Embed Size (px)
Citation preview

0001 1 HEREDITARY DYSAUTONOMIAS 2 CURRENT KNOWLEDGE AND COLLABORATIONS FOR THE FUTURE 3 4 5 NATIONAL INSTITUTE OF NEUROLOGICAL DISORDERS AND STROKE 6 OFFICE OF RARE DISEASES 7 NATIONAL INSTITUTES OF HEALTH 8 9 10 11 12 13 8:40 a.m. 14 Thursday, October 3, 2002 15 16 17 18 19 20 21 Plaza I 22 Doubletree Hotel 23 1750 Rockville Pike 24 Rockville, Maryland 25 0002 1 C O N T E N T S 2 AGENDA ITEM PAGE 3 ANNOUNCEMENTS 4 KATRINA GWINN-HARDY, M.D., NINDS, NIH, 5 Bethesda, Maryland 7 6 WELCOME 7 AUDREY PENN, M.D., Acting Director, NINDS, NIH, 8 Bethesda, Maryland 7 9 STEPHEN GROFT, Pharm.D., Director, Office 10 of Rare Diseases, NIH, Bethesda, Maryland 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 0003 1 C O N T E N T S (Continued) 2 AGENDA ITEM PAGE 3 SESSION 1: 4 FAMILIAL DYSAUTONOMIA-GENETICS AND OTHER FACTORS

5 - - - 6 INTRODUCTION-FAMILIAL DYSAUTONOMIA: HISTORICAL, 7 NEUROPATHOLOGICAL, AND CLINICAL OVERVIEW 8 FELICIA B. AXELROD, M.D., New York University 9 School of Medicine, New York, New York 14 10 GENETICS OF FAMILIAL DYSAUTONOMIA - TISSUE SPECIFIC 11 EXPRESSION OF THE IKBKAP GENE MUTATIONS 12 SUSAN SLAUGENHAUPT, Ph.D., Harvard Medical 13 School, Cambridge, Massachusetts 27 14 AUTONOMIC AND SENSORY ASSESSMENT AND EVALUATION OF 15 FAMILIAL DYSAUTONOMIA WITH STANDARDIZED TESTS 16 MAX J. HILZ, M.D., Ph.D., New York University 17 School of Medicine and University Erlangen- 18 Nuremberg, Germany 47 19 FUTURE DIRECTIONS FOR FAMILIAL DYSAUTONOMIA 20 GAIL SONENSHEIN, Ph.D., Chair, Dysautonomia 21 Foundation Scientific Advisory Board; Boston 22 University School of Medicine, Boston, 23 Massachusetts 62 24 25 0004 1 C O N T E N T S (Continued) 2 AGENDA ITEM PAGE 3 SESSION 1: 4 FAMILIAL DYSAUTONOMIA-GENETICS AND OTHER FACTORS 5 - - - 6 WHAT IS IKAP AND SPECULATIONS ON ITS ROLE IN THE 7 DEVELOPMENT, MAINTENANCE AND SURVIVAL OF AUTONOMIC 8 AND SENSORY NEURONS 9 JESPER Q. SVEJSTRUP, Ph.D., Clare Hall Laboratories, 10 United Kingdom 74 11 SECONDARY NEUROTRANSMITTER ABERRATIONS AS DEMONSTRATED 12 BY IMMUNOREACTIVE STAINS IN DERMAL NEURONS 13 WILLIAM R. KENNEDY, M.D., University of 14 Minnesota, Minneapolis, Minnesota 91 15 CONSTRUCTION OF A MOUSE MODEL TO STUDY MECHANISMS OF 16 PATHOGENESIS IN FAMILIAL DYSAUTONOMIA 17 YANG XU, Ph.D., Division of Biology, University 18 of California, San Diego, California 105 19 OPEN DISCUSSION AND Q&A 20 BERISH RUBIN, Ph.D., Moderator, Fordham 21 University, Bronx, New York 109 22 23 24 25 0005 1 C O N T E N T S (Continued) 2 AGENDA ITEM PAGE 3 SESSION 2: 4 INHERITED DYSAUTONOMIAS: FAMILIAL DYSAUTONOMIA AND BEYOND 5 - - - 6 DYSAUTONOMIA IN FAMILIAL PARKINSON'S DISEASE 7 DAVID S. GOLDSTEIN, M.D., Ph.D., NINDS, NIH, 8 Bethesda, Maryland 138 9 SETTING PRIORITIES FOR BASIC, DISEASE-ORIENTED, AND

10 PATIENT-ORIENTED RESEARCH ABOUT INHERITED DYSAUTONOMIAS: 11 A PATIENT ADVOCACY PERSPECTIVE 12 SONIA PELTZER, M.D., President, Familial 13 Dysautonomia Hope, Newton, North Carolina 151 14 FAMILIAL AMYLOIDOTIC POLYNEUROPATHY 15 YUKIO ANDO, M.D., Ph.D., Kumamoto University 16 School of Medicine, Kumamoto, Japan 162 17 NET DEFICIENCY: PRESIDENT OF A MOLECULAR RESEARCHER 18 MAUREEN HAHN, Ph.D., Center for Molecular 19 Neuroscience, Vanderbilt University, 20 Nashville, Tennessee 171 21 ADRENORECEPTOR POLYMORPHISMS AFFECTING AUTONOMIC 22 REGULATION 23 STEPHEN LIGGETT, M.D., University of Cincinnati, 24 Cincinnati, Ohio 187 25 0006 1 C O N T E N T S (Continued) 2 AGENDA ITEM PAGE 3 SESSION 2: 4 INHERITED DYSAUTONOMIAS: FAMILIAL DYSAUTONOMIA AND BEYOND 5 - - - 6 HYPERTENSION IN AUTONOMIC DISORDERS: GENETIC FACTORS 7 AND PHENOTYPING 8 ITALO BIAGGIONI, M.D., Vanderbilt University, 9 Nashville, Tennessee 202 10 OPEN DISCUSSION AND Q&A 11 DAVID GOLDSTEIN, M.D., Ph.D., Moderator, 12 NINDS, NIH, Bethesda, Maryland 217 13 14 15 16 17 18 19 20 21 22 23 24 25 0007 1 P R O C E E D I N G S 2 (8:40 a.m.) 3 DR. GWINN-HARDY: Hello and welcome, ladies and 4 gentlemen to the Hereditary Dysautonomias Workshop. If I 5 can't say it, hopefully at least I'll be able to learn 6 something today from all of you. And welcome to all the 7 scientists and all the other interested people who are 8 attending today. 9 This workshop is sponsored by the National 10 Institute of Neurological Disorders and Stroke and the 11 Office of Rare Diseases. We also have with us Dr. 12 Guttmacher from the Genome Institute. 13 I'd first like to introduce Dr. Audrey Penn, our 14 acting Director at the NINDS, who is first and foremost a

15 neurologist and always a scientist. Thank you, Audrey. 16 DR. PENN: Good morning. Thank you, Katrina. I 17 thank all of you for coming to this. I should give really 18 very specific and special thanks to the organizers of 19 this. We did talk about the organization and the program 20 a great deal, and I think it is going to be a magnificent 21 meeting. I will say -- and Steve has the same problem -- 22 I won't be able to stay for all of it, but I know everyone 23 here will benefit from it and be able to have a lot of 24 interchange. 25 So I was introduced to this disorder when I was 0008 1 a medical student because Dr. Riley was on the staff of 2 pediatrics at Babies' Hospital. And it was a prize 3 disorder. Even though it's miserable, it was a prize 4 disorder for teaching medical students, and we heard 5 rather a lot about it. And then I have to say I didn't 6 hear a lot about it, and it is very rare, which is why 7 Steve is here. 8 But, on the other hand, for us at NINDS right 9 now, it's an excellent example of our over 250 small 10 genetic, mendelian genetic disorders of the nervous 11 system, both peripheral and central, and Lord knows, in 12 muscle too. So it's very important as an example of where 13 we are, where we have to go. 14 We are very concerned with these disorders. 15 Right now we plan all kinds of programs and initiatives 16 for various stages along the line; that is, find the gene 17 locus, then the gene, the coded protein, and then get the 18 models going, and then see where we can help develop 19 therapies. So we have a brand new or relatively brand 20 new, big program in the institute of translational 21 research programs, and you will see in the NIH guide the 22 set of specific applications for cooperative agreements to 23 achieve all of this. Clearly different disorders are in 24 different stages in this process, but I know now that you 25 have not only the longest, but you have a gene. Pretty 0009 1 soon you'll have a protein. So we might as well see what 2 the models look like. So we are investing in this. 3 And what I am trying to say is that your issue 4 is an issue for, again, many other disorders that we have 5 to fix. And there are all kinds of things about gene 6 therapy that you're well aware of that are going to make 7 this difficult and a challenge. We do work with the FDA 8 on these issues. We will work with the RAC on these 9 issues, but we have to put those genes back and we have to 10 figure out how to do it safely. And we are well aware of 11 that too. We have had setbacks, but we are very 12 determined to get this sort of thing done. 13 I am not entirely sure whether stem cells are 14 pertinent here or not, but it's another one that we spend 15 a lot of time thinking about, particularly because, for 16 all of us, we're talking about the brain, the central 17 nervous system and how to get things back safely. 18 So I'm really glad you all came together to look 19 at this disorder, and I think you know a lot. And I think

20 you're all together, which is just great. We have some 21 disorders where our lay community is not exactly all on 22 the same page, but I think this one is. So I'm trusting 23 that from this will come not only a rechallenge to us, but 24 real progress in this disorder. You know, whatever it is. 25 60 years since Dr. Riley. Let's get on with it. 0010 1 Thank you. Have a good day. 2 (Applause.) 3 DR. GWINN-HARDY: Thank you, Dr. Penn. 4 Now allow me to introduce Dr. Groft, the 5 Director of the Office of Rare Diseases. Dr. Groft. 6 DR. GROFT: Thank you very much, Katrina. And I 7 would like to thank, first, the organizers, Katrina, but 8 also the various chairs of the sessions: Dr. Axelrod, Dr. 9 Goldstein, and Dr. Robertson. It is quite an effort to 10 pull one of these meetings together, and a lot of time and 11 thought goes into the preparation of the speakers and the 12 agenda. So thank you very much for your contributions. 13 These are not easy conferences to pull off. It is a lot 14 of work. 15 I'd also like to thank all of the attendees who 16 have agreed to come in and share their expertise and 17 experience with each other. 18 The Office of Rare Diseases is not a large 19 office. In fact, we're very small. Some of your grants 20 probably exceeded our annual budget of $2 million until 21 last year when, all of a sudden, we got this magnificent 22 jump up to $10 million. What a fortune for us. 23 We've implemented a number of programs. One is 24 our intramural research program that we started, and I'd 25 just like to introduce Dr. Bill Gahl, who's in the back of 0011 1 the room, who is also the Clinical Director for the Human 2 Genome Research Institute. He's our intramural research 3 program director. 4 We will be implementing an extramural program 5 within the coming years to fund centers of emphasis. 6 There's some legislation moving forth in Congress to 7 provide some additional funds to the office, and one of 8 the major areas will be funding these centers of emphasis 9 or excellence throughout the country and groups of rare 10 diseases. So we're looking forward to that. Next year we 11 hope to support maybe seven, and if our budget were to 12 increase, we look forward to funding about 15 of these 13 within about two years. So if everything holds, as we're 14 planning, it should be an exciting time for us. 15 One of the few things, with such a limited 16 budget, that we've been able to do over the years is 17 support workshops such as this. We contribute a small 18 amount of money. It doesn't nearly cover the cost, 19 usually in the range of $20,000 to $25,000, just enough to 20 bring in several speakers and provide some of the 21 facilities and what have you. 22 But what comes out of these workshops really 23 depends on what you contribute and what you bring into the 24 meeting, how much you want to work together, how much you
25 want to share. We encourage the organizers of the meeting 0012 1 to get as many different experts, as many different 2 specialties to come here and talk about their research and 3 to try to tie together the various aspects. With so many 4 of the rare diseases, there are so many organs or systems 5 that are involved, that we need different approaches, 6 different ideas, and I think we can learn from each other. 7 And that's what we try to do in the workshops, is bring a 8 lot of different people together to talk about what is 9 needed. This, in essence, becomes the research agenda for 10 the institute. 11 I know the neurology institute has made an 12 unbelievable commitment over the years to these rare 13 diseases. In fact, at one point we called it the National 14 Institute on Rare Diseases, and we set up our office. We 15 said we're going to take the rare diseases. They do so 16 much, and they probably are the biggest user of our 17 workshops program. 18 And what comes out of this then hopefully are 19 grant applications from you, the research community, into 20 the institute that they can consider. I think that's one 21 of the goals that we'd like to see today is an increase of 22 grants coming from you, an increase of ideas and direction 23 to the institute and to the office. We'll see where we 24 can go in the future, as far as all of the funding. 25 So I don't want to delay the onset of the 0013 1 meeting. I'd like to thank all of you for coming. 2 Traveling is not an easy task these days for everyone. So 3 it really is appreciated that you're able to come in and 4 spend some time with us here and give us the benefit of 5 all your experience. 6 So thank you, and in particular, thanks to 7 Katrina. She did a tremendous job pulling this whole 8 thing together in some difficult circumstances. 9 (Applause.) 10 DR. GWINN-HARDY: Thanks, Dr. Groft. Although 11 I'm not sure how I feel about having the National 12 Institute of Neurological Disorders and Stroke called the 13 National Institute of Rare Diseases, because that says 14 "NIRD" which doesn't sound very good. 15 (Laughter.) 16 DR. GWINN-HARDY: But I guess we can handle it 17 if it means we do a lot of good science. 18 I want to also introduce Math Cuajungco. Is 19 that the right way to say your name? Dr. Cuajungco is 20 standing. He's the person who is actually writing the 21 meeting summary for us. So I'd like all the speakers and 22 moderators of the discussions to share their slides, as 23 well as their notes, with him so that he can put together 24 the most effective summary of the meeting for us. 25 I'd also like to ask each of the moderators to 0014 1 make sure they get one or two points from each of the 2 lectures so that during the discussion and especially 3 during the final discussion, these points can be made and

4 shared with others, so we have a nice summary at the end 5 of the meeting of our goals and directions for the future 6 as well. 7 Without further ado, I'd like to introduce Dr. 8 Felicia Axelrod, our chair of the first session. Dr. 9 Axelrod, thank you very much. 10 (Applause.) 11 DR. AXELROD: I also would like just start off 12 thanking a few people. 13 First of all, I'd like to thank Dr. Sonia 14 Peltzer and the FD Hope group for initiating contact with 15 the NIH and providing the impetus for this important 16 conference. 17 And I also would like to thank Dr. Katrina 18 Gwinn-Hardy for her superlative efforts in coordinating 19 and actually bringing this conference to fruition. 20 And finally, I'd like to express my appreciation 21 to the NIH and really for being sensitive to the 22 importance of this subject matter and hosting this 23 symposium. 24 Really, until recently, interest and financial 25 support for autonomic research really has been less than 0015 1 enthusiastic because it was perceived that the autonomic 2 disorders affected only a select few, and support 3 primarily came from small, but critical organizations like 4 the Dysautonomia Foundation. And for almost 50 years, the 5 Dysautonomia Foundation has really been the sole resource 6 for financial as well as motivational support to promote 7 clinical and basic research for FD. But now that we're 8 here at an NIH-sponsored forum, I think that this 9 indicates that interest in the autonomic nervous system is 10 growing. 11 The hereditary dysautonomias provide a unique 12 opportunity for scientists to obtain greater insight into 13 the complexities, as well as the pervasive nature of the 14 autonomic nervous system. And each of the hereditary 15 dysautonomias really affect autonomic dysfunction, but the 16 time of onset, as well as the extent of impairment, and 17 subsequent manifestations really depend upon the specific 18 genetic abnormality. 19 Over the next day-and-a-half, hopefully each of 20 us will widen our particular focus by learning about the 21 different entities, their genotypes, their phenotypes so 22 that we will be stimulated to try new approaches, 23 establish new collaborations. And the result of our 24 discussion should be really a cross-fertilization of 25 scientific knowledge so that the patients and their 0016 1 families who suffer with these disorders on a daily basis 2 will feel that our efforts have been positive and have the 3 desired long-term effects. 4 The first of these three sessions will, of 5 course, be devoted to familial dysautonomia, and I think 6 that this really is an appropriate place to start because 7 this is the first of the hereditary dysautonomias to be 8 well described and extensively studied. It affects a

9 genetically and pathologically homogeneous population and 10 therefore can be considered an excellent model to 11 understand the mechanisms involved in development and 12 survival of the autonomic nervous system. 13 I will start off by providing an overview on the 14 history, the pathology, as well as describing some of the 15 clinical features of the disorder and how we maintain 16 patient data so that we can evaluate clinical course and 17 treatment and how this will be eventually the way we could 18 possibly approach treatment therapy. 19 The other speakers this morning will provide 20 further information regarding current knowledge of the 21 disorder, as well as provide some thoughts on possible 22 future directions for FD research. 23 Well, it all began about 53 years ago when Drs. 24 Riley and Day reported five cases of central autonomic 25 dysfunction with defective lacrimation, and you can see 0017 1 that he really stressed "central" autonomic dysfunction at 2 this time. Since that time, we realized that there also 3 are sensory perturbations. He did not really describe in 4 that paper any problems with pain and temperature 5 perception, which these patients do have. 6 We also know that the autonomic problems extend 7 more than he described at that time. They involve 8 oropharyngeal incoordination, poor speech, esophageal 9 dysmotility, insensitivity to hypoxia and hypercapnia, as 10 well as blood pressure lability. 11 The other central problems really involve 12 peripheral as well as central manifestations of autonomic 13 dysfunction. There are eye problems, as well as general 14 hypotonia, and gait problems. 15 Interestingly, intellect is usually normal, but 16 there are particular characteristic features. Visual 17 skills tend to exceed verbal skills, and there are 18 problems with executive planning and organizational skills 19 which tend to be frontal lobe problems. 20 The clinical features are present from birth. 21 Multiple systems are affected secondarily, and the 22 expression varies widely. These are two different 23 individuals, both 16 years of age, and you can see this 24 young man really barely has any physical abnormalities 25 that might be discernible to a pediatrician, whereas this 0018 1 young man is very short in stature, has severe spinal 2 curvature. You can't see it on this slide, but he's 3 drooling and has mottling of the skin. 4 Now, until the last two years, diagnosis was 5 really based on clinical signs and there had to be 6 evidence of sensory as well as autonomic dysfunction, and 7 we used five diagnostic criteria. The first three were 8 all described by Riley in his original report: the lack 9 of overflow tears or absent lacrimation with emotional 10 crying, the fact that there was decreased deep tendon 11 reflexes, and as he noted, all five of his children were 12 Ashkenazi Jewish extraction from the Eastern European area 13 which the Ashkenazi Jews are from.

14 Then in the 1960s, Drs. Smith and Dancis 15 described the tongue findings, and that became the fourth 16 of the diagnostic criteria. In a normal individual, there 17 are highly vascularized papillae on the tip of the tongue. 18 This is lacking in the FD patient, giving the tip of the 19 tongue a smooth, glistening appearance. 20 The fifth sign that was also described in the 21 early 1960's by Drs. Dancis and Smith was the abnormal 22 axon flare with intradermal histamine. And in the FD 23 patient, the intradermal injection of histamine gives you 24 really a very circumscribed area of redness where in the 25 normal individual, there's a diffuse area of erythema, 0019 1 which is the axon flare. 2 Interestingly, this particular sign is present 3 in all of the hereditary sensory and autonomic 4 neuropathies, which is the other types V, IV, I, and II. 5 Dysautonomia is type III of these hereditary sensory and 6 autonomic neuropathies. 7 So in questionable cases, for instance, if we 8 were sent a patient who seemed to have most of these signs 9 and had an abnormal histamine test and if their parents 10 weren't Jewish, well, then we would suggest doing a sural 11 nerve biopsy, and based on pathological findings in the 12 sural nerve biopsy, we were able to differentiate the 13 disorder. However, as of 1993, with haplotype analysis 14 and now in 2001, DNA diagnosis is possible, and definitive 15 diagnoses can be given in this way. 16 So as of 2001, we had the FD gene identification 17 confirmed. IKBKAP is the gene. IKAP is the protein 18 product. We know that two mutations can cause FD, and we 19 have tissue-specific expression. 20 So what now? Well, we have carrier testing in 21 the general population, and this has had a tremendous 22 impact for the patients, their families, and for the 23 general population at large. 24 But there is a bigger job now, and that's to 25 start the search for gene function. What is the role of 0020 1 IKAP and its associated protein in the development and the 2 maintenance of the sensory and the autonomic nervous 3 system? And how can we correlate the previous information 4 with these new genetic findings? What about the 5 pathological reports that we had until this time and the 6 observed clinical symptoms? Of course, the final goal 7 will be to develop definitive therapies. 8 Well, in 1958 to 1978, really before we had 9 pathological findings reported, most of the efforts were 10 spent on looking at catecholamines, and it appeared that 11 the products of dopamine were elevated and the end product 12 of norepinephrine was decreased in the affected 13 individual, and when you gave these particular drugs, 14 there were abnormal physiologic responses. So based on 15 that without any pathological findings, they said patients 16 were acting like they had denervated hypersensitivity and 17 that there was probably a problem in norepinephrine 18 synthesis, release, or degradation. They assumed that

19 this was secondary to a decreased peripheral sympathetic 20 system. 21 And then in 1971, we had the first report of 22 pathological findings, and that was really by Dr. Aguayo 23 in Canada, and he showed that the unmyelinated and small 24 myelinated neuronal population was decreased in the 25 patient with FD, and this was in a sural nerve. 0021 1 Dr. John Pearson at NYU then looked at 2 sympathetic ganglia and he found the same thing, the 3 decreased numbers of neurons in cervical sympathetic 4 ganglia, and when he actually did counts, he saw that the 5 FD population has about a tenth of the normal neuronal 6 population in their sensory as well as their cervical 7 ganglia and minimal involvement of the parasympathetic 8 ganglia, at least the ones that he looked at. 9 Since that time, there has been more 10 investigation, and this has been confirmed, again the 11 sympathetic chain has been looked at, the dorsal root 12 ganglia, and we have also found the same findings of 13 decreased innervation in vascular nerve terminals which 14 probably accounts for the vasomotor instability in these 15 patients. But really, where no one has been able to look 16 or give us accurate information is the brain. 17 So the consistent pathological findings show 18 inadequate development of small myelinated and 19 unmyelinated neurons in the sensory system, the autonomic 20 nervous system, and one cranial nerve that has been looked 21 at is the sphenopalatine ganglia. We also know it's a 22 progressive disorder because there are residual nodules in 23 dorsal root ganglia. 24 So this seems to be a neurodevelopmental and a 25 progressive disorder. There is consistent peripheral 0022 1 neuropathology, but we've never been able to document 2 central neuropathology. 3 Yet, we know that there are autonomic tracks in 4 ganglia, as highlighted in red here on this cartoon, and 5 we wonder now whether the peripheral nervous system is 6 affected primarily or secondarily, and how can we account 7 for the wide variability of clinical expression? Is it 8 just differences in neuronal number, differences in 9 neurotransmitter? And which of the genes and peptides 10 might be secondarily affected? 11 In treatment challenges, there are really four 12 that I struggle with and Dr. Maayan struggles with on a 13 daily basis. The gastrointestinal system. The GI 14 dysfunction in FD is prominent and probably one of the 15 symptoms that plagues the families the most. The 16 oropharyngeal incoordination is seen at birth and the 17 children have difficulty feeding. There's esophageal 18 dysmotility, as well as gastric dysfunction, but it's the 19 vomiting or the protracted retching which significantly 20 impacts on the quality of the patient's life. 21 Crisis can occur in any FD patient with 22 sufficient stress. 40 percent will have a cyclical 23 pattern that usually starts in the morning after arousal,

24 and the pattern tends to be consistent for an individual. 25 Either it occurs daily, weekly, or even monthly. The 0023 1 stressors can be physiologic, they can be emotional, which 2 suggests again central problems, and again, this constant 3 theme that it occurs with arousal from sleep. 4 But what is a dysautonomic crisis? Well, it's a 5 constellation of symptoms. Yes, there are GI 6 manifestations. They don't want to swallow. They drool 7 during these crises. They develop an ileus. Nausea and 8 retching are prominent. The vomiting is only the tip of 9 the iceberg. The nausea is really what they can't stand 10 more than the vomiting. There are also cardiovascular 11 perturbations, as well as increased secretions. The whole 12 child is wet, and the personality changes. 13 When we looked at serum catecholamines during an 14 FD crisis, we were struck by the fact that -- these are 15 three determinations early in crisis -- the dopamine 16 levels were extremely high. With that information, we 17 went to Dr. Pearson and had him look again at the 18 sympathetic ganglia, and he stained for tyrosine 19 hydroxylase, the precursor of dopamine, and found that the 20 FD patient actually had increased stores of tyrosine 21 hydroxylase as compared to the control, suggesting that 22 with stress, they had the potential of pouring out 23 enormous amounts of dopamine. 24 And dopamine really has a lot of central effects 25 that we can think of as causing these problems that see, 0024 1 the vomiting, the anxiety, and the grimacing that occurs 2 during crisis. It also has peripheral effects on GI 3 motility. It decreases motility. It increases sodium 4 excretion, and dopamine also can be converted peripherally 5 by DBH to norepinephrine and give us hypertension, 6 tachycardia, sweating, and hyperglycemia. 7 And so there's debate: Is this a GI tract 8 problem or a brain problem? And we think that there's 9 more brain problems and therefore that this is acting like 10 an autonomic seizure and nausea is the aura. 11 We have also done SPECT studies that have shown 12 that during crisis there's hyperperfusion of areas of the 13 temporal lobe that disappear when the patient is out of 14 crisis. 15 So we treat for a possible autonomic seizure 16 with GABA-enhancing agents, central adrenergic agonists, 17 and even anticholinergic agonists. 18 The causes of respiratory problems are 19 aspiration, restrictive lung disease, and chemoreceptor 20 dysfunction. There really is not an increased incidence 21 of wheezing in this population other than based on family 22 history. 23 However, there is marked chemoreflex sensitivity 24 abnormalities. In particular, they have a diminished 25 response to low oxygen so that when they are challenged 0025 1 with a low oxygen situation and you bring the saturation 2 down from 100 to 70, the normal group increases their

3 minute ventilation, but the FD group does not and this is 4 significantly different. With CO2, it's not as remarkable 5 as with low oxygen. 6 And what is more dangerous to the patients is 7 that in this particular study, they were brought from 100 8 percent oxygen and they then were breathing 12 percent 9 oxygen, they did not increase their minute ventilation, as 10 the controls did, but also their blood pressure started to 11 drop and their heart rate did not compensate. So 12 physiological hypoxia, which would be pneumonia, high 13 altitudes, airplane travel, and underwater swimming, 14 basically can be life-threatening for the patients with 15 familial dysautonomia. 16 Blood pressure. They have postural hypotension 17 without compensatory tachycardia and episodic 18 hypertension. This seems to be a peripheral problem, but 19 this seems to be really induced by central abnormalities. 20 And the peripheral problems, of course, are accentuated by 21 the fact that they're denervated and they cannot mount a 22 normal norepinephrine rise as they go from supine to erect 23 and even then with exercise. 24 Of course, hypoxic hypotension is a problem, as 25 I just explained, and then they have supine hypertension. 0026 1 In a nice study that was done in collaboration with Dr. 2 Goldstein and Dr. Kopin, we noticed that when the patients 3 were supine, their norepinephrine levels actually were 4 elevated, and the only way I can explain that would be 5 possibly this is the effect of increased dopamine being 6 converted to norepinephrine. Interestingly, DOPA levels 7 are high and yet their DHP levels are low. 8 Neurologic. As they get older, their gait gets 9 worse and there is progression. We're not sure whether 10 this is due to the cardiovascular lability or intrinsic 11 problems with the nervous system. Probably it is 12 intrinsic problems with the nervous system. 13 Now, I think really what has made our treatment 14 so effective is that there have been two FD centers, one 15 in New York and one in Israel, and that these two centers 16 work very well together. We share our data and therefore 17 we're able to generate sufficient numbers and 18 collaborative studies to be able to see which treatments 19 are effective and which treatments are not. And I could 20 not do that without really the help of my colleague, Dr. 21 Channa Maayan. 22 There are now 580 FD patients registered in the 23 combined clinic registry. More than 60 percent are 24 surviving. 17 percent are less than 5 years of age, and 25 35 percent are greater than 20 years of age. 0027 1 The effect of just supportive treatment without 2 a gene therapy has been improved survival. In 1965, Brunt 3 and McKusick said that 50 percent of the children would 4 not survive past their 5th birthday. In a repeat analysis 5 of our data, in 1985 we said that 50 percent of the 6 patients were reaching 30 years of age, and in a paper 7 that's coming out this month in the Journal of Pediatrics,

8 Dr. Maayan and I have shown that 50 percent of our 9 patients are now reaching 40 years of age. 10 So not only have we improved survival, we feel 11 we have improved the quality of life, improved the 12 appearance of the patients. They seem to have less 13 disability and increase in function, but we hope we can 14 still do better and perhaps with meetings like this, we'll 15 have some insight in how to do that. 16 Thank you. 17 (Applause.) 18 DR. AXELROD: I think the next speaker is Dr. 19 Slaugenhaupt. 20 DR. SLAUGENHAUPT: I too would like to thank the 21 organizers of this meeting and also thank Felicia for 22 inviting me to speak on our work on FD today. 23 So I'm charged with introducing to you the FD 24 gene that we recently discovered, and today I'll describe 25 to you the mutations that cause FD and this unique tissue- 0028 1 specific splicing defect we see in this disease and also 2 tell you about some studies that are currently underway in 3 my laboratory. 4 FD is an autosomal recessive disease with a very 5 high carrier frequency of approximately 1 in 30 in the 6 Ashkenazi Jewish population. And in fact, recent large 7 scale population screening using the mutations has 8 confirmed this high frequency. This leads to an incidence 9 of approximately 1 in 3,600 live births. As I said, to 10 date this disease is limited to the Ashkenazi Jewish 11 population, and in 1993, we linked this gene to chromosome 12 9q31. 13 Now, in January of last year, two groups 14 identified and published the two mutations that cause FD, 15 ours and a group at Fordham University led by Dr. Berish 16 Rubin. The MGH group started working on FD in the late 17 1980s under the direction of Jim Gusella by doing family 18 studies to try to identify the genetic locus. This slide 19 basically summarizes the work that we did over the years 20 that culminated with the discovery of the FD gene. 21 As I mentioned, we linked the gene using family 22 studies in 1993 to chromosome 9, and ultimately we were 23 able to narrow the candidate region to approximately 178 24 kb by haplotype analysis. 99.5 percent of all FD 25 chromosomes are identical to one another, with only 4 0029 1 patients heterozygous for a second haplotype, and this is 2 a remarkably high frequency of a founder mutation in the 3 Ashkenazi Jewish population. 4 In order to identify candidate genes, we 5 employed exon trapping, cDNA selection and direct gene 6 prediction once we had some sequence, and in order to 7 identify mutations, we used a combination of SSCP and 8 direct sequencing. 9 Now, a few years ago, we had not identified the 10 FD mutation as yet, and we were approached by Mike 11 Brownstein who said, why don't you just sequence the whole 12 thing? So we began a collaboration with him and generated
13 the sequence of the entire candidate region. This was 14 before the human genome project sequence was available. 15 At that time, it was approximately 500 kb, and we 16 generated an FD cosmid library from a patient homozygous 17 for the major mutation and we sequenced that from that 18 region and directly compared the control and the FD 19 sequence. Direct comparison of these two sequences 20 identified 152 DNA differences in this region, only one of 21 which was unique to FD, and so we hypothesized that this 22 was, in fact, the pathogenic mutation. 23 Subsequent to this, we sequenced the four 24 heterozygous patients and identified a second DNA change 25 that was unique to the minor haplotype. 0030 1 I'm going to discuss these mutations in detail 2 in a moment, but first I'd like to just introduce you to 3 the FD gene. This slide shows a schematic of the FD 4 candidate region, 178 FD candidate region, which 5 ultimately contained five different genes, one of which is 6 IKBKAP. The name of this gene is IKBKAP, but I'm probably 7 going to say IKAP a lot during this talk because it's 8 easier. 9 This gene contains 37 exons with the start codon 10 on exon 2. It spans approximately 70 kb of the candidate 11 region. There are two different messages, 4.8 and 5.9 kb, 12 and this is due to differential polyadenylation of the 13 message. It encodes a 1,332 amino acid protein called 14 IKAP, and the message is ubiquitously expressed with the 15 4.8 kb band being slightly more abundant. 16 I'm only going to say a few words about the 17 protein IKAP. Jesper Svejstrup is here and his lab has 18 done a lot of work on this protein, and he's speaking 19 later this morning and will hopefully enlighten us. 20 IKAP was originally isolated as a scaffold 21 protein of the I-kappa B kinase complex in 1998. 22 Subsequent work, however, showed that IKAP is not 23 associated with the IKK's and plays no specific role in 24 NF-kappa B activation. We know that IKAP is homologous to 25 a yeast gene, Elp1 and that Elp1 is a member of the 0031 1 Elongator complex, so named because it was isolated in 2 association with RNA polymerase 2 during transcriptional 3 elongation. 4 Elongator is a six-subunit complex, and in fact, 5 earlier this year, Jesper's lab cloned the human Elongator 6 and has shown that it's also a six-subunit complex. 7 So recently in the literature, the role of this 8 Elongator complex in transcriptional elongation has been 9 questioned. In fact, there's a new paper suggesting that 10 IKAP plays a role in the regulation of activation of the 11 mammalian stress response via the JNK signaling pathway. 12 So clearly the verdict is still out on exactly what IKAP 13 is doing in this cell, but I think it's likely that it 14 might have multiple roles. 15 The major FD mutation that is present on over 16 99.5 percent of all chromosomes is a single base 17 substitution at base pair 6 of intron 20. It's a T to C

