Embed Size (px)
Citation preview
1
Investor Presentation
March 2010
2Forward-Looking Statements
This presentation contains forward-looking statements made pursuant to the safe harbor provisions of the U.S. Securities Litigation Reform Act of 1995. Forward-looking statements involve known and unknown risks and uncertainties, which could cause the Æterna Zentaris’ actual results to differ materially from those in the forward-looking statements. Such risks and uncertainties include, among others, the availability of funds and resources to pursue R&D projects, the successful and timely completion of clinical studies, the ability of the Company to take advantage of business opportunities in the pharmaceutical industry, uncertainties related to the regulatory process and general changes in economic conditions. Investors should consult the Company’s quarterly and annual filings with the Canadian and U.S. securities commissions for additional information on risks and uncertainties relating to the forward-looking statements. Investors are cautioned not to rely on these forward-looking statements. The Company does not undertake to update these forward-looking statements and disclaims any obligation to update any such factors or to publicly announce the result of any revisions to any of the forward-looking statements contained herein to reflect future results, events or developments, except if we are required by a governmental authority or applicable law.

3Æterna Zentaris
Late-Stage Drug Development Company Specialized in Oncology
and Endocrinology

4Æterna Zentaris
Management team
Juergen ErnstExecutive Chairman 30+ years experience: Solvay
Juergen Engel, Ph.D.President and CEO 30+ years experience: ASTA Medica
Paul Blake, M.D.Senior VP and CMO 25+ years experience: Cephalon, SmithKline Beecham
(now GSK), ICI Pharmaceuticals (now Astra Zeneca)
Nicholas J. Pelliccione, Ph.D.Senior VP, Regulatory Affairs and QA 20+ years experience: Chugai Pharma USA , Schering-
Plough
Matthias Seeber, M.B.A.Senior VP, Administration and Legal Affairs 15+ years experience: Altana AG, Deka Investment
Management, Dresdner Bank AG
Dennis Turpin, CASenior VP and CFO 20+ years experience: Coopers & Lybrand (now PWC)

5Late-Stage Oncology & Endocrinology Pipeline
Compound Indication Preclinical Phase 1 Phase 2 Phase 3 Commercial
Perifosine
Multiple Myeloma
Metastatic Colon Cancer
Kidney Cancer and Others
AEZS-108
Endometrial Cancer
Ovarian Cancer
Other Cancers
AEZS-112 Solid Tumor
AEZS-120 Tumor Vaccine
Prostate Cancer
AEZS-129/131 PI3K/Erk Inhibitor
Oncology
Cetrotide® In Vitro Fertilization
AEZS-130 (SolorelTM)
Diagnostic – Adult Growth Hormone Deficiency
AEZS-130 (macimorelin)
Therapeutic – Endocrinology
AEZS-123 Ghrelin Antagonist
Endocrinology
Partners: Merck Serono, Nippon Kayaku / Shionogi (Japan)
Partners: Keryx (North America) & Handok (Korea)
Partners: Keryx (North America) & Handok (Korea)
Partners: Keryx (N. America) & Handok (Korea)

