Embed Size (px)
Citation preview
RESPIRATORY SYSTEM HISTOLOGY
1

Respiration
Mechanical respiration which involves the following steps: Air is drawn into the body (to the lungs) from the
atmosphere by inhalation. Before it reaches the lungs, the air is cleaned by removal
of particulate matter, warmed so that its temperature equals that of the body, and moistened.
In the lung parenchyma, oxygen is extracted from the air and transferred into the blood vascular system where it bonds tightly with hemoglobin in the red cells for transport in the systemic arterial circulation.
At the same time that oxygen is passing from air into the blood, carbon dioxide is transferred from the blood to the air.
After gaseous exchange, the air is returned to the atmosphere by exhalation.
2

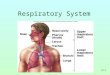
Respiratory System
The respiratory system has two main functional elements a conducting/cleaning system and respiratory portion,
A conducting portion (where there is no gas exchange), consisting of the nasal cavity, pharynx, larynx, trachea, bronchi, bronchioles, and terminal bronchioles.
A respiratory portion (gas exchange takes place), consisting of respiratory bronchioles, alveolar ducts, alveolar sacs and alveoli. Gas exchange occurs in alveoli, which first appear on the respiratory bronchioles.
3

Respiratory system
4

1.Conducting portion/cleaning system
Nasal cavity, nasopharynx, oropharynx, larynx, trachea, bronchi, bronchioles and terminal bronchioles.
Cleansing, warming and moistening of air before it reaches the sites where gas exchange occurs.
These cavities are lined by respiratory epithelium with two cell types, one of which secretes mucus which traps particulate matter, and the other bears surface cilia which moves the thin layer of mucus.
Abundant blood vessels beneath the epithelium warm the air.
Seromucous glands secrete both mucus and a watery fluid which moistens the air.
Lymphoid tissue in the nasopharynx provides immunological surveillance against inhaled antigens.
5

2. Respiratory portion of the respiratory system
Respiratory bronchioles, alveolar ducts alveolar sacs, and alveoli, all of which are located within the lung.
The exchange of gases takes place in this portion of the respiratory system.
6
Respiratory epithelium (cell types)
Ciliated columnar cells Goblet cells Brush cells Basal cells Small granule cells Clara cells
7

Ciliated columnar cells
Columnar cells extend from the basal membrane to the luminal surface.
200-300 apical motile cilia/cell that project into the mucus.
Many mitochondria exist near the basal bodies, providing the ATP required for ciliary beating.
Function – The cilia are motile and beat to help move the secreted mucus layer out of the respiratory system.
8
In the respiratory system, the surface modification consists of cilia (arrow). In addition, goblet cells (arrowhead) are
present in the tissue

Goblet cells
Goblet cells secrete a polysaccharide mucous material into the lumen of trachea.
Mucus production is supplementd by secretions of the submucosal mixed glands.
The mucus layer traps particulate substances (dust, bacteria and virus) and absorbs noxious water-soluble gases such as Ozone and So2.
9

Goblet cells
The mucus sticky layer is moved by the beating cilia toward the pharynx where it is swallowed. This movement is known as Mucociliary Escalator System.
10

Ciliated and Goblet cell
11

Brush cells
Brush cells may represent goblet cells that have secreted their products or intermediate stages in the formation of goblet or the tall ciliated cells.
They have short blunt microvilli on their apical surfaces.
Some of these cells have synapses with intraepithelial nerves, suggesting that these cells may be sensory receptors.
12

Short or basal cells
These cells rest on the basal lamina but do not extend to the lumen.
Are able to divide and replace the other cell types.
These cells, along with epithelial neuroendocrine cells, are responsible for the pseudostratified appearance of the trachea.
13

Small granule cells
These cells occur in clusters, resemble basal cells but contain secretory granules concentrated in their basal cytoplasm are comparable to the endocrine cells in the gut.
APUD cells (Amino Precursor Uptake Decarboxylase), K (Kulchitsky) cells or DNES (Diffuse Neuro Endocrine System), Argentaffin are various name for the cells.
The granules in these neuroendocrine cells contain hormones,active peptides, bombesin (gastrin-releasing factor), leu-enkephalin, serotonin and somatostatin.
They are often located at airway branch points.
14

Clara cells (Bronchiolar secretory cells )
Non ciliated and secrete a serous solution similar to surfactant (glycosaminoglycans) that decrease surface tension of fluid that moistens the surface of lung epithelia.
They have a peculiar domed apex that contains numerous apical granules.
Clara cells are most abundant in the terminal bronchioles (80% of the epithelial
lining).
15

Functions of Clara cells
They aid in the detoxification of airborne toxins, and serve as a stem cell for the ciliated cells and for themselves.
The number of clara cells increases in response to increased level of pollutants like cigarette smoke.
They are also involved with chloride ion transport into the lumens of the terminal bronchioles.
16