18 change, as I've shown here in pink. And as I mentioned, 19 it's an intron. 20 When we first identified this change, we didn't 21 see any functional consequence of this DNA change. It was 22 not a coding sequence change, and so therefore, we 23 continued to genotype large numbers of chromosomes in 24 order to build the genetic evidence that this was, in 25 fact, the pathogenic mutation. 0032 1 Over the years, we had amassed a large sample of 2 extended FD families that have been completely haplotyped, 3 which afforded us a very large pool of what we referred to 4 as non-FD chromosomes. Basically what this is chromosomes 5 we know not to carry FD by virtue of their haplotype. And 6 as you can see, the genetic evidence here is very strong 7 that, indeed, this DNA change is specific to the FD 8 chromosome. 9 The second mutation was identified by direct 10 side-by-side exon/intron sequencing of all four 11 heterozygous patients and identified a single base 12 substitution. Again, this is in exon 19 in the coding 13 sequence that causes an arginine to proline substitution. 14 This amino acid substitution is predicted to disrupt a 15 threonine phosphorylation site and in fact, Anderson, et 16 al. showed that R696P IKAP does, indeed, show reduced 17 phosphorylation in cells. 18 Now, as I mentioned to you, when we first 19 identified the FD mutation, we didn't see any functional 20 consequence. What do I mean by this? Well, if you look 21 here, when we amplified in the message over the region 22 that harbored the mutation from exon 18 to 23, we saw that 23 FD patients expressed the right-sized band. This is the 24 message. We had begun a collaboration with researchers in 25 Claus Scheidereit's group in Germany and had obtained IKAP 0033 1 antibodies, and we had, in fact, done a Western blot, 2 which is shown on this slide, that shows that FD patients 3 have IKAP protein. I'll remind you that FD is a recessive 4 disease, so our a priori expectation was that patients 5 would be missing a specific protein. 6 The key to understanding what was really going 7 on in FD came when we were able to examine FD brain. 8 Through our collaborators at NYU, we were able to obtain 9 two FD postmortem samples, and when we amplified across 10 the region in FD brain, what we saw was in fact this band 11 coming up which is missing exon 20. I'll refer to this 12 from now on as the mutant band. So we see that this band 13 was missing exon 20. 14 And when we went back and reexamined our 15 lymphoblast and fibroblast cell lines and optimized the 16 PCR conditions, you can see this band coming up in all FD 17 cell lines and not in controls missing exon 20, but 18 clearly there's a preponderance of the normal or wild type 19 message here. You can see from looking at this slide -- 20 and this is actually the figure that was published in our 21 paper -- lymphoblast lines express significantly more 22 normal than mutant, whereas several fibroblast lines show

23 more equal expression of these. 24 So, we went on then to develop assays that would 25 allow us to look at both the wild type and the mutant 0034 1 messages independently and amplify only those messages. 2 So what I'm showing on this slide is just an example of 3 this in FD cells. If you look at lymphoblasts and 4 fibroblasts, you can see clearly when you do what we call 5 the over-PCR or amplification using primers that flank the 6 exon 20, you see both bands coming up, and by the design 7 of primers, it allows us to amplify only the wild type 8 message and only the mutant message. And you can see in 9 all cases we see the presence of both. 10 In fact, when we went back with these specific 11 assays to the brain samples that we had originally 12 received, using the wild type assay, we actually saw 13 amplification of wild type IKAP from the brain samples. 14 So originally it appeared that the brain was expressing 15 only mutant, but when we looked specifically for the wild 16 type message, in fact, even though it is slight, it is 17 there. 18 So this observation led us to suggest that this 19 mutation in FD was manifesting in a tissue-specific 20 manner, and it also serves as the basis for a discrepancy 21 between the two original gene reports. So in the 22 Anderson, et al. paper, they showed us an FD lymphoblast 23 line that was expressing only the mutant band, not the 24 wild type, and so when we first saw this, we were very 25 puzzled. And it led us to hypothesize that perhaps the 0035 1 difference in our observations was due to tissue culture 2 techniques, since we were using cultured cells. So we 3 went on to do several different studies, IKAP expression 4 studies, to see if we could address this question. 5 To date, we've looked at over 81 different FD 6 lymphoblast cell lines and we assay these lines using a 7 combination of methods. We use a densitometric assay in 8 which we generate the integrated density value of each 9 band on ethidium-stained gel using an alpha imager, and we 10 calculate a ratio, a wild type to mutant ratio, of 11 message. And we also use quantitative PCR. And all of 12 the studies that I'll summarize for you today that we've 13 done in my lab over the last year have been verified using 14 quantitative PCR. 15 So the first thing we did was we went to 16 patients and we collected blood and made new cell lines 17 because clearly the cell lines that we were using in our 18 laboratory had been around for quite a number of years. 19 So those are shown by N here. So we made new cell lines. 20 We went to Corielle and we ordered some FD cell 21 lines from the Corielle cell repository because these were 22 the source of the lines that were used in the Anderson 23 study. And then we pulled some old cell lines out of the 24 freezer, ones that had been around for a long time and we 25 grew them under the conditions that we grew them all. 0036 1 What I'm showing in pink here is the Corielle line that
2 was presented in an Anderson paper and the same line that 3 was in our freezer for many years, and we pulled them out 4 and grew them. What we saw here was indicative of what we 5 saw in all lymphoblast lines, which was definitely 6 expression of both the wild type and the mutant message. 7 So we went on to do several other studies, and 8 overall I can tell you that in the lymphoblast lines that 9 we've looked at, the average wild type to mutant IKBKAP 10 ratio is approximately 3 to 1. We do see significant 11 fluctuation, however, between harvests and between cell 12 lines. It appears, however, that the cell lines vary in 13 concert. When we assayed these, they're either all up a 14 little or all down a little, which suggests that there is 15 some uncontrolled variability in the culture or in 16 harvesting that is shared by all cell lines. 17 We don't see any difference in expression due to 18 common antibiotics that are used in tissue culture, and we 19 also don't see any difference due to switching FBS, fetal 20 bovine serum, percentage. And the reason we did this was 21 because some of the cell lines that we ordered from 22 Corielle suggest that they be grown in 20 percent FBS, and 23 we routinely culture our lymphoblasts in 10 percent FBS. 24 But we didn't see any difference. 25 One difference we did observe is a significant 0037 1 difference. We see a higher wild type to mutant ratio in 2 cultures that are saturated rather than cultures that are 3 in log phase. And we don't have an explanation for this 4 right now, but we could suppose clearly the environment in 5 which cells are growing in saturation is very different 6 than those growing in log phase. 7 So the bottom line is we consistently see 8 expression of wild type IKAP in all patient cells, and in 9 fact, I can tell you we see expression in all patient 10 tissues of wild type. So to date, the discrepancy between 11 the original reports remains unexplained. 12 We've gone on to look at IKAP expression in FD 13 tissues. Through our collaborations at NYU and in 14 cooperation with the Brain Bank in Miami and our 15 collaborator at Hadassah, we've collected a large sample 16 of different FD tissues and looked at expression. What 17 I'd like to point out on this slide is just two things. 18 One is if you look over here, what we see in the 19 neural tissue is a preponderance of the mutant message. 20 As you can see, they do express some wild type message, 21 but they primarily express mutant message. You can see 22 some differences, some equal expression. 23 But the other thing I'd like to point out is if 24 you look at this lymphoblast line, clearly lymphoblast 25 cell lines are producing a lot of the wild type message, 0038 1 more than any of the other tissues. 2 We did one other thing that I haven't shown on 3 this slide. We went back to patients and we drew many 4 blood samples and we isolated RNA directly from the blood 5 to look at the expression levels in blood and compared 6 them to the lymphoblast cell lines that we had made on the

7 patients. In fact, what we see is more akin to the 8 fibroblasts. We see roughly equal expression of these two 9 messages in the RNA isolated directly from blood, whereas 10 the cell lines clearly express more wild type. So this is 11 obviously due to something going on in tissue culture, and 12 we don't know exactly what that is right now. 13 So now we've made what I think is a pretty 14 amazing observation, and that is, that FD cells are not 15 behaving as we would have supposed. Despite the fact that 16 it's a recessive disease, they are able to make some wild 17 type IKAP and wild type normal IKAP protein. 18 So the next logical question I think is can we 19 somehow increase the amounts or the ratio of wild type to 20 mutant IKAP. 21 So what we wanted to do was search for chemical 22 compounds that might increase this expression. So the 23 first thing we had to see was if we could use FD cells as 24 the basis for a screening tool. So what we did was looked 25 at parallel cultures. I mentioned that we see fluctuation 0039 1 in this ratio between cell lines and, in fact, across 2 harvests, but what you can see here is when you look at 3 parallel cultures, if we take a single cell line and split 4 them into parallel cultures and isolate and screen those 5 cultures, you can see very consistent expression in these 6 parallel cultures of the ratio of mutant to wild type. So 7 even though there's variability within the parallel 8 cultures, it's very consistent, which suggests that we 9 could use these FD cell lines as the basis for screening. 10 So we took part in the Neurodegeneration Drug 11 Screening Consortium that was sponsored by NINDS earlier 12 this year, and what we and the other consortium members 13 did was screen a panel of drugs. We did a first-pass 14 screen of a panel of 1,040 already FDA-approved drugs and 15 natural compounds to see if we can effect a change in our 16 cells. This month the meeting report will appear in 17 Trends in Neurosciences. 18 We completed the initial screen and what we are 19 doing now is doing the follow-up studies. We took the top 20 20 compounds that effected a change in terms of increasing 21 wild type to mutant because it is our hope that these 22 could potentially lead to therapies for FD. We're also 23 examining, however, the bottom 20, I guess you would call 24 it, the compounds that increased expression of the mutant 25 because these may be interesting mechanistically. 0040 1 So in our follow-up screen, we did a first-pass 2 screen using a single cell line for the initial pass. So 3 what we're doing is we're using multiple cell lines, 4 different cell types, and calculating dose curves and 5 things like this. And these studies are currently 6 underway. What we hope to do is to be able to use these 7 to then test these compounds that we identified in animal 8 models that are currently under construction. 9 So I'm going to switch gears a little bit here 10 now and take you back to your early basic genetics days 11 and talk about some other studies that are underway in my
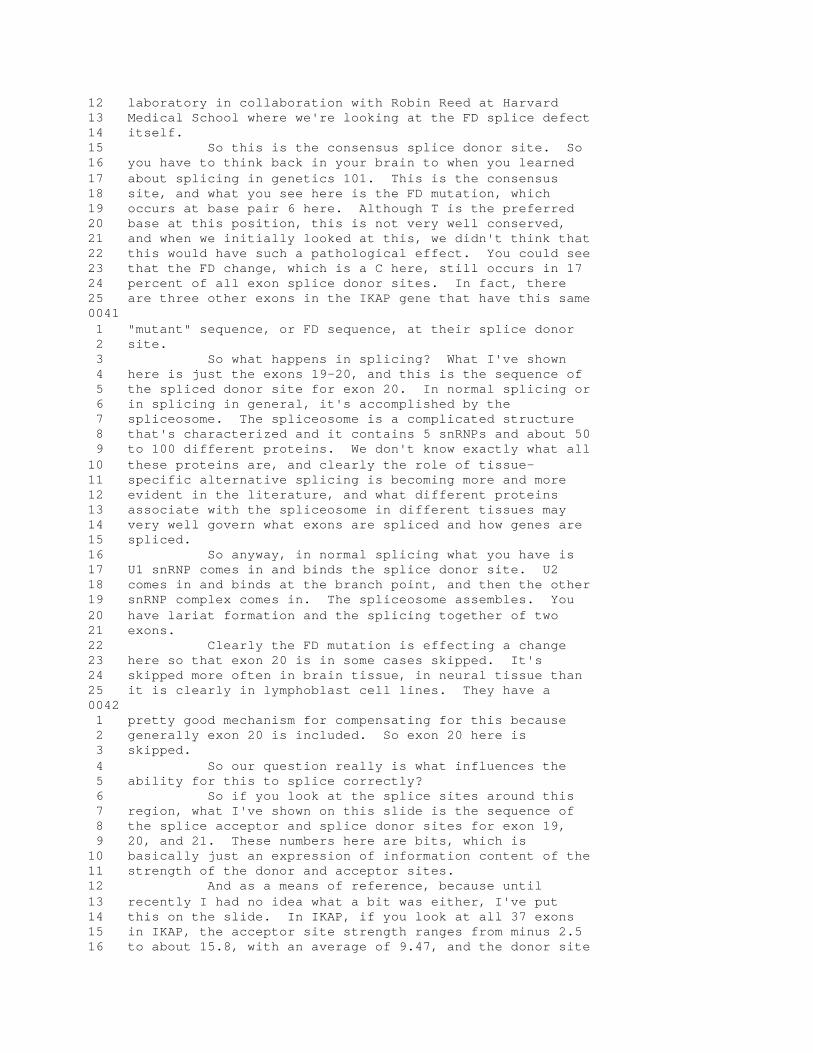
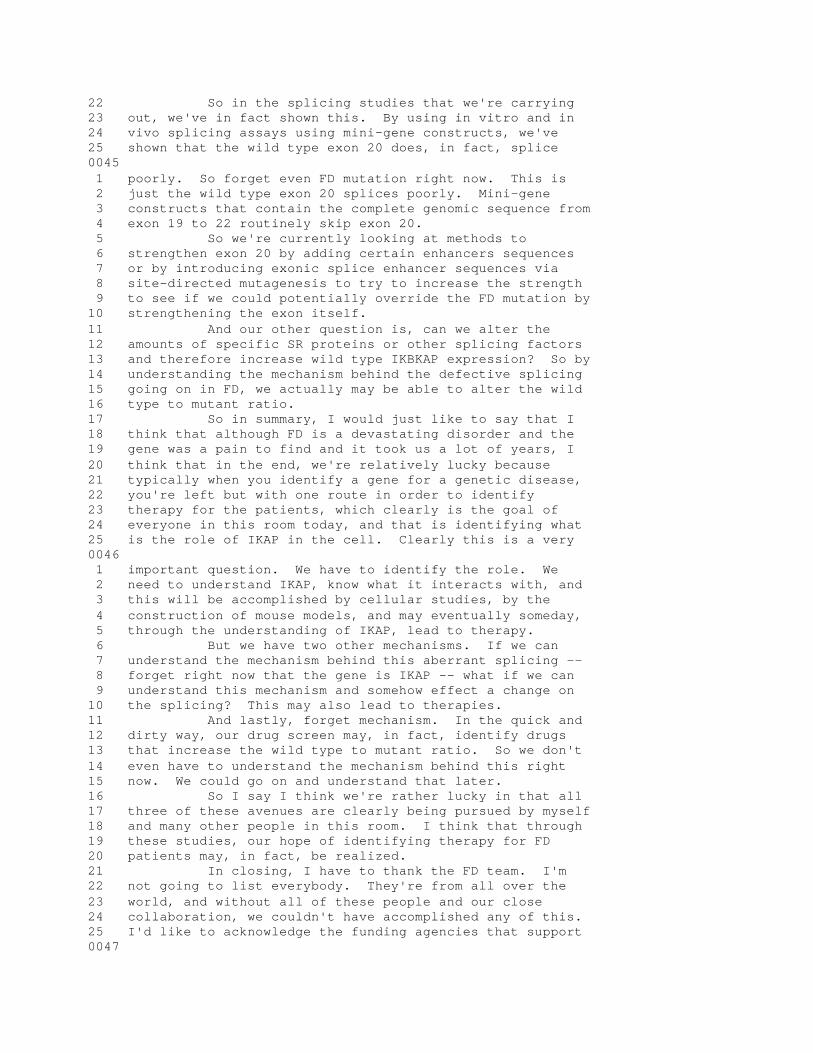
12 laboratory in collaboration with Robin Reed at Harvard 13 Medical School where we're looking at the FD splice defect 14 itself. 15 So this is the consensus splice donor site. So 16 you have to think back in your brain to when you learned 17 about splicing in genetics 101. This is the consensus 18 site, and what you see here is the FD mutation, which 19 occurs at base pair 6 here. Although T is the preferred 20 base at this position, this is not very well conserved, 21 and when we initially looked at this, we didn't think that 22 this would have such a pathological effect. You could see 23 that the FD change, which is a C here, still occurs in 17 24 percent of all exon splice donor sites. In fact, there 25 are three other exons in the IKAP gene that have this same 0041 1 "mutant" sequence, or FD sequence, at their splice donor 2 site. 3 So what happens in splicing? What I've shown 4 here is just the exons 19-20, and this is the sequence of 5 the spliced donor site for exon 20. In normal splicing or 6 in splicing in general, it's accomplished by the 7 spliceosome. The spliceosome is a complicated structure 8 that's characterized and it contains 5 snRNPs and about 50 9 to 100 different proteins. We don't know exactly what all 10 these proteins are, and clearly the role of tissue- 11 specific alternative splicing is becoming more and more 12 evident in the literature, and what different proteins 13 associate with the spliceosome in different tissues may 14 very well govern what exons are spliced and how genes are 15 spliced. 16 So anyway, in normal splicing what you have is 17 U1 snRNP comes in and binds the splice donor site. U2 18 comes in and binds at the branch point, and then the other 19 snRNP complex comes in. The spliceosome assembles. You 20 have lariat formation and the splicing together of two 21 exons. 22 Clearly the FD mutation is effecting a change 23 here so that exon 20 is in some cases skipped. It's 24 skipped more often in brain tissue, in neural tissue than 25 it is clearly in lymphoblast cell lines. They have a 0042 1 pretty good mechanism for compensating for this because 2 generally exon 20 is included. So exon 20 here is 3 skipped. 4 So our question really is what influences the 5 ability for this to splice correctly? 6 So if you look at the splice sites around this 7 region, what I've shown on this slide is the sequence of 8 the splice acceptor and splice donor sites for exon 19, 9 20, and 21. These numbers here are bits, which is 10 basically just an expression of information content of the 11 strength of the donor and acceptor sites. 12 And as a means of reference, because until 13 recently I had no idea what a bit was either, I've put 14 this on the slide. In IKAP, if you look at all 37 exons 15 in IKAP, the acceptor site strength ranges from minus 2.5 16 to about 15.8, with an average of 9.47, and the donor site

17 strength ranges from 3.2 to 13, with an average of 8.94. 18 So you can see that if you look at exon 19, it 19 has an incredibly weak -- in fact, the weakest in the gene 20 -- splice acceptor site. However, we know exon 19 doesn't 21 have any problems with splicing. 22 If you look here, the FD mutation drops the 23 bits, or the information, for the splice donor site from 24 10.1 to 8.7, but still not a drastic change or a drastic 25 reduction in the information content in this splice site. 0043 1 So clearly there's more going on in splicing than just 2 this strength or weakness of the splice sites. 3 So in this lovely figure that I lifted from a 4 review, I'm going to talk to you a minute about exonic 5 splice enhancers. As I said, the splicing process is very 6 complicated, and the spliceosome is made of many different 7 proteins. And there's a class of proteins called SR 8 proteins that are known to contribute to splicing. And in 9 fact, through knock-out studies, it's been shown that 10 these SR proteins are not only necessary for splicing, but 11 necessary for development. 12 So there are sequences called exonic splice 13 enhancers that are able to bind these SR proteins, and the 14 SR proteins serve as splice enhancers, which then serve to 15 recruit the splicing complexes and enhance the splicing of 16 particular exons. 17 So for the class of SR proteins, now these 18 exonic splice enhancers, there are sequences that have 19 been identified using various methods. It is now believed 20 that all exons contain exonic splice enhancers, multiple 21 exonic splice enhancers it is likely. I need to point 22 out, though, that these are just predicted based on 23 binding sequence, and certainly, like I said, it's a very 24 complex process. There are also exonic splice silencers. 25 So until you look at a specific region experimentally, 0044 1 it's very difficult to say exactly what's going on. But 2 looking at this slide gives us an idea. 3 If you look at exon 19, which has the worst 4 splice acceptor site in all of IKBKAP, and then you do an 5 exonic splice enhancer prediction, you see that there are 6 23 different exonic splice enhancers predicted to lie 7 within this exon. If you look at exon 21, which has very 8 strong splice sites, there are only 6. But if you look at 9 exon 20, which has pretty weak acceptor sites, you see 10 that there's only 4 predicted splice sits. In fact, if 11 you look at all of the IKAP gene, at all exons with weak 12 splice sites, the average number of predicted exonic 13 splice enhancers is 16.8. So 4 is pretty low. 14 So what we begin to see emerging here is 15 potentially a picture of a weakly splicing area and 16 perhaps the FD mutation is just the straw that broke the 17 camel's back, that this area is weak in terms of splicing 18 and that this mutation introduced here has a drastic 19 effect on splicing; whereas, a similar mutation at base 20 pair 6 of the splice donor site in another exon may not, 21 in fact, be pathogenic at all.
22 So in the splicing studies that we're carrying 23 out, we've in fact shown this. By using in vitro and in 24 vivo splicing assays using mini-gene constructs, we've 25 shown that the wild type exon 20 does, in fact, splice 0045 1 poorly. So forget even FD mutation right now. This is 2 just the wild type exon 20 splices poorly. Mini-gene 3 constructs that contain the complete genomic sequence from 4 exon 19 to 22 routinely skip exon 20. 5 So we're currently looking at methods to 6 strengthen exon 20 by adding certain enhancers sequences 7 or by introducing exonic splice enhancer sequences via 8 site-directed mutagenesis to try to increase the strength 9 to see if we could potentially override the FD mutation by 10 strengthening the exon itself. 11 And our other question is, can we alter the 12 amounts of specific SR proteins or other splicing factors 13 and therefore increase wild type IKBKAP expression? So by 14 understanding the mechanism behind the defective splicing 15 going on in FD, we actually may be able to alter the wild 16 type to mutant ratio. 17 So in summary, I would just like to say that I 18 think that although FD is a devastating disorder and the 19 gene was a pain to find and it took us a lot of years, I 20 think that in the end, we're relatively lucky because 21 typically when you identify a gene for a genetic disease, 22 you're left but with one route in order to identify 23 therapy for the patients, which clearly is the goal of 24 everyone in this room today, and that is identifying what 25 is the role of IKAP in the cell. Clearly this is a very 0046 1 important question. We have to identify the role. We 2 need to understand IKAP, know what it interacts with, and 3 this will be accomplished by cellular studies, by the 4 construction of mouse models, and may eventually someday, 5 through the understanding of IKAP, lead to therapy. 6 But we have two other mechanisms. If we can 7 understand the mechanism behind this aberrant splicing -- 8 forget right now that the gene is IKAP -- what if we can 9 understand this mechanism and somehow effect a change on 10 the splicing? This may also lead to therapies. 11 And lastly, forget mechanism. In the quick and 12 dirty way, our drug screen may, in fact, identify drugs 13 that increase the wild type to mutant ratio. So we don't 14 even have to understand the mechanism behind this right 15 now. We could go on and understand that later. 16 So I say I think we're rather lucky in that all 17 three of these avenues are clearly being pursued by myself 18 and many other people in this room. I think that through 19 these studies, our hope of identifying therapy for FD 20 patients may, in fact, be realized. 21 In closing, I have to thank the FD team. I'm 22 not going to list everybody. They're from all over the 23 world, and without all of these people and our close 24 collaboration, we couldn't have accomplished any of this. 25 I'd like to acknowledge the funding agencies that support 0047

1 the work in my laboratory. 2 Thank you. 3 (Applause.) 4 DR. AXELROD: Thank you, Dr. Slaugenhaupt. 5 Our next speaker will be the professor, Dr. 6 Hilz. We're talking about eventually treating FD 7 patients, but without a way of assessing what has happened 8 before, we will not be able to judge what will happen in 9 the future. So Professor Hilz will give us an insight as 10 to clinical assessment of our patients. 11 DR. HILZ: Thank you, Felicia. I'd also like to 12 thank the organizers for giving me the opportunity to 13 present some of the work we have done over the last 10 14 years. 15 When I first started to work with Dr. Axelrod, I 16 looked at the patients from the perspective of a 17 conventional neurophysiologist and I rapidly learned that 18 the given neuropathology, which you have already been 19 introduced to, does not allow us to use conventional 20 techniques. 21 You have seen this slide that indicates that it 22 is primarily the unmyelinated fibers that are largely 23 reduced. In the peripheral nerves, you barely find any of 24 the unmyelinated fibers in the sural nerve biopsy. And 25 therefore, conventional techniques of nerve conduction 0048 1 studies don't take us very far. What we saw is this 2 double-peaked response in the motor conduction velocity or 3 a double peak in the sensory nerve action potential, a 4 finding that's been already described in '67 that does not 5 allow us to really quantify severity of the pathology. It 6 might be helpful to assess disease progression over 7 decades, but it doesn't assess the current situation of 8 the patient. 9 In order to quantify peripheral nerve function, 10 we had to use psychophysical methods of quantitative 11 thermal testing. This procedure depends on the patient 12 cooperation. A small Peltier element, also called the 13 Thermode, is attached to the patient's skin and with 14 quantitative stimuli of cold or of warm or heat, we can 15 then judge the function of thinly myelinated A delta 16 fibers that mediate cold or unmyelinated C fibers that 17 mediate heat or warmth perception. 18 There are various algorithms that can be used. 19 We used the simple method of limits because it is 20 straightforward and allows us to test children. After 21 calibration, the Thermode delivers a warm stimulus. As 22 soon as the patient perceives the stimulus, he stops 23 further stimulation. The stimulation returns to baseline, 24 and this is repeated several times. We then take the warm 25 or cold threshold as the average of the peak-to-baseline 0049 1 differences, and that gives us quite a good impression of 2 A delta and C fiber function. 3 The question was does that work in the young 4 children. There were no data available in children, so we 5 had to first establish a database that clearly showed that

6 even in very young children, the technique provides 7 reliable information regarding small fiber function. 8 What we saw is highly abnormal warm and cold 9 perception in the FD patient. On average, cold and warm 10 thresholds were up to 8 to 10 times higher than in the 11 control group regardless of the tested body site. We 12 tested up to six different body sites. 13 Dr. Axelrod already pointed out that the 14 reduction of peripheral small nerve fibers is very similar 15 to the reduction of sympathetic neurons, of neurons in the 16 intermediolateral column or in cervical and thoracic 17 ganglia. And she also pointed out that there is a high 18 rate of unexplained death, and so far, there are no risk 19 predictors that might indicate whether an individual 20 patient is at specific risk. 21 So we were wondering whether a combination of 22 evaluation of the peripheral nerve function and autonomic 23 function might help us identify patients at risk, and we 24 did a correlation of peripheral small fiber function as 25 assessed with a temperature perception procedure and of 0050 1 cardiac parameters, and for that we used the corrected QT 2 interval. 3 What we actually saw is that there is a 4 correlation between impaired small fiber function as 5 expressed by increased thermal perception thresholds and 6 impaired autonomic control, in this case expressed by QTc 7 prolongation. What we found was that 4 of our patients in 8 a group out of 20 who had abnormal cardiac parameters also 9 had severely impaired peripheral small fiber function. 10 Probably more importantly, 3 of the patients who had 11 severely abnormal peripheral nerve function experienced 12 cardiac arrest within one year after the study. 13 Of course, this is just a surrogate marker, and 14 to better understand risk factors, we conducted a variety 15 of studies evaluating the peripheral cardiovascular and 16 the central autonomic nervous system. And I cannot go 17 into all these tests. We did a cold face, cold pressor, 18 Valsalva test. We challenged the orthostatic control. We 19 conducted baro- and chemoreflex studies and tested 20 vasomotor control and lately conducted a gastrointestinal 21 challenge test. 22 I'd just like to point out that a trivial test 23 like the cold face test allows us to gain further insight 24 into the pathology. This is a test where you stimulate 25 the trigeminal area with ice and that activates in the 0051 1 brainstem a response to the peripheral sympathetic 2 sudomotor system with vasoconstriction and blood pressure 3 increase, but simultaneously activates in the brainstem 4 the cardiovagal, the parasympathetic system and induces a 5 bradycardia, and this bradycardia is considered to be 6 independent from the baroreflex. 7 So in the patients, we did not see with this 8 test any increase of blood pressure as we saw in the 9 controls. We did not see any reflex bradycardia, and more 10 importantly, heart rate variability didn't change at all
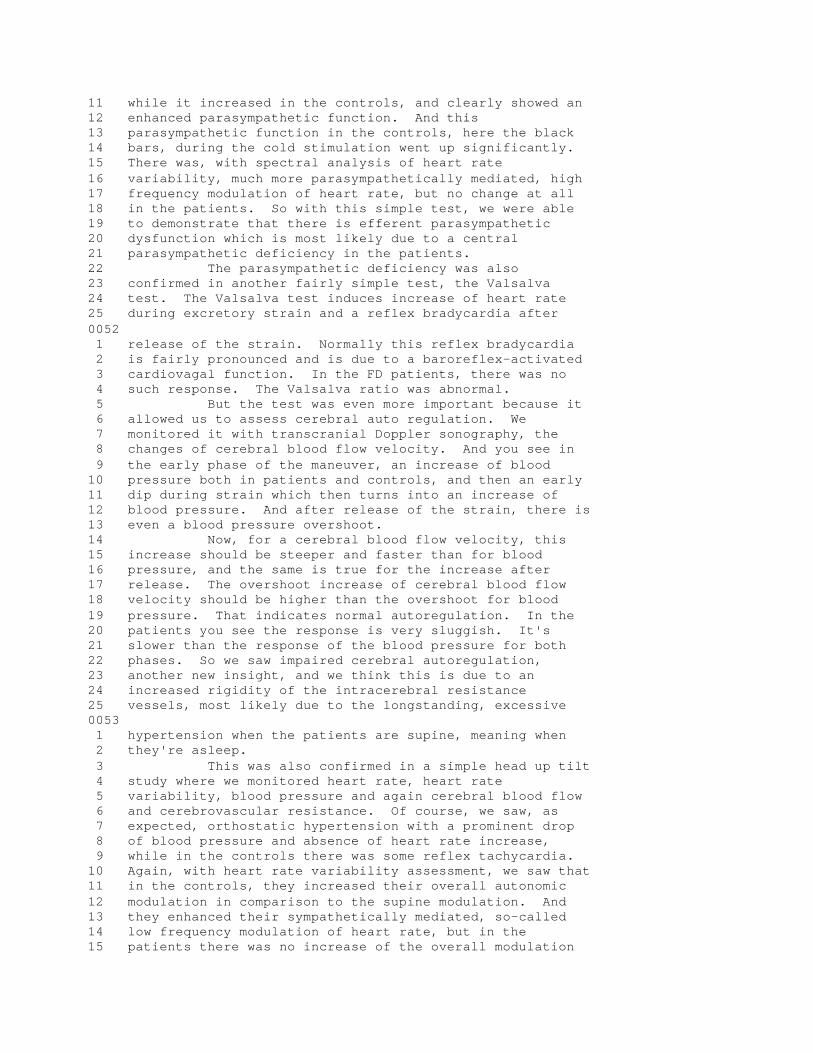
11 while it increased in the controls, and clearly showed an 12 enhanced parasympathetic function. And this 13 parasympathetic function in the controls, here the black 14 bars, during the cold stimulation went up significantly. 15 There was, with spectral analysis of heart rate 16 variability, much more parasympathetically mediated, high 17 frequency modulation of heart rate, but no change at all 18 in the patients. So with this simple test, we were able 19 to demonstrate that there is efferent parasympathetic 20 dysfunction which is most likely due to a central 21 parasympathetic deficiency in the patients. 22 The parasympathetic deficiency was also 23 confirmed in another fairly simple test, the Valsalva 24 test. The Valsalva test induces increase of heart rate 25 during excretory strain and a reflex bradycardia after 0052 1 release of the strain. Normally this reflex bradycardia 2 is fairly pronounced and is due to a baroreflex-activated 3 cardiovagal function. In the FD patients, there was no 4 such response. The Valsalva ratio was abnormal. 5 But the test was even more important because it 6 allowed us to assess cerebral auto regulation. We 7 monitored it with transcranial Doppler sonography, the 8 changes of cerebral blood flow velocity. And you see in 9 the early phase of the maneuver, an increase of blood 10 pressure both in patients and controls, and then an early 11 dip during strain which then turns into an increase of 12 blood pressure. And after release of the strain, there is 13 even a blood pressure overshoot. 14 Now, for a cerebral blood flow velocity, this 15 increase should be steeper and faster than for blood 16 pressure, and the same is true for the increase after 17 release. The overshoot increase of cerebral blood flow 18 velocity should be higher than the overshoot for blood 19 pressure. That indicates normal autoregulation. In the 20 patients you see the response is very sluggish. It's 21 slower than the response of the blood pressure for both 22 phases. So we saw impaired cerebral autoregulation, 23 another new insight, and we think this is due to an 24 increased rigidity of the intracerebral resistance 25 vessels, most likely due to the longstanding, excessive 0053 1 hypertension when the patients are supine, meaning when 2 they're asleep. 3 This was also confirmed in a simple head up tilt 4 study where we monitored heart rate, heart rate 5 variability, blood pressure and again cerebral blood flow 6 and cerebrovascular resistance. Of course, we saw, as 7 expected, orthostatic hypertension with a prominent drop 8 of blood pressure and absence of heart rate increase, 9 while in the controls there was some reflex tachycardia. 10 Again, with heart rate variability assessment, we saw that 11 in the controls, they increased their overall autonomic 12 modulation in comparison to the supine modulation. And 13 they enhanced their sympathetically mediated, so-called 14 low frequency modulation of heart rate, but in the 15 patients there was no increase of the overall modulation