6Vision & Business Strategy of Æterna Zentaris
Our vision: to become a fully-integrated specialty biopharmaceutical company
Our Business Development Strategy
− To retain co-marketing and/or co-promotion rights for our products
− To retain rights for certain territories for our products
− To have access to the development data of Licensee at no cost outside their territory
• Example: Perifosine (Keryx for North America and Handok for Korea)
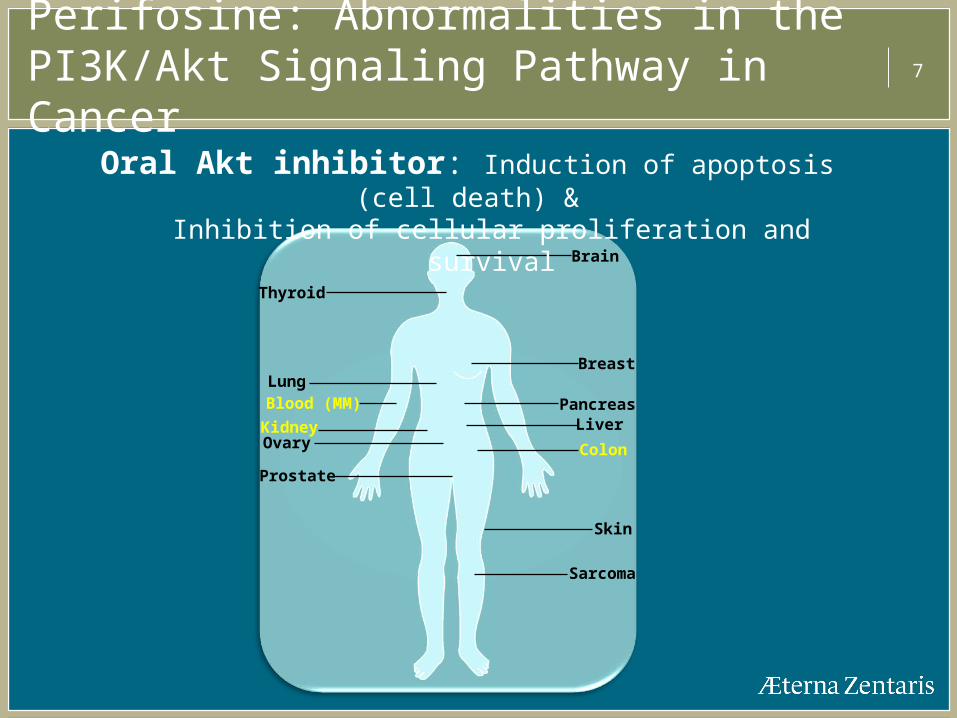
7Perifosine: Abnormalities in the PI3K/Akt Signaling Pathway in Cancer
Brain
Breast
Pancreas
Colon
Liver
Prostate
Skin
Ovary
Blood (MM)Lung
Thyroid
Sarcoma
Kidney
Oral Akt inhibitor: Induction of apoptosis (cell death) &Inhibition of cellular proliferation and survival

8
0
20
40
60
80
100
120
0 5 7.5
Bortezomib (nM)%
con
trol
24hPerifosine (μM)
0
2.5
5
Reference: Hideshima et al. Blood 2006
Perifosine in Multiple Myeloma (MM):Synergistic Effect to Velcade®
Velcade® (bortezomib)
caspase ↑ Akt ↑
anti-apoptosis
Perifosine blocksVelcade®-activated Akt
apoptosis
20 nM
Perifosine (-) Perifosine (+) 5 μM
p-ERK
p-Akt
0 5 10 20 0 5 10
Akt
ERK2
Velcade®(bortezomib)

9Perifosine in MM: Phase 1 and 2 results
Perifosine + Velcade® +/- Dexamethasone in patients with relapsed / refractory MM
ASH 2009. Poster #1869
Nb of patients
ORR Median TTP
Perifosine + Velcade® +/- Dex
73 41% 6.4 months
Velcade® refractory 53 32% 5.7 months
Velcade® relapsed 20 65% 8.8 months
Perifosine + Velcade® + Dex well tolerated and active in heavily pre-treated and relapsed/refractory MM including Velcade® resistant patients
Durable responses with an extended PFS
10
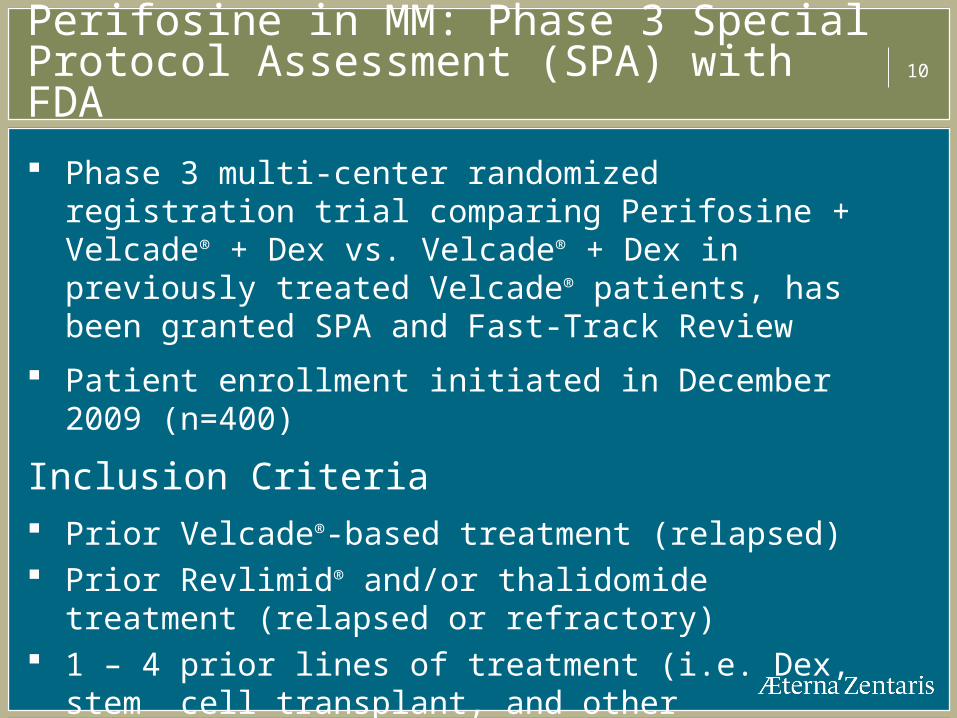
Phase 3 multi-center randomized registration trial comparing Perifosine + Velcade® + Dex vs. Velcade® + Dex in previously treated Velcade® patients, has been granted SPA and Fast-Track Review
Patient enrollment initiated in December 2009 (n=400)
Inclusion Criteria Prior Velcade®-based treatment (relapsed) Prior Revlimid® and/or thalidomide treatment (relapsed or
refractory) 1 – 4 prior lines of treatment (i.e. Dex, stem cell
transplant, and other approved/non-approved MM treatment)
Perifosine in MM: Phase 3 Special Protocol Assessment (SPA) with FDA