Clinical considerations
The columnar ciliated and goblet cells are sensitive to irritation. The ciliated cells become taller and there is an increase in the number of goblet cells and submucosal glands.
Intensive irritation from smoking leads to a squamous metaplasia where the ciliated epithelium becomes a squamous epithelium. This process is reversible.
17
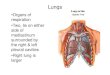
Nasal cavity
Divided into the external nares and the internal nasal cavity.
External nares - their outer portions are lined by thin skin. They open into the vestibule
Nasal cavity is divided in half by the nasal septum.
Floor of the nasal cavity is formed by the palate. Anterior is the hard palate. Posterior is the
soft palate. It is primarily composed of skeletal muscle.
Particles 10 microns in diameter or larger are trapped in the nose and are removed by sneezing, blowing or swallowing. 18

Nasal cavity
The vestibule is the first portion of the nasal cavity, where the epithelial lining becomes nonkeratinized.
Posteriorly, the lining changes to respiratory epithelium (pseudostratified ciliated columnar epithelium with goblet cells).
The vestibule contains vibrissae (thick short hairs), which filter large particles from the inspired air.
It has a lamina propria that is vascular (many venous plexuses) and contains seromucous glands.
19
Nasal cavity
20

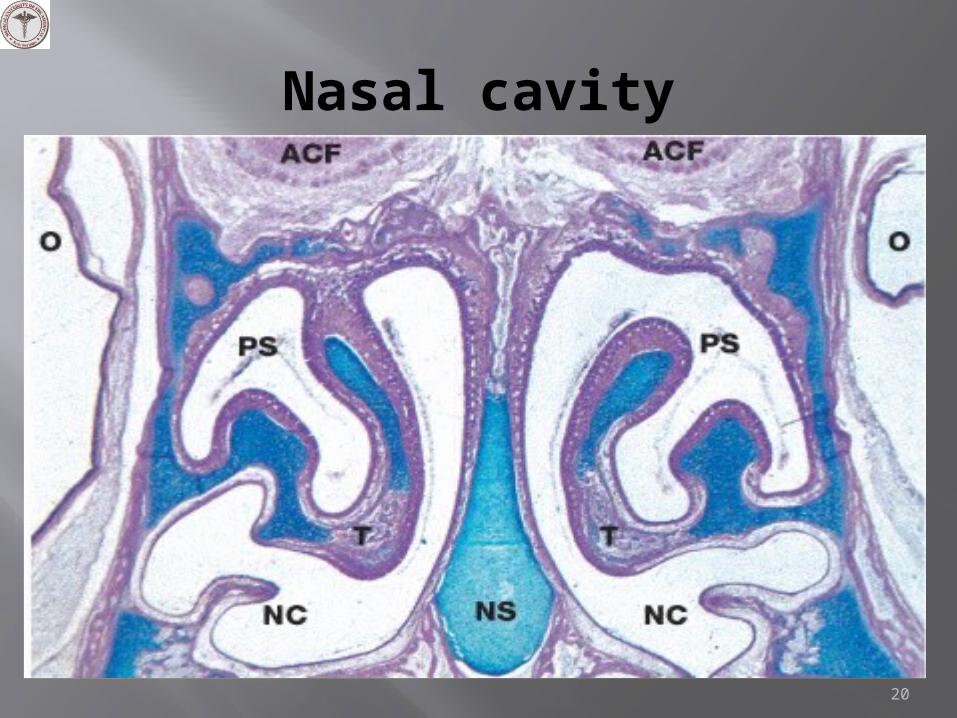
Lateral walls of the nasal cavity
3 pairs of nasal conchae (turbinate). superior, middle and inferior nasal
conchae. The nasal conchae make airflow within
the nasal cavity turbulent. The turbulence slows the flow of air down which increases the available time for inspired air to be filtered, warmed, and humidified. Also, provide a sensory surface for olfaction.
21
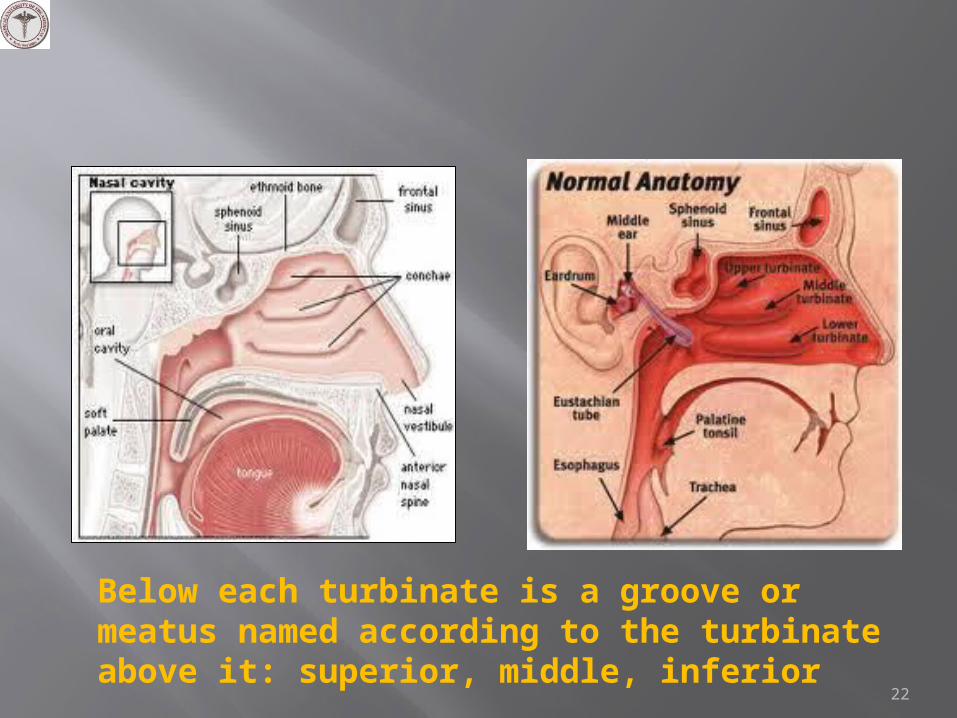
Below each turbinate is a groove or meatus named according to the turbinate above it: superior, middle, inferior
22
Olfactory epithelium
The olfactory epithelium is located in the roof of the nasal cavity, on either side of the nasal septum and on the superior conchae (inferior and middle conchae have respiratory epithelium).
It is a tall pseudostratified columnar ciliated epithelium (nonmotile cilia without goblet cell) consisting of olfactory cells, supporting (sustentacular) cells, and basal cells. It has a lamina propria that contains many veins and
unmyelinated nerves and Bowman glands. Bowman glands produce serous fluid, which dissolves
odorous substances.
23