16 and no change of the sympathetic or parasympathetic 17 activity. 18 More importantly, we saw a discrepancy between 19 the peripheral drop of blood pressure due to lack of 20 peripheral sympathetic activity and an unexpected 21 secondary increase of cerebral blood flow velocity which 22 contrasted with the slight drop of cerebral blood flow 23 velocity in the controls. This again indicates impaired 24 cerebral autoregulation and might be due to a preserved 25 central sympathetic activity or discharge of neural 0054 1 humoral factors. It seems to be due to increased rigidity 2 of the resistance vessels and that again might result from 3 the longstanding changes between permanent orthostatic 4 hypotension and nocturnal hypertension. 5 During orthostasis, the patients are not only 6 unable to modulate their autonomic control, but they, 7 moreover, cannot even enhance their cardiac stroke volume. 8 While the cardiac output increases significantly upon 9 orthostatic challenge in control persons, there's even a 10 drop of cardiac output in the patients, and the patients 11 cannot compensate the shift of the fluid to the lower 12 extremities by increasing peripheral vasoconstriction, but 13 the total peripheral resistance that goes up significantly 14 in the controls only increases insignificantly and 15 sluggishly in the patients. 16 So given the lack of central and peripheral 17 sympathetic and parasympathetic modulation, the lack of 18 adaptation of stroke volume or peripheral resistance, we 19 were wondering how do the patients still increase their 20 blood pressure and their autonomic output during this 21 autonomic crisis, how do they generate sweating, 22 peripheral vasoconstriction, mottling of skin. Is that 23 due to denervation or hypersensitivity or is it due to a 24 central autonomic dysregulation? 25 To better understand this, we did a 0055 1 microdialysis study. We inserted a micro-catheter into 2 the superficial skin layers, and this catheter was 3 perfused with electrolyte solution, and then we added some 4 drugs to the solution. We were able to measure the drug- 5 induced changes of skin blood flow by means of laser 6 Doppler flowmetry, the changes of humidity output, and of 7 course, we were able to measure the amount of plasma 8 extravasation. 9 For vasoconstriction, we added norepinephrine 10 and we analyzed changes of skin blood flow, plasma 11 extravasation, and the area of skin blanching due to the 12 vasoconstrictor substance. 13 For sudomotor function, we added acetylcholine 14 and measured sweat output by means of quantitative 15 sudomotor axon reflex testing and transepidermal water 16 loss measurement. 17 We didn't see any major changes of the axon 18 reflex sweating, no difference between patients and 19 controls, but we saw hypersensitivity to norepinephrine. 20 There was an earlier start of vasoconstriction in the

21 patients, here the dotted line, and the reduction of 22 plasma extravasation with norepinephrine just lasted 23 longer than in the control group. Moreover, the area of 24 blanching was greater than in the controls. 25 So there seems to be a peripheral denervation 0056 1 hypersensitivity, and that might account for some of the 2 hypertension seen during crisis. But there must also be 3 some central component as suggested by the normal sweat 4 responses. 5 To better understand the central mechanisms, we 6 did a selective stimulation of the response of the 7 sympathetic branch and the parasympathetic branch of the 8 autonomic nervous system by activating the baroreflex with 9 suction-neck chamber. We applied a sinusoidal vacuum that 10 stimulates the carotid baroreceptors and we used a 11 pressure of minus 30 millimeters mercury. This procedure, 12 developed by Luciano Bernardi, allows us to quantify the 13 response of the sympathetic system at the level of the 14 heart and blood vessels. If you apply this stimulus at a 15 frequency of 6 cycles per minute, that's .1 hertz, and if 16 you double the frequency to 12 cycles, the sympathetic 17 cannot follow anymore and the response is only a 18 parasympathetically mediated response at the level of the 19 heart. Respiration is kept constant to avoid 20 interferences of the respiratory influences. 21 So here in one control person, you see the 22 respiratory peak due to the paced breathing. You see the 23 same peak in the patient, and now with sympathetic 24 stimulation, or a .1 hertz stimulation, we have a clear- 25 cut sympathetic response in the control, but no such 0057 1 response in the patient. 2 The same held true for the whole group. In the 3 controls we saw a clear-cut increase of sympathetic 4 output, but no such response in the patients. And for the 5 parasympathetic, .2 hertz stimulation, or the 6 parasympathetic response to the .2 hertz stimulation, 7 again in the controls we see a significant parasympathetic 8 activity, but no increase in the patients. So they're 9 unable to enhance their sympathetic and parasympathetic 10 responses. 11 The same was confirmed when we looked at 12 systolic and diastolic blood pressure changes during .1 13 hertz stimulation in controls and in patients. Again, in 14 the patients, no sympathetic response. 15 Now, given the fact that the baroreflex is 16 compromised and knowing that the patients have respiratory 17 problems -- they have breath-holding spells, sleep apnea. 18 They can, as Dr. Axelrod already pointed out, not trust 19 their respiratory pattern to environmental needs when 20 they're in an airplane, or when they have respiratory 21 infection, they cannot trust the frequency or the volume. 22 And we also know that many of the causes of death are due 23 to pulmonary or unexplained cardiovascular events. 24 This is extremely important if we see this in 25 combination with the impaired baroreflex function. Somers
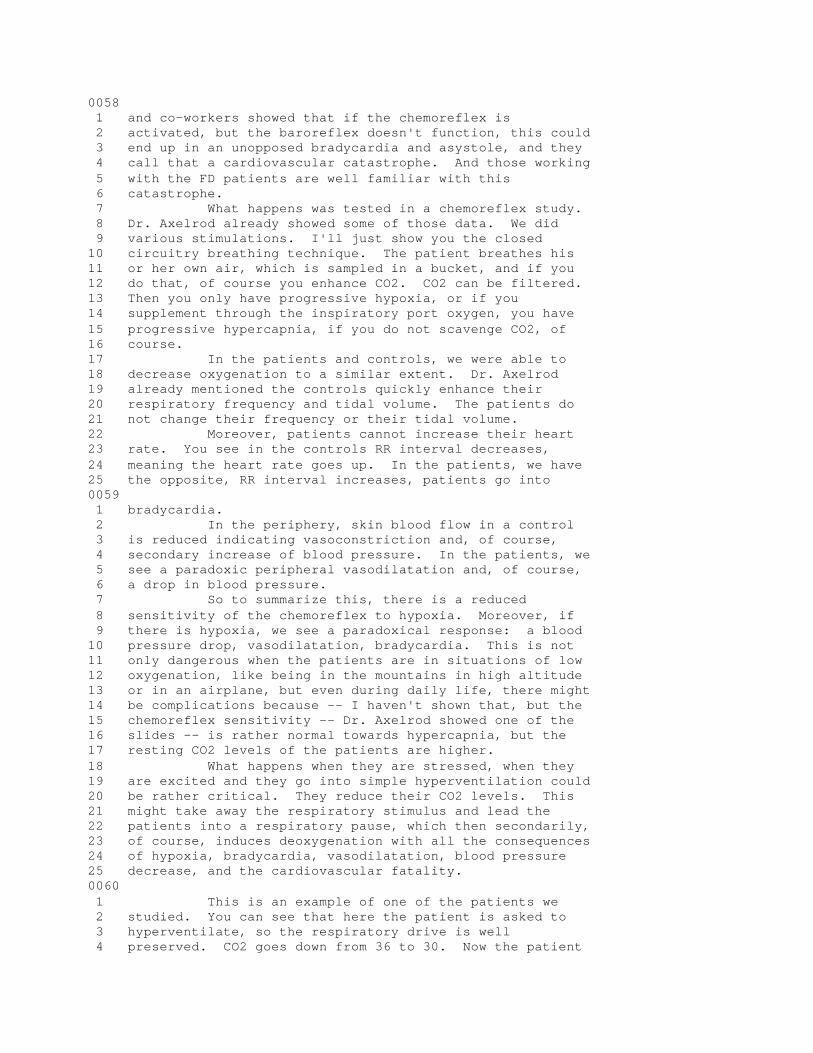
0058 1 and co-workers showed that if the chemoreflex is 2 activated, but the baroreflex doesn't function, this could 3 end up in an unopposed bradycardia and asystole, and they 4 call that a cardiovascular catastrophe. And those working 5 with the FD patients are well familiar with this 6 catastrophe. 7 What happens was tested in a chemoreflex study. 8 Dr. Axelrod already showed some of those data. We did 9 various stimulations. I'll just show you the closed 10 circuitry breathing technique. The patient breathes his 11 or her own air, which is sampled in a bucket, and if you 12 do that, of course you enhance CO2. CO2 can be filtered. 13 Then you only have progressive hypoxia, or if you 14 supplement through the inspiratory port oxygen, you have 15 progressive hypercapnia, if you do not scavenge CO2, of 16 course. 17 In the patients and controls, we were able to 18 decrease oxygenation to a similar extent. Dr. Axelrod 19 already mentioned the controls quickly enhance their 20 respiratory frequency and tidal volume. The patients do 21 not change their frequency or their tidal volume. 22 Moreover, patients cannot increase their heart 23 rate. You see in the controls RR interval decreases, 24 meaning the heart rate goes up. In the patients, we have 25 the opposite, RR interval increases, patients go into 0059 1 bradycardia. 2 In the periphery, skin blood flow in a control 3 is reduced indicating vasoconstriction and, of course, 4 secondary increase of blood pressure. In the patients, we 5 see a paradoxic peripheral vasodilatation and, of course, 6 a drop in blood pressure. 7 So to summarize this, there is a reduced 8 sensitivity of the chemoreflex to hypoxia. Moreover, if 9 there is hypoxia, we see a paradoxical response: a blood 10 pressure drop, vasodilatation, bradycardia. This is not 11 only dangerous when the patients are in situations of low 12 oxygenation, like being in the mountains in high altitude 13 or in an airplane, but even during daily life, there might 14 be complications because -- I haven't shown that, but the 15 chemoreflex sensitivity -- Dr. Axelrod showed one of the 16 slides -- is rather normal towards hypercapnia, but the 17 resting CO2 levels of the patients are higher. 18 What happens when they are stressed, when they 19 are excited and they go into simple hyperventilation could 20 be rather critical. They reduce their CO2 levels. This 21 might take away the respiratory stimulus and lead the 22 patients into a respiratory pause, which then secondarily, 23 of course, induces deoxygenation with all the consequences 24 of hypoxia, bradycardia, vasodilatation, blood pressure 25 decrease, and the cardiovascular fatality. 0060 1 This is an example of one of the patients we 2 studied. You can see that here the patient is asked to 3 hyperventilate, so the respiratory drive is well 4 preserved. CO2 goes down from 36 to 30. Now the patient
5 suddenly stops to breathe. Here the patient went into 6 tachycardia, shortening of RR intervals. As soon as 7 respiration stops, this tachycardia turns into bradycardia 8 which would progress. Here you see the secondary 9 deoxygenation. Oxygen goes down. And now Dr. Axelrod 10 just squeezed the patient and said, come on, take a 11 breath, and this stabilizes the situation again. But what 12 if Dr. Axelrod or Dr. Maayan is not around at night? Then 13 the patients might well go into unopposed asystole, and 14 this might lead to a fatality. 15 Let me end by saying we know FD is a progressive 16 disease. Still, the treatment efforts, the clinical risk 17 stratification like fundoplication, gastrostomy, have 18 improved the life expectancy significantly, as Dr. Axelrod 19 has indicated. And there is a chance to further improve 20 it. 21 I am afraid -- as a clinician I may say that -- 22 that those patients who taught us about the disease and 23 who taught us about the gene are not likely to benefit 24 from gene therapy within the next one or two years, but 25 their disease and their problems are still progressing. 0061 1 Therefore, I believe that it is essential to further 2 improve the understanding of the peripheral and central 3 autonomic pathophysiology, particularly of the changes 4 that happen during daytime and during nighttime, and this 5 might lead us to further therapeutical options that 6 hopefully help to improve the quality of the patients and 7 their lives. 8 Thank you. 9 (Applause.) 10 DR. GWINN-HARDY: Thanks a lot. I'm going to, 11 in the interest of time, suggest that we skip the break 12 and move right on into the next talk. Of course, I want 13 people to feel free to get up and get snacks and go to the 14 bathroom as they need to. But the most important thing I 15 think is that we don't sacrifice the discussion because I 16 know that I for one have a lot of questions to ask the 17 speakers. So let's move right on into the next talk then, 18 if that's all right. 19 Felicia, do you want to briefly introduce the 20 next speaker? Thank you. 21 DR. AXELROD: Our next speaker is Dr. Gail 22 Sonenshein. She is the head of the Scientific Advisory 23 Board of the Dysautonomia Foundation, and she is going to 24 talk about future directions for familial dysautonomia, 25 sort of an overview and maybe a wish list. 0062 1 DR. SONENSHEIN: I too want to thank the 2 organizers and the NIH for sponsoring this meeting. 3 I think following the successful identification 4 of the involvement of the IKAP protein in FD by two 5 groups, it led the Scientific Advisory Board to sponsor a 6 brainstorming session in New York last year, and that 7 Scientific Advisory Board was being headed at that point 8 by Kurt Hirschhorn, and actually I was invited to 9 participate. Little did I know what would happen as a

10 result of that invitation. 11 So from that brainstorming session, what came 12 out was an RFA for what we viewed at the time were the 13 research directions that we would like to forward in the 14 quest of understanding more of the disease and possibly 15 arriving at a treatment. So this summarizes the research 16 directions that came out of that. 17 One was to elucidate the function of the IKAP 18 protein and to identify interacting proteins. 19 Next was to determine the loss of IKAP function 20 and how it affects cellular processes and survival. 21 To elucidate the control of tissue-specific 22 splicing in gene expression and potential to mediate 23 correction of splicing defects. 24 To elucidate the role of IKAP in the development 25 and maintenance of the autonomic and sensory nervous 0063 1 system. 2 And to determine the effects of IKAP knock-in 3 and knock-out mutations using mouse or other animal 4 models. 5 And lastly, but certainly not least, to search 6 for novel therapeutic strategies for FD. We've already 7 heard from Sue, and we're going to hear from Drs. 8 Svejstrup and Xu who are all being actually funded by the 9 foundation. 10 So I think the key issue still to date is 11 exactly what does IKAP do, and I think that Sue sort of 12 summarized a little bit, but IKAP was originally 13 identified as a component of the IKK complex which is 14 involved in activation of NF-kappa B which is actually the 15 transcription factor that I work on. 16 It turned out that that appears to be a false 17 lead. Many people now have repurified the IKK, and when I 18 called members of the NF-kappa B group who work on it, I 19 either got polite or rude or sort of aggressive answers, 20 telling me that they have, of course, wasted a lot of 21 their time. IKAP is not in the IKK complex. 22 Fortunately, work by Dr. Jasper has shown that 23 IKAP is part of a complex which was first identified in 24 yeast. It appears to be involved in transcriptional 25 elongation control. The whole complex is called 0064 1 Elongator. The yeast homologue is Elp1, and as Sue 2 mentioned, Elongator has now been found in mammalian cells 3 both by Dr. Svejstrup's group and also by Danny Reinberg's 4 group. 5 I think there are some issues related to this 6 about the localization of the IKAP and the Elongator 7 complex, and I'll show you a few reasons why I think 8 there's still an issue with this in just a few seconds. 9 Microarray data was performed on the yeast by 10 Krogan and Greenblatt, and they identified a subset of 11 genes that were affected and many of them are, in fact, 12 involved in metabolism. But there's still a lot to learn 13 about the function of IKAP, and hopefully we'll get some 14 more microarray data shortly to help us with this in human

15 cells. 16 I think since Dr. Svejstrup is really going to 17 talk about the Elongator, I just want to point out that 18 there is a new paper that has just been published on 19 another role, a potential functional role of IKAP. I 20 don't think that the fact that we have two potential 21 functions means that one is right and one is wrong. I 22 think that in many cases in eukaryotic biology, you can 23 have a component of one complex actually play another 24 functional role. So it remains to be seen what's really 25 happening, and obviously the next six months will probably 0065 1 be very helpful in elucidating some of this. 2 The other functional role of IKAP is involving 3 it in stress responses, and the evidence indicates that 4 IKAP can interact with a specific kinase called the c-Jun 5 kinase, or JNK, and it is interacting via its C terminus, 6 IKAP C terminus. JNK not only targets IKAP, but IKAP 7 potentiates the kinase activity. Actually I didn't 8 realize that the senior author of this would be here, Dr. 9 Kallunki. I think this is sufficiently important for 10 people to know about this data that I took some of the 11 figures. That's the power of the Adobe Acrobat. I took 12 some of the figures her paper illustrate some of the 13 points. 14 So it was a yeast two-hybrid screen that 15 identified the interaction between JNK and IKAP, but 16 that's actually not considered stringent enough proof. So 17 the group showed by co-immunoprecipitation that if you 18 precipitate JNK, you find IKAP. So that clearly indicates 19 an IKAP-JNK association. 20 This is an immunohistochemistry looking at IKAP 21 and JNK localization within the cell, and this is the 22 issue. IKAP complex appears to be located not exclusively 23 because Danny Reinberg's group purified the Elongator 24 complex actually from the nucleus of HeLa cells. So 25 there's clearly presence in the nucleus, but a lot of it 0066 1 appears to be in the cytoplasm. 2 This is the JNK staining, and here is the 3 overlay. Actually it's not yellow. It's orange, so 4 unless I'm reading this wrong -- and fortunately, Dr. 5 Kallunki is here so she could comment if I'm misstating. 6 But it looks like it's not a total overlap. 7 These are further analyses showing the presence 8 of IKAP using a tagged IKAP, and what you can see, again 9 here's one tag or another tag. It's predominantly in the 10 cytoplasm, and that's actually also been shown in Danny 11 Reinberg's paper where he actually also looked at making 12 in HeLa cells with an antibody he prepared and also finds 13 it predominantly in the cytoplasm. It doesn't mean it 14 cannot move to the nucleus under certain stimuli, and 15 that's actually one of the issues that may become 16 important to look at. 17 This is evidence. I didn't take the figure that 18 shows that JNK actually can phosphorylate IKAP, but that 19 was done in vitro. These are analyses showing that the
20 signaling cascade by JNK is affected by IKAP in the sense 21 that it potentiates the ability of the kinase to function. 22 So this is downstream. There's a full cascade that's been 23 worked out, and this is one of the kinases that's 24 upstream. What you can see is this is the kinase activity 25 in the absence of IKAP, and this is the presence of IKAP. 0067 1 And you see there's enhanced activity. 2 JNK kinase is what responds in stress to certain 3 stimuli, UV, TNF, and EGF. And this is the JNK activity 4 in the absence of IKAP in all these responses. They are 5 stimulated in the presence of IKAP. 6 So what this implicates is the IKAP protein may 7 be playing an important role in modulating JNK activity, 8 that this kinase activity is the major stress response. 9 I think what's even more interesting was the 10 fact that when they did the yeast two-hybrid work, the 11 IKAP protein that they pulled out was actually a portion 12 of the C terminus and that's the part that interacts. So 13 if you look at the IKAP protein that would be produced by 14 the FD as a result of the mutation, what you see is it's 15 not containing that part. So if the role of IKAP is to, 16 in some way, affect the JNK response, then the FD kids 17 would have an altered response. 18 I apologize for taking so much time. Dr. 19 Kallunki obviously should have, I guess, been here to 20 present it. 21 So what do we need? I think what we need is 22 mouse models. We have to able to elucidate the role of 23 IKAP and the effects of the mutations on the nervous 24 system. One of the things that we'll be able to do from 25 knock-in mice, with both major and minor mutations, would 0068 1 be to get models and cells to elucidate both mechanisms, 2 as well as to test potential treatments for therapy. 3 We're also looking at making knock-out mice with 4 the Cre locks which would allow us to put it into any 5 developmental system or actually in any cell type 6 depending upon the promoter. And all of this work is 7 being funded, and Dr. Xu is going to talk today. 8 So where do we go from here? I think obviously 9 there are a lot of things we need to do. One is to 10 identify potential therapeutic drugs that promote the 11 splicing. This would obviously be in many ways we presume 12 for the major mutation, although we don't know. Maybe 13 pushing a splicing might be of help in other ways as well. 14 The FD Foundation is funding work by Jim Gusella in this 15 aspect. 16 We're also interested in elucidating the role of 17 IKAP in neural cell survival and to identify potential 18 targets of IKAP or the total Elongator. The targets may 19 be alternative ways of treating patients because these are 20 essential pharmacologic targets as well as the IKAP 21 itself. So that's another way of looking at the issue. 22 And the foundation is funding Math Cuajungco to look at 23 this. 24 Now there is stuff we're just starting to think

25 about as a result of some of the new work that's being 0069 1 done, but also some of the old work. We'd obviously like 2 to look at factors that interact with IKAP, specifically 3 also neural cells, because the JNK signaling kinase 4 pathway, and actually almost every signaling pathway, 5 shows some cell type specificity. So I work on NF-kappa 6 B. NF-kappa B in almost all cells protects from cell 7 death by any number of agents, but it turns out in neural 8 cells it actually sometimes promotes death. So there are 9 cell type specific effects even on the most common 10 signaling cascades that exist. So we really need to look 11 at the effect of IKAP in neural cell survival and 12 particularly the neural cells that we're dealing with 13 here. 14 We also would obviously like to look at yeast 15 model systems because they're easier to work with, and we 16 want to use both biochemical and genetic tests. There are 17 vectors, besides these new, fancy vectors that would allow 18 you to clone out within the space of a short time, that 19 have two tags on them that allow you to go from unpure to 20 a million-fold purification in basically a single step. 21 We could look at what are the factors 22 interacting with IKAP in multiple cell types, look in 23 specific cell types. There are new yeast methods. The 24 Elp1 is not lethal. But the question is could you make a 25 double mutant or find something that, instead of 0070 1 complementing the Elp1, would actually promote the disease 2 progression, promote the death of the cell. And that's a 3 very common way for looking at getting two members in the 4 same complex and that would allow you to maybe sort out 5 better what Elp1 IKAP is doing. 6 We'd like to look at the control of IKAP 7 expression because we'd like to see what the effects are 8 on the level of IKAP. What affects the level? Does it 9 get altered? 10 I have to say that I tried not to work on IKAP 11 now, but when it was first discovered that IKAP was 12 involved in FD, since I work on NF-kappa B, we quickly did 13 a few experiments. This is unpublished data that was done 14 by a former post doctoral fellow in my lab. This has been 15 done in vascular smooth muscle cells, which we work on. 16 It was also done in NIH toto3 cells. The result in the 17 red -- if you look at red staining, this is the result of 18 TNF-alpha treatment which is a stress response. What we 19 saw was in the absence of TNF, low levels, and in the 20 presence of TNF, much higher staining. 21 Originally we didn't do anything with this 22 because some of the original work implied that IKAP was 23 only in the cytoplasm, and we said, oh, we must have a 24 mistake here. We put it in the drawer and it wasn't until 25 the recent paper on JNK came out that I said, wait a 0071 1 minute, let's go back and take a look. So it is possible 2 that things can modulate and then affect the actual 3 response of the IKAP.

4 Not only do we want to look at level, but we 5 want to look at cellular localization. Does IKAP always 6 sit in the cytoplasm, or is there something that will 7 induce it? Maybe there's a combined stress response that 8 will move IKAP and the Elongator maybe more into the 9 nucleus where it might have more of a functional role in 10 controlling transcription. 11 There's obviously evidence for post- 12 transcriptional modification. There was worked that 13 Berish published originally that the point mutation 14 affects the phosphorylation of IKAP protein. But there's 15 also the data that just came out that JNK kinase 16 phosphorylates IKAP. How does this affect its functional 17 role? This could be a very critical issue. 18 And lastly, I just want to mention that there 19 are viruses that affect JNK kinase and signaling. We have 20 work that's totally unrelated to this. In fact, I never 21 work on JNK. I don't work on JNK, and then all of a 22 sudden, it's surrounding me. We work on cytomegalovirus. 23 There's a protein IE1 of cytomegalo which promotes growth, 24 vascular smooth muscle cells, and other cell types. It 25 turns out it induces JNK kinase. So do other viruses 0072 1 induce it? Rous sarcoma virus has been implicated. Does 2 that have some role in affecting the JNK kinase signaling 3 pathway? 4 Lastly and not least now, the question is what 5 are the effects of IKAP on stress responses in neural 6 cells and obviously then in vivo once the mouse models 7 become available. 8 Lastly, as I was talking to people here, some 9 people had seen the JNK kinase paper. Some people had 10 not, and I think that we need to have better 11 communication, at least as far as what's happening. I 12 think that the more rapidly things get communicated, the 13 better it's going to be. I was going to propose that I 14 would be happy to make an e-mail list. If we make e-mail 15 list, any paper that comes out can be circulated. If you 16 want to submit a preprint, you can decide. If you don't 17 want to submit it before it's accepted, fine. If you want 18 to submit it after it's accepted, fine. But if we make an 19 e-mail list, with a press of a button everybody is going 20 to have those papers. We could make a list. I'm happy to 21 put out a pad out in the hallway, and anybody who wants to 22 be on the e-mail list, let's make one so that everybody 23 gets the information as quickly as possible. The more 24 information passed, the better we're all going to be. 25 My only agenda in this is to help the kids. 0073 1 Many people don't know but actually my nephew has FD which 2 is the reason why I'm here and the fact that my sister- 3 in-law Jennifer is so persuasive. 4 (Laughter.) 5 DR. SONENSHEIN: And I'll stop there. Thank 6 you. 7 (Applause.) 8 DR. AXELROD: Thank you, Gail. I think really
9 the e-mail list is an excellent idea. I think if you put 10 a pad outside, I think a lot of people will put their e- 11 mail address on it. 12 Now we're all really waiting to hear the next 13 presenter, and that's going to be what is IKAP and 14 speculations on its role in development, maintenance, and 15 survival of autonomic and sensory neurons by Dr. 16 Svejstrup. 17 DR. GWINN-HARDY: Why don't we just take a 10- 18 minute break while we're setting up the computer because 19 there's no reason for you guys to sit in here while we're 20 doing this anyway, and a lot of people probably have to go 21 to the bathroom. But come back in 10 minutes. 22 (Recess.) 23 DR. GWINN-HARDY: I'd like to introduce our next 24 speaker who is Dr. Svejstrup, who is going to talk about 25 what is IKAP and speculations on its role in hte 0074 1 development, maintenance, and survival of autonomic and 2 sensory neurons. Dr. Svejstrup, thank you very much. 3 (Applause.) 4 DR. SVEJSTRUP: I think I'll get started. I too 5 would like to thank the organizers for this opportunity to 6 come and present some of our work to you today. 7 I want to start out by emphasizing that I am not 8 in any way an expert on familial dysautonomia. As a 9 matter of fact, just two years ago I had never heard about 10 FD before, and now as you've seen on some of the previous 11 slides, we are part of the important battle against this 12 disease in that we are trying our best to understand the 13 molecular function of the IKAP protein. 14 Our starting point into all this is not work 15 with patients. It's not even work in human or mammalian 16 cells, but actually in the lowly eukaryote Saccharomyces 17 cerevisiae, or baker's yeast, where we try to understand 18 how genes are regulated and transcribed with a mixture of 19 biochemical and genetic techniques. 20 During the course of our work in yeast, we have 21 realized that even though this is a low eukaryote, all the 22 major or the very important basic cellular processes that 23 govern the cell remain highly conserved in evolution and 24 that we can, therefore, actually very often learn quite a 25 bit about human disease by investigating life in yeast. 0075 1 This first slide shows you the focal point for 2 all work in my lab, namely, the elongating form of RNA 3 polymerase II which, of course as you all know, 4 transcribes all protein encoding genes in eukaryotes. We 5 are interested in the question of how this polymerase, as 6 it leaves the promoter and travels to coding regions, so 7 to say, deals with obstacles such as chromatin structure 8 and also DNA damages or DNA lesions such as those that are 9 produced by UV lights and therefore are a common feature 10 of all cells. 11 Now, in this talk today, I will not be talking 12 about DNA damage at all, but I will be talking about how 13 we think the IKAP protein has a connection to how

14 elongating polymerase might be able to deal with the 15 obstacle that chromatin is during transcription. 16 From the outset, we knew quite a bit about the 17 polymerase form, the form of RNA polymerase II, that is 18 involved in initiating the transcript. Because the 19 majority of research into regulation of gene transcription 20 is at this level, because the majority of regulation of 21 transcription is actually at the initiation level, we knew 22 quite a bit about the initiating polymerase and about the 23 basal factors that are required for it to recognize a 24 promoter and get transcription started. But we knew much, 25 much less about the polymerase form that is involved in 0076 1 elongation. 2 So basically that was our starting point. Are 3 there other factors that are specifically able to 4 associate with the polymerase when it is engaged in 5 transcription? 6 So what we did was to make simple biochemical 7 assay by which we caught in the act the polymerase as it 8 was transcribing DNA. I shall not bore you with all the 9 biochemical detail of how we did this, but just show you 10 the endpoint of this endeavor, namely the isolation of a 11 novel, very, very large protein complex containing RNA 12 polymerase II, here designated by its Rpb subunits, and a 13 number of novel proteins, only some of which we have so 14 far been able to isolate and identify by mass SPECT 15 analysis, a very powerful tool, by which you can basically 16 cut out the bands in a protein gel like this and identify 17 them. And because of all the genomes, not the least that 18 of yeast, have been fully sequenced, we immediately know 19 what the gene that encodes this protein is. 20 As you will see later, we've been able to now 21 identify all the six subunits of the human Elongator 22 complex and thereby the five proteins that interact in our 23 hands. The strongest were the IKAP protein. 24 So this basically is what we call the elongating 25 form of RNA polymerase II even though we have to admit 0077 1 that the definition is somewhat loose. 2 Now the p150, p90, and p60 subunits, which is 3 what we identified first, turned out to actually in 4 themselves form a complex that then interacts directly 5 with RNA polymerase II. And we now know that the 6 Elongator complex, which you've heard mentioned a few 7 times, actually is six subunits: Elp1, Elp2, Elp3, Elp4, 8 Elp5, and Elp6. And we can purify those from both yeast 9 and mammalian cells fairly rapidly because we developed 10 very powerful tools for this endeavor. 11 What do we know about these genes? Now I'm 12 confining myself to yeast. Well, of course, of interest 13 to this audience is the fact that Elp1, also called IKI3 14 is the yeast homologue of IKAP. But actually of most 15 importance for us in terms of our quest to understand how 16 polymerase deals with obstacles is defining at Elp3 -- 17 it's a very highly conserved -- you'll see that later -- 18 histone acetyltransferase. In other words, an enzyme that

19 modifies chromatin. So this, even though it is just a 20 working model, has led us to think that Elongator 21 associates with the elongating form of polymerase as it 22 travels chromatin and enables loosening of the chromatin 23 structure by acetylation of the tails of histones H3 and 24 H4. 25 As some of you may know, this is an area of very 0078 1 great interest to a lot of people right now, and we have 2 found that mutations in yeast which debilitate Elongator 3 function do, indeed, have a profound effect on the 4 transcribability of genes. It was proposed that we should 5 exchange papers, and will be happy to send interested 6 parties a paper which will appear in next month's 7 Molecular Cell about this issue. 8 Now, this is a working model. Of course, we 9 need to understand not only what Elongator does in yeast 10 but, more importantly, what Elongator might be doing in 11 mammalian cells. But let me just try to go through what 12 we know from yeast research about the Elongator complex. 13 We know, as I already told you, it was isolated 14 as a component of the elongating form of RNA polymerase II 15 and the integrity of this holoenzyme I showed you is 16 dependent upon a hyperphosphorylated CTD. So the RNA 17 polymerase II enzyme has a C terminal repeat domain, which 18 is hyperphosphorylated in the elongating form of the 19 enzyme but not in the initiating form. And our complex 20 specifically binds or preferentially binds to the form of 21 polymerase, the elongating form, that has a 22 hyperphosphorylated CTD. 23 The highly purified Elongator complex that I 24 just showed you binds to highly purified RNA polymerase 25 II. So it is a direct interaction in vitro. 0079 1 And in vivo, yeast strains lacking all the Elp 2 genes have similar phenotypes. So it is not so that we 3 think at least in yeast that Elp1 does a lot of things and 4 just one of the things it does is with the other Elongator 5 proteins. So we think that the activity, the role of the 6 IKAP protein is tightly coupled to the ability of Elp3 to 7 act as a histone acetyltransferase. 8 You already heard speculations about where is 9 Elongator. Of course, you need histone acetylation both 10 in the cytoplasm in order to enable assembly of chromatin 11 when the nucleosomes are transferred to the nucleus. But, 12 of course, you also need histone acetylation during 13 transcription because you need to have an open chromatin 14 structure that enables polymerases to travel through 15 chromatin and to associate with chromatin in the first 16 place. 17 In this respect, it is interesting that yeast 18 strains lacking Elp genes have a number of phenotypes, 19 many of which can be explained by defects in transcription 20 activations, and indeed Elp delete strains show slow 21 activation of some but not all regulated genes. So even 22 though we think that Elongator is quite generally involved 23 with RNA polymerase II, it clearly only affects a small

24 subset of genes and perhaps transcription of such genes, 25 when we think in mammalian cells, could be important for 0080 1 the development of FD. 2 Yeast Elp strains are sensitive to the 3 elongation-inhibitor 6-azauracil. So this is a trick that 4 yeast researchers use to try and assess whether certain 5 gene knock-out strains are likely to have a connection to 6 transcriptional elongation. Elongator delete strains are, 7 indeed -- at least some of them -- sensitive to 8 elongation-inhibitor 6-azauracil. 9 Now, it was already mentioned that we could do 10 genetic studies of Elongator, and actually that has been 11 done by quite a few researchers. It is very important in 12 this connection to mention that Elongator deletes 13 genetically interact with several transcription related 14 factors, such as CTK1 which is a kinase which specifically 15 phosphorylates RNA polymerase II. If you mutate CTK1 and 16 mutate Elp1, you die. Yeast cells cannot survive this. 17 If you mutate one of the nonessential polymerase subunits, 18 RPB9 and Elp1 or the yeast IKAP homologue, you die. If 19 you mutate the FCP1 gene, which encodes the phosphatase 20 that removes phosphorylation from the polymerase during 21 and after transcription, you also die. So these are clear 22 genetic evidences for a role of the Elongator complex and 23 thereby the IKAP homologue Elp1 in some sort of 24 transcriptional regulation or pathway. 25 Now, it's important, of course, to mention that 0081 1 Elongator does, indeed, have histone acetyltransferase 2 activity in vitro and that the main target is histone H3. 3 I'll show you more direct data on that later. 4 Elongator binds DNA and RNA in vitro. So 5 purified Elongator complex binds directly to DNA and RNA. 6 At least as a biochemist, this is very strong evidence 7 that it is relevant to look at what Elongator might be 8 doing in the nucleus. 9 And as mentioned already, Elongator is found 10 both in the nucleus and in the cytoplasm of cells, and 11 this is something that is very important for us to 12 understand. Our angle on this has been the role in the 13 nucleus, but of course this does not mean that the reason 14 why patients get familial dysautonomia cannot be because 15 of a separate role in the cytoplasm. This is just 16 important to keep in mind in that I am bias in what I tell 17 you now because what I'm interested in first and foremost, 18 in terms of my basic research, is of course what the 19 Elongator complex does in connection with transcription. 20 But of course, my interest in the familial 21 dysautonomia disease kind of broadens my view on what I 22 should study, and indeed we have started a number of 23 studies which will be addressing the potential role of 24 Elongator not only in the nucleus but also in the 25 cytoplasm. 0082 1 Now, this is just to remind me to tell you how 2 highly conserved the histone acetyltransferase Elp3 is.

