$6,131 $36 $60 $4,021
$5,000 per month drug cost
$6,731 $36 $60 $4,026
*The calculations do not take into account any other drugs which a patient make be taking at the time. Includes premium.

20
Formulary Design
• Formularies must include at least two drugs for each category and class•Most formularies exceed minimum requirements
• Six drug classes of special concern in which all or “substantially all” drugs will be on formulary
•Anti-cancer, anti-HIV/AIDS, immunosuppressant, anti-psychotics, anti-depressants, and anti-convulsants
•All drugs will be on formulary, but plans can still impose coverage restrictions on these products
Prior Authorization Step Therapy
• Non-formulary drugs may be provided through an appeals and exceptions process
20

21
Tiering and Formulary Exceptions
Tiering Exception
Content of Physician’s Supporting Statement should indicate:
• Drug in preferred tier would not be as effective as requested drug• Preferred drug would have adverse effects
Formulary Exception
Content of Physician’s Statement Should State:
•All of the formulary drugs for treatment for the same condition would not be as effective as the requested non-formulary drug• Formulary drugs would have adverse effects
21

22
Issues and Challenges for Practices
• Medicare beneficiaries will have new coverage options•Patients may seek counseling from your office on:
Enrollment decisions Cost-sharing concerns Drug Coverage
• Dual eligibles•Complete change of benefits for this population•Education and counseling efforts will be needed
• Part D will follow Medicaid guidelines governing off-label use of drugs, not Medicare guidelines•Medicaid only recognizes compendia, not published literature• Important for drugs with prior authorization or diagnosis restrictions
22

23
Issues and Challenges for Practices (cont.)
• Tightly controlled drug formularies•Appeals and exception process for non-covered drugs is time and resource-consuming
7 days for re-determinations and up to 72 hours for expedited requests 72 hours for exceptions and 24 hours for expedited requests
• Changes to formulary mid-year•Plans can add/delete drug throughout the year with 60 days notice•Access to new drugs impeded
• Patients who do not enroll in Part D•Will they still be eligible for Patient Assistance Programs?
• How will your practice respond to these changes?
23

24
Practice Administrative Considerations
• Assess office ability to support Medicare beneficiaries in educating them about Part D options
• Practices need to be proactive in communicating beneficiary copay responsibilities upfront as part of the beneficiaries pre-treatment planning
• Practices do not have to be “experts” on Medicare and Part D options, but know your resources
•Advocacy groups and pharmaceutical companies can assist patients
• Understand the coverage guidelines for the PDPs and MA-PD plans in your market. If in doubt, verify coverage.
24

25
Issues and Challenges for Beneficiaries• Education and communication
•Deciding whether to enroll in Part D in 2006•Financial penalties for delayed enrollment
• Enrolling in limited income subsidy program•Will beneficiaries, not auto-enrolled, know they are eligible? •Will they sign up?
• Comparing plans and deciding which to join•Will face wide variations in premiums, benefit design, formularies and preferred drug lists each year
• Facing potential consequences of a bad decision•Annual lock-in
• Tracking and affording their total and out-of-pocket Rx costs• Important due to benefit gap•Who will manage?
25

26
What do Beneficiaries Need to Consider?
• Assess current health insurance coverage•Are prescription drugs covered?•What is current cost?•Are current benefits equal to or richer than Part D benefits?
• Determine if they qualify for low income subsidy assistance
• If selecting the PDP or MA-PD plan, are current medications on formulary?
• Enroll by May 15, 2006 to avoid possible late enrollment penalty
26

27
Medicare Part D Plan Finder Tool-Supporting Part D Enrollment
• Prescription Drug Plan Finder Tool on www.medicare.gov launched October 17, 2005
• The Prescription Drug Plan Finder tool will:•Only be accessible through www.medicare.gov•Provide plan cost, drug pricing and pharmacy network information for all PDPs and MA-PDs
•Provide ranking of plan’s net cost based on beneficiary’s location, income level, drugs, and pharmacy selection
•Update pricing information weekly
• The Prescription Drug Plan Finder Tool will not: •Make specific plan recommendations
27

28
Nexavar REACH Program
Resources for Expert Assistance and Care Helpline
Reimbursement Services Toll-Free Number
1-866-NEXAVAR
A REACH Program Counselor will help to:
• Answer questions about insurance coverage, including questions about the new Medicare Part D drug benefit
• Assist with insurance verifications for Nexavar
• Identify and assist with applying for alternate sources of coverage and payment for Nexavar
• Review eligibility, if necessary, for Nexavar patient assistance for uninsured patients
• Identify a specialty pharmacy that will fill prescriptions and ship directly to the patient’s home

29
Conclusion• Medicare Part D benefit will provide greater access to
medications for Medicare beneficiaries
• Medicare beneficiaries will look to providers for assistance in selecting the appropriate plan and navigating the appeals process
• Education and communication will be key in ensuring successful implementation of the Part D benefit
• Beneficiaries should be directed to utilize the resources and support services being provided through Medicare and other organizations
• Bayer/Onyx REACH Program can assist providers and patients with reimbursement services related to Medicare and all other payers