Olfactory MembraneOlfactory epithelium
Lamina propria with nerve bundles ( ) and Glands of Bowman ( )

Olfactory epithelium
1. Olfactory cell 2. Supporting (sustentacular) cells 3. Basal cells 4. Bowman’s glands
25
1. Olfactory cells (neurons)
Olfactory cells are bipolar nerve cells (modified neurons)
A single dendrite extends to the surface to form a swelling, the olfactory vesicle, from which nonmotile cilia. These cilia increase surface area and act as receptors for odor.
Axons carry the action potential to the olfactory lobe of the CNS.
26

27
Olfactory epithelium

Olfactory epithelium2. Supporting (sustentacular) cells:
Are the most numerous cells. The nuclei of these tall columnar cells are more apically located
than those of the other two cell types. Lipofuscin granules are present.
Many microvilli are present.
3. Basal cells: The basal cells are stem cells that continuously turn over to
replace the olfactory receptor cells. This is the only example in the adult human where neurons are replaced.
4. Bowman’s glands (serous acini in lamina propria) produce a thin, watery secretion that is released onto the olfactory epithelial surface via narrow ducts. Odorous substances dissolved in this watery material are detected by the olfactory cilia. The secretion also flushes the epithelial surface, preparing the receptors to receive new odorous stimuli.
28

Swell bodies
Within the lamina propria of the conchae are large venous plexuses known as swell bodies.
Every 20 to 30 min, the swell bodies on one side of the nasal fossae become engorged with blood, resulting in distention of the conchal mucosa and a concomitant decrease in the flow of air. During this time, most of the air is directed through the other nasal fossa. These periodic intervals of occlusion reduce airflow, allowing the respiratory epithelium to recover from desiccation.
In addition to swell bodies, the nasal cavity has a rich vascular system.
29

Epiglottis
The epiglottis is a flap of tissue containing elastic cartilage, which directs swallowed food into the esophagus and prevents it from entering the larynx.
The epiglottis, which projects from the rim of the larynx has both a lingual and a laryngeal surface.
The entire lingual surface and the apical portion of the laryngeal surface are covered with nonkeratinized stratified squamous epithelium. Toward the base of the epiglottis on the laryngeal surface, the epithelium undergoes a transition into ciliated pseudostratified columnar epithelium.
Mixed seromucous glands are found beneath the epithelium.
30

Epiglottis
Core of Elastic cartilage covered by a respiratory mucus membrane
31
Larynx
The larynx connects the pharynx with the trachea , the passageway for air between the oropharynx and trachea.
The wall of the larynx is supported by hyaline cartilages (thyroid, cricoid, and lower part of arytenoids) and elastic cartilages (epiglottis, corniculate, and tips of arytenoids).
The larynx helps in the production of voice (phonation).
32