3 This is an alignment of several versions of Elp3 from many 4 of the sequenced genomes that we have by now. Now, you 5 can't read this, and that's not the purpose. The purpose 6 is to show you all the red regions are identical amino 7 acid residues and all the yellow residues are similar. 8 And it is striking that Elp3 protein is more than 75 9 percent identical at the protein level from the lowly 10 yeast, the single cellular organism of yeast, to man. So 11 this is an unusually conserved histone acetyltransferase. 12 Now, using antibodies that we got from Claus 13 Scheidereit against the IKAP protein, very, very specific 14 antibodies, which recognize a little C terminal tip of the 15 protein, combined with antibodies against the human Elp3 16 protein that we raised ourselves, which is also very, very 17 specific, we simply followed Elp3 and IKAP protein during 18 a very long protocol of conventional purification, pouring 19 extracts onto columns and seeing where the proteins come 20 off. They usually always follow each other, but it is 21 important to point out that there are fractions containing 22 IKAP not containing Elp3. We're not sure how important 23 this is because we also know that the Elongator complex, 24 unfortunately, is quite fragile, and as soon as you 25 subject these complexes to purification, you are in 0083 1 another situation that you are in in the cell, and we 2 could, therefore, not be sure whether these fractions of 3 IKAP not containing Elp3 are actually relevant at all in 4 vivo or in the cell. 5 Now, the first thing we purified -- we did this 6 the brute force method. You see many, many columns of 7 purification and hundreds of liters of HeLa cells that we 8 grew to make this possible. We end up with a three 9 subunit complex, IKAP, human Elp2, and human Elp3. So 10 these are all homologues of the yeast proteins, Elp1, 11 Elp2, and Elp3. 12 Now, we knew from yeast that there had to be 13 more to the story than just Elp1, Elp2, and Elp3, and 14 knowing this, we went back and did a more careful study of 15 the Elongator complex using this IKAP antibody to do a 16 mild purification of Elongator. When we did that, we 17 actually found that just like in yeast holo-Elongator 18 complexes six subunits, IKAP, Elp1, Elp2, and Elp4. And 19 I'll show you that we now know the identity of p38 and 20 p30. 21 So, Elongator, six subunits in both yeast and 22 man, all are homologues. So this is very striking. It's 23 likely we can learn something from yeast in terms of what 24 human Elongator might be doing. 25 I should also mention that this human Elongator 0084 1 complex was purified from the nucleus. It was a nuclear 2 extract, but also that some recent results that I did not 3 want to bring here because I'm not sure about them yet 4 indicate that perhaps Elongator might be slightly 5 different in the cytoplasm than in the nucleus. So when 6 we do a very short purification procedure, which skips 7 some of these steps, but most importantly retains this

8 one, we get the six subunit complex from the nucleus, but 9 something quite different and potentially bigger from the 10 cytoplasm. We do not know the significance of this yet, 11 but this is something we are definitely addressing right 12 now. 13 Now, importantly, this holo-Elongator complex 14 that I showed you, the six subunit complex, but not core 15 Elongator, has histone acetyltransferase activity in 16 vitro. This is just a comparison of the activity of this 17 core complex with that of holo when we add radiolabeled 18 acetyl CoA to a reaction with the holoenzyme and purified 19 histones. We find that core enzyme has no HAT activity 20 whereas the holoenzyme, the six subunit complex, has HAT 21 activity directed against histone H3 and, to a much lesser 22 extent, histone H4. 23 This on the right here is just a control to show 24 that holo contains the Elp4, 5, and 6 protein, but core 25 does not. 0085 1 Now, when we did studies of where we can find 2 Elongator, that is, using the very specific IKAP antibody 3 and our very specific Elp3 antibody, we got a result which 4 is actually surprisingly dissimilar to what others have 5 reported. We found that in our hands the majority, as you 6 can see here, is clearly in the nucleus, whereas others 7 have found it predominantly to be cytoplasmic. But you 8 cannot see from our research that that's clearly a lot of 9 Elongator in our hands in the cytoplasm. It is an 10 important issue for us to understand why do we find 11 Elongator where we find it. Can it change localization 12 with stress signals, as has already been suggested? And 13 what is the role, if any, of Elongator in the cytoplasm 14 versus the nucleus? 15 So in terms of the human data which have been 16 derived by us and also by a study by Danny Reinberg and 17 his co-workers, human Elongator also binds directly to RNA 18 polymerase II in vitro, something found by both groups. 19 Very nice experiments by Reinberg and co-workers show that 20 HeLa nuclear extracts depleted for human Elongator can 21 transcribe naked DNA in vitro, but seems to be severely 22 impaired for transcription of chromatin templates, a very 23 strong indication in my opinion that there is some 24 connection, a direct biochemical connection, which of 25 course are the connections that I tend to believe the 0086 1 most, that Elongator is, indeed, involved in chromatin 2 transcription. 3 I also want to remind you that it's been shown 4 already by Scheidereit and co-workers and over-expression 5 of the IKAP protein abolishes transcription activation of 6 several genes in human cells, again indicating there's 7 some sort of role in transcription for this protein. As 8 has been pointed out several times also by me now, a 9 significant portion of Elongator is cytoplasmic found by 10 Reinberg and co-workers, and we also see a very 11 significant portion in the cytoplasm. So it's not only 12 Reinberg and co-workers.

13 And the mouse Elp2 protein StIP1 seems to be 14 translocated to the nucleus upon cell stimulation, which 15 is work by Schindler and co-workers a couple of years ago 16 published in PNAS, which I am sorry to miss out here. 17 Now, of course, one of the things that we were 18 given a grant to investigate was IKAP interaction 19 proteins. It's already in the database or in publications 20 at least what Elp2, Elp3, and Elp4 are, but also again, by 21 cutting out these bands and sending to them our 22 collaborator Paul Tempst to identify, we now know what 23 these proteins are. 24 So the identity of the human Elp5 gene is here. 25 This is the gene number that we found. We find virtually 0087 1 identical genes on chromosome 16 and 17, or we don't but 2 the Yeast Genome Project, of course, has done this for us. 3 So this is one thing that is so powerful about 4 biochemistry these days, and something that is often 5 overlooked. You think that the genome was for 6 geneticists, but it is actually also truly for biochemists 7 in that as soon as you identify a protein, you immediately 8 know where the gene is. You immediately know where the 9 gene is and whether there's a connection to human disease. 10 And I think that is something that I have not even had 11 time to look at yet, whether there might be some 12 connections between these gene regions and human disease. 13 And I'm sure that lots of people in the audience here are 14 probably better placed to do that than I am. 15 The Elp6 homologue, again the accession number 16 here, seems to be encoded by a single gene on chromosome 17 3. One thing I didn't point out is here's the homology 18 indicated to the yeast protein. All the red bars are 19 identical residues. All the yellow bars are similar 20 residues. So the homology of these proteins to the yeast 21 counterpart is visible but not compelling and therefore it 22 was only by doing the mass SPECT analysis that we dare 23 trust that this is, indeed, the homologue. We could not 24 find this by searching the genome with the yeast 25 sequences. We had to get hard core data. 0088 1 So the title of my talk, I should say, is not my 2 title because I do not really think I'm in a position to 3 speculate on the specific role of Elongator in the courses 4 and maintenance of FD symptoms. But I can, of course, 5 more broadly speculate about what I think IKAP and 6 Elongator might be doing, and I think it's implicit in 7 what I've been saying already what I think might be going 8 on. 9 It is, of course, important for us to discover. 10 This is indeed a major part of what we are trying to do 11 now in the human Elongator part of my work, and that is, 12 the question is whether FD is caused by its transcription 13 defects due to impaired Elongator function. One thing we 14 can do is to ask whether functional Elongator complex 15 actually assembles in cells which expresses the truncated 16 IKAP protein. And this is not easy because we rely on 17 cells from patients. So what we are doing right now is to

18 try and express truncated or FD-mimicked proteins which 19 has an epitope tag. So, we can actually pull out the 20 shorter version of the IKAP protein and see whether it 21 still interacts with Elp2, 3, 4, 5, and 6. And these 22 experiments are still in progress. 23 Of course, once we have pulled it out, if it is 24 there at all, we can ask the question of whether this 25 complex is functional. Does it bind DNA? Does it have 0089 1 histone acetyltransferase activity? Can it transcribe 2 chromatin in vitro? So very, very basic biochemical 3 techniques, which do not necessarily tell us what is the 4 cause of the disease but at least gives us some insight 5 into the function of the IKAP protein. 6 I should emphasize again that we have failed to 7 pull out IKAP with IKAP-specific antibodies without also 8 pulling out Elp3. So I want to emphasize that the role of 9 IKAP I think is tightly connected to that of the histone 10 acetyltransferase Elp3. 11 Now, this might prove that I don't know enough 12 about familial dysautonomia, but I was under the 13 impression that some of the patients do not have the 14 classical IKAP mutations. Of course, it would be very 15 important to discover whether such patients, if they exist 16 at all, actually carry mutations in the other Elongator 17 genes. It is actually puzzling that it is only mutations 18 in IKAP that give you these symptoms, this disease. 19 But I want to remind you that it might be 20 interesting to compare the symptoms in FD patients and 21 patients with transcription-related diseases such as 22 Cockayne's syndrome, which is due to mutation in a protein 23 which is also known to be involved in transcript 24 elongation. One of the important symptoms in Cockayne's 25 syndrome is actually also neurological disorders and the 0090 1 patients with Cockayne's syndrome also often suffer an 2 early death. So, again, I'm not a doctor and I can only 3 give you wild speculation, but some of you who know more 4 about symptoms and comparisons of them might want to look 5 into this possibility. 6 Of course, as I told you, we need to know 7 whether IKAP is also a component of other protein 8 complexes than Elongator. And if so, what is their 9 function and what are the subunits? This is something 10 we're actually pursuing as well. 11 Finally, I just need to acknowledge the people 12 who actually did the work I presented today. This was 13 mostly the work of a very talented post doc in my lab, 14 Nicola Hawkes, who is right now supported by the Familial 15 Dysautonomia Foundation, that is, the work on the human 16 Elongator complex. And this partly was started by Gabriel 17 Otero when he was a post doc in my lab several years ago. 18 I should also thank Paul Tempst's lab at Sloan- 19 Kettering who has been doing all the mass SPECT analysis 20 of the proteins we isolate, and Claus Scheidereit in 21 Berlin who has supplied us with a very, very good reagent, 22 the IKAP antibody, which unfortunately, in terms of FD, is

23 against a C terminus which, of course, does not exist in 24 the disease-causing protein. 25 And then I should also thank Michael Dahmus who 0091 1 helped us with some of the functional assays on human 2 Elongator. 3 Thank you very much for your attention. 4 (Applause.) 5 DR. AXELROD: Our next speaker is going to 6 address the question about secondary expressions of other 7 neurotransmitters. The title of the talk is secondary 8 neurotransmitter aberrations as demonstrated by 9 immunoreactive stains in dermal neurons, and it will be by 10 Dr. William Kennedy. 11 DR. KENNEDY: I'd like to express my 12 appreciation to Dr. Axelrod and to the foundation. 13 I'm going to report on a collaboration between 14 Drs. Hilz, Stemper, Axelrod, and myself in Minnesota with 15 Gwen Crabb, and Gwen did most of the work on this. 16 I'll first talk about the methods that we used 17 because they may be a little bit new, findings in FD, and 18 then as requested by the committee, an overview, trying to 19 fit this with other disorders and the general use. 20 The neurologists would call me an electrician. 21 I'm a neurophysiologist, and for many years I have looked 22 at pancreas transplant recipients. And I found that using 23 most of the tests that Dr. Hilz reported upon and 24 following pancreas recipients -- and these are diabetic 25 patients who are cured of their diabetes. It's no longer 0092 1 necessary to take insulin. I found that the patient was 2 better but my tests weren't, and this was very 3 frustrating. So I thought I must start looking at the 4 nerves themselves to see what they look like. This was 5 about 1990. 6 Fortunately at that time, three things were 7 happening. One, Thompson in England had shown us a 8 protein gene product 9.5 that is present in all central, 9 peripheral, and autonomic nerves. At the same time, the 10 confocal microscope was making its appearance, and I'll 11 talk more about that in a moment. And we were able to, on 12 the same selection of the same nerve, do double or triple 13 staining so we can look at several antigens. 14 Confocal microscopy is much like the CT of the 15 brain that you know so much about. One can take a thick 16 section of tissue and cut it -- optically section it, not 17 cut it. These are two micron slices. We take 16, 20. We 18 can take 50, and then you can page through these like 19 going through pages of a book and follow nerves and follow 20 their direction and their course. And you can look at 21 each individual one or you can put them all together, and 22 that's what we'll be doing today, looking at their 23 combined so-called Z series. 24 On each section, fortunately, there have been 25 different fluorfors brought forth, mainly by Jackson 0093 1 Immunonuclear Labs, and by using three individual spectrum

2 and separating them by filters, you can look at one, two 3 or three, combining each to different antibodies. So you 4 can do so-called triple staining and look at three 5 proteins in the very same nerve fiber in the very same 6 section. 7 This is just a quick orientation to skin. Not 8 all sections of skin look like this with all these 9 structures. This happens to have sweat glands, hair, a 10 large artery in it, and I'll talk in a moment quickly 11 about the nerves. This is an artery. The nerves here are 12 yellow or green. You see the arteries are almost covered 13 with vasomotor fibers and autonomic fibers. Two sweat 14 glands here. The sweat glands are not stained, but there 15 is so much nerve you can get an idea of the tubules of the 16 sweat gland. In addition to being stained for nerves, 17 this is stained for blood vessels. You'll see all the 18 capillaries. Blood does not have that many capillaries 19 ordinarily unless there are sweat glands in the section or 20 hair follicles. This has both. 21 Following up, this is a hair follicle. It's not 22 cut so you can see the nerves, but you see the outline of 23 a sebaceous gland, and hanging off the chin is the beard, 24 which is made up of nerve fibers and arrectores pilorum 25 muscle, which gives you goose bumps. We're from here on 0094 1 interested only in the epidermis which is up here. It 2 happens to be a diabetic patient so there are only two 3 little nerve fibers here, but we can see nerves in 4 epidermis better in this normal section. 5 This is the epidermis. This is the dermis. In 6 between, we've stained the basement membrane with collagen 7 IV, so this reddish thing here is a basement membrane. 8 It's a very thin layer. It looks thick there because this 9 is maybe 20 sections and you're looking at more of a 10 profile rather than on the edge. 11 The same collagen IV is in the basement membrane 12 around blood vessels. Here you can see the blood vessels. 13 Here are the nerves down here, nerve trunks. A nerve 14 trunk here goes up. It innervates sort of a segment of 15 skin. And fortunately for us for quantitation, the nerve 16 trunks branch into single nerve fibers just below the 17 basement membrane. For example, here you see a single 18 nerve fiber going up, another nerve fiber going up. So if 19 they're single, you can count them and therefore quantify 20 rather accurately. 21 And to give you an idea of the thickness of the 22 section, you see back in here? It's a dermal papillae 23 going up. This capillary will go up and end in a 24 capillary loop, but it's deep in the section so you can't 25 see it clearly. But we could thumb through it or page 0095 1 through it and see it very clearly. 2 Dr. Axelrod and her group sent me tissues from 3 10 subjects, mean age of 34. She had biopsied the calf 4 and the back. We had normal in our laboratory. We had 5 informed consent and IRB approval to do the work. 6 Quickly, these were 3 millimeter biopsies, about

7 an eighth of an inch in diameter, fixed, cryoprotected 8 section, and mounted and examined in the confocal 9 microscope. And this is a program by Michael Breakefield 10 to quantify those nerve fibers. 11 Here are two sections, normal and from an FD 12 patient. Again, you see the blood vessels and the nerves 13 in the epidermis. We're going to quantify these, but also 14 we're trying to quantify the nerves under the basement 15 membrane which you see here, and it's a nice capillary 16 loop. These are more difficult to quantify. 17 Normally these do not stain for substance P, 18 calcitonin gene-related peptide, or VIP. The first two 19 substances, P and CGRP, are often seen in this area in 20 normal skin. From an FD patient, you see quite a 21 difference. There's only one nerve fiber in the epidermis 22 as opposed to many. Very thin subepidermal neuroplexus, 23 which I may revert to call SNP. 24 We quantified in two ways. This is a very 25 simple way, but it's very effective. That is, the way we 0096 1 usually quantify anything in ordinary life: we call it 2 normal, which would be 0; mild, moderate, severe, 1, 2, 3; 3 or minus 4, there's nothing there. Absent. 4 This is the back and the calf. Let's look at 5 the calf first. 6 These are nerves in the epidermis. You see 7 almost all of them are minus 4. So there were no nerves, 8 very few nerves in the epidermis. Now these nerves are 9 nociceptors for mechanical pain, that is, pin, or for 10 noxious, heat pain such as touching a hot stove, and Dr. 11 Hilz tested for those. 12 Over here in the back -- and we chose back 13 because it's more proximal and most neuropathies are 14 distal, affect the distal extremities, mainly starting in 15 the feet. So we thought, okay, we'll go very proximal, 16 close to the spinal cord, but we were fooled in that those 17 are affected also. 18 We did that for diabetes too, and we were fooled 19 there also. They were affected. 20 And then we quantified in the same method the 21 subepidermal neuroplexus, and you see those are affected 22 rather severely too, not quite as bad as this. But if you 23 take the average, it's almost the same. Severe here too. 24 This would be moderate in our language, but pretty much 25 involved. 0097 1 I mentioned CGRP and substance P. Normally we 2 always see those. None, none, none. There's one fiber in 3 all 10 patients. 4 I mentioned in passing VIP, vasoactive 5 intestinal polypeptide. We never see that normally up in 6 the top of the skin near the epidermis or just under the 7 basement membrane, and we didn't see it in the calf. But 8 here it was present in all the patients. 9 Now, we've done regeneration patients mainly on 10 mice but also some in humans, and so has Story Landis, and 11 we find this if their nerves are regenerating. So this is

12 somewhat of a hopeful sign. We're not sure if those 13 nerves belong down where they're usually seen in sweat 14 glands and around blood vessels and are aberrant, are 15 someplace where they're not supposed to be, or if for some 16 reason, the neuron elaborates VIP for a short period of 17 time and we see it. So it may be a sign that there are 18 some efforts for regeneration. 19 I'll go through some slides of FD patients from 20 showing no nerves to a small innervation down here below 21 the basement membrane. A couple of nerve fibers. A few 22 more here. A little better. A couple fibers up here, but 23 a little more down here. Almost to normal except there's 24 a branch over here where there's not much. And absolutely 25 absent nerve fibers. So that's about the range we saw. 0098 1 We also quantified by counting the nerve fibers. 2 The normal in the back is much higher than in the calf, 70 3 versus 16, and this is per millimeter of epidermis. We 4 can also do it per area, so you can compare one lab to the 5 other. This is easier to present. 6 In the back, if you use this as the normal, this 7 was the best, less than a third of the normal. The rest 8 ranged down from there. 9 In the calf, this is normal. You see this is 10 the mean, less than one nerve fiber. So almost absent. 11 So the sensory tests Dr. Hilz was doing -- this 12 is one explanation why they're abnormal, at least in those 13 two areas. I assume in other areas too, though, we'd find 14 the same. 15 Another way to look at it, the normal range for 16 the back. By back, I mean T4-5, just off midline and 1 17 standard deviation on each side. And here are the 18 findings in the patients. This is a range for the normal 19 calf, and the findings in the patients. 20 Just something about VIP I mentioned. This is 21 one of the patients from the back that had some. If we do 22 look at the VIP, well, that stained different fibers plus 23 those that we saw. And if we look at double staining, you 24 can see these were not stained for VIP. These had both 25 VIP and PGP 9.5. So that's how you can see. We could do 0099 1 triple and show another substance in that nerve too. 2 This is another interesting fact. This is S100 3 antibody and it stains the Langerhans cells, but also it 4 stains the sheath cells, the Schwann cell sheaths here, 5 here, here, here, here. Now stains that just show the PGP 6 9.5, which is only in the axon, and we see they're here 7 too. But that nerve fiber does not show the axon. If we 8 do the double staining, well, we can see both here, here, 9 here. But this one just has the sheath. So it's an empty 10 Schwann cell sheath. And we saw this several times. So 11 there's some sign of progression. A Schwann cell sheath 12 will eventually disappear too, but much, much later after 13 the axon. 14 I put this in here because we saw this curious 15 excess of capillary loops. We're not sure what it means 16 and we didn't follow it up. We're not capillary people,

17 and we hope to find somebody to help us with this. 18 So in conclusion, in the FD patient, we saw the 19 epidermal nerve fibers decreased in density. Substance P 20 and CGRP loss was observed. VIP, usually absent, was up 21 near the epidermis. Empty Schwann cell sheaths suggest 22 some progression. Capillary abnormalities were observed. 23 We don't know what they mean. And FD patients, therefore, 24 have profound changes in the sensory innervation of the 25 skin. 0100 1 Myself and Gwen Crabb did most of this work and 2 a lot of people in the lab helped us, particularly Dr. 3 Selim, who is a post doc from Cairo. 4 Now, I was asked by the committee to look in a 5 more overview fashion. What I showed you were 6 unmyelinated nerve fibers, and I told you that we happened 7 in 1990 to be at the right place at the right time when 8 PGP became available, the confocal microscope became 9 available because neurologists, or anybody else, were not 10 able to see unmyelinated nerves very well before. In 11 fact, a very famous Mayo Clinic dermatologist said in 1988 12 that there's no good evidence that unmyelinated nerves 13 exist in human epidermis. And he was good at staining 14 skin. He was very good. He invented many silver stains. 15 So it wasn't him. It was the methods. So we're very 16 fortunate. 17 Now, unmyelinated nerves are the majority of 18 nerves in peripheral nerve, and they make up almost the 19 entire innervation to the autonomic nervous system. So 20 suddenly we're able to look at nerves that we couldn't see 21 before. It's like opening up the West to the settlers. 22 There will be a stampede to look at unmyelinated nerves in 23 other structures because that's the majority. 24 So the start was in skin, and I'll speak just a 25 little bit about skin on these unmyelinated nerve fibers 0101 1 that I've been showing you, these nociceptors to 2 epidermis. 3 Well, they're abnormal or missing in many places 4 where we'd expect them to be. We looked at FD, congenital 5 insensitivity to pain and hidrosis and some others where 6 we would expect them to be abnormal. Here's an entity, 7 patients that show up with burning feet. Neurological is 8 often normal. Sural nerve biopsy is sometimes normal. 9 Being smart, neurologists sent them to psychiatrists. 10 Well, they have severe abnormalities of unmyelinated 11 nerves, so this is a syndrome. It may be the most common 12 type of neuropathy. 13 We expected unmyelinated nerves in the epidermis 14 to be absent or reduced in diabetes, HIV, and leprosy, and 15 they've been shown to be so. 16 I'm not so sure we expected them to be reduced 17 in Friedreich's ataxia which involves the spinal cord and 18 the large nerve fibers. Maria Nalano in Napoli showed 19 that they're almost absent in Friedreich's. 20 Guillian Barre. Well, maybe they should be 21 involved, but I'm not so sure in these.
22 Here's spinal and bulbar muscular atrophy, which 23 I have a personal interest in. I've only looked at one 24 patient, but we'll look at more with the folks at NIH. 25 They were severely involved. That's a motor disease with 0102 1 some sensory conduction problems. It's not a sensory 2 disease. 3 Well, are these unmyelinated nerves some 4 surrogate messages of something is wrong with the nervous 5 system? Well, we'll go further. That is, what about 6 other organs? What about the gut? 7 We started with gut because of my interest in 8 the diabetic patients. Many of them have these same 9 complaints as normal people, but they're more severe. 10 We've been diagnosing those patients with autonomic 11 neuropathy for over 50 years, and it's a certain 12 diagnosis. We know they have it. We've never proven it 13 pathologically. We do it by tests that Dr. Hilz did, 14 sweat tests and other tests, which have never been 15 pathologically proven to have abnormalities. 16 This is a jejunum stained for nerves in the 17 green and blood vessels in the red. We'll look at one of 18 those. Here it is. And if we just look at the nerves, 19 you see it's loaded with nerve fibers. Here are the blood 20 vessels loaded with capillaries. Crypts down here. We 21 see a nice neural pattern around those crypts. We see 22 many nerve fibers. These are the enterocytes. So this is 23 the surface of the intestine. They're right under the 24 enterocytes, little nerve endings or naked endings. So 25 there's no apparatus there. So it's quite a complex 0103 1 situation. 2 Here's a mild and a severe from a diabetic and 3 the normal here. These villi are longer. They have 4 longer enterocytes, so there are more enterocytes so the 5 villi grow longer. This particular one looks rather full. 6 We didn't see many of those little endings I showed you. 7 It's maybe a little disorganized here, but I'm not good 8 enough to recognize that often. 9 But if you go a step further or maybe several 10 steps further to the advanced case, you see the nerves 11 don't reach the end. These villi are clumped together. 12 There are no enterocytes. I don't know if that's for real 13 or not. We don't know if it's due to the handling, the 14 processing, or whether the enterocytes are lost. If 15 they're lost, it's going to be difficult to absorb and 16 secrete from these villi. But the nerves are severely 17 abnormal. 18 So we have to worry about what does that do to 19 function. What does it to do stomach emptying which gives 20 those symptoms that I showed? About half the diabetics 21 have been shown to have delayed gastric emptying, and they 22 have feelings of fullness, early filling, et cetera. Is 23 that because they're functionally without a sensory supply 24 in the tips here? And I was talking about stomach, so in 25 a moment I'll look at stomach, but I wanted to look at 0104
1 cross section. 2 Here's a normal villi with a basement membrane 3 under enterocytes. The green and the yellow are nerves. 4 Many in here. You can see a large central vein and some 5 arterioles. The patients had arterioles, had a central 6 vein. There are no enterocytes, so they're clumped 7 together. They're much larger than this one and no 8 nerves. 9 This is stomach. Normal, somewhat different 10 because of different morphology, but the nerves go right 11 up to the surface. And here there are fewer nerves and 12 they've died back, so to speak. At least they're absent 13 up here. 14 So this is a method for early diagnosis. You 15 have to go down into the stomach to get that piece of 16 tissue, though. It may be related to the motility 17 problems. It opens a new field of neurological research 18 certainly. I think maybe, though, the skin nerves, the 19 epidermal nerves may be surrogates. It may be easier just 20 to take a biopsy of skin. In fact, we have another method 21 where we just make a blister and look at the nerves in the 22 skin. You don't even have a scar afterwards. 23 Well, where do we go next? Gall bladder, 24 pancreas, bladder? These haven't really been looked at. 25 And this is bladder. And we're not going to look at them 0105 1 today but just to give you an idea that they can be looked 2 at. 3 Well, what's the importance of all this to FD? 4 Well, diagnosis would be helpful I guess, but when a 5 treatment does come, how do we know it works? Even if we 6 can prevent the disease, there are a lot of people around 7 that have it, and it's too late to prevent it. We like to 8 know if they get better. So, we need clinical ways, 9 morphological ways to tell if the patient is better after 10 treatment. So maybe a skin biopsy or biopsy of the 11 intestine. Maybe bladder will help. 12 Thank you. 13 (Applause.) 14 DR. AXELROD: Thank you, Dr. Kennedy. 15 Now we're going to come to our final formal 16 presentation of the morning before we have our open 17 discussion, and this is going to be the construction of a 18 mouse model to study mechanisms of pathogenesis in 19 familial dysautonomia by Dr. Xu. 20 DR. XU: So I would also like to start by 21 thanking the organizer for the invitation. 22 I'm relatively new to the FD field. So this 23 meeting will be extremely educational on my part. 24 In my lab, one focus of my research is 25 constructing mouse models to study various human genetic 0106 1 diseases. In the past five or six years, we have 2 constructed a mouse model for ataxia telangiectasia and 3 more recently for MBS. These research experiments have 4 convinced me that a successful mouse model would be 5 critical to study the basis of defects in human genetic
6 disease. Especially exampled by the ATM-deficient mouse, 7 it has been used by a large number of groups now to study 8 the functions of ATM, as well as the basis of defects in 9 AT. 10 So, when the pathogenic disease mutation was 11 identified in FD, we decided to move into the research 12 area by constructing a mouse model to study the 13 pathogenesis in this disease, of course, with funding 14 provided by the FD Foundation. 15 So since construction of a mouse model is a 16 relatively time consuming process, the work is not 17 complete, so here I can only share some of the strategies 18 of how to do the mouse model in this case. 19 So we first have to clone out the mouse genomic 20 DNA of the IKB gene. Luckily for us, after we mapped and 21 screened the exons of the mouse gene -- and also published 22 by a number of groups -- the mouse IKB gene is highly 23 conserved to humans. Especially, lucky for us, the 24 genomic configuration of the mouse, the IKB gene is very 25 similar. It's completely conserved to humans. Like exon 0107 1 19, 20, and 21, their sequence is completely conserved. 2 Especially interesting in these studies is the splicing 3 donor sites for the exon 20 is also conserved. 4 So after we cloned the genomic piece, we 5 introduced a mutation. The first mutation we introduced 6 into the splicing site exon 20 and now we have also 7 introduced another mutation, the minor haplotype mutation 8 into the exon 19. 9 The gene construct of making mutations -- what 10 we need to do is basically insert a selection marker. In 11 this case it's PGK mu gene, recessant gene, into the 12 introns, between the exon 20 and 21, which is downstream 13 somewhere here. Also this selection marker is flanked by 14 log P site. 15 So we transfected the knock-in construct into 16 the ES cells, mouse embryonic stem cells, and ________ 17 combination between the flanking sequence. What we'll do 18 is replace the wild type exon, endogenous wild type exon 19 20, with the mutant exon containing the mutation in the 20 splice site. Of course, in this case the PGK mu gene is 21 also going to be introduced into the endogenous locus. 22 We know for a number of studies that PGK mu gene 23 by itself has a suppression effect on the transcription 24 through the locus, integrating. So I will have to get rid 25 of the PGK mu gene. In this case we can breed mice which 0108 1 carry these mutations with Cre transgenic mice that 2 expressed a Cre gene in a germline, and eventually we'll 3 delete the log P site, leaving only the PGK mu gene and 4 recombining the log P site in the intron 21. 5 Of course, we know that log P site by itself 6 doesn't really have any effect in the transcriptional 7 suppression or activation. So it wouldn't affect the 8 expression of the mutant knock-in allele. 9 So our work now has progressed to this level. 10 The most time consuming stage of the project is to

