Embed Size (px)
Citation preview

1
INTRODUCTION1STRUCTURE OF NORMAL BONE
The skeleton serves several important func-tions, for which its structure is ideally suited. First, it performs a mechanical function by supporting the body and providing attachment sites for muscles and tendons that provide mo-tion. Second, it protects vital organs and houses the bone marrow. Third, it serves as a reservoir for various minerals, especially calcium, and has a role in meeting the immediate needs of the organism for calcium (3).
Bones are divided into two main types: the flat bones of the axial skeleton (skull, scapula, clavicle, vertebra, jaw, and pelvis) and the tubu-lar bones of the appendicular skeleton (9). Both types consist of cortical (or compact) bone and cancellous (or spongy) bone.
In a typical long bone such as the femur, the diaphysis, or shaft, is composed of cortical bone surrounding a voluminous marrow, or medul-lary, cavity (fig. 1-1). The epiphyses at the ends of long bones consist mostly of cancellous bone and a thin peripheral rim of cortical bone. In an immature skeleton, the epiphyses are separated from the diaphysis by the epiphyseal cartilage plates. The broad part of the long bone between the epiphyseal plate and the tubular diaphysis is termed the metaphysis. The epiphys eal cartilage and the metaphyseal portion form the growth apparatus.
The cortex of the bone consists of compact osseous tissue and the medullary cavity contains cancellous bone. Cancellous bone is made up of plates and bars that form an interconnect-ing network (fig. 1-2). These plates and bars are composed of varying numbers of contiguous thin layers (lamellae). The bony trabeculae are arranged along the lines of maximal pressure or tension.
The haversian system, or osteon, is the basic structural unit of cortical bone (fig. 1-3). It con-sists of a central haversian canal, which contains blood vessels, and lamellae of bone arranged
concentrically around the central canal. The haversian canals form an anastomosing system of canals arranged along the long axis of the bone; thus, in cross section, bones appear as round openings surrounded by rings of bone. The lamellae have a large number of lacunae, which contain osteocytes and connect with one another through a series of canaliculi. The haversian canals are connected to the external
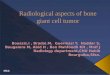
Figure 1-1
LONG BONE
The normal tibia and fibula of a 7-year-old boy illustrate the anatomy of a long bone.

Tumors of the Bones and Joints
2
surface of bone and the marrow cavity through the canals of Volkmann.
Bone is covered by a connective tissue layer, the periosteum, except where it is in contact with the articular cartilage. The attachment between bone and periosteum is tight where bundles of collagen (Sharpey fibers) from the periosteum penetrate cortical bone. Large blood vessels and nerves enter the bone at these points. The periosteum has two layers: an outer layer composed of dense connective tissue and an inner cambium layer composed of loosely arranged collagen and elastic fibers and a few spindle cells. The inner aspect of the cortex is separated from the marrow space by a thin layer of connective tissue called the endosteum.
DEVELOPMENT OF BONE
Bone develops either from preexisting car-tilage (endochondral ossification) or in mem-branous connective tissue (intramembranous ossification).
Intramembranous Ossification
The first signs of bone development are thin bars of a dense intercellular substance. The cells that remain in this meshwork are large, assume a polyhedral shape, and become osteoblasts. The cells are surrounded by a dense interstitial substance that undergoes calcification and be-comes bone.
Figure 1-2
CANCELLOUS BONE
Left: An interconnecting network is created by plates and bars of lamellar bone.Right: Higher-power view shows cancellous trabeculae surrounded by the marrow cavity containing fat and hematopoietic
elements.
Figure 1-3
CORTICAL BONE
Dense compact cortical bone with haversian canals is surrounded by concentric lamellar bone.

3
Introduction
Figure 1-4
ENDOCHONDRAL OSSIFICATION
Left: Low-power appearance of an epiphyseal plate, with bone formation seen in the lower portion of the panel.Right: Columns of cartilage cells in the zone of provisional calcification just before osteoid production.