11
Randomize
Progression
Off Study
Velcade® 1.3 mg/m2 x 4dDex 20 mg x 8d
Placebo 50 mg daily(n=200 patients)
Progression
Off Study
Velcade® 1.3 mg/m2 x 4d
Dex 20 mg x 8dPerifosine 50 mg daily
(n=200 patients)
Evaluate after 6 wks
If SD or > remain on tx
~ 265 events (PD/death)
Primary EndpointProgression Free Survival
Each cycle = 21 days
Perifosine in MM: Phase 3 Special Protocol Assessment (SPA) with FDA

12Perifosine in MM: Large Market Opportunity
MM is the 2nd most prevalent blood cancer affecting 200,000 people worldwide and nearly 60,000 deaths/year
Prevalence for
− U.S.: 15,000− EU – G5: 16,000− Japan: 3,500
MM U.S. market: Over $3 billion in revenue in the coming years
MM Current therapies
− Velcade® (bortezomib – Millenium/Takeda): 2008 sales > $1 billion− Revlimid® (lenalidomide – Celgene): 2009 sales > $1.7 billion
Source: Globocan 2002 & Frost and Sullivan

13
NF-B
5-FU sensitiveColon Cancer
Apoptosis
+ Xeloda® (capecitabine)
5-FU resistantColon Cancer
+ Xeloda® (capecitabine)
NF-B↑
AKT
Perifosine
IKK
Leleu et al., Blood, 2008.
Synergy 5-FU treatment and Akt inhibition described in Kodach et al., Carcinogenesis, 2006
NF-B↓
Perifosine in Metastatic Colon Cancer (MCC):Synergistic Effect to Xeloda®