11 construct the mice. We already have the mutant ES cells. 12 So just based on my very limited understanding 13 of FD, so when we get the mouse, we'll be able to address 14 a number of very obvious questions to test whether this 15 mouse indeed can be used as a mouse model for FD disease. 16 Here, as a number of speakers have mentioned, 17 the splice mutant might affect IKB splicing in a tissue- 18 specific manner. So this can be very easily tested also 19 in the mouse model. 20 Of course, with the mouse, in collaboration with 21 people here, we can have a very comprehensive analysis of 22 the different tissues for the defects observed in FD. 23 So I will conclude by thanking the foundation 24 for funding, as well as the two persons in the lab now 25 that are focusing on this project. Thanks. 0109 1 (Applause.) 2 DR. AXELROD: I'd like to thank all my speakers 3 this morning, and now I'd like to invite them all to come 4 up and sit at the table. We'll have to add about three 5 more chairs to this table. I'll invite our moderator, Dr. 6 Rubin to come up and moderate an open discussion. I hope 7 you're all stimulated to ask lots of questions, and we'll 8 try to answer them. 9 Dr. Rubin? 10 DR. RUBIN: I guess everybody has settled in. I 11 have the easy job as serving as moderator. I wanted to 12 thank the organizers for making it possible for me to be 13 here, and I wanted to thank FD Hope for supporting the 14 research in our laboratory and for their efforts to ensure 15 my presence here at this meeting today. 16 If you have questions -- and I'm sure there will 17 be many -- if I could ask if you would move to the 18 microphone so that people can hear the questions 19 throughout the audience, that would be helpful. Go ahead. 20 DR. HIRSCHHORN: We've had a lot of talks and 21 couldn't ask questions in between, so I've got a few 22 comments and questions. I'm Kurt Hirschhorn, by the way. 23 And they're addressed to three, perhaps four people. 24 The first is really sort of a suggestion for Sue 25 in terms of the tissue culture question that you're 0110 1 asking. What's happening in the tissue culture? 2 Many years ago, several labs, including ours, 3 showed changes in activity of specific enzymes involved in 4 in-borne errors in the carriers for those, but also to 5 some extent in the affecteds, during stimulation of 6 lymphocytes by PHA. The first of these actually was ours 7 with alpha-glucosidase. The second was by Joe Goldstein 8 with S-methionine synthase, and the third was by my wife 9 Rochelle with adenosine deaminase. I would suggest that 10 you might try to see what happens to try to explain the 11 differences between the various labs in terms of what you 12 consider in the log phase versus stationary phase to see 13 what happens to these resting lymphocytes when you 14 stimulate them with PHA and they go into a log phase. 15 That's the first thing.
16 The second is a comment about something that was 17 said by Felicia and actually by a couple of other people 18 too who said, well, it's very important to look at the 19 proteins and genes affected by IKAP and perhaps its 20 changes because this could explain a lot of the things. 21 Well, one of the things that will be going on 22 with an enormously exponential increase over the next few 23 years is the search for modifier genes. There is no such 24 thing as a mendelian disease anymore. They all are going 25 to vary. They're all going to be varied by mutations, 0111 1 variations, and so on and a whole host of other genes that 2 are going to affect the expression of the particular gene 3 that we're talking about. 4 So the search perhaps should not only be for 5 those proteins and those genes that are downstream from 6 IKAP, but much more important perhaps, by things that are 7 upstream from IKAP that might affect the activity of IKAP 8 and even possibly its splicing. 9 With that in mind, Dr. Svejstrup, I have a 10 question regarding the transcription factors. One of the 11 transcription factors that seems to be necessary in terms 12 of its activity before histone acetylation is the whole 13 SWI-NEF complex which opens chromatin. And that was 14 first, of course, described in yeast. And I'm wondering 15 whether you have any idea of an interaction between this 16 and the Elongator situation. 17 DR. SVEJSTRUP: We have looked for such evidence 18 both biochemically and genetically, and one thing that 19 should be mentioned about the SWI-NEF complex is that that 20 started out as a nice single model. It has now become so 21 varied that there are so many of these complexes that 22 studying this is a major endeavor. There are so many 23 possibilities. But we are trying, but we have yet to find 24 any genetic or biochemical interactions. We know better 25 now where to look, so I think our studies will be more 0112 1 directed in this direction because is obvious to look for 2 interactions between Elongator complex and such other 3 chromatin binding complexes. 4 We know there's a very strong functional overlap 5 between the Elongator complex and the classical 6 transcription with histone acetyltransferase called GCN5 7 which is the first one to really be discovered as a 8 histone acetyltransferase that is involved in 9 transcription. If you mutate both GCN5 and Elp3 at the 10 same time, actually just point-mutate them so that they no 11 longer function as HATs, then yeast cells are very, very 12 sick. 13 The study that's coming out soon and which, as I 14 said, I'll be happy to make available now is showing that 15 these cells have a very severe defect in acetylation of 16 the whole genome, and that this leads to consequences for 17 the transcription of several genes which become 18 hypoacetylated, specifically in the coding region, and are 19 lowly transcribed. 20 So, I think in terms of all the very nice cell

21 biology that has been done on FD, it would be interesting 22 to try and investigate acetylation levels in chromatin and 23 perhaps in cytoplasm as well of FD patient cells. They're 24 a very powerful tool for this, and I think time is right 25 to do these kinds of experiments. 0113 1 DR. HIRSCHHORN: Thank you very much. 2 Sort of as a last comment, I'm hoping that our 3 moderator will address some of what he might be doing in 4 relation to clarifying the differences between the two 5 original -- 6 DR. RUBIN: Go ahead. 7 DR. HARDY: John Hardy, National Institute on 8 Aging. 9 I'd like to ask Dr. Svejstrup if the exon 19 10 mutation is conserved. Well, of course, the original 11 minor ________ is conserved in yeast, and if there have 12 been any attempts to just putting that mutation into the 13 yeast gene to see what the effects of that mutation are on 14 the complex and so on. 15 DR. SVEJSTRUP: This is a very good experiment. 16 So, first of all, Saccharomyces do not have very much 17 splicing. 18 DR. HARDY: Sure, yes. 19 DR. SVEJSTRUP: So there is no splice donor and 20 acceptor in that region. It's just a contiguous gene. 21 But we have tried to make the mutation, and I 22 have to say for reasons that are beyond me -- and we're 23 looking into this right now because it was published last 24 week by another group that when they do a C terminal 25 truncation of Elp1, they see phenotypes that are 0114 1 consistent with the failure of Elongator to function. So 2 this is consistent with a role for the C terminus in 3 normal Elongator functioning, also in yeast. 4 We did this mutation as soon as heard about the 5 IKAP results, and we have not seen this. But we not have 6 looked at the right phenotype, and it would be interesting 7 if there's one phenotype that is affected by this mutation 8 and others that are not. It would actually be the first 9 time for us to have a separation of function mutation in 10 any of the Elongator genes because no matter which one you 11 knock out, you get exactly the same phenotype. So this 12 would be very important. 13 DR. HARDY: Isn't the minor mutation a missense 14 mutation? That might be a better one to try in a sense. 15 It's a more selective effect perhaps. 16 DR. SVEJSTRUP: It's a phosphorylation site 17 mutation, as I remember it, and that phosphorylation site 18 does not seem, as I recall it again, to be conserved in 19 yeast. 20 DR. KALLUNKI: Hi. My name is Tuula Kallunki 21 and I'm the senior author of this paper that Dr. 22 Sonenshein mentioned in her talk. First of all, I would 23 like to answer her question, and then I have a couple of 24 questions for you. 25 She wanted to know why there was not a total

0115 1 overlap between JNK and IKAP in this immunocytochemical 2 picture that we showed in the paper. And my answer for 3 this is that we had a technical problem there because the 4 antibody that is normally used to detect JNK in 5 immunocytochemistry does not work under conditions that 6 the IKAP antibody works. So then by post doc Christian 7 tested another antibody which doesn't give as nice a 8 staining. But if you look at the papers where people show 9 JNK staining with this antibody that is normally used, 10 it's much more similar to IKAP staining. 11 I have one question for Dr. Slaugenhaupt. I 12 would be interested to know, because it wasn't clear to me 13 from this talk, what about the carriers? Do they also 14 express mutated IKAP or not? 15 DR. SLAUGENHAUPT: Yes, they do. When we look 16 at the message levels, we can see a very faint band of the 17 mutated, as you would expect. 18 DR. KALLUNKI: Okay, but there's absolutely no 19 phenotype. Right? 20 DR. SLAUGENHAUPT: As far as I know from 21 discussing with the clinicians. That might be better 22 directed at Felicia to address phenotype in carriers, but 23 as far as I know right now, there's none. 24 DR. AXELROD: The carriers manifest no sign of 25 the phenotype at all. 0116 1 DR. KALLUNKI: Okay. Do you think it's kind of 2 a dose effect? 3 DR. SLAUGENHAUPT: Exactly, a threshold effect 4 is our guess. 5 DR. KALLUNKI: I also have a question for Dr. 6 Svejstrup. My first question for him actually was about 7 reconstitution of the holo-Elongator with this mutant 8 IKAP, but that was part of the question of the previous 9 person. 10 But then also I would like to know if you have 11 any experiments underway or if you're planning to do 12 anything on studying the possible role of IKAP in stress 13 response. 14 DR. SVEJSTRUP: First of all, I should say I 15 have only one post doc working on this issue in human 16 cells. We do other studies in human cells, most notably 17 on the Cockayne's syndrome. That's why I mentioned this 18 as a possible interesting correlative. But most of our 19 work is in yeast, and we simply do not have hands enough 20 to do all the things we'd like to do. 21 I am actually trying to recruit post doc 22 students. If any of you here are people who are 23 interested in studying FD, please send them my way if they 24 want to do biochemistry. 25 We have no plans of studying stress responses 0117 1 because we do not have the right tools to do so. We will 2 focus on purely biochemical experiments and try to figure 3 out what Elongator complexes from IKAP patients, albeit 4 artificial IKAP patients, if you know what I mean, by

5 expressing mutated versions of IKAP, how they behave in 6 our biochemical assays basically. 7 I should comment because you asked about the 8 integrity of the Elongator complex in IKAP patients. We 9 don't know about in the patients or even in mammalian 10 cells, but we do know that if we express the truncated 11 Elp1 protein that mimics the IKAP mutation, we still have 12 Elongator complex. So it doesn't seem to completely fall 13 apart, but this, of course, does not argue that it is not 14 unstable and therefore useless. But we can in IP, 15 immunoprecipitation, pull down Elp3 and we can detect this 16 truncated message. So it is not in itself inherently 17 unstable, it seems. But much more work needs to be done 18 before we understand. 19 DR. KALLUNKI: Thank you very much. 20 DR. MAAYAN: Channa Maayan from Hadassah, 21 Jerusalem. I have two comments and one question. 22 One comment is for Dr. Kennedy. We have just 23 concluded the study on the innervation of the 24 gastrointestinal tract, especially the small intestine, 25 and we also saw an increase of density of the innervation 0118 1 and especially the NOS activity. 2 Another comment is for Dr. Hilz. Among other 3 factors that affect instability during sleep is definitely 4 the decreased lung volume that they have because of 5 scoliosis. This definitely will increase the instability 6 during sleep. 7 The other question is also for Dr. Hilz. Many 8 years ago, we saw an increase of the parasympathetic heart 9 rate variability, especially in the high frequency band, 10 when they went from supine to standing. You showed that 11 there is a decrease of the baroreceptor especially in the 12 high frequency band. How do you explain the difference? 13 DR. HILZ: Did I correctly understand you that 14 you said you saw an increase of the parasympathetic during 15 standing up? I think I'm aware of that paper on the 16 baroreflex function. 17 I don't have a good explanation for that because 18 when we did selective -- I mean, we analyzed, as I showed 19 in one of the slides, the heart rate variability in the 20 supine and standing positions and we didn't see any major 21 change. However, when we did selective stimulation with 22 the sinusoidal stimulation where you can really separate 23 sympathetic and parasympathetic responses, again we didn't 24 see a response. 25 Perhaps there are differences between individual 0119 1 patients. Dr. Axelrod always pointed out that there is 2 quite some heterogeneity in the clinic in manifestations. 3 So that would be my own explanation. 4 From those two studies, we did not see an 5 increase of parasympathetic response, not even in the 6 sense that when you look at the cardiovagal balance and 7 the comparison of low and high frequency activities, that 8 there is enhanced parasympathetic activity because there 9 is a withdrawal of sympathetic response. So I have no

10 clear cut answer. 11 And the other comment. Of course, reduction of 12 lung volume due to the orthopedic problems just adds to 13 the risk of the patients, particularly at night. So I 14 fully agree with that. 15 DR. HARDY: John Hardy, NIA, again. 16 My apologies. This might have been dealt with. 17 I missed the first hour. But is my understanding correct 18 that there has just been found two mutations so far in 19 this disease, or have others been found as well? And if 20 only two have been found, have other populations been 21 looked at for the occurrence of FD? 22 DR. RUBIN: Dr. Slaugenhaupt, would you take 23 that question? 24 DR. SLAUGENHAUPT: To date we've only identified 25 two mutations in the Ashkenazi Jewish population. Clearly 0120 1 there have been, for many years, reports in the literature 2 of patients with FD that don't have Jewish ancestry and 3 other FD-like syndromes. Jesper actually touched on this. 4 We are starting to look at these patients to see if they 5 might have other IKAP mutations, and there's also the 6 possibility that these related disorders may be due to 7 mutations in the other Elongator complex members. So only 8 two mutations and we don't really know the answer to the 9 second question yet. 10 DR. RUBIN: Let me just follow up on that. I 11 seem to recall the paper that was published by yourself 12 and others that reflected on a non-Jewish person who had 13 -- I'm sorry -- a child born to a Jewish mother or Jewish 14 father. Only one was Jewish and the child had one of the 15 mutations. Can you elaborate on that? 16 DR. SLAUGENHAUPT: That was a haplotype paper 17 that we published a couple years ago, and in fact, there 18 is a patient that is heterozygous for the major FD 19 mutation and we have not yet identified the mutation, if 20 there is a mutation, on the other strand in that patient. 21 DR. RUBIN: So there may very well be other 22 mutations in other populations. 23 DR. HARDY: Thank you. 24 DR. RUBIN: Go ahead. 25 DR. GROSS: Hi. My name is Bob Gross. I have a 0121 1 question for Dr. Svejstrup. 2 On your slides with the staining for the IKAP, 3 you showed a lot of cytoplasmic staining in sort of a 4 punctate pattern. Have you looked in the electron 5 microscope or other ways to see what that is associated 6 with? 7 And then a question for everybody I guess is, if 8 there is a lot of cytoplasmic localization, has anybody 9 thought of a function or begun to look at a potential 10 function for IKAP as part of some other complex perhaps in 11 the cytoplasm? 12 DR. SVEJSTRUP: As I mentioned, in terms of 13 cytoplasmic function, what we can do is to try to isolate 14 these proteins and try to understand where they interact.
15 We have, as of just last week, identified with these very 16 powerful anti-IKAP antibodies the six subunit complex, and 17 we started from the nucleus. But something that seems to 18 be much more complicated and much more subunits is from 19 the cytoplasm. So that's our way of addressing this. 20 One obvious thing to look for with an antibody 21 is with a JNK kinase, for example, comes down with these 22 immunoprecipitates even though they are much more than 23 that because they're actually highly purified when we get 24 to this point. 25 So what I have learned from doing it this way is 0122 1 that very often we get very good clues to function by 2 finding the proteins because if we find a JNK kinase, we 3 find kinase in a signaling cascade, we are in the 4 direction of, yes, that is what is wrong perhaps if it is 5 in the cytoplasm, the IKAP phenotypes originate. 6 But, of course, my own bias here is that I 7 didn't start studying this because of familial 8 dysautonomia. I want to contribute to solving what is 9 going on, but our own bias is on things that go on in the 10 nucleus. Of course, for us it is important to show that 11 indeed what Elongator is doing in the nucleus is relevant, 12 and that has been a great deal of our emphasis. Again, a 13 lack of hands is a problem in many labs, and not least in 14 mine. 15 DR. HUANG: Just a quick comment about the 16 phenotype in both human and the anticipation of the 17 phenotype in mouse. 18 Oh, by the way, I'm Eric Huang from UC-San 19 Francisco. First, I want to thank the foundation for 20 funding future research analyzing the mutation. 21 But I want to point out the striking similarity 22 in the neurological deficit in humans compared with a 23 mouse with various neurotropin knock-outs and 24 transcription knock-out where you see almost more than 80 25 percent of neuronal loss in the sensory nervous system, as 0123 1 well as the sympathetic nervous system. 2 So, for example, the congenital insensitivity to 3 pain in humans has been shown to be a mutation in trkA. 4 So that kind of supports a survival pathway. In the 5 absence of trkA, there's severe cell loss during 6 embryogenesis. 7 Looking forward, in terms of analyzing the IKAP 8 mutant, I anticipate that this will be a severe mutation 9 which will -- in the mouse mutation, it will lead to 10 embryonic ________. And so that calls for the analysis 11 using a conditional approach. 12 Also kind of to bring on the perspective in 13 looking for therapeutic means, because looking at these 14 mouse mutant neurotropin mutation where a gene has been 15 knocked out, it's very clear that the neuronal loss 16 happened really early during embryogenesis. So in terms 17 of therapeutics in adult or in postnatal life, perhaps the 18 best way is to look for regeneration rather than 19 therapeutics because there's no neuron to rescue anyway.

20 That's just my personal perspective. 21 DR. AXELROD: I think you bring up a very good 22 point in terms of the neuronal loss being early in utero, 23 and we've shown that even at birth these children 24 obviously have terrible problems. 25 But I think if we also try to avoid the 0124 1 progression or the progressive loss, if we can enhance 2 survival of what they have at birth -- because we really 3 do very well with the patients until about the teen years, 4 the adolescent years. We improve their tone and we give 5 them therapy. We can compensate. But then no matter what 6 we do, it seems that in the adult years that progression 7 takes place. So if we can prevent that, that would be 8 wonderful. 9 DR. RUBIN: Go ahead. 10 DR. LACHTER: Jesse Lachter from Haifa, Israel. 11 I'm a gastroenterologist. 12 The first question is for Dr. Kennedy about 13 progression which was very interesting, and you showed an 14 empty Schwann cell. But as Dr. Axelrod mentioned, maybe 15 things are present very early on. Was there a simple 16 progression of the age of the patients? You had 17 relatively older patients. I think you had a mean of 18 about age 34. But you had a span there. As the patients 19 got older, did you see something? 20 And the second short question for you is do you 21 need only fresh samples or can you take cell blocks? 22 And my question for Dr. Slaugenhaupt was that 23 various tissues were tested for the mutant versus wild 24 type, but I think you didn't mention GI tissues among many 25 of the different samples which you took from different 0125 1 parts of the body. And I would be very interested in 2 finding out if that was done. 3 And last, I would just mention as a comment, 4 because this is such a great meeting, that some kind of 5 focus groups or break-out groups for clinicians at the 6 next meeting -- I hope it will be only a year from now. 7 Maybe it will be two years from now that the NIH can put 8 together a group like this so there could be focus groups 9 for clinicians in the various areas. We had one a couple 10 of years ago at an AGA and different things like that, but 11 putting these minds together would be very helpful that 12 way too. 13 DR. RUBIN: Thank you. 14 Dr. Kennedy. 15 DR. KENNEDY: I can't tell you today which 16 patients showed the empty Schwann cell sheaths, so I can't 17 tell you the ages. We could easily do that by sorting 18 through. I think it's a little stretched to say that that 19 proves that there's progression. I don't know if it does. 20 As far as your second question, a month ago I 21 would have said no, but the answer today is yes. One of 22 the pathology residents has had the same question about 23 Hirschsprung's disease, and she said, I don't have any 24 fresh patients, but I have a lot of tissue banked away.

25 So we've been able to deparaffinize and react with protein 0126 1 gene product 9.5 and other antibodies and shown beautiful 2 staining. So suddenly all the tissue banked in all the 3 hospitals of the world may become available, and that's 4 kind of an exciting development. 5 DR. RUBIN: Sue, did you want to answer that 6 other question? 7 DR. SLAUGENHAUPT: Yes. I don't remember off 8 the top of my head all the tissues that I had on the 9 slide. I know we've looked at esophagus. I don't know 10 that we got a sample of the stomach or not. 11 But there's one thing I want to point out about 12 that study and that is that certainly the FD tissue is 13 very scarce and all of those samples came from FD 14 postmortem tissues that we obtained from either NYU or the 15 Brain Bank in Miami and, therefore, certainly don't 16 represent I think what's going on necessarily. We have 17 not surveyed many different sections from different 18 patients to see what's going on. 19 So although I think that our conclusions that 20 clearly splicing is worse in neuronal tissue are valid. 21 Whether there's more in the heart or less in the heart, 22 exactly looking at what's going on, we would have to look 23 at many different heart samples, for example, from 24 different patients before we can conclusively say exactly 25 what's going on in the different tissues. 0127 1 DR. LACHTER: There is a bank of GI tissue, yes. 2 DR. SLAUGENHAUPT: FD? 3 DR. LACHTER: All those patients were scoped and 4 biopsied and then operated. 5 DR. SLAUGENHAUPT: So that's something we could 6 definitely look at then. Thank you. 7 DR. RUBIN: Go ahead. 8 DR. PELTZER: Hello. I'm Sonia Peltzer. I'm 9 President of FD Hope, a parent of two children with FD. 10 Actually I first want to make a comment, and 11 that's with regard to whether or not carrier status does 12 impose any symptomatology. Whereas I clearly think that 13 the phenotype of a carrier is vastly different than the 14 phenotype of an affected individual, I think the verdict 15 is still out whether or not there is some evidence of 16 disease. 17 Dr. Maayan had written a paper several years ago 18 about the incidence of varicella and that because of the 19 decreased number of neurons, you have decreased risk for 20 varicella infection in affected individuals. There was a 21 very casual survey done of approximately 40 carriers also 22 several years ago. It was never published, did not do any 23 matched control comparisons. But there seems to be a 24 decreased risk for varicella infection among carriers as 25 well or perhaps delayed onset of infection. You would 0128 1 expect it in younger years, and these individuals were 2 either adults or much later in life. So it would follow 3 that perhaps doing the same skin biopsies that Dr. Kennedy
4 has done on carriers might be able to provide that answer 5 for you to see if there is some evidence of disease in 6 carriers. 7 My question is actually for Dr. Axelrod. I've 8 heard the statistics. Let me first preface this by saying 9 we all are aware you can interpret statistics in different 10 ways. I've heard the statistic that 50 percent of 11 patients will reach age 40, and I'd like to get an 12 understanding of where that number is coming from. 13 DR. AXELROD: That's the result of a combined 14 study that Dr. Channa Maayan and I did based on data from 15 the Dysautonomia Center because we combine our data. It's 16 going to be coming out in this month's Journal of 17 Pediatrics. 18 DR. PELTZER: How did that statistic derive? 19 Did you look at a cohort that was born 50 years ago and 20 determine that 50 have survived to age 40? 21 DR. AXELROD: These are probability of survival. 22 It was done with a group of statisticians and based on 23 births, deaths. It was subjected to statistical analysis. 24 DR. PELTZER: We've done a little bit more of a 25 different interpretation of probably the same data. 0129 1 Again, with stats, you can look at things very 2 differently. But looking at a sample of approximately a 3 third of the patients, which we've had access to, and 4 their deaths over a period of three years, it seems that 5 50 percent do not survive to 30 if you take the different 6 age groups and add them up. The bottom line I think we 7 can all share is that this is a devastating disease. 8 DR. AXELROD: Yes, but I think one also has to 9 be very careful how one obtains data and that there is no 10 bias in obtaining the data and that the number of 11 individuals that you're talking about, when you look at 12 data from 580 patients, and if you looked at 30 patients 13 or 40 patients in the last three years, the last three 14 years are not the history of -- 15 DR. PELTZER: We looked at 150. 16 DR. AXELROD: Well, I'm not going to -- 17 DR. PELTZER: Right. I'm saying I think we have 18 that agreement. I'll be interested in seeing how that 19 statistic was derived. Thank you. 20 DR. RUBIN: Actually I had that question on my 21 list because there were 580 patients. 60 percent are 22 surviving according to the report that you put up there 23 today. 50 percent of them -- and I don't know how to 24 interpret it as well -- reached the age of 40 or I guess 25 have the potential. Can you just tell us how many 0130 1 patients there are of the 580 that are over 40? 2 DR. AXELROD: I can't give you the exact number, 3 but the present statistic was -- I had said 35 percent 4 were greater than 20 years of age at the present time. I 5 can't give you the actual number at this time. You can 6 look at the paper. The paper will be out in the Journal 7 of Pediatrics this month. 8 DR. GUSELLA: Jim Gusella, Mass General.

9 I'd like to go back to biochemistry and ask 10 Jesper a more general question which relates somewhat to 11 what Kurt was asking, and that is, to what degree have 12 histone acetylases been looked at to see what targets they 13 have in the cytoplasm and whether they have specific 14 acetylation targets or not. 15 DR. SVEJSTRUP: This is actually a surprisingly 16 under-developed area. We do know some cytoplasmic HATs, 17 and the definition is basically biochemical. A 18 cytoplasmic HAT is a histone acetyltransferase that will 19 hit core histones but not histones packed into DNA. And 20 our HAT will hit histones not packed into DNA and histones 21 packed into DNA. So per definition, we are working with a 22 type B HAT because we can do both, whereas the typical 23 cytoplasmic HATs will only hit free histones. 24 So we don't know very much about histone 25 acetylation in the cytoplasm except that we know that 0131 1 histone proteins are assembled with chromatin assembly 2 factors in the cytoplasm and can be purified as such as a 3 component of chromatin assembly factors. And those 4 histones are always acetylated on certain residues. So we 5 do know quite a bit about the positions of acetylation 6 which are important for assembling chromatin. But in my 7 opinion, there's nothing wrong with being a HAT in the 8 cytoplasm and being a HAT in the nucleus at the same time 9 and play a role in both things. 10 What surprises me about Elongator is that if it 11 played an important role in being a HAT in the cytoplasm, 12 you would expect it to have genetic phenotypes when you 13 combine it with a mutation, when you remove their other 14 cytoplasmic HATs, and then you will be relying much more 15 on Elongator. Yet, we do not have synthetic phenotypes. 16 We do not have a more activated phenotype of an Elp3 HAT 17 1W which is the cytoplasmic HAT. Whereas, as soon as we 18 start combining with the nuclear HATs, we get a very 19 severe phenotype, indicating the important function of 20 Elongator is in the nucleus so that when you remove two, 21 you have a problem. But when we remove just one HAT, you 22 don't. But again, these things are not absolute. 23 DR. GUSELLA: And were the experiments that were 24 done to show that the histone acetylases worked on the 25 histone present in the cytoplasm done in such a way that 0132 1 they excluded the idea that these proteins could acetylate 2 non-histone proteins? 3 DR. SVEJSTRUP: Not at all, and many of these 4 histone acetyltransferases have many targets. So we have 5 genetic and biochemical evidence that Elongator, as one of 6 its targets, has histones, but it could well hit other 7 things as well. 8 DR. BROWNSTEIN: Mike Brownstein, NIH. 9 Felicia, I have a question for you about samples 10 that have been collected and studied over the years. Has 11 anyone done an extensive survey of CNS neuropathology in 12 the brain samples of these patients? Because if the 13 splicing is abnormal throughout the nervous system, I

14 guess you'd expect to see more neuronal loss than just 15 neurons in sensory and sympathetic ganglia. 16 DR. AXELROD: Dr. Zagzag, I'm going to allow you 17 to answer that. Okay? I know that when Dr. Pearson was 18 here -- he left a while ago and he was having difficulty 19 approaching the brain just because of the mass and the 20 technology not available at that time. 21 DR. ZAGZAG: The answer to your question is Dr. 22 Pearson primarily focused on the peripheral nervous 23 system, and to the best of my knowledge, the 24 neuropathology for examination of the central nervous 25 system is basically undone. 0133 1 DR. RUBIN: So my task was to facilitate 2 questions, and I had a whole list of questions here to, 3 hopefully, get the ball rolling, but it seems that many of 4 the questions have been asked by others. I'm just going 5 to ask one or two questions if I might, and I'd like to 6 address the first question to Dr. Slaugenhaupt. 7 I was just curious. This screening panel of 8 compounds sounds like a very interesting piece of work, 9 but you didn't tell us, I don't think, about the mechanism 10 by which you're evaluating the ratio between wild type and 11 mutant. 12 DR. SLAUGENHAUPT: For the first-pass screening 13 data, what we did was use the densitometric assay. So we 14 took an FD cell line that was split into parallel cultures 15 and we did a first-pass screen by treating the cultures 16 with the drug and then isolating RNA and evaluating a 17 ratio using densitometric data. 18 So we take the most active compounds and as 19 we're going back and doing the follow-up, we'll do the 20 follow-up in multiple cell lines and then assay by 21 quantitative PCR for the wild type mutant separately to 22 see if we see an effect. 23 DR. RUBIN: And did I understand correctly that 24 this is going to be published soon? 25 DR. SLAUGENHAUPT: The meeting report is up 0134 1 there. Our data is not ready to be published on the 2 specific compounds and what's going on with those 3 compounds. We're doing the follow-up studies now. So 4 hopefully we'll have some positive results in which will 5 be published then. 6 DR. RUBIN: Dr. Sonenshein, we haven't picked on 7 you yet, so it's your turn. Treatment with increasing 8 concentrations of TNF is having some impact on IKAP. Can 9 you tell us is that at the transcriptional level? 10 DR. SONENSHEIN: We only looked at doing 11 immunohistochemistry, so we have no idea at what level 12 it's affected. 13 DR. RUBIN: I guess there are no other 14 questions. Go ahead. 15 MS. DORNBERG: I'm Greta Dornberg, a parent of a 16 child with FD. This is more of a clinical question. 17 There's an FDnet with a lot of people writing about their 18 symptoms, and a lot of the parents are reporting that once

19 their child is put on IV solution, their child is doing so 20 well and they're not showing symptoms of crisis when 21 awakening. Do you think there's something to that, giving 22 the solution IV rather than the way the children are 23 normally? Is there something in their stomach that's not 24 working correctly, and is that something to do with the 25 hyponatremia we've been seeing and so forth? 0135 1 DR. AXELROD: Are you talking about IV hydration 2 fluid or are you talking about IV medication? 3 MS. DORNBERG: Hydration fluid. They've all 4 been writing that even though they get adequate liquids 5 normally. 6 DR. AXELROD: Yes. Well, sometimes the stomach 7 is not able to absorb the fluid well when they're in 8 crisis, and so the hydration is restoring the vascular 9 volume and the patient is perfusing their tissues better. 10 So they do feel better. 11 MS. DORNBERG: Is that something, though, to do 12 with Dr. Kennedy's work? Is there something in the 13 stomach that's not really picking things up, whereas it is 14 through the veins? 15 DR. KENNEDY: We haven't looked, so I can't 16 answer that. But from looking at the peripheral nervous 17 system, those C fibers, I would put a bet and maybe give 18 odds that they'll find abnormalities in the stomach too. 19 DR. AXELROD: We have some preliminary data that 20 indicates that during crisis that there is a 21 vasoconstriction or poor perfusion of the gut so that even 22 if you're delivering fluid, therefore the fluid can't get 23 absorbed from the GI tract. It's what we would call a 24 vascular problem. 25 DR. SONENSHEIN: Can I mention that if people do 0136 1 have manuscripts that are in press or they're saying you 2 can get it, if people could e-mail them to me. Then 3 anybody who puts their name on that e-mail list, I will 4 forward all the papers to them. 5 DR. RUBIN: Gail, I wanted to thank you for that 6 offer and that is helpful. 7 I did have a question for Dr. Kennedy about the 8 innervation, and I was wondering whether the differences 9 that you're seeing are related to severity of disease or 10 age of the patients. 11 DR. KENNEDY: Our controls covered a very wide 12 range and even people in their 60s have much greater 13 innervation. So it's not due to age. 14 Severity of disease I can't really answer 15 because the samples we got -- they were all quite severe, 16 as you saw, absent nerves in many. So we would have to 17 either sample people who were less involved or perhaps 18 different locations would show that. 19 DR. AXELROD: The other thing is that when 20 sampling all of the patients -- there were only 10. 21 Again, numbers are very important. And the 10 patients 22 were all post-adolescence. So maybe the way to have 23 looked at it was to do biopsies on pre-adolescents versus