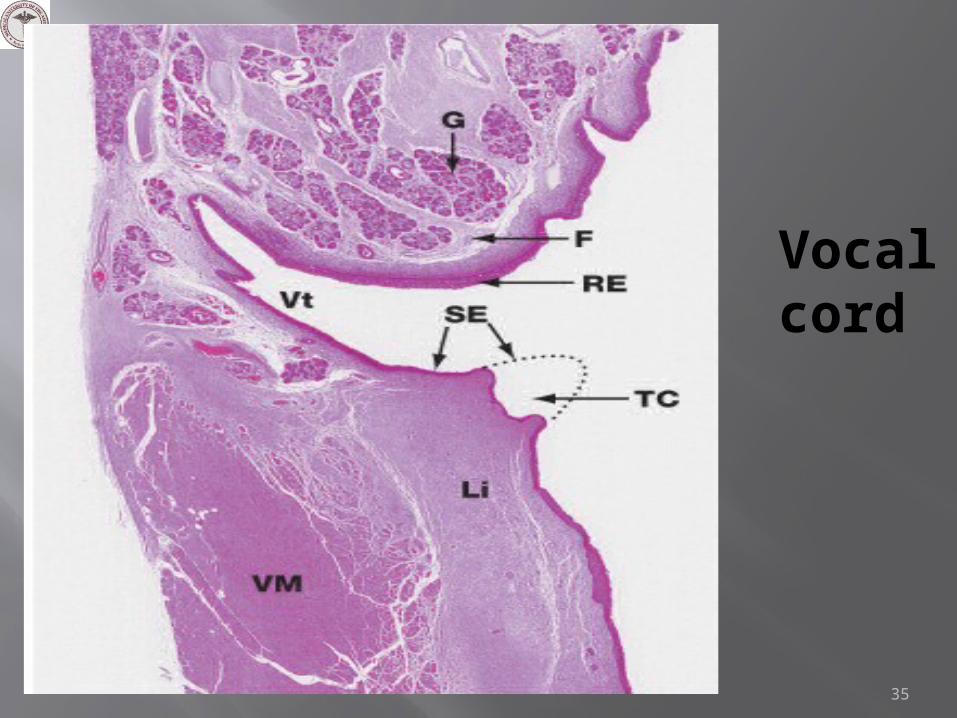
Vocal cords
These are two folds of mucosa that project into the lumen of the larynx.
The vocal cords consist of : A covering of stratified squamous nonkeratinized
epithelium on the superior surface. Vocal ligament (formed by a band of elastic fibers), and Vocalis muscle (skeletal muscle)
Inferior to the vocal cords, the lining epithelium changes to respiratory epithelium, which lines air passages down through the trachea and intrapulmonary bronchi.
Contraction of the laryngeal muscles changes the size of the opening between the vocal cords, which affects the pitch of the sounds caused by air passing through the larynx.
33

34
Vocal cord
35

Thyroid cartilage protects the vocal cords and assists in phonation. The structure consists of hyaline cartilage (HC) covered by a perichondrium, which anchors the
structure to the surrounding connective tissue. In this specimen, a layer of adipose tissue separates the perichondrium from the connective tissue of the vocalis muscle
(arrow). 36

False vocal cords
Above the true vocal folds is an elongated recess in the larynx called the ventricle.
A pair of mucosal folds situated immediately above the ventricle is ventricular folds or false vocal cords.
These are covered with typical respiratory epithelium beneath which lie numerous seromucous glands within the lamina propria.
They do not modulate in phonation.37
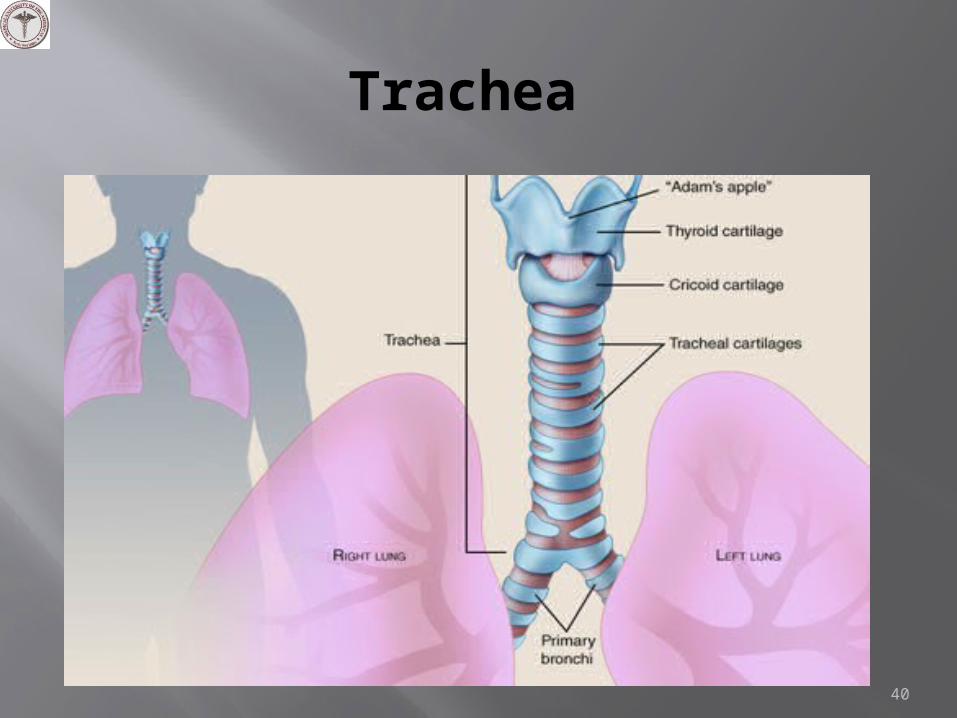
Trachea
Trachea is a hollow tube (10 cm long), extends from the larynx to its bifurcation at the carina where it divides into the two main or primary bronchi.
The most striking structures of the trachea are the C-shaped hyaline cartilage (16-20), distributed along the length of the trachea.
The rings overlap in the anterior part but free posterior ends are interconnected by fibroelastic tissue and trachealis smooth-muscle bridge the gap.
The wall of the trachea consists of 4 layers: Mucosa Submucosa Cartilaginous layer Adventitia
38
Tracheal wall Mucosa:
1. Epithelium - pseudostratified columnar ciliated with goblet cell.2. Thick basement membrane and 3. Lamina propria- consists of loose connective tissue, blood
vessels and lymphatic aggregations. Beneath it is a layer made up of elastic tissue (elastic lamina).
Submucosa - composed of relatively denser irregular connective tissue and seromucous glands (mixed acini) contains the secretory components of serous and mucous glands whose ducts empty into the tracheal lumen.
Cartilaginous layer, composed of C-shaped hyaline cartilage covered by perichondrium.
• Adventitia, outer covering of the trachea composed of connective tissue that binds the trachea to adjacent structures (esophagus).
39
Trachea
40