Endochondral Ossification
Endochondral ossification is the mechanism by which long tubular bones grow in length, and is also is the process in fracture callus. The chondrocytes of the epiphyseal plate are ar-ranged in columns, and near the metaphyseal end, they undergo hypertrophy and vacuoliza-tion of the cytoplasm and eventually become calcified (fig. 1-4). Loops of blood vessels and connective tissue invade the hypertrophic cartilage cells, which are then removed. The connective tissue cells are transformed into osteoblasts. Between the cartilage cells and osteoblasts, connective tissue becomes calci-fied, giving rise to columns of bone. With the cessation of longitudinal growth of bone, the epiphyseal plate disappears.
CLASSIFICATION OF BONE TUMORS
The classification of bone tumors is based on either the cytologic features of the tumor cells or the matrix produced by them (11,15). The classification system that follows is a slight modification of these two schemes. Malignant tumors rarely arise from benign ones, although it is convenient to divide tumors into benign and malignant counterparts (Table 1-1). Neo-plasm simulators are discussed in chapter 14.
INCIDENCE OF BONE TUMORS
Primary tumors of bone are extremely rare, and no reliable statistics are available for the whole group. In the SEER (Surveillance, Epi-demiology, and End Results) program, during 1973 to 1987, only 0.2 percent of all cancers

Tumors of the Bones and Joints
4
were bone sarcomas (7). It has been estimated that 93,000 new cases of lung cancer and 88,000 cases of breast cancer occur annually in the United States, compared with only 1,500 cases of sarcoma of bone. Myeloma is the most com-mon primary bone tumor, although one may ar-gue that myelomas are tumors of bone marrow; most of them are diagnosed by biopsy of the bone marrow. In the SEER program, 35 percent of all sarcomas were osteosarcoma (however, myelomas and lymphomas were not included in that study). Chondrosarcoma and Ewing’s sarcoma are the next most common types. There is a bimodal distribution, with osteosarcoma and Ewing’s sarcoma occurring in the first and second decades of life and chondrosarcoma and myeloma in the older age groups.
METHODS OF BIOPSY
Diagnostic material from a bone tumor may be obtained in one of three ways: open biopsy, needle biopsy, or fine-needle aspiration (FNA).
Open Biopsy
Open biopsy is still the most common method for diagnosing bone tumors. It has the great advantage of obtaining the maximal amount of tissue. It is important to plan the biopsy so that the tract could be removed at the time of definitive surgical procedure. It is preferable for the surgeon who would perform the surgical procedure to perform the biopsy. An ill-conceived biopsy may preclude a limb salvage procedure (12). The biopsy should be planned with consultation among the radiolo-gist, pathologist, and orthopedic surgeon.
Table 1-1
CLASSIFICATION OF BONE TUMORSa
Benign Malignant Histologic Total Class No. of No. of Type No. % Tumor Cases Tumor Cases
Hematopoietic 1,788 18.8 Myeloma 986 Lymphoma 802
Chondrogenic 2,914 30.6 Osteochondroma 946 Chondrosarcoma 1,023 Chondroma 469 Secondary chondrosarcoma 128 Chondroblastoma 138 Dedifferentiated chondrosarcoma 130 Chondromyxoid 48 Mesenchymal chondrosarcoma 32 fibroma
Osteogenic 2,480 26.0 Osteoid osteoma 369 Osteosarcoma 1,941 Osteoblastoma 97 Parosteal osteosarcoma 73
Unknown 1,281 13.4 Giant cell tumor 627 Ewing’s sarcoma 578 Malignancy in giant cell tumor 36 Adamantinoma 40
Histiocytic 99 1.0 Fibrous histiocytoma 9 Malignant fibrous histiocytoma 90
Fibrogenic 285 3.0 Desmoplastic fibroma 14 Fibrosarcoma 271
Notochordal 411 4.3 Chordoma 411
Vascular 244 2.6 Hemangioma 131 Hemangioendothelioma 98 Hemangiopericytoma 15
Lipogenic 10 0.1 Lipoma 8 Liposarcoma 2
Neurogenic 18 0.2 Neurilemmoma 18
Total 9,530 100.0 Total 2,860 Total 6,670
aThe number of cases in the Mayo Clinic files.