24 adolescents so that you actually could pick up some 25 difference. 0137 1 DR. RUBIN: Dr. Maayan will get the last 2 question. 3 DR. MAAYAN: It's just a comment on your 4 question. We were looking at the same thing on the 5 innervation of the gastrointestinal biopsies, and looking 6 at the age and severity. And we were looking at about, I 7 think it was, more than 20 patients. Because the range 8 was not so big and, after all, 20 was not enough, it was 9 not significant. But there were some trends, definitely. 10 DR. RUBIN: Thank you. I'll turn it over to Dr. 11 Gwinn-Hardy. 12 DR. GWINN-HARDY: Thank you to all the speakers 13 and discussants in this section, and thank you, Dr. Rubin, 14 for leading the discussion. I can see we have a lot more 15 to talk about, but I want you guys to get some food in 16 your stomachs too. Let's meet back here at 1:15. 17 (Whereupon, at 12:15 p.m., the meeting was 18 recessed, to reconvene at 1:15 p.m., this same day.) 19 20 21 22 23 24 25 0138 1 AFTERNOON SESSION 2 (1:26 p.m.) 3 DR. GWINN-HARDY: It's my pleasure to introduce 4 David Goldstein, who is a friend, as well as a colleague. 5 He's the chair of the next session, and he is going to 6 talk to us about dysautonomia in Parkinson's disease as 7 well as help us with the rest of the session and lead the 8 discussion at the end of the session. Thank you very 9 much, Dr. Goldstein. 10 DR. GOLDSTEIN: Thanks, Katrina. 11 Well, I think the contents and flow of this 12 session are going to differ drastically from the contents 13 and flow of the first. The first session was highly 14 focused on a specific disease entity, familial 15 dysautonomia, which is, as everybody now knows, a quite 16 rare condition. I'm going to be heading a session that 17 hopefully will expand your perspective a little bit both 18 in terms of other forms of inherited dysautonomia besides 19 FD and also in terms of other -- how do I put it -- other 20 constituencies, including a patient support group and the 21 point of view of the people who are actually severely 22 affected by being in a family with an inherited 23 dysautonomia. 24 Now, one of the themes in my talk, which I'll be 25 starting in a minute, is that although FD is quite rare, 0139 1 inherited dysautonomia is not rare. Inherited 2 dysautonomia is actually quite common. This is my

3 editorial, but probably the most common form of inherited 4 dysautonomia is in a disease where it hasn't thought to be 5 a dysautonomia at all, and that's Parkinson's disease. 6 So, we're going to be shifting from a rare condition 7 that's definitely Office of Rare Diseases material to a 8 common disease that's bread and butter NINDS material, and 9 I think we'll be able to come up with some interesting 10 comparisons and contrasts in the discussion. 11 The first order of business is to dispel the 12 notion that there's an autonomic nervous system. There 13 are actually five components to the autonomic nervous 14 system. They could be affected or not affected in a 15 particular disease, and I think it's a terrible mistake to 16 lump all forms of autonomic failure together. 17 Just to refresh your memory, about a century ago 18 Langley defined the autonomic nervous system in terms of 19 three components: parasympathetic, which is a term that 20 he coined -- he also coined the term "autonomic nervous 21 system" for that matter -- sympathetic, and enteric. 22 In the early 20th century, Walter Cannon, a 23 great American physiologist, added another component which 24 was the adrenal medulla. And he lumped together the 25 sympathetic nervous system and adrenomedullary hormonal 0140 1 system, as shown here, into something that's been called 2 the sympathoadrenal system, or sympathicoadrenal system. 3 He was wrong, but this is still a dominant thought in 4 physiology. 5 Finally, a fifth component of the autonomic 6 nervous system, discussed briefly this morning, is 7 sympathetic cholinergic function where the 8 neurotransmitter is not norepinephrine, but is 9 acetylcholine, and that is the transmitter that's 10 responsible for thermoregulatory, gustatory, and emotional 11 sweating. 12 So there are five components of the autonomic 13 nervous system, and I think all bets are off at this point 14 as to which exactly are deranged in FD or any other form 15 of inherited dysautonomia because of the view that all 16 autonomic failure can be lumped. 17 Now, just as there are different components of 18 the autonomic nervous system, there are also different 19 symptoms and signs of failure of the autonomic nervous 20 system, depending on the component that's affected. Here 21 you see the symptoms and signs that would be associated 22 with sympathetic noradrenergic failure, parasympathetic 23 cholinergic, and sympathetic cholinergic. The enteric 24 system remains a complete mystery, or just about a 25 complete mystery, as far as I know, and the 0141 1 adrenomedullary hormonal system is rarely studied. 2 What I'm going to be focusing on today is 3 sympathetic noradrenergic failure which is manifested by 4 orthostatic or postprandial hypotension. And conversely, 5 because the sympathetic nervous system is absolutely 6 required to tolerate simply standing up, orthostatic 7 hypotension is a cardinal manifestation of sympathetic

8 noradrenergic failure. 9 Well, orthostatic hypotension occurs remarkably 10 commonly in Parkinson's disease. You just have to measure 11 the blood pressure lying down and standing up, something 12 that neurologists have not, until recently, routinely 13 done. But if you define orthostatic hypotension as a fall 14 in systolic pressure of 20 millimeters of mercury or more 15 between lying down and standing up, then a substantial 16 minority, if not about half of all patients with 17 Parkinson's disease, have orthostatic hypotension, and you 18 can argue about the percents, but you can't argue about 19 the importance I think of orthostatic intolerance, 20 orthostatic hypotension, as an imminently treatable cause 21 of morbidity and mortality in patients with Parkinson's 22 disease. 23 Now, if a patient has orthostatic hypotension, 24 that doesn't necessarily mean that the orthostatic 25 hypotension is from failure of the sympathetic nervous 0142 1 system. After all, just being bed-ridden or dehydrated 2 will cause orthostatic hypotension. 3 How do you know that there's a problem with the 4 sympathetic nervous system or with regulation of 5 sympathetically mediated vasoconstriction in a response to 6 a fall in venous return to the heart? One way is by 7 looking at the beat-to-beat blood pressure responses to 8 the Valsalva maneuver where the person blows against a 9 resistance for several seconds and then relaxes. 10 During phase II of the maneuver, as shown on the 11 left, the blood pressure measured beat to beat goes down 12 because of the fall in stroke volume, but then it starts 13 to creep up, and that is because of reflexive 14 sympathetically mediated vasoconstriction. You can think 15 of it simply in terms of an analogy to a garden hose. And 16 you're measuring the pressure in a garden hose, and you 17 turn down the faucet. The pressure goes down. But if you 18 tighten the nozzle, then the pressure can creep back up in 19 that hose, even though the faucet is still turned down. 20 These people normally tighten the nozzle. 21 Now, in phase IV, after the person relaxes, the 22 blood comes into the heart. The heart pumps the blood 23 into a reflexively constricted vasculature. It's like 24 turning the faucet back on, but you forgot to loosen the 25 nozzle. Because of that, the blood pressure overshoots, 0143 1 and that's what you see here. 2 Now, in patients who have neurogenic orthostatic 3 hypotension, as I call it, during phase II, the blood 4 pressure just goes down, down, down, down, down. That's 5 because the person can't tighten the nozzle. In phase IV, 6 the blood pressure slowly comes up to baseline but doesn't 7 overshoot for the same reason. 8 So the two manifestations that I use for 9 determining whether orthostatic hypotension is really 10 neurogenic is what happens to the blood pressure in phase 11 IIL and what happens to blood pressure in phase IV. I 12 only define an abnormality if I see both because there are

13 cases where you can have one or the other, but I'm talking 14 about both. 15 Now, in chronic autonomic failure, the syndromes 16 have been divided up into three: pure autonomic failure, 17 this large box called multiple system atrophy; and there 18 are parkinsonian, cerebellar, and mixed forms; and then 19 Parkinson's disease with autonomic failure. And I think 20 you can see immediately there's a problem. How do you 21 tell the parkinsonian form of MSA from the autonomic 22 failure in Parkinson's disease? After all, both groups 23 have "autonomic failure." And again, I'm lumping together 24 all autonomic failure as if it was all one thing. And of 25 course, they have parkinsonism. Up until very recently, 0144 1 this has been a big problem because although it's thought 2 that a good response to Sinemet would tend to make the 3 person in this category, there are patients with the 4 parkinsonian form of MSA who improve on Sinemet. 5 Moreover, it's deeply ingrained in neurological 6 lore that if you treat a patient with Parkinson's disease 7 who has orthostatic hypotension with Sinemet, this will 8 worsen the orthostatic hypotension. Therefore, there are 9 many patients I think who don't have the benefit of a 10 trial with Sinemet because they have orthostatic 11 hypotension in the setting of their Parkinson's disease, 12 and this is unfortunate. 13 By the way, Sinemet doesn't cause orthostatic 14 hypotension. 15 Now, in Parkinson's disease, where is the 16 lesion? This is the game neurologists love to play. Is 17 it a free ganglionic lesion such as in multiple system 18 atrophy? Well, everybody knows there's a brain problem in 19 Parkinson's disease. If you'll excuse the pun, that's a 20 no-brainer. 21 (Laughter.) 22 DR. GOLDSTEIN: And the sympathetic innervation, 23 such as of the heart, should be intact because the problem 24 is with regulation of the nerve traffic to the terminals, 25 but the terminals are there. 0145 1 In pure autonomic failure, it's pretty clear, 2 the problem is postganglionic. There's a loss of the 3 nerve terminals themselves, and at least until recently, 4 there was not really well-accepted evidence for central 5 neurodegeneration in PAF. 6 Well, what about Parkinson's? In order to 7 distinguish these two conditions, we applied 8 fluorodopamine PET scanning. Fluorodopamine is a 9 sympathetic imaging agent that our group developed at the 10 NIH about a decade ago now. A fluorodopamine scan of the 11 heart -- for those of you who are neurologists, this is a 12 heart, and this is the left ventricular septum. This is 13 the free wall and this is the left ventricular chamber. 14 This is where the blood comes out and goes to the brain. 15 And you see a beautiful image of the left ventricular 16 myocardium. It looks like a horseshoe or a McDonald's M. 17 We applied this in patients with different forms

18 of autonomic failure. To control for perfusion, we used 19 13N-ammonium perfusion scanning. Basically all these 20 patients have normal perfusion. 21 Here you see that in pure autonomic failure, the 22 perfusion is okay, but the heart is gone. 23 In multiple system atrophy with sympathetic 24 failure, the perfusion is okay. The nerves are there. 25 And in Parkinson's disease, at least in this 0146 1 patient, the perfusion is there. The nerves are gone. 2 Well, that was a weird one. That says that this is a 3 postganglionic lesion? That means that Parkinson's is not 4 just a brain disease? 5 We had to follow up on that, so we did. And 6 this shows the results of a lot of PET scans now we've 7 done in several groups. All patients with Parkinson's 8 disease and orthostatic hypotension -- every one that 9 we've studied -- has had a marked decrease in 10 fluorodopamine-derived radioactivity and therefore, I 11 believe, a loss of sympathetic innervation of the heart. 12 And there's no overlap between this group and this group 13 at all. This is 2 standard deviations below the normal 14 mean. 15 The white circles represent patients with 16 familial Parkinson's disease. Now, when I'm talking about 17 familial Parkinson's disease, the way I'm defining it is 18 the patient, as well as at least two other family members 19 have or had Parkinson's disease. So it's a rather 20 conservative definition. 21 But even by that definition, we were able to 22 find 7 patients. You can see that the majority of them 23 have orthostatic hypotension that's associated with 24 sympathetic denervation of the heart. You can see there 25 was 1 patient who didn't have orthostatic hypotension but 0147 1 did have denervation of the heart, and there are 2 2 patients who did not have orthostatic hypotension and had 3 radioactivity that was within the normal range. You could 4 argue about whether this group is different from that 5 group or not. 6 I wanted to compare these groups of patients 7 with familial Parkinson's disease who did or did not have 8 orthostatic hypotension. Here's what I found. In the 9 patients with orthostatic hypotension, the plasma 10 norepinephrine level during supine rest was lower. The 11 fractional increase in plasma norepinephrine during 12 standing was decreased. Normally plasma norepinephrine 13 levels double within 5 minutes of standing. This is 14 backwards. Of course, the patients who had orthostatic 15 hypotension had orthostatic hypotension. 16 Finally, baroreflex-cardiovagal gain, which is 17 to say the amount of change in heart rate that occurs 18 reflexively for a given change in blood pressure, was 19 markedly decreased in the patients with orthostatic 20 hypotension. 21 Among patients who did not have orthostatic 22 hypotension -- now we're talking sporadic or familial --

23 about half have a complete loss of sympathetic innervation 24 of the heart. The remaining half have a partial loss of 25 sympathetic innervation of the heart, and a very small 0148 1 minority have normal innervation of the heart. This means 2 that sympathetic denervation in Parkinson's is 3 characteristic of the disease. 4 Well, what happens to these patients with 5 partial denervation? This is a patient who happens to 6 have familial Parkinson's disease who did not have 7 orthostatic hypotension and was studied twice. You can 8 see -- it's kind of obvious -- that there's a progression 9 of the loss of the innervation of the heart in this 10 patient. 11 Here's a different patient with familial 12 Parkinson's disease who we studied after about three 13 years. We're looking at the blood pressure and pulse rate 14 responses to get a measure of baroreflex-cardiovagal gain. 15 But I don't think we have to give numbers here. You can 16 see that at this time the Valsalva maneuver -- well, let's 17 see. The blood pressure goes up at the end of phase II. 18 There's a nice overshoot at the end of phase IV. That is 19 -- anyone? 20 VOICE: Normal. 21 DR. GOLDSTEIN: Normal. And here you see the 22 reflexive tachycardia. So the baroreflex gain is 23 excellent. 24 Here's the same patient but about three years 25 later. Well, the blood pressure goes down a lot. You can 0149 1 make an argument here, well, maybe there's some return up 2 here. There is still an overshoot. This is still normal 3 by my criterion. But you can see that the heart rate 4 response is obviously blunted even though the fall in 5 blood pressure is greater. You can even make a case for 6 autonomic bradykinesia in this patient because the heart 7 rate increase is late. But the bottom line is that the 8 baroreflex gain has gone down tremendously in this 9 individual with familial Parkinson's disease. 10 We've had 2 patients with familial Parkinson's 11 disease who we followed over three years. Obviously, this 12 is preliminary and hasn't been published. The left 13 ventricular radioactivity goes down. Plasma 14 norepinephrine goes down. The baroreflex-cardiovagal gain 15 goes down tremendously. And these patients still have 16 roughly normal fractional increases in norepinephrine 17 during standing, and they don't have orthostatic 18 hypotension yet, but I wouldn't be surprised if they 19 develop it. 20 Well, what causes the dysautonomia in familial 21 Parkinson's disease? Well, obviously, I don't know, but 22 one cause certainly is synucleinopathy. And the reason I 23 say that is we had an opportunity to study a patient who 24 is part of this large Greek-Italian kindred, whom many of 25 you know about, where Parkinson's disease is transmitted 0150 1 as an autosomal dominant trait due to mutation of the gene
2 that encodes alpha-synuclein. And one of these patients 3 was studied at the NIH. 4 We found that he did have orthostatic 5 hypotension. He had never been diagnosed as having 6 orthostatic hypotension until he came to the NIH where 7 somebody measured his pressure lying down and standing up. 8 The orthostatic hypotension was from sympathetic failure 9 because of the abnormal baroreflex response. The problem 10 with phase II, lack of overshoot in phase IV. And here 11 you can see that although the perfusion of the heart was 12 okay, the sympathetic innervation of the heart was 13 essentially gone. 14 So at least one cause of the dysautonomia in 15 familial Parkinson's disease is the same cause as the 16 cause of the movement disorder which is the 17 synucleinopathy. 18 So in conclusion, cardiac sympathetic 19 denervation characterizes both familial and sporadic 20 Parkinson's disease. The denervation appears early. It 21 progresses over time. Neurogenic orthostatic hypotension 22 in familial Parkinson's, as well as in sporadic 23 Parkinson's, is associated with more generalized 24 noradrenergic denervation, and baroreflex cardiovagal 25 failure. And finally, alpha-synucleinopathy can cause 0151 1 both a dysautonomia and the movement disorder in familial 2 Parkinson's disease. 3 And I want to thank the members of my 4 neurocardiology team. For those of you who were up late 5 watching the Yankees, you recognize Yankee Stadium here. 6 Courtney Holmes is our star short stop. Sandra Brentzel 7 is the one who refers all the patients, so she's at a 8 pivot position. Teresa Jenkins is our patient care 9 coordinator. She's the one who catches all the calls from 10 the patients and their physicians. Irv Kopin, who was the 11 scientific director of our institute for 11 years, now is 12 in a scientist emeritus position, so he's in the coaching 13 box. And I'm the one who gets to give the pitch. 14 (Laughter.) 15 DR. GOLDSTEIN: Thank you. 16 (Applause.) 17 DR. GOLDSTEIN: The next speaker is Sonia 18 Peltzer. Sonia is the President and founder of FD Hope 19 and I think will provide a very different perspective 20 about research and the future of research into mechanisms 21 and treatment of FD. 22 DR. PELTZER: Thank you, Dr. Goldstein. I'd 23 like to thank particularly Katrina Gwinn-Hardy for all her 24 help in making this whole conference a reality. 25 I'm going to first introduce myself and tell you 0152 1 a little bit about myself. I'm here for three reasons. 2 The most important reason is I'm the mother of four 3 children. My oldest 9, Benjamin; my second is a 7-year- 4 old Rachel. And they asked me to say something about 5 them, so I'd like to say that it is because of their 6 generous sharing of their mother that I'm here today. And

7 I have a 4-year-old son, who will be 5 on Sunday, by the 8 name of Samuel. Samuel has familial dysautonomia. I also 9 have a 3-year-old daughter named Sarah who will be 4 in 10 December, and she also has familial dysautonomia. That is 11 why I'm here, and in some small part that's why we're all 12 here. 13 I'm also here because, as Dr. Goldstein 14 mentioned, I'm one of the founders of FD Hope, and I'm the 15 current President. Familial Dysautonomia Hope is a 16 nonprofit organization that was founded in the early 17 months of 2001. Almost immediately upon founding, we 18 initiated contacts with the NIH because one of our major 19 goals was to get a conference like this going. Our 20 mission is to expand research, accelerate research to find 21 a cure, and that's what you're going to hear about from me 22 today, encouraging more of that. 23 Almost 20 years ago, I was graduate student at 24 Johns Hopkins studying these. These are cuneiform 25 tablets. There are thousands of them. Many of them have 0153 1 yet to be translated. This particular one is about the 2 Gilgamesh epoch for those of you who know about that. And 3 I sat in my little cubicle looking at my Acadian language 4 studies, and I thought to myself one day if I never 5 translate these tablets, if no one ever translates these 6 tablets, will it ever make a difference? And the answer 7 was a resounding no. Within three months, I had left 8 graduate school and had planned to go to medical school. 9 You can make a difference and that's why I'm 10 sure most of you have gone into the fields that you have. 11 One way to make a difference, whether you're a 12 basic scientist or a clinician, is to do translational 13 research. The key to translation is mentoring a new 14 generation of translational researchers not only for you 15 to do research but for you to encourage those who follow 16 you to do translational research. 17 And this is the definition of translational 18 research that I got from the Scientist, which came out 19 just this past week. Essentially it's research that goes 20 from the lab to bedside and then back to the lab bench. 21 This morning we heard a lot about possible 22 mechanisms behind some of the clinical symptoms of 23 familial dysautonomia, and I'd like to talk a little bit 24 about that. 25 The bottom line is patients are dying. Children 0154 1 are dying of FD. Adults are dying of FD. They're dying 2 because of cardiovascular complications, heart attack, 3 stroke, dysrhythmias. You expect heart attacks in your 4 60's. These are 20-year-olds. Renal failure, pulmonary 5 complications, not just the aspiration but the restrictive 6 lung disease caused by scoliosis which fortunately, 7 because of the interventions introduced by Dr. Axelrod and 8 Dr. Maayan, the surgeries, et cetera, we're seeing less 9 of. Baroreceptor dysfunction. Patients are suffering. 10 Autonomic crisis Dr. Axelrod touched on briefly 11 and we got a list of some symptoms, and I'll do the same
12 thing. I'll give you a list of symptoms. But I want to 13 give you a true sense of what autonomic crisis is, and I'm 14 going to describe briefly what my daughter Sarah goes 15 through when she goes into crisis. 16 Sarah is, as I mentioned, 3. For a year-and-a- 17 half, she was in crisis once or twice a month. I started 18 her on some different products, and she's been essentially 19 crisis-free. She's had five episodes of crisis in the 20 succeeding year-and-a-half, but I cannot tell you enough 21 what a horrible thing this is. 22 A child who is pre-crisis, which you sometimes 23 see before they go into full-blown crisis, isn't hungry. 24 She might go from eating six times during the day to 25 eating once or twice and refusing all other food. And 0155 1 this is eating through a gastrostomy tube. They sweat. 2 They drool. They're uncomfortable. Those who have 3 geographic tongues, the geographic tongue tends to become 4 more prominent during the pre-crisis phase. 5 When she goes into crisis, Sarah will start 6 vomiting. Now, she has a fundoplication. Depending on 7 your philosophy, you either don't expect or do expect 8 vomiting. When she starts to vomit, she will vomit for 12 9 hours. I know that you've all had gastrointestinal 10 viruses. Imagine your very worst one and stretch it out 11 for up to a week. That's what crisis is. She will vomit. 12 She will sweat. She's in abdominal pain. Blood pressures 13 are sky high. Heart rate, 150s, 160s. When she was in an 14 ICU at one point as an infant, she had an arterial line 15 placed, and we documented blood pressures of 240 over 160 16 in a 3-month-old. 17 This is not something to be taken lightly. 18 Children die because of crisis, and those who don't, I've 19 heard parents say their children wish that they were dead. 20 This is a horrible, horrible disease. 21 When Sarah starts to come out of crisis, she'll 22 throw up for about 12 hours and then she'll lay there and 23 be miserable. And part of crisis symptoms are these 24 personality changes. They cry. They're unhappy. Nothing 25 makes them happy. Their abdomens hurt. She will go into 0156 1 a period of half awake/half asleep, almost an 2 encephalopathic picture, not completely out of crisis. 3 You can't push more than 5 cc's. And for those who don't 4 know what that means, it's a teaspoon of saline type 5 solution through her G-tube every 5-10 minutes. And 6 you're up for 24 hours a day, 7 days a week until she goes 7 out of this period unless you're in the hospital to get IV 8 fluid. 9 From there, she will eventually go into what's 10 called the restorative sleep, and when she starts to 11 sleep, we all breathe a sigh of relief. She will sleep -- 12 and the longest we've documented in Sarah -- and other 13 children have different amounts -- was 27 hours straight. 14 And we were thrilled. She comes out of it, bounces back 15 as if she had never been sick. 16 I'm going to show you a video that will show you

17 what crisis is like. It shows a child actually in the 18 throes of crisis. 19 (Video shown.) 20 DR. PELTZER: As a physician, I'm going to go 21 through all the list of symptoms that you see, cardiac 22 symptoms, the high blood pressure, the tachycardia, cold 23 extremities, mottling, purple mottling of the extremities, 24 and blotching, GI symptoms, retching or vomiting, retching 25 when you have really tight fundoplication, inability to 0157 1 swallow or to talk, abdominal pain, increased gastric 2 acid, gastric secretions. You get gastritis and ulcers. 3 Hypersalivation and drooling. We also know the 4 bronchorrhea as well. Increased reflux and impaired 5 esophageal motility. 6 The interesting thing is that when a child is in 7 what I term, for lack of a better term, pre-crisis, a 8 child cannot be in crisis but for up to a month be not 9 quite right either. You will see an increase in reflux in 10 those children. You see decreased swallowing ability and 11 loss of some speech ability as well. They're not in 12 crisis, but you still see these early crisis symptoms. 13 Constipation, gaseousness. Renal. You can see 14 the urinary retention. Headache, emotional ability, 15 feeling panicky. 16 I described my daughter's crisis. My son's 17 crises are very, very few and far between. I can count on 18 one hand the number of times he's been in crisis, and some 19 of those have been only an hour at a time. But he is 20 wild. He cannot lay still in bed. He just goes from one 21 side to the other. A totally different picture of crisis 22 in two siblings. 23 Thrashing, moaning, lethargy, agitation, being 24 out of it. These are all words written by parents about 25 children with FD. Fever, chills. They can have normal 0158 1 temperatures and within a space of 5 minutes have a 2 temperature of 103 and an hour later be normal again. 3 Dilated pupils, obviously, and the 4 hyperhidrosis. When I say hyperhidrosis, that sounds like 5 a very clinical term. In reality it means, if you don't 6 put towels down on your bed, you're washing about five 7 sets of sheets during a crisis day. They absolutely soak 8 through. You can literally take a shirt off and wring it 9 and see sweat drip off. 10 Rubbing the body is another sign that a lot of 11 parents say that they see their children do before they 12 actually go into the full-blown crisis. They'll rub their 13 nose, their extremities. One parent says that her child 14 will rub their dog. 15 Self-mutilation. There have been children who 16 have had horrible disfiguring scars on their face. Finger 17 biting, but scratching at the face as if they're trying to 18 get something gone. Something is bothering them. 19 The severity of the problem. Well, I hope I 20 have described for you how significant this problem is. 21 A year-and-a-half ago, we did a survey of

22 families, a patient-based survey on symptoms, and we did 23 particularly the gastrointestinal symptoms prior to going 24 to the GI conference, the DDW conference. One of the 25 questions we asked was about crisis. We had 54 0159 1 respondents. 13 of 16 respondents that did answer this 2 question on impact on quality of life gave crisis a 10 out 3 of 10 in severity. 85 percent of the 55 patients have had 4 autonomic crisis, and our numbers, it was 45 percent of 5 them had crisis at least monthly, and that's daily, 6 weekly, or monthly. 17 percent of the patients who 7 experienced crisis have it daily. Now, for those 8 patients, it may not be quite as full-blown as I had 9 described. They may have a crisis period in the morning. 10 Unfortunately, the treatment for crisis is medications 11 that are pretty sedating. So even though you may be out 12 of crisis, you've lost your day. 13 Aspiration pneumonia and pulmonary damage. You 14 see regression of developmental milestones during that 15 period. 16 Another thing is impact on lifestyle. Like I 17 said, these drugs are sedating. 18 And the piece that I cannot describe enough is 19 the impact on the family. We think of diseases as 20 affecting individual patients. This disease, as most 21 diseases, affects families. Parents can't go away. My 22 husband and I have been out together four times in the 23 past five years. You cannot get out of the house unless 24 you have someone you can trust with your children. And 25 this disease is so unpredictable and devastating, you 0160 1 cannot trust just anyone with your children. It is the 2 unpredictability of crisis that is just so horrible. 3 There is an individual with familial 4 dysautonomia who goes into crisis when she urinates, not 5 all the time, but sometimes. So this young woman, who's 6 in what should be the prime of her life, rarely goes out 7 of her house. 8 Things that can trigger. I'll just put these 9 all up. These are some of the triggers of autonomic 10 crisis again from the patient family survey, as well as 11 adolescents. 12 There are things that can be done by all of you. 13 You're here because you have a lot of experience in your 14 respective fields and you're very talented. It is my hope 15 that when you leave today that you're going to go back to 16 your bench, if you do research, with a goal in mind, and 17 that is to make a difference in patients' lives. 18 Translational research is not just a buzzword. It's an 19 essential form of research today. 20 We heard this morning from Dr. Hilz that heart 21 rate variability decreases with Valsalva. There have been 22 several studies looking at alpha-lipoic acid in diabetics 23 with cardiovascular dysautonomia, and they suggest that 24 there is improvement in heart rate variability. An alpha- 25 lipoic acid is an antioxidant. Taking that clinical 0161

1 piece, applying it to FD, and then going back to the lab 2 to say, if it does make a difference, do antioxidants 3 impact on heart rate variability and why. That's the kind 4 of research that I charge you all to do today. 5 The need for translational research. We need 6 both clinical as well as genetic research, and clinically 7 significant research that's going to address the areas 8 with the greatest impact are things that will impact on 9 blood pressure control, hypertension, as well as 10 orthostatic, renal protecting, cardiac dysrhythmias, 11 autonomic crisis, preventing crisis, what are some common 12 mechanisms behind those triggers, as well as new 13 treatments. 14 Genetic research that will have impact. We've 15 heard a lot about these, obviously. I'm not a geneticist. 16 I'm not going to go over this in detail. 17 Even the smallest person can change the course 18 of the future. You all are not small people. You're big 19 people. Please change the course of our children's 20 future. 21 I'm going to end with some photos. This is 22 Michele. These are all children with FD. Dovi, Evan, 23 Michele, David. David Rancer is no longer with us. He 24 died a year ago of malignant hypertension we believe. 25 Rebecca, Zack, and this is my own, Sammy and Sarah. 0162 1 Our future is in your hands. I implore you not 2 to be lured by the fascination of science for science's 3 sake. If you apply your talents towards translational 4 research and encourage those who come under you for 5 training, you can save a life. You can save lots of 6 lives. 7 So because FD is a Jewish disease, I'm going to 8 end with a quote from the Talmud. If you save a life, you 9 save the world. 10 Thank you. 11 (Applause.) 12 DR. GOLDSTEIN: I told you it would be 13 different, and it will continue to be. 14 The next speaker is Dr. Ando who's an associate 15 professor and Vice Director of Laboratory Medicine at 16 Kumamoto University School of Medicine in Japan. Dr. Ando 17 is an expert on a different type of inherited 18 dysautonomia, familial amyloidotic polyneuropathy. I'm 19 very interested in hearing what he has to say about this 20 other condition, also rare, but I think you'll see some 21 rather striking similarities in the issues and the 22 strategies scientists have tried to employ to understand 23 and treat this condition. 24 DR. ANDO: Thank you very much, Dr. Goldstein. 25 First of all, I would like to express my 0163 1 gratitude to the organizing committee of this workshop for 2 giving me a chance to talk about our original research on 3 FAP and autonomic dysfunction. 4 FAP is amyloidosis and amyloidosis is a disorder 5 of protein metabolism in which soluble proteins are
6 deposited in the tissues as abnormal insoluble fibrils. 7 Amyloid fibrils are like nylon fibrils. In other words, 8 amyloidosis is similar to nylon storage disease. 9 Familial amyloidotic polyneuropathy, or FAP, is 10 an incurable hereditary amyloidosis and transmitted via 11 autosomal dominant mode of inheritance. 12 The precursor protein of amyloid deposition in 13 FAP is a mutated transthyretin which is predominantly 14 produced by the liver and binds to T4 and retinol-binding 15 protein in plasma. 16 About 100 point-mutations or deletions have been 17 reported, and most of them lead to FAP. Of those, 20 show 18 mainly autonomic dysfunction. 19 This slide shows amyloid deposition in the 20 nervous system in FAP patients. Amyloid deposits are 21 commonly found in sympathetic and dorsal ganglia and in 22 peripheral nerves in addition to systemic organs. 23 Of the various types of FAP, the FAP TTR 24 methionine 30 type is the most common. The clinical 25 manifestations are classified into three major groups. 0164 1 Among them, those of the autonomic dysfunction group have 2 the greatest effect on the patients' lives because they 3 restrict their daily life. 4 The duration of FAP, after the onset of the 5 disease, is about 10 years. In addition to various 6 autonomic dysfunction, severe systemic organ dysfunction 7 is commonly observed. 8 Until 10 years ago, the foci of FAP Met 30 were 9 restricted to several endemic geographic areas. However, 10 owing to the progress of molecular genetics and protein 11 chemistry, now this disease is considered to be a 12 worldwide occurrence. This is a map of Japan. In 13 addition to two major foci of Met 30, various other types 14 of FAP have been discovered in many districts of Japan. 15 To evaluate autonomic dysfunctions found in FAP 16 patients, we employed those, some of which we originally 17 developed. 18 In terms of autonomic dysfunction, orthostatic 19 hypotension causes FAP patients to have terrible problems. 20 The trauma to this patient's left eye was noted when he 21 tumbled down after he stood up. We recently reported the 22 interaction between cerebral blood flow and autonomic 23 dysfunction. As you can see in this slide, the reverse 24 flows in common carotid artery and vertebral arteries are 25 always noted when the patient stood up and experienced 0165 1 clinical symptoms such as syncope and a feeling of 2 faintness. No reverse flow could be detected when the 3 clinical manifestations were absent. 4 As shown in this slide, the clinical 5 manifestations correlated with the presence of reverse 6 flow. However, no correlations between the degree of 7 orthostatic hypotension and the reverse flow, the presence 8 of reverse flow, were observed. 9 I would like to talk about the disturbance of 10 peripheral circulation in FAP. Various clinical symptoms