41

42
Layers and components of a trachea

The trachea and primary bronchi
Epithelium - pseudostratified with cilia and goblet cells with a thick basement membrane.
Lamina propria of loose connective tissue
Elastic lamina of longitudinally arranged elastic fibers.
Submucosa with mixed glands
C-shaped cartilage rings.
Adventitia is present.
43

The ciliated epithelium and hyaline cartilage (arrow) of the bronchus. The hyaline cartilage is arranged as plates of tissue in the bronchial wall and is covered by a perichondrium. The structure is surrounded by the
alveoli of the lung.44
Bronchus

Division of Trachea
The trachea divides into two branches forming the main (primary) bronchus.
On entering the hilum of the lung each main (primary) bronchus divides into the lobar or secondary bronchi.
Right bronchus divides into three lobar or secondary bronchial branches and the left into two.
Further, in the right lung the lobar bronchi give rise to 10 segmental or tertiary bronchi and the lobar bronchi of the left lung give rise to 8 segmental bronchi.
45

46

Bronchial-associated lymphoid tissue (BALT)
Bronchial-associated lymphoid tissue (arrow) can be found in the mucosa of the bronchus and forms an important defensive tissue protecting the entrance of the lungs from pathogens.
The tissue is not encapsulated and consists of diffuse accumulations of phagocytic cells, lymphocytes, and plasma cells.
47

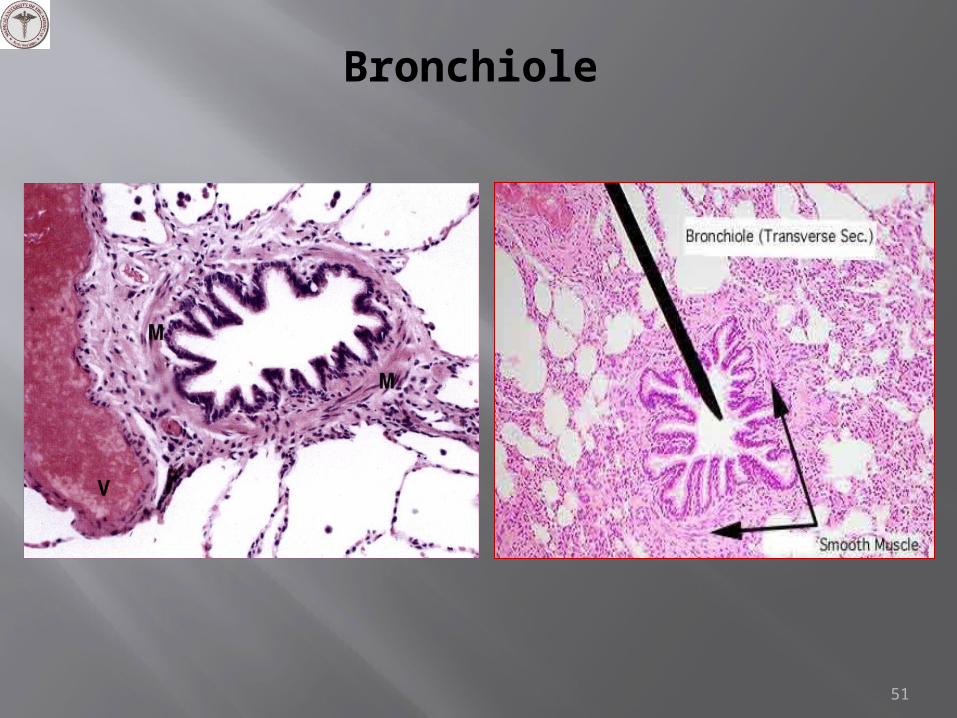
Bronchioles
Diameter 1 mm or less Epithelium is simple columnar to simple cuboidal
with fewer cilia. Non-ciliated Clara cells are present in epithelium.
The greatest changes in histology occur in the walls of the bronchioles as glands and cartilage are eliminated.
The smooth muscle layer is well developed. Elastic fibers are prominent. Lambert’s canal - direct communication between
bronchioles and adjacent alveoli.
48
3 Types of Bronchioles
Large (muscular) bronchioles - branch repeatedly, final branches are the terminal bronchioles. Epithelium is ciliated simple columnar to cuboidal with
interspersed clara cells.
Terminal bronchioles - form connection between larger bronchioles and respiratory bronchioles. Is the last conducting bronchiole. This bronchiole is followed by respiratory bronchioles which are
periodically interrupted by alveoli in their walls. Goblet cells are absent but sparse ciliated cuboidal
epithelium is present to prevent the movement of mucous into the alveoli.
Clara cells are most abundant in terminal bronchioles (80% of the epithelial lining) and secrete a mucus-poor, watery proteinaceous secretion.
49