5
Introduction
It is important to examine the biopsy speci-men before the wound is closed. Frozen sections are convenient for confirming that diagnostic material has been obtained.
Role of Frozen Sections in Diagnosis of Bone Tumors. The common misconception is that bone tumors are too hard (literally and figu-ratively) for frozen section diagnosis. However, if a few simple rules are followed, frozen sections can be made successfully. As with any diagnostic method (such as paraffin-embedded tissue and FNA), it is important to have good communica-tion between the pathologist and the clinicians involved in caring for the patient. It is convenient to have the frozen section laboratory close to the surgical suites. Most bone tumors have soft mate-rial that can be used for frozen sections. The biopsy sample should be examined before the material is immersed in formalin or decalcification solution. The soft material should be separated from the bony fragments before the sample is processed. It is important to do this whether the material is used for frozen section or paraffin embedding procedures. Almost without exception, bone tu-mors can be processed without decalcification, and microscopic sections should be available within 24 hours.
Frozen sections can be made with either a cryostat or freezing microtome. Hematoxylin and eosin (H&E) or toluidine blue is used to stain the specimen (fig. 1-5). The nuclear details are excellent with the toluidine blue stain.
Frozen sections have several advantages over other diagnostic techniques. Perhaps the most important reason for making frozen sections is to check the adequacy of the specimen. If diagnostic tissue is received, part of it can be reserved for special studies such as microbio-logic cultures, cytogenetics, and flow cytometry. Margins can be checked on frozen sections. It is not possible to check all the margins on large tu-mors, but those that are closest, such as the bone marrow margin, can be examined. In benign and low-grade malignant lesions, a definitive diagnosis can be made and immediate treatment instituted. With experience, a diagnosis can be based on frozen section specimens just as well as it can with paraffin sections.
Needle Biopsy
Percutaneous needle biopsy is an effective and safe technique (17) for obtaining diagnos-tic material from bone lesions, especially from metastatic carcinoma (2,13). Various needles have been used. The advantage over FNA is that a larger amount of tissue is obtained with a needle biopsy. Imprint cytologic preparations can also be made from the tissue.
Fine-Needle Aspiration Biopsy
The technique of FNA biopsy was pioneered eight decades ago by Ewing, Coley, Martin, and Ellis at Memorial Sloan-Kettering Cancer Center in New York City. Despite the accumulation of
Figure 1-5
FROZEN SECTION
A hematoxylin and eosin–stained frozen section of syno-vial chondromatosis shows the characteristic clustering pattern of the chondrocytes.

Tumors of the Bones and Joints
6
extensive experience with FNA worldwide, par-ticularly in Scandinavia, many centers have not adopted it as a standard part of the diagnostic work-up of bone lesions.
The interpretation of FNA specimens of bone has problems similar to those of a histologic diagnosis based on open biopsy. However, the scarcity of morphologic material, the loss of certain architectural features, and the introduc-tion of artifacts unique to FNA probably account for some of the reluctance of many centers to incorporate it into their routine diagnostic rep-ertoire. Moreover, the accurate interpretation of FNA specimens of bone lesions requires a high degree of expertise within the specialty area, but this expertise is sparse because of the relative rarity of bone tumors, their wide morphologic spectrum, and diagnostic pitfalls. FNA findings must be interpreted in the context of the clini-cal and radiographic findings. Hence, FNA of bone lesions should be performed at medical centers that have experience and expertise in the diagnosis and treatment of musculoskeletal tumors. If FNA is performed in this setting, it is useful in most cases for determining whether a bone lesion is primary or metastatic, benign or malignant, and a low-grade or high-grade neo-plasm. In many cases, a specific diagnosis can be suggested. The technique is particularly useful for rapidly distinguishing among primary bone tumor, metastasis, myeloma, and lymphoma. The technical aspects of performing FNA on bone lesions has been described in detail else-where (4,10,16,19,20).