11 reflecting autonomic dysfunction are commonly found in FAP 12 patients as initial symptoms. However, it was not yet 13 known when autonomic dysfunction starts in FAP patients. 14 So to elucidate the question, we applied laser Doppler 15 flowmetry to measure the change in the blood flow in the 16 phenotype. As shown in this slide, in control subjects a 17 significant decrease in the blood flow was detected after 18 deep inspiration. In contrast, in the FAP patients in the 19 advanced stage, no such responses were sighted at all. 20 Interestingly, some asymptomatic carrier of the Met 30 21 gene showed poor responses for the stimulations. These 22 results suggest that peripheral or sympathetic C fiber may 23 be first impaired prior to the sensory and the motor 24 nerves. 25 We could detect abnormal vessels microscopically 0166 1 in the conjunctival vessels in FAP patients interestingly, 2 as shown in the slide. ________ of the vessels and 3 micro________-like changes, these, could be found in most 4 of FAP patients. Moreover, these changes could be 5 detected in patients with pan-dysautonomia and Shy-Drager 6 syndrome. These results suggest that these abnormal 7 vessels can be formed via autonomic dysfunction. 8 We could detect abnormal venules in the finger 9 of FAP patients, as shown in this slide, by near-infrared 10 spectroscopy system. These abnormal vessels could be 11 detected in most of FAP patients. 12 As you know very well, cardiac autonomic 13 dysfunction can be evaluated by two methods as shown in 14 the right-hand side of this slide. In the advanced stage 15 of FAP patients, neither low nor high frequency component 16 could be detected at all. 17 MIBG accumulates in the peripheral sympathetic 18 nerves of myocardium. However, in the advanced stage of 19 FAP patients, no such accumulation was observed. 20 Next I would like to talk about disturbed 21 glandular secretion in FAP patients. This slide shows 75 22 gram OGTT pattern in FAP patients, as shown in this slide. 23 Significant hypoglycemia followed after hyper-insulinemia. 24 Interestingly, some FAP patients showed hypoglycemia. 25 We also examined the secretory function of 0167 1 salivary glands and lacrimal glands. This slide shows 2 amount of salivary secretion in different FAP patients. 3 Right is FAP patients and left is healthy volunteers. 4 Although the total amount of salivary secretion was very 5 low in the static state, after they chewed the gum, the 6 ________ hypersecretion of saliva was detected in several 7 FAP patients. As shown in these slides, the same 8 phenomenon could be detected in tears secretion after 9 topical installation of pilocarpine. These results 10 suggest that denervation super-sensitivity occurs not only 11 in the exocrine glands, but also in the endocrine glands. 12 It is very important to note the dynamic aspect of 13 secretory function in these glands. 14 This slide shows increased postprandial 15 hypotension and hypoglycemia after taking a meal. 60

16 minutes after taking a meal, increased postprandial 17 hypotension and hypoglycemia were observed in this 18 patient. 19 To elucidate the disturbed glucose metabolism in 20 FAP patients, we performed a histochemical analysis for 21 autopsy of FAP patient samples. As shown in this slide, 22 although the Langerhans islet itself remained intact, 23 significant amyloid deposition was observed in the 24 pancreatic stroma, enteropancreatic nerves, and around the 25 vessels. These amyloid depositions can be the results of 0168 1 denervation hypersensitivity of glucose metabolism. 2 Next, I would like to talk about the 3 gastrointestinal motility in FAP. In most FAP patients, 4 drugs given by oral administration sometimes cannot 5 express their maximum effect. Therefore, we synthesized a 6 nasal application of L-threoDOPS, the drug for orthostatic 7 hypotension, with a ________ mixture. With this 8 application, the plasma norepinephrine levels, the 9 converted form of L-threoDOPS, was significantly elevated 10 2 hours after application. However, no such increase was 11 observed with oral or vehicle alone application. 12 To evaluate the gastrointestinal motility in FAP 13 patients, we applied electrogastrography. In healthy 14 volunteers, the motility of 3 ________ per minute were 15 usually observed. And after taking a meal, the increase 16 gastrointestinal motility could be detected for more than 17 30 minutes. In contrast, in FAP patients with severe 18 diarrhea, after taking a meal, the increased gastric 19 motility continued for more than several hours. In 20 patients with constipation, no such increase was observed. 21 By the way, anemia is one of the very common 22 clinical manifestations in FAP. Recently we have reported 23 the correlation between anemia and autonomic dysfunction 24 in several neurological disorders. In FAP patients, 25 significant correlation between two factors were observed. 0169 1 In contrast, in ALS which have no autonomic dysfunction 2 showed no anemia. 3 This slide shows 6-hydroxydopamine-induced 4 anemia in rats. 6-hydroxydopamine damages the peripheral 5 sympathetic nerve terminal, resulting in neurogenic 6 anemia. That was reversibly treated by simultaneous 7 administration of desipramine, a competitive inhibitor of 8 6-hydroxydopamine. 9 To treat the anemia found in FAP patients, we 10 administered human recombinant erythropoietin because the 11 anemia commonly found in FAP patients is usually a 12 normochromic, normocytic pattern, as shown in this slide. 13 Plasma hemoglobin levels were significantly increased, and 14 the frequency of orthostatic hypotension was reduced. 15 In the remainder of my talk, I would like to 16 discuss liver transplantation on autonomic dysfunction in 17 FAP. 18 As I said before, the precursor protein of 19 amyloid deposition in FAP is a mutated transthyretin. 20 Transthyretin is predominantly produced by the liver, so

21 liver transplantation has been studied for the treatment 22 of FAP. After liver transplantation, as shown in this 23 slide, the variant TTR levels in serum were dramatically 24 decreased day by day. Liver transplantation improved 25 partially autonomic dysfunction. This is typical data of 0170 1 an FAP patient 8 months after liver transplantation. And 2 several autonomic function improvements, especially 3 urinary function, bladder function improved greatly. 4 This slide shows MIBG scintigraphy before and 5 after liver transplantation. As shown in this slide, 8 6 months after liver transplantation, significant 7 accumulation of MIBG was observed in the myocardium. This 8 suggests recovery of sympathetic nerve ________. 9 Erectile dysfunction is one of the most serious 10 quality of life problems for FAP patients, so we 11 administered Viagra to FAP patients. This slide shows I 12 evaluated by thermography. One-and-a-half hours after 13 administration, erectile dysfunction was treated, although 14 no ejaculation was observed during sexual intercourse. 15 Because of severe shortage of donor livers, 16 domino liver transplantation using the ________ FAP 17 patients' liver has been performed recently. In the 18 second liver recipient, the variant transthyretin in the 19 serum suddenly started to produce from the liver. 20 However, we do not know what types of autonomic 21 dysfunction can be observed in these patients. We must 22 wait a time. 23 Liver transplantation has several problems, so 24 we must have more noninvasive therapy for FAP patients. 25 So we moved on to the trial of genomic TTR therapy in FAP. 0171 1 We constructed three different types of single- 2 stranded oligonucleotide having the normal TTR gene. With 3 this SSO, we intrahepatically injected the normal gene SSO 4 using the transgenic mice having no Met 30 gene. This is 5 the result. Significant gene conversion from the variant 6 TTR gene to normal gene was observed. Although this is 7 preliminary data, we do hope the day will come when we can 8 analyze the autonomic dysfunction in FAP patients who 9 undergo liver transplantation. 10 Thank you very much for your attention. 11 (Applause.) 12 DR. GOLDSTEIN: Now Dr. Maureen Hahn will talk 13 about another inherited dysautonomia that you'll be 14 hearing about in other talks, but this is the first 15 mention of it in this meeting, and that is dysautonomia 16 from deficiency of function of the cell membrane 17 norepinephrine transporter. Thank you. 18 DR. HAHN: I'd like to thank the organizers for 19 allowing me the opportunity to speak today, and I'm going 20 to tell you a little bit about some of the work I've been 21 doing in the laboratory of Randy Blakely at Vanderbilt 22 University. 23 In a little bit of a switch from some of the 24 other talks we've heard, we're actually not a dysautonomia 25 lab, but we're a laboratory that studies monoamine

0172 1 transporters, one of those being the norepinephrine 2 transporter. The norepinephrine transporter is one of a 3 family of proteins that are localized presynaptically to 4 plasma membranes of sympathetic neurons for one and all 5 noradrenergic neurons, so those in the brain as well. 6 The function of the transporter is to take 7 norepinephrine back up from the extracellular space after 8 it has been released by exocytosis by a neuron. This is a 9 sodium-dependent process. And once the norepinephrine is 10 taken back up into the cell, it can be repackaged into 11 vesicles for further release, or it can also be degraded 12 by monoamine oxidases to the metabolite DHPG, which I'll 13 mention a little bit later. 14 The transporter was cloned in 1991 by Randy 15 Blakely, the cDNA for it, and the cDNA codes for a 617 16 amino acid protein which has 12 putative transmembrane 17 domain spanning regions, as well as intracellularly 18 localized amino and carboxy termini. There are potential 19 sites for phosphorylation, and in the second extracellular 20 loop, there are sites for glycosylation, which is 21 something that I'll touch upon again later in the talk. 22 This slide is just meant to illustrate to you 23 what I've said, which is that the norepinephrine 24 transporter, or NET, is localized to synapses of the 25 sympathetic nervous system. 0173 1 This slide shows a culture of superior cervical 2 ganglion, and on the left, you're seeing staining for FM1- 3 43, which is a dye that is taken up after exocytotic 4 release of neurotransmitter, and so it labels for you 5 sites of neurotransmitter release. On the right we can 6 see the same section co-stained with an antibody to the 7 norepinephrine transporter, showing you that the 8 transporter is localized at sites of release. So this 9 emphasizes the importance of this protein in regulating 10 reuptake of norepinephrine and thereby contributing to 11 norepinephrine homeostasis in the body. 12 I just want to also mention that transporters, 13 including the norepinephrine transporter, are targets for 14 multiple psychoactive drugs, including some that have been 15 mentioned already and some that have not. The 16 norepinephrine transporter is a site for binding for 17 cocaine, amphetamine, MDMA, or ecstasy, antidepressant 18 compounds, or methylphenidate, also known as Ritalin, the 19 drug used for attention deficit disorder. This also 20 emphasizes the importance of this protein and that genetic 21 variation in this gene, which is something that we're 22 interested in, could not only influence norepinephrine 23 homeostasis but the response to various drugs. 24 So we have been in our laboratory looking for 25 genetic variation in the norepinephrine transporter and 0174 1 its possible role in the contribution to disease. This 2 slide just shows you that the gene has been cloned and 3 localized to chromosome 16. And below that you see the 4 organization of the gene which has 16 identified exons
5 which, when transcribed and translated into the protein, 6 give you that protein with 12 transmembrane domain 7 structure that I showed you. In addition, two splice 8 variants have been identified, which I won't talk about 9 today, giving further opportunity for genetic variation to 10 influence expression of the protein. 11 One thing I want to emphasize is that NET is a 12 single-copy gene which would indicate that if there is 13 genetic variation or if the gene were deleted, that there 14 would not be a lot of opportunity for compensation. This 15 is the only protein that is responsible for the high 16 affinity uptake of norepinephrine back into the 17 sympathetic neurons. 18 This slide is a little bit more to remind me 19 than to remind you because we have a lot of dysautonomia 20 experts in the room, but the disease that I'll be focusing 21 on today is classified as a dysautonomia, and I'll be 22 talking about orthostatic intolerance which is also gone 23 by many names, orthostatic tachycardia or postural 24 tachycardial syndrome, or POTS. And it was probably first 25 identified and called Soldier's heart over 100 years ago. 0175 1 Some of the symptoms are listed here. So these 2 are all symptoms that, as the name implies, arise when 3 assuming an upright position for the most part. These 4 include lightheadedness, palpitations, pre-syncope, and 5 dizziness. Syncope can occur. Many of the patients 6 experience fatigue, and there's an orthostatic tachycardia 7 of greater than 30 beats per minute. So the heart rate 8 increases and stays elevated when the upright position is 9 assumed. For orthostatic tachycardia, this is not 10 accompanied by an orthostatic hypotension. And plasma 11 norepinephrine levels exceed 600 picograms per ml in 12 patients who were diagnosed with orthostatic tachycardia. 13 And many of the symptoms are consistent with decreased 14 cerebral blood perfusion. 15 Now, orthostatic intolerance, or orthostatic 16 tachycardia, is a syndrome that can accompany various 17 diseases, and as such, you can imagine that there are many 18 ways to get orthostatic tachycardia. There are many 19 underlying pathophysiologies. As an example, an 20 autoimmune disorder in which the body makes antibodies to 21 a subunit of the nicotinic receptor can result in symptoms 22 of orthostatic tachycardia as well as hypovolemia that can 23 be caused by some chloride channelopathies that are known 24 to exist can result in an orthostatic tachycardia. 25 But what we focused on in our lab and what was 0176 1 of interest to us was that a lot of orthostatic 2 intolerance patients seem to have a very hyperadrenergic 3 state that is primarily responsible for the orthostatic 4 tachycardia. There are several ways to get to this 5 endpoint. You can have increased release or increased 6 activation of the sympathetic nervous system that's in 7 overdrive and is responsible for the increased 8 norepinephrine. And from what I've told you about the 9 norepinephrine transporter now, you can also imagine that

10 a way in which you could get to this endpoint would be to 11 have decreased clearance of norepinephrine following 12 release or NET deficiency. 13 In collaboration with David Robertson's group at 14 the Autonomic Dysfunction Center at Vanderbilt, one such 15 patient was identified who had orthostatic intolerance and 16 also seemed to manifest these symptoms that were 17 consistent with not just hyperadrenergia but specifically 18 a NET deficiency. One of the symptoms that was observed 19 was that when going from a supine to an upright position, 20 the norepinephrine levels would increase greatly, but the 21 levels of the metabolite DHPG did not change much between 22 supine and upright. And as I alluded to earlier, DHPG is 23 the metabolite that is formed from the norepinephrine that 24 is taken back up via the transporter. So if 25 norepinephrine is not taken up via the transporter, then 0177 1 DHPG levels will not rise following release from the 2 sympathetic nerves. So this suggested a NET deficiency. 3 Further evidence of this was that the compound 4 tyramine did not seem to have much of an effect in this 5 proband with OI. And tyramine is a compound that also 6 acts at the transporter. I didn't mention it earlier when 7 I talked about drugs that interact with the transporter. 8 Tyramine is actually a substrate. It's taken up by the 9 transporter and causes norepinephrine to actually come out 10 of the vesicles where it's being stored for release. Once 11 the norepinephrine is in the cytoplasm, the transporter 12 can actually work in reverse, and you can get 13 norepinephrine efflux from the cell. So in a normal 14 individual, tyramine actually causes a rise in plasma 15 norepinephrine, and in the proband in this study, plasma 16 norepinephrine did not rise very much in response to a 17 tyramine infusion. So this was also suggestive of NET 18 deficiency. 19 In fact, when the DNA from this patient was 20 directly sequenced, there was in fact found to be a 21 mutation in the transporter, and it was a single-base 22 substitution that changed the three nucleotide code that 23 codes for the amino acid alanine and converted this to a 24 proline. You can see from the sequencing chromatogram 25 that there are two peaks here where there should actually 0178 1 be one, as you see in the surrounding peaks, and that 2 indicates a change in the nucleotide. And because there 3 are two peaks there, that's also indicating that this is a 4 heterozygous mutation. There actually is one normal 5 sequence at that site and one allele with the mutation. 6 Again, showing you the schematic of what the 7 transporter topology looks like, this mutation, for the 8 alanine to proline switch, is located at amino acid 457 9 which would put that in one of the transmembrane domains 10 of the transporter, or TMD 9. Introduction of a proline 11 is known to cause bends in the helical structure of 12 proteins, and so you can imagine that this would have the 13 potential to influence the protein function. 14 When a pedigree was generated for the patient's

15 family, you can see that we were able to generate a 16 pedigree showing, within three generations, the 17 heterozygous presence of this mutation in several family 18 members. In fact, when the entire family was looked at 19 for phenotype related to this, it would seem that if we 20 divide the family members into those that have alanine and 21 alanine on both chromosomes, so no mutations, and compare 22 them to the alanine and proline, if we look at the mean 23 heart rate, we can see that supine, there's a trend for an 24 increase in the heart rate in those family members with 25 the proline mutation and that upon standing, there was a 0179 1 significant increase in the heart rate in the family 2 members with the proline mutation. So it did seem to 3 track with the phenotype in the family. 4 So what we then did was to create the mutation 5 in the lab and, using an expression vector, expressed the 6 mutation in cell lines in the lab and looked to see what 7 the function of the mutant to norepinephrine transporter 8 was. 9 If you just look at A, what I'm showing here was 10 the ability of the transporter to take up the substrate 11 norepinephrine. So we see on the y axis is a tritiated- 12 labeled norepinephrine that is taken up over 13 concentrations of norepinephrine shown on the x axis. You 14 can see here this top curve represents the normal or the 15 wild type transporter and how you see saturable kinetics 16 of uptake of norepinephrine overall concentrations. If we 17 compare that to the A457P mutation, we see that there is 18 very little, if no uptake at these concentrations of 19 norepinephrine. 20 We also then looked with a radioligand binding, 21 RTI55 is a compound that's similar to cocaine and binds to 22 the transporter. We used this to get an idea of protein 23 binding levels in the cell. So in membrane preparations 24 from the cells that are expressed in the transporter, we'd 25 look and see that over increasing concentrations of 0180 1 RTI-55, we get again saturable kinetics of binding for the 2 wild type transporter and we get binding to A457P, but it 3 appears to be much lower compared to the wild type. 4 We also looked, as you'll see in C, at the 5 ability of A457P to bind the substrate norepinephrine. We 6 knew it wasn't transporting from the experiments we did 7 here, and we were curious to know if the binding site had 8 changed. In this experiment, we're competing the binding 9 of the radiolabeled ligand with increasing concentrations 10 of norepinephrine, shown on the x axis. We can see that 11 the wild type is the curve to the left, and we can see 12 that norepinephrine is able to compete off the RTI-55 and 13 that the A457P curve, which is shown to the right, has 14 shifted to the right, indicating a decrease in the ability 15 of norepinephrine to compete off the radioligand, 16 suggesting that it had lost some affinity, although it 17 does seem to bind to the transporter. 18 So we knew that we had, therefore, a transporter 19 that had some -- we knew there was some protein expression

20 from the membrane binding and that it had some ability to 21 bind norepinephrine, although there was really a complete 22 lack of transport. So we decided to use Western analysis 23 with specific antibodies to the transporter to look at the 24 actual protein expression in these cells. 25 A shows you a typical Western blot analysis. 0181 1 What you see on the left is extracts from cells that are 2 run on a gel and then blotted with an antibody that binds 3 to the transporter. And in untransfected cells, you see 4 no signal. And if we look at the hNET wild type, you see 5 several dark bands on this gel. These are all 6 norepinephrine transporter, and there are several 7 different sizes because, as I mentioned earlier, the 8 protein has the ability to be glycosylated. What we've 9 shown in our lab previously is that these lower bands 10 around 56 kilodalton are a glycosylated form that happens 11 initially, probably in the ER, and then this higher 12 molecular weight form, between 80 and 100 kilodaltons, is 13 a further processed glycosylated form. 14 If we look at the hNET A457P, we see that 15 there's a lot of this lower form, but there really is a 16 great decrease in this higher molecular weight form. So 17 although the A457P is making protein, it seems to not be 18 making this higher glycosylated form as much as the wild 19 type. 20 On the right, where I have surface expression, 21 we've used cell impermeant biotinylating reagents which 22 can label the surface proteins of a cell, and then we 23 collect those on streptavidin beads, and we can look and 24 see how much of that transporter that was made is actually 25 on the surface of the cell because we know we have a lack 0182 1 of transport and we're trying to understand the reason 2 why. 3 You can see in the wild type NET that you get a 4 large amount of the 80 to 100 kilodalton form on the cell 5 surface. And we've shown in our lab previously that this 6 is the case, that this larger form, or the fully 7 glycosylated form, is the form that's expressed on the 8 surface and is, therefore, responsible for the transport 9 of norepinephrine. 10 And the A457P again is diminished in this 80 11 kilodalton form, as it was in the totals, but this just 12 emphasizes that that form is, in fact, diminished on the 13 cell surface. And that's just graphically represented in 14 B that there's a decrease in the mature form of the 15 protein, both in the totals and on the cell surface. 16 So what I've told you thus far is that if we 17 compare in C, if this is just wild type activity in the 18 blue bar, and we compare various features of A457P to 19 that, you can see that we have a decrease in the amount of 20 protein present, as indicated by binding, Western 21 analysis, and wholesale binding, which I didn't show 22 today, and that even though there is some protein that is 23 being expressed on the surface of the cells we've measured 24 by these biotinylation studies, even that protein is

25 inactive because the uptake is much less, less than 1 0183 1 percent, virtually not there. 2 So being we had a protein that was -- some of 3 the protein was present, although it was a nonfunctional 4 transporter, we became very interested in whether or not 5 we would see a dominant negative interaction of the mutant 6 on the wild type protein. Just by way of review, a 7 dominant negative interaction would mean that the mutant 8 not only loses its function but interferes with the 9 function of the normal allele that is present. So this 10 would be very important in a disease with features of 11 heterogeneity. 12 Now, a dominant negative should, therefore, 13 cause a more severe phenotype than if the gene were 14 completely deleted or the protein not expressed at all. 15 So if it wasn't there, it wouldn't be able to interfere 16 with the normally functioning allele. 17 Finally, a physical association of the normal 18 and the mutant protein forms is a potential mechanism for 19 this to occur. So the way in which a mutant protein could 20 influence the wild type function would be if they existed 21 in some kind of complex together and the mutant couldn't 22 interfere with the wild type. 23 And in order to examine this, what we did was we 24 put tags in the amino terminus of the protein, tags that 25 could be identified with unique antibodies because, 0184 1 remember, the mutation that we have here is only different 2 from wild type NET by one amino acid. So in order to look 3 at the wild type and the mutant together in the same cells 4 to look for dominant negative interactions, we have tags 5 in the amino terminus, either a His tag or an HA tag that 6 can use different antibodies. 7 What we found when we did this was that if we 8 co-expressed the mutant and the wild type together, which 9 is shown here at the bottom of the graph -- that's just 10 the amount of DNA that is transfected into the cells, and 11 it's either wild type or A457P. And the y axis is showing 12 you the tritiated norepinephrine uptake. You can see that 13 we have a certain amount of uptake for the wild type 14 transfected alone, and when we transfect that with the 15 mutant, there is actually a decrease in the uptake 16 compared to that same amount of wild type transfected 17 alone. And the only difference now is the presence of the 18 mutant. 19 And in part B, we see another Western blot 20 analysis that mirrors the experiment in A. The wild type 21 here is labeled with that HA tag, and now we use an 22 antibody that only recognizes that tag on the Western. 23 And so what we're looking at here is the wild type 24 expression and not the mutant, wild type alone. And we're 25 looking at it in a biotinylation experiment. So we're 0185 1 looking at what's on the surface of the cell. 2 What we can see here is that under the same 3 conditions, wild type expressed alone gives you this

4 amount of protein on the surface, and when it was co- 5 expressed with the mutant, in fact, the wild type 6 expressed on the surface actually decreased. 7 And this next lane on the gel shows you that 8 when we transfect twice the amount of wild type, that we 9 actually do get an increase in wild type, when we double 10 it, compared to this first lane. And that's graphically 11 represented here, showing you that again the mutant can 12 decrease the wild type surface expression and that 13 transfecting even more wild type in does increase the 14 surface expression. And that indicates to us that we're 15 not just saturating either some machinery in the cell for 16 making the protein or trafficking it because we can get 17 more expression when we double the amount of DNA. So this 18 said to us that there was, in fact, a dominant negative 19 interaction. 20 Next we wanted to look at whether or not there 21 was a physical association between the proteins. And it's 22 been shown for many G-protein coupled receptors and also 23 recently it has been shown for transporters in this gene 24 family that the proteins do exist in oligomeric complexes. 25 So our next experiment was to look to see if NET existed 0186 1 in a complex, and one way to do that is to try to co- 2 immunoprecipitate the two proteins. So, again, you're 3 using differentially tagged NETs, and if one tag 4 precipitates the other, then the proteins are together in 5 a complex. 6 So what we did here was to, again, transfect 7 cells with the DNA shown on the bottom of the graph. The 8 first two lanes just show you controls, showing that 9 either when the wild type or the A457P was transfected 10 alone separately and subjected to immunoprecipitation, 11 there was no signal on the blot which was to be expected. 12 When the two differentially tagged His hNET or 13 HA hNET were transfected together -- and I'm just showing 14 you wild type in this gel. I'm sorry. I forgot to 15 indicate that. The evidence of NET in a complex hadn't 16 been shown before. So prior to looking at the mutation, 17 we needed to look at the wild type. What in fact we saw 18 was that we could co-immunoprecipitate the protein. 19 And I'll just quickly show you that in part B. 20 When we repeated the experiment, if we look at the 21 immunoprecipitated lanes, the first lane showing wild 22 type/wild type and the second lane now showing mutant and 23 wild type interaction, in fact the A457P can 24 immunoprecipitate the hNET wild type, showing that these 25 could exist together in a complex and be responsible for 0187 1 the dominant negative effects that we saw. 2 And that's just all summarized here. The 3 important take-home message from this really is that 4 individuals that have a heterozygous mutation for hNET, 5 such as the OI family, might actually have less than 50 6 percent of the normal NET capacity if dominant negative 7 mutations are involved. 8 And I'll just end there and I won't have time to
9 read the people, but to acknowledge the people who have 10 contributed either in our lab or in David Robertson's 11 group to this research. Thank you. 12 (Applause.) 13 DR. GOLDSTEIN: Of course, in between alleles 14 and genetic mutations are polymorphisms, and I think 15 there's been an explosion of information about genetic 16 polymorphisms. This certainly applies to autonomic 17 regulation, and Steve Liggett will give us an update about 18 that. 19 DR. LIGGETT: Thank you. I'm going to go ahead 20 and get started while things warm up here. 21 I want to make sure we're all on the same page 22 here in terms of definitions. A polymorphism I'm going to 23 define here as genetic variant which occurs at a frequency 24 of 1 percent or greater in the population. This really 25 differs from what we've been talking about over the last 0188 1 few hours which are mutations which are very uncommon and 2 typically are sufficient to cause the disease. In 3 contrast, polymorphisms are occurring throughout the 4 population of apparently normal individuals. They're 5 present in this room amongst us, and the intriguing 6 concept is that they may modify diseases or perhaps in 7 concert several of them that have significant impact on a 8 protein function together might lead to a substantial risk 9 of a disease. But individually they may not be such 10 powerful predictors. 11 So today I want to go over with you the work 12 that we have done on adrenergic receptor polymorphisms. 13 Now, why have I picked that? Well, I think that's pretty 14 obvious that the adrenergic receptors, both the alpha 1 15 class, the alpha 2 class, and the beta adrenergic 16 receptors, are all critical for homeostasis and are a 17 major limb in the sympathetic part of the autonomic 18 nervous system which has already been described. 19 So in doing these types of studies, I want to 20 emphasize that we have been very careful, as shown by the 21 previous speaker, not to simply find a single nucleotide 22 polymorphism, sometimes called SNP, and then go do an 23 association study and then be happy if we see some sort of 24 weak association. We think that's bad science. Our 25 approach has been rather, if we find a polymorphism, to 0189 1 build it, put it into cells, study its pharmacology and 2 its biology, and if in fact there is a difference in the 3 pharmacology, then we'll pursue it in an appropriately 4 hypothesis-based clinical study. 5 So these are the receptor subtypes that I'm 6 going to talk about, and I want to just quickly remind 7 everyone of the coupling pathways. The alpha 2 receptor 8 is coupled to GI. They inhibit adenylyl cyclase. The 9 beta receptor is coupled to GS. They stimulate adenylyl 10 cyclase. There are three members of the beta receptor 11 family. There are three members of the alpha 2 receptor 12 family. There are three members of the alpha 1 family 13 which couple to GQ and couple to phospholipase C.

14 Interestingly enough, there is one polymorphism 15 in the alpha 1B receptor. We don't know about these two, 16 and this doesn't appear to do anything. So I'm going to 17 concentrate on these two families in particular. I 18 thought the best way to approach this was to simply march 19 through the receptors and show you what their phenotypes 20 are, not spend a lot of time on why the particular 21 polymorphism does what it does -- those are in the papers 22 -- and then show you a straightforward hypothesis-based 23 study which will show you the power of polymorphisms, 24 particularly when they are in combination. 25 So the alpha 2A receptor is a centrally 0190 1 localized receptor also found in the peripheral 2 sympathetic nervous system and there is one polymorphism 3 that we have found that is very rare. It occurs in .4 4 percent of whites and 4 percent of African Americans. And 5 it is a substitution of lysine for a spare gene at this 6 position in the third intracellular loop. 7 The phenotype of this receptor, when put into 8 Chinese hamster ovary cells, is interesting in that it's a 9 gain of function. So individuals who have this receptor 10 would have an increased function of the alpha 2A receptor. 11 That's shown here as an increase in the ability to inhibit 12 adenylyl cyclase. And this is both with the endogenous 13 catecholamine as well as a synthetic drug. 14 Now, interestingly, the signals sometimes are 15 much greater -- the phenotype is much greater depending on 16 which signal you look at. So the alpha 2 is also coupled 17 to MAP kinase, and you can see the gain of function with 18 this lysine 251 polymorphism is actually quite striking 19 when you look at this signal as compared to inhibition of 20 adenylyl cyclase. 21 Nevertheless, this is relatively rare, and in 22 the work that I work with hypertension, heart failure, and 23 asthma, it probably wasn't going to be a player. 24 Now, to the alpha 2B's. These receptors are 25 localized both centrally and peripherally as well. Here 0191 1 the allele frequency is 31 percent in caucasians and 12 2 percent in African Americans, and it consists of a 3 deletion of three glutamic acid residues right in the 4 middle of a known region of phosphorylation by G-protein 5 coupled receptor kinases which are important for 6 desensitization of the receptor. 7 I will tell you this is actually a 7 8 transmembrane receptor, but for clarity I'm just showing 9 the areas where the polymorphisms occur. 10 So for this polymorphism, when these were 11 expressed, these receptors were expressed in CHO cells. 12 You can see that in fact we have a minor decrease in the 13 ability to inhibit adenylyl cyclase with the polymorphic 14 receptor, fairly small, a little rightward shift in the 15 dose-response curve, but not very impressive. 16 But as I said to you before, this area is very 17 important in the receptor for phosphorylation by G-protein 18 coupled receptor kinases which is involved in agonist-

19 promoted desensitization. So we looked at this particular 20 property and found that wild type alpha 2B receptors 21 undergo about a 50 percent desensitization after 15 22 minutes of exposure to norepinephrine in the culture dish, 23 whereas the deletion polymorphism receptors do not at all. 24 In fact, the phosphorylation of the receptor when purified 25 using epitope-tagged receptors is substantially less in 0192 1 the deletion 301 through 303 polymorphic receptor. 2 So the phenotype of this receptor is one of some 3 uncoupling, but particularly a lack of desensitization. 4 And desensitization is a critical mechanism for 5 homeostasis in most G-protein coupled receptor systems and 6 is important for sort of integrating all these signals 7 that are coming into the cell. 8 Now, the alpha 2C receptor. I will show you a 9 lot about where this is and what it does. It's localized 10 both centrally and in the peripheral presynaptic 11 sympathetic nerves. There is a single polymorphism that 12 we have found which consists of a deletion of a GAGP again 13 in the third intracellular loop. It's sort of interesting 14 that all known polymorphisms of the alpha 2 receptors are 15 in the third loop of the three subtypes. 16 This occurs with a frequency of only 4 percent 17 in caucasians but 40 percent in African Americans, and 18 this is one of the biggest differences that we've seen in 19 coding block polymorphisms of any of the G-protein coupled 20 receptors. This receptor is markedly uncoupled. 21 So this is again a read-out of inhibition of 22 forskolin-stimulated adenylyl cyclase. These are 23 transfected equal levels in CHO cells, and you can see 24 that there's this marked inability to inhibit. It's 25 almost dead really. The lower we go in expression towards 0193 1 a more physiologic level, we essentially see no response 2 at all. 3 Now to the betas. I know this is fast, but 4 there's a story in the end, and one of the important 5 things that I think we need to realize, as disease 6 modifiers this group ought to be looking at these 7 receptors and these polymorphisms because they have a 8 marked physiologic effect, which I'll show you in a 9 moment. 10 So the beta 1 receptor, as you know, is 11 localized primarily on the heart, on the myocyte, 12 responsible for increased contraction as well as rate. 13 There are two polymorphisms. The one I want to 14 concentrate on is the substitution of arginine for glycine 15 at position 389. The allele frequencies are fairly 16 common, as high as 42 percent in African Americans. And 17 this polymorphism results in a gain of function. So the y 18 axis here is adenylyl cyclase either presented as absolute 19 levels, or as a percent forskolin, you can see that the 20 Arg389 receptors are clearly sort of a hyperfunctional 21 receptor. They stimulate to a much greater degree, either 22 absolute levels or fold stimulation over basal. So you're 23 beginning to see that these polymorphisms have a lot of