14Perifosine in MCC: Phase 2 Results
Group nCR
n (%)
PR
n (%)
SD > 12 wks
n (%)CBR*
PD < 12 wks
n (%)
Xeloda® + Perifosine
20 1 (5%) 3 (15%) 11 (55%) 15 (75%) 5 (25%)
Xeloda® + Placebo
15 0 1 (7%) 5 (33%) 6 (40%) 9 (60%)
* CBR: Clinical Benefit Rate defined as patients on treatment > 12 weeks achieving stable disease (SD) or better; p=0.036
Duration of response: Xeloda® + perifosine: CR – 34 months (ongoing); PR – 21, 19, 11 months Xeloda® + placebo: PR – 7 months
Reference: ASCO-GI Symposium 2010
38 patients were enrolled, of whom 35 were evaluable
Average number of prior therapies: 2
Xeloda® 825mg/m2 BID d1-14 and perifosine 50 mg daily
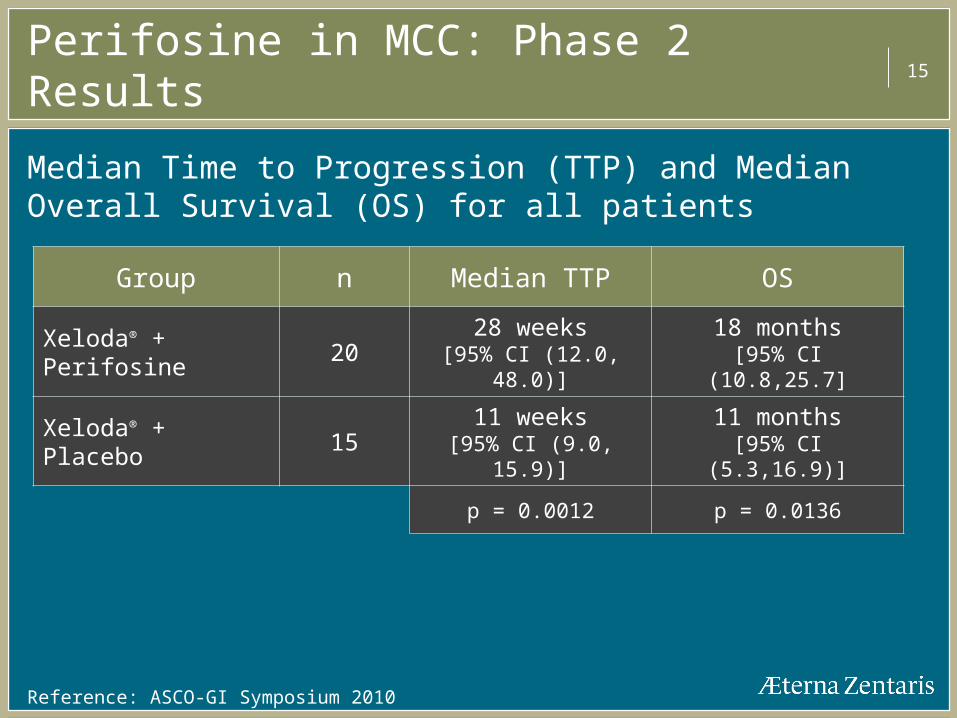
15Perifosine in MCC: Phase 2 Results
Group n Median TTP OS
Xeloda® + Perifosine 20 28 weeks[95% CI (12.0, 48.0)]
18 months[95% CI (10.8,25.7]
Xeloda® + Placebo 15 11 weeks[95% CI (9.0, 15.9)]
11 months[95% CI (5.3,16.9)]
p = 0.0012 p = 0.0136
Reference: ASCO-GI Symposium 2010
Median Time to Progression (TTP) and Median Overall Survival (OS) for all patients

16Perifosine in MCC: Phase 2 ResultsSubgroup of 5-FU Refractory Patients
Group nPR
n (%)
SD > 12 wks
n (%)CBR*
PD < 12 wks
n (%)
Xeloda® + Perifosine
14 1 (7%) 8 (57%) 9 (64%) 5 (36%)
Xeloda® + Placebo
11 0 3 (27%) 3 (27%) 8 (73%)
* CBR: Clinical Benefit Rate defined as patients on treatment > 12 weeks achieving stable disease (SD) or better; p=0.066
Duration of response for PR: 19 months
Reference: ASCO-GI Symposium 2010
A subgroup of 25 patients was evaluable for response

17Perifosine in MCC: Phase 2 ResultsMedian TTP – 5-FU Refractory Patients
A = 11 patients [95% CI (6.6, 11.0)]
B = 14 patients [95% CI (12.0,36.0]
Reference: Bendell J. ASCO-GI Symposium 2010
p=0.0004
10 wks 18 wks
A B

18Perifosine in MCC: Phase 2 Results Median OS – 5-FU Refractory Patients
Reference: Bendell J. ASCO-GI Symposium 2010
A = 11 patients [95% CI (4.8,11.7)]
B = 14 patients [95% CI (8.4,26.0]
p=0.0088
A B
6.8 months 15.3 months
19Perifosine in MCC: Phase 3 Special Protocol Assessment (SPA) with FDA
SPA granted by FDA in February 2010 for Phase 3 X-PECT (Xeloda® + Perifosine Evaluation in Colorectal cancer Treament) trial
Study will be a randomized (1:1), double-blind trial comparing the efficacy and safety of Xeloda® + perifosine vs. Xeloda® + placebo
Approximately 40-50 U.S. sites will participate in the study
Study is expect to begin in Q2-2010 and enrollment is expected to be completed in H2-2011
Primary endpoint is overall survival and secondary endpoints include ORR, PFS and safety