Palpable lesions that have cortical thinning or breakthrough are easily aspirated, in most instances, with a 0.7- to 0.9-mm needle (20–22 gauge). Nonpalpable lesions with an intact cortex require a cutting needle or Tru-cut instrument as a leader for the needle; these biopsies usually are performed under the guidance of computer-ized tomography (CT) or other imaging tech-niques. Several aspirations are ideal to ensure that representative material has been obtained. May-Grünwald-Giemsa and H&E stains are pref-erable to the Papanicolaou stain for bone lesions because they enhance the matrix component of the lesion, which is critical in evaluating the lesion. Aspirates may be useful for performing routine histochemical stains, immunohisto-chemistry, DNA ploidy studies, fluorescence in
situ hybridization studies, and the polymerase chain reaction as well as for tissue culture and karyotyping (provided the number of cells is adequate for the latter two studies). Also, aspi-rated material can be used for traditional light and electron microscopic studies.
HANDLING OF SPECIMENS
A special laboratory is not needed to handle gross specimens of bone lesions. At Mayo Clinic, the gross specimen is examined in the frozen section laboratory, which is adjacent to the surgical suites. The gross specimen may take the following forms.
Incisional Biopsy. It is important for the surgeon to take the biopsy specimen from the soft regions of the lesion. In instances of osteo-sarcoma, this usually involves the soft tissue extension. It rarely is necessary to take a biopsy specimen from the intraosseous component, which is usually more heavily mineralized.
Excisional Biopsy. In the case of bone tu-mors, excisional biopsy specimens usually are removed by curettage. If the specimen contains fragments of bone, the fragments should be separated from the tumor before the specimen is sectioned. No hard and fast rules exist for how many sections should be taken from any tumor. Areas that grossly appear to be different should be sampled.
Resection. Most patients who have high-grade sarcomas have preoperative chemotherapy, and the bone containing the tumor is resected. The specimen consists of the segment of bone with the surrounding soft tissue. An ellipse of skin con-taining the biopsy tract is also usually removed.
There are two ways to handle these speci-mens. First, the dissection can be performed immediately. All the soft tissue is dissected away, leaving the tumor with the involved bone. It is best to slice the bone open along the longitudinal axis, through the middle of the marrow cavity. The bone can be opened with either a band saw or butcher’s meat saw (fig. 1-6). If the latter is used, the specimen has to be held in a vise. The cut sur-face should be washed with a brush (e.g., surgical scrub brush) under running water. This removes the bone dust from the specimen, thus reducing artifact. The surgeon usually sends a separate sample of bone marrow from the bony margin or margins. These can be checked by frozen section

7
Introduction
evaluation. It is not possible to use frozen sec-tions to check all the radial margins of a large tumor. However, if the surgeon is concerned about a specific margin, such as the neurovas-cular bundle, it can be checked separately. This technique has several advantages: the margins can be checked grossly immediately; if neces-sary, tissue can be saved for special studies, such as cytogenetics; and gross photographs appear more natural when the tissue is not frozen.
The second method for handling resection specimens is to freeze the entire specimen until it becomes hard enough that it can be sliced open in its entirety. This has the advantage of keeping the gross contours of the tumor intact, including the relationships with other struc-tures. However, it has the disadvantage of delay.
Decalcification
Several techniques are available for decalcify-ing bone specimens. Whatever method is used, it is important to saw the bone into thin slices to hasten decalcification. Thick cortical bone rarely needs to be decalcified for diagnostic purposes. De-calcifying it will only delay in making the sections. The slice should be washed to remove bone dust.