Respiratory bronchioles - form connection between terminal bronchioles and alveolar ducts This is the transitional structure connecting the
conducting zone to the respiratory zone. Structures similar to the terminal bronchioles,
but the wall is interrupted by alveoli Alveoli open into this structure along its length. Clara cells are abundant in epithelium.
50
A respiratory bronchiole (arrow) and its accompanying pulmonary artery (arrowhead)
Bronchiole
51

TEM of Bronchiole Epithelium
Cla, Clara Cells; Cil, Ciliated Columnar

Components of the respiratory portion of the respiratory system
53

Respiratory portion of the respiratory system
Each respiratory bronchiole divides into several alveolar ducts.
The alveolar ducts end in an alveolar sac, which in turn opens into several alveoli.
The epithelium of the respiratory bronchioles is devoid of goblet cells and contain smaller numbers of non-ciliated cells called Clara cells.
In the most distal part of the respiratory bronchioles Clara cells become the predominant cell type.
54

Terminal portion of the respiratory tree
55

Trachea Bronchi Bronchioles
Epithelia Pseudostratified ciliated
columnar cells, goblet cells
PCC to simple columnar cells
Ciliated, Clara cells in terminal
bronchioles
Cartilage 16-20 “C” shaped cartilage
Irregular plates None
Glands Seromucous glands
Few glands None
Smooth muscles
Between open ends of “C”
shaped cartilage
Prominent Highest proportion in bronchial tree
Elastic fibres Present Abundant Abundant
56

Alveolar ducts, Alveolar sacs and the Alveoli
The alveolar ducts and sacs have little or no walls and consist almost entirely of alveoli.
Elastic and reticular fibers provide support to these ducts.
The alveoli constitute 80 to 85 % of the volume of the normal lung. Alveoli are the terminal, thin-walled sacs of the respiratory tree that are responsible for gas exchange.
The cuboidal epithelium of the respiratory bronchioles and the alveolar ducts are continuous with squamous cells lining the alveoli composed of type I and type II pneumocytes.
57

Alveoli
Each alveolus is surrounded by a dense network of capillaries. The extremely thin walls of the alveoli allow gaseous exchange.
They are separated from each other by interalveolar septae, which may contain one or more alveolar pores (pores of Kohn).
These pores permit equalization of pressure between alveoli.
They are rimmed by elastic fibers at their openings and are supported by many reticular fibers in their walls.
58

59

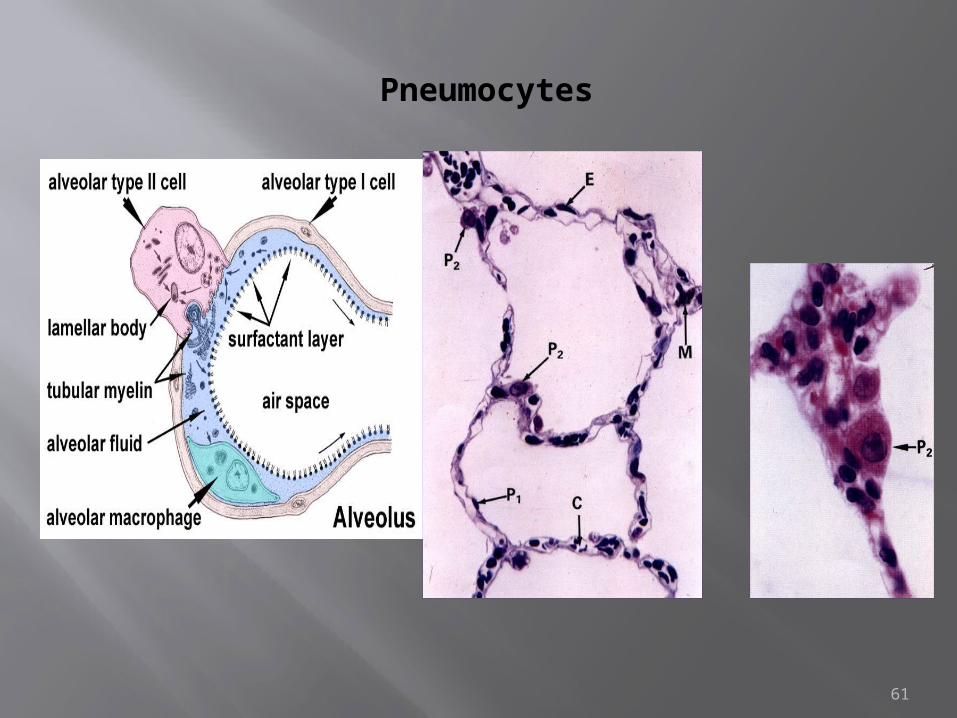
Type I pneumocytes(small alveolar cells or alveolar type I cell)
These cells represent only 40% of the alveolar lining cells but cover about 95% of the alveolar surface.
Flat cells with thin cytoplasm having pinocytic vesicles.
Junctional complexes (desmosomes & tight junctions) with adjacent cells.
They can not divide. The blood-air barrier is formed by the type
I pneumocyte, the capillary endothelial cell, and their fused basal laminae.
60