20Perifosine in MCC: Market Opportunity
The fourth most commonly diagnosed cancer and second leading cause of cancer-related deaths in the U.S.
− Prevalence of colon cancer for:
• U.S.: 146,000• EU – G5: 110,000• Japan: 85,000
About one third of patients already have metastatic disease at diagnosis
No new FDA approved drugs since 2006 – need for new agents
Current therapies for 1st and 2nd line of treatment [Xeloda®; Avastin® ; Erbitux®] have overall sales of 4 billion US$
Source: Globocan 2002

21Perifosine in Advanced Metastatic Renal Cell Carcinoma (RCC): Rationale
December 2009, The Journal of Urology, Camillo Porta and Robert A. Figlin:
“Cumulative evidence links PI3K/Akt alterations with RCC and represents an ideal target for therapeutic intervention”
“Only perifosine has already proven to be clinically active”
Reference: J. Urol 2009;182:2569-2577
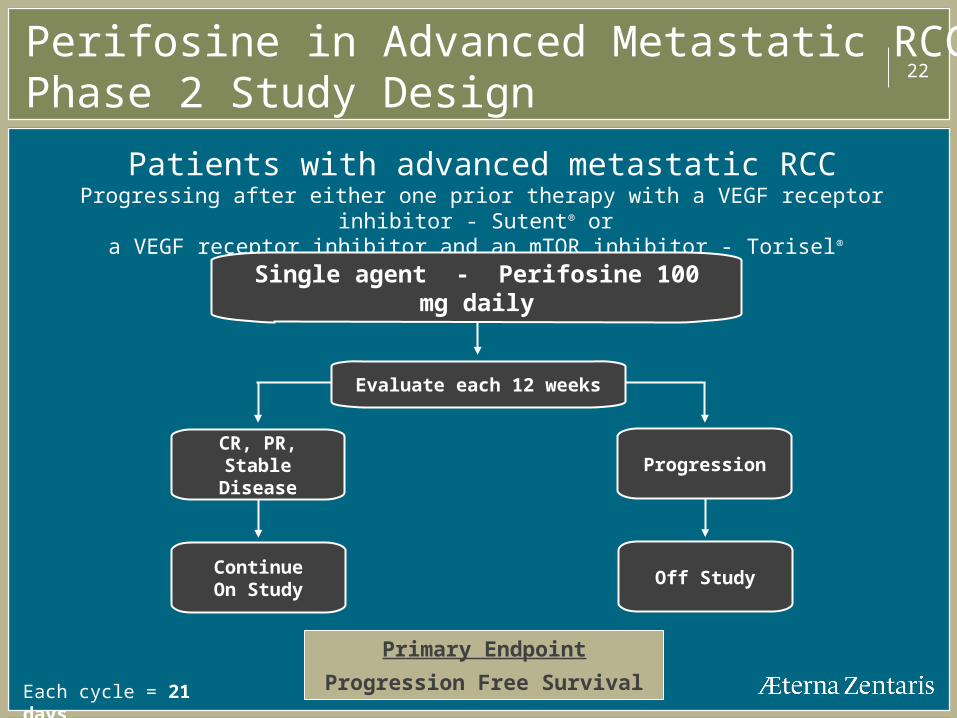
22
Patients with advanced metastatic RCCProgressing after either one prior therapy with a VEGF receptor inhibitor - Sutent® or
a VEGF receptor inhibitor and an mTOR inhibitor - Torisel®
Perifosine in Advanced Metastatic RCC:Phase 2 Study Design
Single agent - Perifosine 100 mg daily
Each cycle = 21 days
Primary Endpoint
Progression Free Survival
Evaluate each 12 weeks
CR, PR,Stable Disease
ContinueOn Study
Progression
Off Study