A practical method is to use a solution of 20 percent formic acid and 10 percent formalin,
which is made by mixing 400 ml of formic acid in 1,600 ml of 10 percent formalin. The specimen should be checked frequently with a pair of forceps to avoid overdecalcification. Specimens without cortical bone are ready for sectioning within 24 hours. Other specialized decalcification solutions, such as ethylenedia-minetetraacetic acid (EDTA), are available but not necessary for routine work. The addition of caustic acids has no advantage.
Assessment of Chemotherapy Effect
Most patients with high-grade sarcomas, especially osteosarcoma, are treated routinely with neoadjuvant chemotherapy before surgi-cal removal of the neoplasm. Several studies (1,14) have shown a correlation between the effect of chemotherapy and survival. Hence, it is necessary to evaluate the extent of necrosis after chemotherapy. The gross specimen is dis-sected as described above, and the bone is cut along its longitudinal axis. One thin slice of the entire bone with tumor is obtained. This slice is put in a clear plastic bag and “photographed” on a photocopier. The photocopy image can be used as a template. The entire slice is decalcified. Decalcification may take several days because of cortical bone. When the bone is soft enough, it is cut into several smaller blocks, which should be numbered sequentially. These numbers are marked on the photocopy so that the location of each block can be identified. The number of blocks depends on the size of the tumor.
The effect of chemotherapy can take several forms. 1) The tumor is replaced with new bone formation. The marrow spaces, where the tumor was present, are filled with new bone. Malignant cells may or may not be present in the sclerotic bone; this is the feature that determines whether the tumor is viable. One problem is that os-teoblastic osteosarcomas can have the same pattern, and it is impossible to decide whether the sclerotic bone is a result of chemotherapy. 2) The ghost outlines of the original neoplasm with infarct-like necrosis are present. 3) The part of the bone marrow containing the tumor is replaced with a proliferation of loosely arranged vessels and spindle cells. Frequently, there are collections of hemosiderin-containing histio-cytes. It usually is possible to discern where the tumor was and where normal marrow is present.
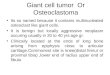
Figure 1-6
BAND SAW
A band saw is used to cut longitudinally through a resected femur.

Tumors of the Bones and Joints
8
The areas of viable tumor are identified with the microscope. Areas with viable tumor can be mapped on the photocopy image of the gross specimen and the amount of persistent tumor calculated. It is not always possible to be certain about the viability of some areas of the tumor. In spite of this problem, many studies have shown (1,14) that evaluation of response to chemotherapy is prognostically important. As recent studies have shown (1,14), it is only necessary to establish whether 95 percent or more of the tumor is viable. It has also been suggested that any residual viable tumor is important prognostically and, hence, it is only necessary to decide whether 99 percent or more of the tumor is necrotic.
GRADING OF BONE TUMORS
Grading is an attempt to predict the biologic behavior of a tumor on the basis of its histologic appearance. Many techniques of molecular biology are used to predict prognosis when a malignancy is diagnosed. Microscopic grading, however, is the basic attempt to describe the malignancy of a tumor. Interest has resurged in the histologic grading of tumors, and grading systems have proliferated which are unique to organs and even to specific tumors of an organ.
The grading system used at Mayo Clinic is based on the technique first described by Brod-ers (5) while studying squamous cell carcinoma of the lip. He described four grades, depending on the “differentiation” of the tumor cells. Tu-mor cells were considered “differentiated” or “undifferentiated” on the basis of how similar or dissimilar their appearance was to that of normal precursor cells. This concept was similar to “anaplasia” described by Von Hansemann (18). The four grades were described as follows: grade 1, 0 to 25 percent of the cells are undif-ferentiated; grade 2, 25 to 50 percent of the cells are undifferentiated; grade 3, 50 to 75 percent of the cells are undifferentiated; and grade 4, 75 to 100 percent of the cells are undifferentiated. Broders showed a correlation between histologic grade of the tumor and survival of the patient.
Originally, Broders described this grading system for squamous cell carcinoma, but he later applied it to other epithelial malignancies. There is no logical reason why the principles cannot be applied to grading sarcomas.