Type II pneumocytes(great alveolar cell)
Granular pneumocyte, septal cell, corner cell, niche cell or alveolar type II. They constitute 60% of the cells lining the alveoli; they form only 5 to 10% of the surface.
Type II cells are cuboidal-like cells that rest on the basal lamina of the epithelium and contain membrane-bound granules of phospholipid and protein (lamellar bodies).
The contents of these lamellar bodies are secreted onto the alveolar surface to provide a coating of surfactant that reduces alveolar surface tension.
The type II cells serve as stem cell for themselves and type I cells.
62

Secretion of surfactant by a type II cell
63

Alveolar macrophages (alveolar phagocytes; dust cells)
They are derived from monocytes that exit the blood vessels in the lungs. The resident alveolar macrophages can undergo limited mitoses.
These cells can reside in the interalveolar septa or in the alveoli (1-3 per alveolus)
Alveolar macrophages continuously remove particles and other irritants in the alveoli by phagocytosis.
Macrophages can pass out of the alveoli to the bronchioles and enter the lymphatics or become trapped in the moving mucus layer towards the pharynx to be swallowed and digested.
64

Alveolar macrophages (alveolar phagocytes; dust cells)
65
The blood-air barrier
This refers to the substances/structures that lie between the air in the alveolar sacs and the blood in the capillaries.
The blood-air barrier prevents air in gaseous form from mixing with the blood.
Starting in the alveolar lumen this barrier consists of Surfactant Type I alveolar cells lining the alveolus Basal lamina of both alveolar cells and capillary endothelial
cells (fused in some areas) Non-fenestrated (continuous) endothelium of capillary In areas where basal lamina of the two endothelial layers are
not fused, reticular and elastic fibers are present.
66
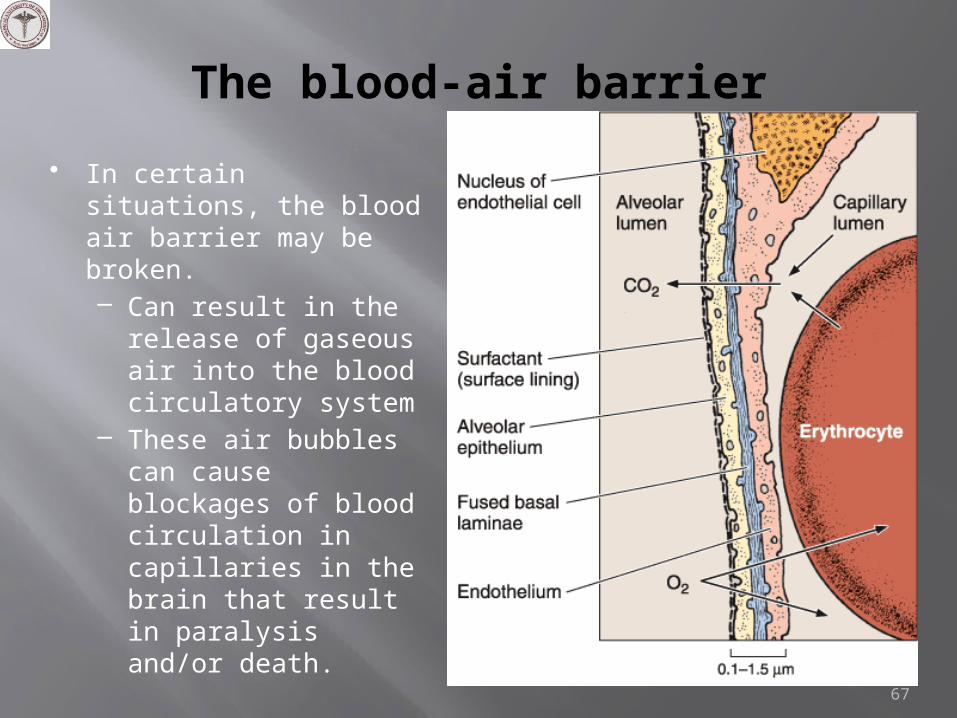
The blood-air barrier
67
• In certain situations, the blood air barrier may be broken. – Can result in the
release of gaseous air into the blood circulatory system
– These air bubbles can cause blockages of blood circulation in capillaries in the brain that result in paralysis and/or death.