23Perifosine in Advanced Metastatic RCC: Phase 2 Results - Monotherapy
nPR
n (%)
SD > 12wks
n (%)
Median PFS
(all patients)
Median PFS
(patients SD or >)
Overall
survival
All patients (VEGF-R inhibitor)
Not reached (14/16 alive at 22+ months)
46 5 (11%) 16 (35%)12.5 weeks
[95% CI (11.9, 19)]33 weeks
[95% CI (24,60)]
Refractory patients (VEGF-R inhibitor + mTOR inhibitor)
16 1 (6%) 7 (44%)16 weeks
[95% CI (11.7, 33.6)]33.6 weeks
[95% CI (24, NR)]
Reference: ASCO 2009 and 8th International Kidney Cancer Symposium, Sept 2009
50 patients were enrolled of whom 46 were evaluable − 16 patients were refractory to both VEGF-R and mTOR
inhibitors
24Perifosine Summary
> 1,800 patients studied in Phase 1 and 2
− Single agent and combination− No major haematological toxicity
Phase 3 study in MM with SPA, Fast-Track review and Orphan Drug status granted by FDA and EMA – Patient enrollment initiated in Dec 2009 by our partner Keryx
Phase 3 study in metastatic colon cancer with SPA granted by the FDA – Patient enrollment will be initiated in Q2-2010 by our partner Keryx
Phase 2 studies ongoing in several other tumor types including renal cell cancer, glioma, Waldenstrom’s macroglobulinemia, and AML

25AEZS-108: Magic Bullet Doxorubicin Targeted Conjugate
Binding
Internalization
Nucleus Migration
DOXpayload
LHRH targeting agent
AEZS-108conjugate
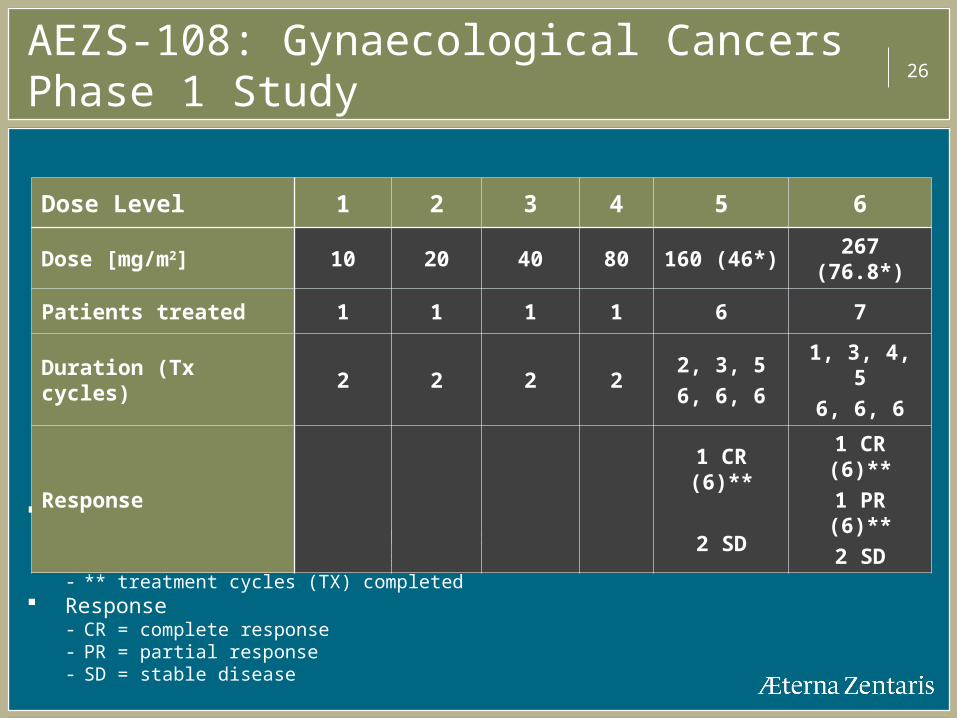
26AEZS-108: Gynaecological Cancers Phase 1 Study
Duration- Re-dosing at 3-week intervals (= 1 cycle)- * equivalent doxorubicin dose - ** treatment cycles (TX) completed
Response- CR = complete response- PR = partial response- SD = stable disease
Dose Level 1 2 3 4 5 6
Dose [mg/m2] 10 20 40 80 160 (46*) 267 (76.8*)
Patients treated 1 1 1 1 6 7
Duration (Tx cycles) 2 2 2 22, 3, 5
6, 6, 6
1, 3, 4, 5
6, 6, 6
Response
1 CR (6)**
2 SD
1 CR (6)**
1 PR (6)**
2 SD