Sarcomas of bone are graded predominantly on the basis of two features: cytologic atypia (anaplasia) and cellularity. Mitotic figures usu-ally are more common in high-grade tumors, as is necrosis. Most sarcomas are diagnosed with a small biopsy sample; hence, necrosis and mi-totic figures are hard to evaluate, but cytologic atypia is not. Grading requires that tumors show histologic variability. For example, one of the distinguishing features of Ewing’s sarcoma is the uniformity of the cells in a tumor and between different tumors. Thus, Ewing’s sarcoma cannot be graded. Studies have shown that histologic grading is not useful for chordoma, adamanti-noma, or myeloma. It is helpful to grade chon-drosarcomas, malignant vascular tumors, and spindle cell sarcomas of all kinds.
Grading is subjective, but this deficiency is not unique to the system described by Brod-ers. The same caveat applies to reproducibility. Nevertheless, the results of each grading system have been shown to correlate with prognosis.
STAGING OF BONE TUMORS
Although a radiologic staging system for be-nign bone tumors has been proposed (and may be helpful in planning surgical management) (6), this section considers only the staging of sarcomas. The system that is used almost uni-versally by musculoskeletal oncologists is that of Enneking et al. (8), which takes into account the histologic grade and anatomic extent of the neoplasm. Tumors are considered to occur in anatomic compartments. A sarcoma confined to the bone is intracompartmental; it is extracom-partmental if it extends into soft tissues.
Sarcomas are graded as high-grade (grades 3 and 4) and low-grade (grades 1 and 2) tumors. The histologic grade and the anatomic descrip-tion of the tumor are combined to define the stage: stage 1A—low-grade, intracompart mental; stage 1B—low-grade, extracompartmen tal; stage 2A—high-grade, intracompartmental; stage 2B—high-grade, extracompartmental; and stage 3—distant metastasis regardless of other factors.
This staging system also includes a descrip-tion of surgical margins: 1) radical—the entire compartment involved by the tumor is re-moved; 2) wide—the tumor is removed with sur-rounding normal tissue, and the “reactive zone” (composed of the fibrovascular pseudocapsule)

9
Introduction
is removed intact; 3) marginal—the tumor is removed entirely, but the incision goes through the reactive zone; and 4) intra lesional—the
Table 1-2
TNM CLINICAL CLASSIFICATION
T Primary Tumor TX Primary tumor cannot be assessed T0 No evidence of primary tumor T1 Tumor 5 cm or less in greatest dimension T1a Superficial tumor T1b Deep tumor T2 Tumor more than 5 cm in greatest dimension T2a Superficial tumor T2b Deep tumor
N Regional Lymph Nodes NX Regional lymph nodes cannot be assessed N0 No regional lymph node metastasis N1 Regional lymph node metastasis
M Distant Metastasis MX Distant metastasis cannot be assessed M0 No distant metastasis M1 Distant metastasis
G Histopathologic Grade GX Grade cannot be assessed G1 Well differentiated G2 Moderately differentiated G3 Poorly differentiated G4 Undifferentiated
Stage Grouping
Stage IA Low-grade, small, superficial, deep G1, T1a-b N0 M0
Stage IB Low-grade, large, superficial G1-2, T2a N0 M0
Stage IIA Low-grade, large, deep G1-2, T2b N0 M0
Stage IIB High-grade, small, superficial, deep G3-4, T1a-b N0 M0
Stage IIC High-grade, large, superficial G3-4, T2a N0 M0
Stage III High-grade, large, deep G3-4, T2b N0 M0
Stage IV Any metastasis Any G, any T N1 M0
Any G, any T N0 M1
tumor is not removed intact, and margins are involved.
The TNM classification is given in Table 1-2.
1. Ayala AG, Murray JA, Erling MA, Raymond AK. Osteoid-osteoma: intraoperative tetracycline-fluorescence demonstration of the nidus. J Bone Joint Surg Am 1986;68:747–51.