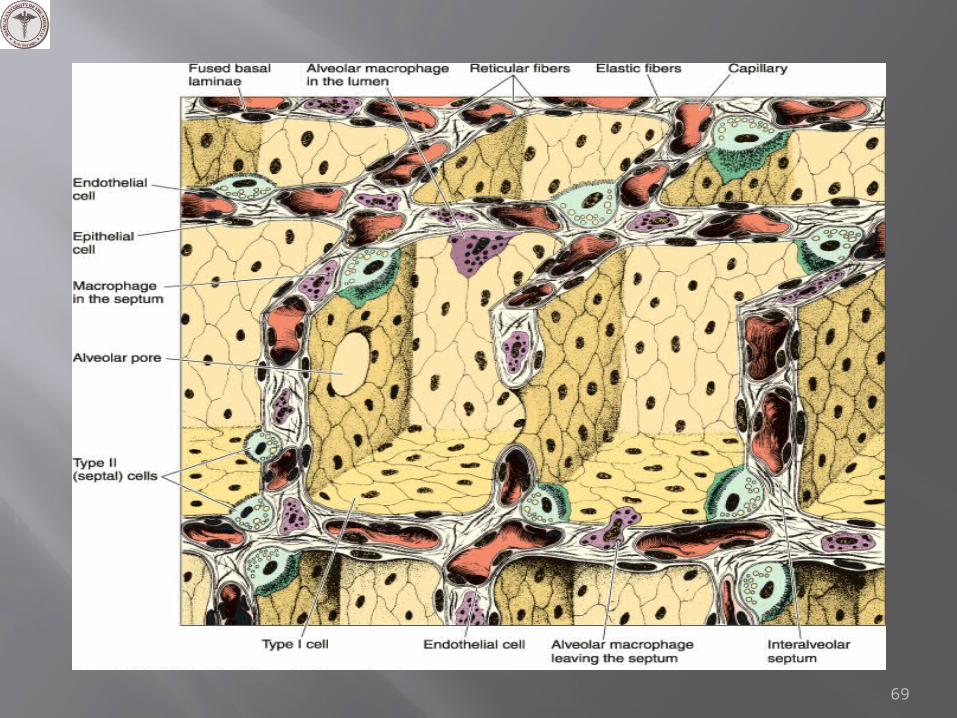
Interalveolar septum
An alveolar septum consists of two thin squamous epithelial layers between which lie capillaries, fibroblasts, elastic and reticular fibers, and macrophages.
Within the interalveolar septum, anastomosing pulmonary capillaries are supported by a meshwork of reticular and elastic fibers.
68
69

Pleura
The pleura is the serous membrane covering the lung consists of two layers, parietal and visceral.
Both membranes are composed of mesothelial cells (simple squamous) resting on connective tissue layer that contains collagen and elastic fibers.
This pleural cavity contains only a film of liquid that acts as a lubricant during respiratory movements.
70

Emphysema
Etiology: cigarette smoke and air pollution substances that inhibit anti-proteases, a protein that normally protects the lungs from the action of elastase produced by alveolar macrophages and neutrophils.
It can be a hereditary condition resulting from a defective α1-antitrypsin.
In smoking there is an increase in the neutrophils and macrophages in alveoli and increased elastase activity from these leading to the destruction of the bronchiolar and alveolar septal elastic tissue support.
71

Emphysema
Abnormal permanent enlargement of the air spaces distal to the terminal bronchiole due to destruction of their elastic tissue support.
All or the part of the respiratory unit (respiratory bronchiole, alveolar ducts and alveoli) may be involved.
Loss of elastic recoil allows small airways to collapse at the beginning of expiration and enlarged air spaces.
The destruction of the elasticity in emphysema leads to diminished breath sounds.
72

Emphysema
73
• Barrel chest• Thinning and destruction of alveolar walls.• Adjacent alveoli fuse resulting in large airspaces• Permanent dilatation of the air spaces

74
• Protease/ antiprotease imbalance• Proteases (including elastase) are
produced by neutrophils and macrophages.
• Anti-proteases include α1-antitrypsin, α1-macroglobulin, and secretory leukoprotease inhibitor.
Clinical presentation
Progressive dyspnea Prolonged expiration
and hyperventilation Attempting to squeeze
air out of the lungs with pursed lips. To prevent respiratory
bronchioles from collapsing.
Diminished breath sounds due to lung hyperinflation.
• Barrel chest (increased AP diameter)
75

Asthma
Asthma is characterized by hyper-reactivity of the respiratory tree to various stimuli leading to narrowing of airways due to bronchospasm.
Types: Extrinsic asthma (allergic, atopic) Intrinsic asthma (non-allergic asthma)
Constriction of bronchial muscles, mucosal inflammation and excessive secretion of mucus (reversible).
Clinically presentation: Dyspnea (difficulty in breathing) Wheezing (a soft whistling sound during expiration) Diminished breath sounds Nocturnal cough Increased AP diameter due to air trapping.
76

77