27AEZS-108: Phase 2 Study in Endometrial and Ovarian Cancer
Design− Conventional “Simon Design”− Open-label study in patients with advanced or recurrent
endometrial and platinum-resistant ovarian cancer− Two-stage design with up to 82 patients, 41 patients for each
indication− Opening of stage 2 requires tumor remission in at least 2 of 21
evaluable patients in each indication
Status− Response criteria for opening stage 2 were met for both indications− Enrollment for second stage completed for both indications− Preliminary evaluation revealed that primary endpoint of 5 or
more responders was met for both indications− Study ongoing for PFS and OS

28AEZS-112: Oral Tubulin and Topoisomerase II Inhibitor
Novel small molecule with oral capsule formulation
Multiple modes of action:− Inhibition of tubulin polymerization− Inhibition of topoisomerase II− Antiangiogenic properties− Cell cycle arrest
Strong in vivo activity and efficacy in multi-drug resistant (mdr) tumor cell lines
Phase 1 study (Dr Von Hoff, PI): 42 patients treated 12 patients with stable disease and time to failure of 5 – 14+ months Signs of activity in various indications including melanoma and cancers of
colon/rectum, lung, pancreas, prostate.
Safety profile makes AEZS-112 an excellent candidate for drug combinations

29AEZS-120 (Prostate cancer vaccine)
Oral live prostate cancer vaccine Basic feature: recombinant Salmonella strain with proprietary
secretion system of tumor antigen fused to immunostimulatory factor
Bacterial carrier acts as “intrinsic adjuvant” and has the potential to activate components of the innate and adaptive immune system
Based on approved oral typhoid live vaccine Salmonella typhi Ty21a, which has already been safely applied in > 250 Mio. doses
Proof-of-Principle in animal model Off the shelf product, low cost of goods allows flexible pricing
Platform technology

30AEZS-130 (SolorelTM; macimorelin (INN))A Growth Hormone (GH) Secretagogue Oral Ghrelin Mimetic
Oral administration Excellent binding to human ghrelin receptor (agonist
mode) 5 Phase 1 clinical trials completed to date with a total of
100 subjects treated Status: Phase 3 diagnostic of adult GH deficiency Orphan drug status for use as diagnostic test granted by
FDA Potential for Therapeutic indications given AEZS-130’s
GHS Activity and Ghrelin mimetic activity

31GH Concentration Following Oral Administration of AEZS-130 in Healthy Volunteers
0 60 120 180 240
-20
0
20
40
60
80
100
120
GH
con
cent
ratio
n (n
g/m
l)
time (min)
0.005 mg/kg AEZS-130 0.05 mg/kg AEZS-130 0.125 mg/kg AEZS-130 0.25 mg/kgAEZS-130 0.5 mg/kg AEZS-130 Placebo

32AEZS-130 (SolorelTM): Diagnostic Test for Adult GH Deficiency Preliminary Results
Better discrimination between adult GH deficiency patients and normal controls with SolorelTM, oral solution, compared to the currently used test with GHRH-Arginine, i.v. administration
Reference: 2009 ENDO meeting. G. Merriam et al. Poster P2-749
PEAK GH RESPONSES TO GHRH-ARGININE, SOLORELTM, AND ITT
SolorelTM

33Potential Therapeutic Indications for a GHS Ghrelin Mimetic Drug
GHS activity
− Hypo-pituitary deficiency in adults
− Idiopathic short stature, Turner’s syndrome, chronic renal failure in children
− Lipodystrophy associated with HIV treatment
Ghrelin mimetic activity
− Cachexia associated with cancer, COPD and AIDS
• U.S. prevalence for cachexia:
Cancer: 420 000 COPD: 3 200 000 AIDS: 315 000
− Post-operative ileus, diabetic gastroparesis
Ref.: JE Morley et al. Am J clin Nutr 2006;83:735-743