2. Ayala AG, Raymond AK, Ro JY, Carrasco CH, Fan-ning CV, Murray JA. Needle biopsy of primary bone lesions. M.D. Anderson experience. Pathol Annu 1989;24:219–51.
3. Bloom W, Fawcett DW. A textbook of histology, 8th ed. Philadelphia: WB Saunders; 1962:153–86.
4. Bommer KK, Ramzy I, Mody D. Fine-needle aspi-ration biopsy in the diagnosis and management
of bone lesions: a study of 450 cases. Cancer 1997;81:148–56.
5. Broders AC. Squamous cell epithelioma of the lip. A study of 537 cases. JAMA 1920;74:656–64.
6. Campanacci M. Bone and soft tissue tumors: clinical features, imaging, pathology and treatment, 2nd ed. Padova, Italy: Piccin Nuova Libraria; 1999:1131.
7. Dorfman HD, Czerniak B. Bone cancers. Cancer 1995;75(Suppl):203–10.
8. Enneking WF, Spanier SS, Goodman MA. A sys-tem for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980:106–20.
REFERENCES

Tumors of the Bones and Joints
10
9. Fechner RE, Mills SE. Tumors of the bones and joints. Atlas of Tumor Pathology, 3rd Series, Fas-cicle 8. Washington, DC: Armed Forces Institute of Pathology; 1993:1–16.
10. Kreicbergs A, Bauer HC, Brosjo O, Lindholm J, Skoog L, Soderlund V. Cytological diagnosis of bone tumours. J Bone Joint Surg Br 1996;78:258–63.
11. Lichtenstein L. Classification of primary tumors of bone. Cancer 1951;4:335–41.
12. Mankin HJ, Lange TA, Spanier SS. The hazards of biopsy in patients with malignant primary bone and soft-tissue tumors. J Bone Joint Surg Am 1982;64:1121–7.
13. Murphy WA, Destouet JM, Gilula LA. Percutane-ous skeletal biopsy 1981: a procedure for radi-ologists—results, review, and recommendations. Radiology 1981;139:545–9.
14. Onikul E, Fletcher BD, Parham DM, Chen G. Ac-curacy of MR imaging for estimating intraosseous extent of osteosarcoma. AJR Am J Roentgenol 1996;167:1211–5.
15. Schajowicz F, Sissons HA, Sobin LH. The World Health Organization’s histologic classification of bone tumors. A commentary on the second edition. Cancer 1995;75:1208–14.
16. Snyder RE, Coley BL. Further studies on the diagnosis of bone tumors by aspiration biopsy. Surg Gynecol Obstet 1945;80:517–22.
17. Stoker DJ, Cobb JP, Pringle JA. Needle biopsy of musculoskeletal lesions. A review of 208 proce-dures. J Bone Joint Surg Br 1991;73:498–500.
18. Von Hansemann HD. Cited by Broders AC. The microscopic grading of cancer. In: Pack GT, Livingston EM, eds. Treatment of cancer and allied diseases: by one hundred and forty-seven international authors, vol. 1. New York: Paul B. Hoeber; 1940:19–41.
19. Willems JS. Aspiration biopsy cytology of soft tis-sue tumors. In: Linsk JA, Franzén S, eds. Clinical aspiration cytology. Philadelphia: JP Lippincott; 1983:219–347.
20. Willen H. Fine needle aspiration in the diagno-sis of bone tumors. Acta Orthop Scand Suppl 1997;273:47–53.







![Recurrent primary mediastinal giant cell tumor of soft tissue ......Discussion Giant cell tumor of soft tissue (GCT-ST) is a rare tumor. GCT-ST, which resembles osseous GCT [2], broadly](https://img.pdfslide.us/doc/110x75/608dfb4a7de20e33185e8616/recurrent-primary-mediastinal-giant-cell-tumor-of-soft-tissue-discussion.jpg)