34
Financials

35Selected Annual Financial Results
(in millions of US dollars) For the years ended
December 31, 2009 December 31, 2008Revenues
License fees 42.2 8.5
Sales and royalties 21.0 29.5
Other - 0.5
63.2 38.5
Operating Expenses
Cost of sales, excluding D&A 16.5 19.3
R&D costs, net 43.8 57.1
SG&A expenses 16.0 17.3
D&A 10.8 7.1
87.1 100.8
Loss from operations (23.9) (62.3)
Other income (expenses) (0.8) 3.7
Loss before income taxes (24.7) (58.6)
Income tax expense - (1.2)
Net loss (24.7) (59.8)
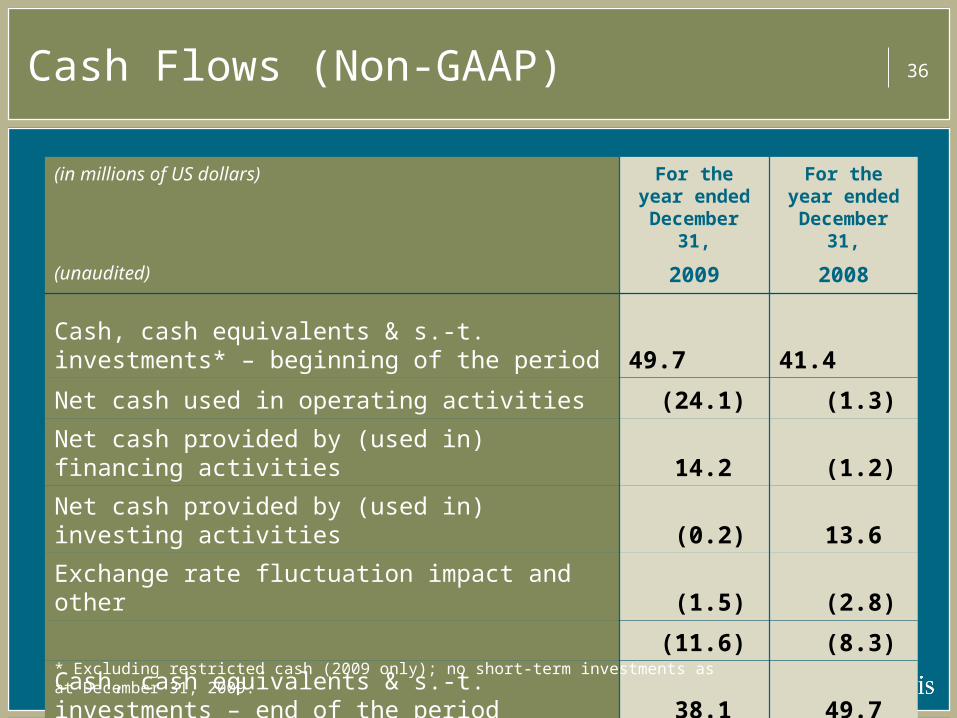
36Cash Flows (Non-GAAP)
(in millions of US dollars) For the year ended
December 31,
For the year ended
December 31,
(unaudited) 2009 2008
Cash, cash equivalents & s.-t. investments* – beginning of the period 49.7 41.4
Net cash used in operating activities (24.1) (1.3)
Net cash provided by (used in) financing activities 14.2 (1.2)
Net cash provided by (used in) investing activities (0.2) 13.6
Exchange rate fluctuation impact and other (1.5) (2.8)
(11.6) (8.3)
Cash, cash equivalents & s.-t. investments – end of the period 38.1 49.7
* Excluding restricted cash (2009 only); no short-term investments as at December 31, 2009.

37
Goals for 2010
382010 Goals
Perifosine: Oral Akt inhibitor Our partner, Keryx, to progress patient enrollment for the
randomized Phase 3 placebo-controlled registration study in multiple myeloma (MM) according to the SPA agreed protocol with FDA
Keryx to initiate a Phase 3 trial in Metastatic Colon Cancer in Q2-2010 according to the SPA protocol with the FDA
Report results for ongoing Phase 2 studies in MM, Metastatic Colon Cancer, Pediatric Solid Tumors and other cancers
AEZS to update development and registration strategy for ex-North American territories, including Europe and Asia

392010 Goals
AEZS-108: Doxorubicin-targeted conjugate Report final results from Phase 2 study in advanced
ovarian and advanced endometrial cancer
Initiation of additional clinical studies in advanced ovarian or advanced endometrial cancer
Initiation of one or more Phase 1/2 trials in other LHRH expressing cancer types

402010 Goals
AEZS-130 (SolorelTM): Oral ghrelin agonist Completion of Phase 3 study for diagnostic test for adult
growth hormone deficiency (GHD)
Filing of an NDA in U.S. as diagnostic test for adult GHD pending successful completion of Phase 3 study
Initiation of clinical program in pediatric GHD
Update development and registration strategy
− “Rest of world” as diagnostic test in adult and pediatric GHD
Explore potential for therapeutic use



