24 different phenotypes. 25 The beta 2 receptors I won't go into in detail. 0194 1 We've published a fair amount in Asthma on these. It's 2 interesting to note that there are four polymorphic sites 3 in the beta 2 receptor, really only three of which occur 4 with any frequency you can find. And most interesting I 5 think is this Ile164 polymorphism which I have down here, 6 having an allele frequency of 5 percent, but that's 7 actually the allele frequency of heterozygotes. We've 8 never found a homozygous individual -- and we've looked at 9 over 10,000 now -- who is homozygous for Ile164. 10 And this receptor is, in fact, pretty 11 dysfunctional as well. Lower basal activity of adenylyl 12 cyclase and lower maximal stimulation. Probably since 13 it's expressed in lungs and it's required for removal of 14 lung water at the time of birth, the homozygous 15 individuals do not come to term or die shortly thereafter. 16 From a resolution standpoint, this is pretty 17 hard to read and it's not important, so I'm going to let 18 it go, but just to tell you that the position 16 and 27 19 polymorphisms of the beta 2 receptor actually affect more 20 the loss of receptor number after prolonged agonist 21 exposure as compared to these short-term events that I've 22 showed you just recently. 23 So I put this slide up here to now give you an 24 idea of where I think the usefulness of these 25 polymorphisms can be. I've mentioned before that they 0195 1 might be risk factors. I've also said that they might 2 have something to do with response to therapy because we 3 do use a lot of adrenergic receptor agonists and 4 antagonists for treatment. 5 But because of their relatively high frequency, 6 one of the concerns has been -- and I actually got this 7 from a fair number of classic geneticists -- this notion 8 that, well, since they're common, they probably don't do 9 anything, which was a little discouraging back in the 10 early days. 11 I would modify that in thinking another way, and 12 perhaps this is a little more true. If they're common, 13 they probably have a small effect, and if they're rare, 14 they might have a big effect. So common polymorphisms 15 which have been allowed to exist through evolutionary 16 time, if they have a big effect, it was for a specific 17 survival reason. If they're sort of a negative effect 18 overall, they probably shouldn't be common anymore. 19 So I'm going to give you an example, though, of 20 where you have two fairly common polymorphisms. Both have 21 effects in cells but, when together, can give you a major 22 physiologic effect. 23 So I want to talk about heart failure, and 24 there's a hypothesis that's generated over a number of 25 years, both in animal and human studies, that prolonged, 0196 1 persistent activation of cardiac beta receptors results in 2 hypertrophy or heart failure regardless of what the

3 initial insult is. So it could be some ischemia, a little 4 myocarditis, or hypertension, or the so-called idiopathic 5 forms. But nevertheless, persistent activation is bad. 6 And that's why beta blockers actually paradoxically work 7 in congestive heart failure where you would think they 8 might not. They tend to relieve the heart of this 9 persistent norepinephrine that is present because the 10 cardiac output is low and the body is trying to increase 11 its cardiac output. 12 Well, it turns out that the alpha 2C receptors 13 inhibit norepinephrine release at low stimulation 14 frequencies in the cardiac presynaptic nerve. This is 15 what we believe to set sort of the basal or all-day-long 16 norepinephrine secretion. The alpha 2A's inhibit 17 norepinephrine at high stimulation frequencies, so this 18 would be an acute response. 19 Now, we also know that the beta 1 receptor is 20 the primary cardiomyocyte beta receptor, and if you begin 21 to think about this, we have the makings of an issue here. 22 In mice I can tell you that knocking these two receptors 23 out results in uncontrolled norepinephrine release and 24 heart failure. 25 And I'm going to show you the mouse data now 0197 1 with the two beta 1 polymorphisms very briefly. When we 2 built these mice, we studied them in vivo, and you can see 3 that at 3 months, the Arg389 beta 1 polymorphism mice, 4 which is the hyperfunctional mice, have this enhanced 5 basal and dobutamine-stimulated contractility. The Gly 6 mice are somewhere in between, and these are non- 7 transgenic. So these are equally expressed. 8 However, by 6 months, these Arg389 mice have no 9 response to infused dobutamine whatsoever, and this is 10 sort of a hallmark in human heart failure, the lack of 11 beta receptor responsiveness. Indeed, when we looked by 12 echocardiography by 9 months of age, the Arg389 mice have 13 a significantly decreased fractional shortening as 14 compared to the Gly389 mice. And on microscopy, they show 15 extensive fibrosis, myocyte dropout, and hypertrophy, no 16 apoptosis, interestingly enough, while the Gly389 mice are 17 indistinguishable, so non-transgenic. So we considered 18 that Arg389 might be a predisposing polymorphism for heart 19 failure. But, of course, that's not really the whole 20 picture. 21 This is a presynaptic nerve here, and the 22 overall hypothesis would really be that you need both this 23 alpha 2C polymorphism and the beta 1 in order to have a 24 substantial risk for heart failure. And the reasoning, 25 once again, would be as follows. 0198 1 If you have the alpha 2C Del322 through 325, you 2 have decreased function, therefore increased 3 norepinephrine release at the synapse. At the same time, 4 if you have the beta 1 Arg389, which by itself has 5 increased function and would have increased response at 6 the cardiomyocyte, but is then exposed to the increased 7 norepinephrine as well, it would have this synergistic

8 interaction and potential heart failure. 9 So we did look at a study which is going to come 10 out next week which looked at controls in heart failure 11 patients. We genotyped at these two loci. We did adjust 12 for age, sex, hypertension, and diabetes, which was really 13 not necessary. It was very clear. And because the allele 14 frequencies are quite different between African Americans 15 and caucasians and we did not want to deal with population 16 stratification per se, we carried out the analysis 17 separately for each ethnic group. And I'm just going to 18 show you African Americans today because that's when the 19 allele frequencies are high enough that we had enough 20 power to show something. 21 So now, our normals are squeaky clean normal, 22 and in the heart failure patients, just for those who are 23 interested in phenotypes, there's no doubt they have heart 24 failure. We're not talking about partial phenotypes or 25 sort of questionable diagnosis here. Heart failure is one 0199 1 of those things, when you see it, you know it. And their 2 ejection fractions were around 25 percent which is quite 3 low, and most of them had class III/IV symptoms. 4 So you can see there's a substantial over- 5 representation of the homozygous deletion alpha 2C 6 polymorphism in heart failure. Indeed, 53 percent of 7 heart failure patients were homozygous for this 8 polymorphism compared to only 16 percent of normals. So 9 in fact, the odds ratio is 5.65 with this really nice p 10 value of 0.0001. So in and of itself, the alpha 2C Del322 11 through 325 is a risk factor for heart failure. 12 What about the beta 1? Well, here we don't 13 really see much difference in the allele frequencies, 14 either homozygous Gly, homozygous Arg, or the heterozygous 15 individuals, between normal and heart failure subjects. 16 So there's no risk associated with having heart failure if 17 you have the beta 1 389 polymorphism. 18 But what if you have both? So, as I've shown 19 before, the deletion has an odds ratio of 5.65. The beta 20 1, there's no risk. If you have both, the risk is 10.1 21 with a p value of 0.004. This is, to my knowledge, the 22 highest known genetic risk factor for what we have 23 previously called garden variety or idiopathic dilated 24 cardiomyopathy. 25 So our conclusions are that alone the alpha 2C 0200 1 receptor is a risk factor for heart failure, but alone the 2 beta 1 Arg389 is not. However, together they represent a 3 tenfold risk for heart failure. We think this synergism 4 is consistent both with the transfected cells that I 5 showed you, the gene modified mice that I showed, and this 6 sort of series circuit where you have norepinephrine being 7 released and acting on its receptor. 8 So how can we put this together with what we're 9 talking about today? As we discussed -- and we could 10 spend a long time talking about which adrenergic receptor 11 is localized on which tissue and what the exact circuit 12 is, but it's clear that they are important. It turns out

13 that most of them are polymorphic in so-called normal 14 populations, and that means they're also polymorphic in 15 dysautonomic populations. Whether they are causing it or 16 having an effect on it would be up to a clinical study to 17 determine. 18 We have the opportunity to know that their 19 biologic properties have been characterized in cells in 20 gene-modified mice. So you would have the opportunity at 21 the beginning of your study, if wanted to look, for 22 example, for gene modifiers that sort of direct the 23 phenotype in a familial dysautonomic syndrome, you'd have 24 an idea of how to design the study, gain of function, loss 25 of function, agonist affinity, antagonist affinity, 0201 1 response to drugs. All these can be taken into 2 consideration in designing the clinical trial. 3 And these phenotypes include virtually 4 everything that you can imagine about a receptor, the 5 ligand binding affinities, the coupling of the receptor to 6 the G-protein. I didn't show this but expression of the 7 receptor can be altered by polymorphisms in the promoter 8 region as well as regulation of the receptor over long- 9 term stimulation. So all this has to be taken into 10 account. 11 So I would propose that we need to consider 12 adrenergic receptor polymorphisms possibly in some sort of 13 combination as potential causes or modifiers of 14 dysautonomic syndromes. 15 Thank you. 16 (Applause.) 17 DR. GWINN-HARDY: Let's take a 15-minute break 18 and come back at 3:30. 19 DR. GOLDSTEIN: After the break, Italo Biaggioni 20 will give his talk, and then we'll go right into the 21 discussion. 22 (Recess.) 23 DR. GOLDSTEIN: I want to announce to you 24 briefly, in terms of the scheduling sequence, after Dr. 25 Biaggioni's talk, because of time constraints, we will 0202 1 start with questions for Dr. Liggett. He has to leave a 2 bit early. And then we'll continue with more general 3 questions after that. 4 Dr. Italo Biaggioni is a professor of medicine 5 and pharmacology at Vanderbilt, and he'll be talking about 6 hypertension in autonomic disorders: genetic factors and 7 phenotyping. 8 DR. BIAGGIONI: Thanks, David. We're running a 9 little bit behind schedule. I'll try to be brief. 10 I don't need to introduce the autonomic nervous 11 system to this group, but just to simplify things -- and 12 this is a very simplified scheme. So don't write letters 13 if you find anything that is not correct. 14 There's an afferent portion of it that senses 15 what blood pressure and other many things are doing in the 16 body second by second, central sites where all this 17 information is integrated, and then efferent sites where

18 sympathetic tone is actually delivered to the rest of the 19 body. So problems in any one of these sections can lead 20 to autonomic disorders, and let me focus here on the ones 21 that will produce high blood pressure. 22 The obvious one is if you have an alteration in 23 the afferents, you would lose your ability to buffer all 24 the changes in blood pressure and you actually have labile 25 high blood pressure. 0203 1 The importance of this receptor has been known 2 for a number of years, and in humans they became clear in 3 this study done in the '50s which I doubt that we will see 4 any such clinical research anymore. But this group of 5 investigators actually -- they used themselves as normal 6 subjects, and when they blocked afferents by injecting 7 lidocaine I believe in the neck on themselves, they saw 8 that blood pressure increased by 20 millimeters of mercury 9 if they did one site. Not happy with that, they did both 10 and then blood pressure increased over 200 systolic, and 11 heart rate increased. Again, not happy with that, they 12 studied patients with high blood pressure, and as you can 13 see, they get huge increases in blood pressure. And they 14 studied then patients with severe hypertension and, you 15 know, I don't think our instruments would record those 16 blood pressures anymore. 17 So, obviously, these are very important 18 baroreceptors that inhibit sympathetic tone, and there are 19 patients who have damage of this afferent usually as a 20 consequence of surgery. The most common of them, of 21 course, neck cancer and paragangliomas, are transmitted in 22 families. And the characteristic is severe labile 23 hypertension together with increases in heart rate and 24 blood pressure and plasma norepinephrine. Those are 25 triggered by stress, pain, and mainly because they have 0204 1 absence of this baroreflex modulation. 2 This is just one example of a patient in this 3 case with a cold pressor test. We tend not to do those 4 anymore. But even if you start talking to them or if you 5 turn on the lights, you will see this huge increase in 6 blood pressure. This patient was originally described by 7 David Robertson. So very minor stimuli that we could 8 handle all the time in these patients will produce a 9 hypertensive crisis not unlike what Felicia has described 10 in the familial dysautonomia patients. 11 Well, these afferents actually have their first 12 in the synapse in the NTS, and the NTS actually inhibits 13 sympathetic tone. So it provides inhibitory input to the 14 RVLM where pacemaker neurons are believed to be located. 15 And for many years also, people have lesioned the NTS in 16 animals to produce a very similar clinical picture to the 17 one I described. 18 You know, we were unlucky to see a patient with 19 a similar problem with an NTS lesion. Of course, the 20 problem then is the cortical stimuli, the stress and 21 everything will drive hypertension. And this is 22 unfortunate pathology of this patient showing two holes
23 actually where the NTS should be. This is most commonly a 24 familial disorder. In this case it was not, but it shows 25 you the importance of the NTS in inhibiting sympathetic 0205 1 tone. Again, in this patient, handgrip or cold pressor 2 test produces profound increases in blood pressure, and 3 there was complete absence of baroreflex mediated heart 4 rate changes. 5 David already mentioned the other part of the 6 autonomic problems, that is the central and efferent 7 problems, multiple system atrophy. There are lesions in 8 the brainstem nuclei, in the basal ganglia, and also in 9 the pathways that control sympathetic tone. We believe, 10 for reasons that I'm going to explain later, that the 11 actual pacemaker neurons are intact, the neurons on the 12 RVLM. Unfortunately, we don't have still very good 13 neuropathology of that, but we believe that to be the 14 case. But still, they are not able to regulate 15 sympathetic tone, and every time they stand up, they have 16 orthostatic hypotension. 17 There's also another group of patients with pure 18 autonomic failure who actually have central problems, but 19 clinically they don't. Perhaps in later stages they do, 20 but clinically we tend to believe that they have no 21 central neurological problems, but clearly they have loss 22 of peripheral nerve and again they have orthostatic 23 hypotension, their main symptom. And that really 24 dominates the clinical picture of these patients. They 25 don't have as much GI side effects, for example, but they 0206 1 have a lot of orthostatic hypotension. That's the reason 2 why they come to us. 3 And that is shown here. That's normals, 4 systolic/diastolic blood pressure and normal response to 5 posture. And these are patients with pure autonomic 6 failure or multiple system atrophy, and you can see this 7 profound orthostatic hypotension. 8 Like David showed, norepinephrine is very low in 9 pure autonomic failure patients. They do not respond very 10 well. They respond very slightly to upright posture, but 11 that's due to decreased clearance and not really to 12 increased production. Patients with MSA have near normal 13 plasma norepinephrine, but fail to respond appropriately 14 on standing. 15 Now, the other thing I would like to point out 16 is even though orthostatic hypotension predominates 17 clinically, as you can see, these patients actually have 18 supine high blood pressure, not unlike, again, the 19 patients with familial dysautonomia. 20 I just will show you the blood pressure 21 distribution in these patients. This is a number of 22 patients we've collected throughout the years. Supine 23 systolic blood pressure, diastolic blood pressure. So if 24 you define hypertension as blood pressures above 150 over 25 90, about half of the patients have supine hypertension. 0207 1 We've been interested in dissecting why patients

2 without a functioning autonomic nervous system might have 3 that supine hypertension. To make a long story short -- 4 and David has already mentioned some of that -- we believe 5 that in multiple system atrophy, the lesion is proximal to 6 the pacemaker neurons that actually produce sympathetic 7 tone. However, they cannot modulate it. So even though 8 the sympathetic tone is there, it's working on idle, if 9 you wish. They cannot rev it up. So the evidence for 10 that has been the normal or only mildly decreased plasma 11 norepinephrine, and again, David's studies elegantly show 12 that the sympathetic nerves in the heart were able to 13 uptake catechols. 14 So we decided to test the hypothesis that the 15 supine hypertension was also due to that leftover 16 sympathetic tone, and that will be the case in MSA but not 17 in pure autonomic failure which we believe is actually 18 distal to the origin of sympathetic tone. 19 To test that hypothesis, we used a ganglionic 20 blockade with trimethaphan to interrupt any remaining 21 sympathetic tone they may have. So again, our bias is, 22 our hypothesis is that the pacemaker neurons that produce 23 sympathetic tone -- and by the way, they may not be in the 24 RVLM. They might be in the spinal cord as well. Those 25 are intact. These patients have residual sympathetic 0208 1 tone, but there's an interruption on the pathways that 2 control that, so they cannot control that. If we block 3 ganglionic transmission with trimethaphan, any residual 4 sympathetic tone will go away and we'll be able to see if 5 their hypertension is due to that. 6 But in patients with pure autonomic failure 7 whose lesion is distal to the origin of sympathetic tone, 8 then there's nothing to block and nothing much will happen 9 in them. 10 Indeed, again to make a long story short, that's 11 what happened with trimethaphan at very, very tiny doses. 12 In patients with multiple system atrophy, they had a 13 profound drop in blood pressure, almost 70 millimeters of 14 mercury on average. So that means that in some patients 15 it was more like 100. And in patients with pure autonomic 16 failure, they did have some decrease in blood pressure, 17 but not nearly as much as patients with multiple system 18 atrophy. 19 And this is one example, a patient with Shy- 20 Drager who started with a systolic of 200 and with tiny 21 doses that would do almost nothing to a normal subject, he 22 has a profound decrease in blood pressure with now a 23 systolic of below 100. This study was done with Jens 24 Jordan who used to be here, but probably had better things 25 to do than hear my talk. 0209 1 (Laughter.) 2 DR. BIAGGIONI: So I think these and other data, 3 together with David and other labs, do show that in 4 multiple system atrophy, the hypertension is centrally 5 mediated and is due to residual sympathetic tone, most 6 likely acting on denervated hypersensitive receptors,

7 although that may be questionable, and unrestrained by the 8 absence of the baroreflex. 9 In pure autonomic failure, it's still an open 10 question as to what's driving in their hypertension, and 11 whether familial dysautonomia will fit under one or the 12 other I think is not completely known. In pure autonomic 13 failure, the question is more complicated and we don't 14 know yet. 15 Here we're comparing normal with pure autonomic 16 failure patients without hypertension and pure autonomic 17 failure patients with hypertension. And as you can see, 18 both have profound orthostatic hypotension. 19 Norepinephrine is equally impaired in both. You can argue 20 that it's marginally worse in the ones with hypertension. 21 And renin is, if anything, worse in those with 22 hypertension. So we don't believe it's renin. We don't 23 believe it's residual sympathetic tone. ________ is the 24 same. Does that mean that peripheral resistance is 25 increased? 0210 1 So the challenge here is to find what is driving 2 that increased vascular resistance. We know that it is 3 not renin. We know that it is not norepinephrine. We're 4 studying other factors. 5 But back to our point, what lessons can we 6 derive from these patients? I believe that these are 7 models of sympathetically mediated hypertension, and the 8 fact that sympathetic tone can drive sustained 9 hypertension I think is remarkable. In the field of 10 hypertension, we've been focusing on the kidney and for 11 very good reasons. But this just shows you that 12 sympathetic tone can actually also drive sustained 13 hypertension, whereas in pure autonomic failure patients, 14 it's a model of completely independent hypertension of 15 sympathetic tone. 16 Now, in essential hypertension, of course, there 17 is a lot of evidence that there is some genetic component 18 of that, and the monogenic hypertension has been 19 described. Most of those have been due to kidney 20 problems, but in essential hypertension I think there's a 21 lot of evidence that abnormalities in sympathetic tone are 22 segregated in a familial way. For example, in African 23 Americans, they responded in an exaggerated way to 24 sympathetic stress. If you do cold pressor tests, there's 25 a greater increase in sympathetic activation with those 0211 1 stimuli, and that's transmitted in families. 2 We know that hypertension goes along with 3 impaired baroreflex function. There's nothing new about 4 that. But even normotensive siblings or children with 5 hypertensive parents have already impaired baroreflex 6 function, and that's also transmitted in a familial 7 pattern. 8 I will not talk about polymorphism. Stephen, 9 I'm sorry. This is a slide made, about a year old. Every 10 time you make a slide, it becomes obsolete. 11 (Laughter.)

12 DR. BIAGGIONI: This is a very rapidly changing 13 field. And I agree completely with you that a lot of the 14 studies of associations have been done without much 15 thought of the cellular phenotype of these. So there's a 16 lot to learn in this field I'm afraid. 17 But the bottom line is that in essential 18 hypertension, there is a component of genetic autonomic 19 function, and this is a field that is going to advance 20 very quickly. At the same time, I'm afraid that the 21 phenotyping we do in patients is not advancing at such a 22 great a degree. A lot of the problems we have in these 23 association studies is that they take all new-comers, 24 essential hypertensives that have nothing to do with 25 autonomic problems and essential hypertensives that may 0212 1 have a greater autonomic component and not an easy way to 2 segregate between both of them. 3 So how do you phenotype for sympathetic 4 function? The traditional way has been plasma 5 norepinephrine, a very useful marker but not a very 6 sensitive one, and David has run very good reviews or 7 meta-analysis on that. Norepinephrine spillover is a much 8 refined technique, but again very difficult to implement 9 on a population basis. 10 The same is true of microneuropathy. Very 11 important, very powerful, but again difficult to do on a 12 population basis. 13 So we've been looking at spectral analysis of 14 blood pressure fluctuations as an alternative to do this 15 phenotyping. And I'm not here to try to sell that as the 16 best technique, because clearly we have to do more work on 17 that. 18 But just to say a word in terms of spectral 19 analysis, I think most people will agree that high 20 frequency variability of heart rate is an indicator of 21 parasympathetic modulation of heart rate. But there's a 22 little bit more controversy about low frequency 23 variability of blood pressure, and I believe that it has 24 limitations, but I'll show you some data showing that 25 perhaps it is a measurement of sympathetic modulation of 0213 1 vasomotor tone. 2 So normally blood pressure fluctuates in a 3 rhythmic pattern, and you can analyze that in spectral 4 analysis. And it actually goes along with sympathetic 5 nerve traffic measured here with MSNA, and sympathetic 6 nerve traffic is also not continuous. It comes in bursts. 7 That tracks nicely with variability in blood pressure with 8 a lifetime, of course. 9 Now, if you stand up and you increase 10 sympathetic tone, this variability becomes more 11 pronounced, as well as the burst of sympathetic 12 activation. So you can analyze either or both with 13 spectral analysis techniques. 14 So we decided to put that as a test. Again, 15 we're using our ganglionic blocker, the idea being that if 16 low frequency oscillations of blood pressure are a marker

17 of sympathetic tone, if you wipe out sympathetic tone, you 18 will wipe out oscillations of blood pressure. 19 Again, we used as our positive control patients 20 with multiple system atrophy, which we've already shown 21 they are sympathetically mediated, and as a negative 22 control, patients with pure autonomic failure, patients 23 which again don't have much sympathetic tone left. 24 I just will show you that trimethaphan is 25 actually very effective in wiping out the autonomic 0214 1 function. Here we're looking at baroreflex sensitivity, 2 and we're looking at patients with pure autonomic failure 3 who already have almost no baroreflex sensitivity. 4 Patients with Shy-Drager, multiple system atrophy, also 5 have very low levels. So in them trimethaphan will do not 6 much. Normotensives have a normal baroreflex function, 7 and hypertensives have been shown over and over again to 8 have impaired baroreflex function, and that's shown here. 9 With trimethaphan, you can also wipe that out. So, it's a 10 very effective way of eliminating any remaining autonomic 11 tone. 12 Let's concentrate on low frequency oscillations 13 of blood pressure. Here we see pure autonomic failure 14 patients within the noise level. So they have very low 15 oscillations, and this also shows you that the limitation 16 of this technique is that it's very hard to show a 17 decrease in sympathetic function using this technique 18 because levels lower than 1.52 are really noise. But if 19 you have normal subjects, shown here in the circles, you 20 can also reduce that with this drug, with a ganglionic 21 blockade. 22 Now, in patients with multiple system atrophy, 23 who have profound orthostatic hypotension but we've been 24 postulating have residual sympathetic tone, they have 25 actually increased oscillation, together with patients 0215 1 with hypertension. So these are patients with supine 2 hypertension and Shy-Drager and patients with essential 3 hypertension, and both have increased oscillations in 4 blood pressure and both can be abolished by a ganglionic 5 blockade. 6 Just to show you that this is not a fluke, high 7 frequency oscillations of blood pressure, we believe, are 8 many less, and indeed if you use trimethaphan, they go 9 nowhere. So again there's a nice internal control that 10 what we're seeing here is actually physiologic. 11 And that goes along with the findings in terms 12 of blood pressure. So if sympathetic tone is driving your 13 blood pressure, you wipe out sympathetic tone, you should 14 lower blood pressure. And that's what we see in Shy- 15 Drager patients. In normals, there's some drop in blood 16 pressure, as you would expect. Some of the even supine 17 blood pressure is maintained by blood pressure, not a lot, 18 but some of it. Of course, if you stand up, then they 19 will fall, faint. But supine blood pressure is not driven 20 a lot by sympathetic tone. So wiping out sympathetic tone 21 lowers blood pressure a little bit in normotensives, as
22 well as in patients with pure autonomic failure. But in 23 Shy-Drager, again a model of sympathetically driven 24 hypertension, even with tiny doses, you have this 25 profound, even 150 millimeters of mercury, drop in blood 0216 1 pressure. 2 In essential hypertension, it's a mixed bag. It 3 was actually what we had predicted that essential 4 hypertension is not one disease. It's probably many, and 5 they may have different components of autonomic tone. And 6 in some patients, we were not able to give greater doses 7 because their blood pressure dropped. In others, they 8 were able to withstand even higher doses of trimethaphan. 9 So at the end, once we blocked autonomic tone, 10 we come up with an intrinsic blood pressure, that is, what 11 is your final blood pressure in the absence of autonomic 12 tone. And if you're normal, that's usually below 125, 13 120. If you have Shy-Drager, all except one fall below 14 that level. And again, these are patients that started 15 with very, very high blood pressures. 16 In pure autonomic failure patients, they remain 17 hypertensive, meaning that their hypertension is not 18 driven by the sympathetic nervous system. 19 And in hypertensives, it's a mixed bag. Some 20 will have sympathetically independent hypertension and 21 some will be sensitive to sympathetic blockade. And I 22 think that may be a way, although a lot more work -- and 23 we need to study more patients, of course -- needs to be 24 done. I think that may be a way of phenotyping which 25 subset of patients with hypertension will have greater 0217 1 sympathetic component and those will be the ones we might 2 focus on in terms of genetic testing. 3 So to conclude, autonomic failure patients 4 provide us with unique models of sympathetically driven 5 and sympathetically independent hypertension. 6 Trimethaphan especially and perhaps low frequency 7 variability of blood pressure might be useful in 8 phenotyping the contribution of sympathetic tone to 9 hypertension. And let me also add that trimethaphan we 10 find also useful to dissect patients who have a central 11 autonomic problem to those who have a more distal 12 autonomic problem. And again, that might also be helpful 13 in familial dysautonomia. 14 I think I'll stop here and hopefully we're 15 caught up. 16 (Applause.) 17 DR. GOLDSTEIN: The initial questions should be 18 directed to Steve. So, all the speakers from my session. 19 Is anybody still here? 20 DR. BIAGGIONI: I think Steve can probably 21 answer all the questions you might have. 22 (Laughter.) 23 DR. GOLDSTEIN: You're leaving Steve Liggett off 24 the hook. 25 DR. EISENHOFER: No, I'm not. I'm Groeme 0218
1 Eisenhofer from the NIH. 2 Steve, I wonder if you've done any studies to -- 3 I thought they were elegant associations with heart 4 failure, but in terms of the phenotyping, actually a 5 little bit deeper in looking at the sympathetic nervous 6 system in these patients with the alpha 2 polymorphisms in 7 particular. 8 DR. LIGGETT: What I'd really like to do is 9 measure norepinephrine turnover in the cardiac sympathetic 10 nerve system in the cleft and that can be done. It's 11 fairly complicated and we're sort of about halfway there. 12 DR. EISENHOFER: Well, maybe we might be able to 13 help you with that. 14 DR. LIGGETT: Okay, that will be fine. 15 DR. EISENHOFER: We have a lot of experience in 16 those. Dave Goldstein and myself. 17 DR. LIGGETT: Right, but I think that's the way 18 these studies probably are going to go. They're going to 19 be small physiologic studies, big association studies, 20 animal studies, and cell studies, and when you put the 21 whole picture together, you're convinced of what's going 22 on. But any one study doesn't quite do it for me. 23 DR. EISENHOFER: I agree. 24 DR. GOLDSTEIN: It would be especially 25 worthwhile to find out what happens to the spillover of 0219 1 norepinephrine in the heart in response to a drug like 2 yohimbe, for instance, which blocks those alpha 2 3 receptors and is known to increase norepinephrine 4 spillover in the heart. 5 Of course, the interaction doesn't have to be 6 just among polymorphisms for adrenoceptors. There's I 7 think a very high likelihood that polymorphisms related to 8 the transporter and polymorphisms related to alpha 2 9 adrenoceptor function will interact because in people who 10 have a pharmacologic blockade of the transporter, it 11 drastically increases their norepinephrine spillover and 12 blood pressure in response to an alpha 2 blocker. 13 DR. BROWNSTEIN: I wonder if any or all of you 14 could comment on the relationship between long QT interval 15 and autonomic imbalance. 16 DR. BIAGGIONI: The QT? 17 DR. BROWNSTEIN: Long QT. 18 DR. BIAGGIONI: Yes. We see QT prolongation in 19 patients with autonomic failure, and we can induce it with 20 ganglionic blockade as well. But it's hard to know 21 whether these patients have an increased risk of 22 arrhythmias, for example, because of that because we don't 23 follow them in a very systematic way. Some of them have a 24 very poor prognosis. So it's not clear the function or 25 the relevance of that. 0220 1 DR. GOLDSTEIN: I don't think anybody knows. 2 DR. BROWNSTEIN: It's relevant, of course, to FD 3 because those patients also have long QT. They probably 4 get in trouble because of it, and the issue for me is 5 whether or not this is primary, in other words, whether or

6 not the splicing defect could injure myocardial function 7 directly or whether it's secondary to a dysautonomia. So 8 if you could comment on that based on your experience with 9 other -- 10 DR. GOLDSTEIN: Max, why don't you respond? 11 DR. HILZ: I'd just like to mention that there 12 was a paper in '91 or '92 on comparison of QTc in Romano- 13 Ward patients and MIBG uptake showing that the reduction 14 of the cardiac MIBG uptake is even a more sensitive marker 15 for Romano-Ward patients than the patients than the QTc 16 prolongation. So obviously there's evidence of structural 17 dysfunction at the level of the myocardial sympathetic 18 innervation. 19 DR. GOLDSTEIN: Yes. There's a guy named Peter 20 Schwartz I think in Italy who has tried to sell the idea 21 that there are patients who have prolonged QT and 22 susceptibility to sudden death related to an imbalance 23 between the left and right sympathetics coming the 24 stellate ganglion. I think he's actually carried out a 25 large number of left stellate ganglionectomies in an 0221 1 attempt to treat these people. He's not here, so I can 2 say whatever I want. 3 (Laughter.) 4 DR. BIAGGIONI: I think that the patients with 5 FD might be more at risk for QT prolongation because of 6 their crisis. So in our patients with autonomic failure, 7 they have very low sympathetic tone or nonreactive 8 sympathetic tone all of the time, so they have QT 9 prolongation, but normally they will do fine. Now, if we 10 give a beta agonist, they will have a lot of arrhythmias. 11 Now, in the patients with familial dysautonomia, 12 during those autonomic crises, they might be particularly 13 at risk, and I wonder if you have seen that, Felicia, if 14 you have seen arrhythmias during those crises. 15 DR. AXELROD: We haven't seen arrhythmias during 16 crisis except actually during the retching, and at that 17 time they develop often a bradycardia. And the QTc has 18 not been as sensitive as the JTc because the QTc takes 19 care of polarization and depolarization, so it's too much; 20 whereas, the JTc is just repolarization which is more 21 under sympathetic control. So I think it's been a better 22 predictor. 23 And actually we did a study where that 24 subpopulation that had JTc prolongation actually had 25 increased problems with syncope and some of them succumbed 0222 1 to -- we did it prospectively -- sudden death. 2 DR. GOLDSTEIN: It could also be that there's 3 heterogeneity of sympathetic innervation within the 4 myocardium that could result in kind of a dispersion of 5 repolarization, and as a result, since you're only looking 6 at the end of the T wave, all you can say is what the 7 maximum duration of repolarization is. But there could be 8 a lot of heterogeneity in the timing of the repolarization 9 and that could itself be a risk factor. 10 DR. AXELROD: Yes, that could but that's again

11 modifying genes and things to think about. But JTc 12 prolongation might be one indication for use of pacemaker 13 in these patients. 14 DR. GOLDSTEIN: Other questions for Steve 15 Liggett? 16 QUESTION: This is a selfish question, but per 17 all your work, do you see any application for familial 18 dysautonomia and has Vanderbilt actually worked on 19 familial dysautonomia in the past since I know they do 20 work on all the dysautonomias. 21 DR. BIAGGIONI: We saw no reason to work on 22 familial dysautonomia because Felicia had already taken 23 the whole field. 24 (Laughter.) 25 DR. BIAGGIONI: No. We don't see children 0223 1 really, so we haven't been as active. 2 QUESTION: And how about the other work? Does 3 any of the other work have an application, do you think, 4 to familial dysautonomia? 5 DR. LIGGETT: Well, I think as a general concept 6 we might even think of cystic fibrosis in a similar manner 7 to what we see here. So the delta 508 mutation that 8 causes 70 percent of cystic fibrosis is in the CFTR gene. 9 Yet, if you look at all the patients who are homozygous 10 for that mutation, the variability in clinical 11 presentation and various aspects of the disease is quite 12 broad from those who just have lung disease, those who 13 have more pancreatic problems, et cetera. And for those 14 individuals, just like your patients, their life span has 15 improved but it's primarily due to supportive care and 16 understanding nutrition and various aspects. But they've 17 not made a lot of progress in moving beyond that. 18 And I think that one of the hot areas in CF is 19 trying to figure out what modifier genes are controlling 20 why some people have a predominance in one organ system 21 versus another. Since this is an autonomic conference, I 22 got to think that autonomic receptor variation, which is 23 normally tolerated fairly well in people, but if you have 24 this bad disease plus an altered autonomic receptor 25 system, it could give you a predominance of one symptom 0224 1 versus another. 2 So I think it is actually potentially 3 applicable. It just needs to be done with the right 4 populations and the right phenotyping in the patients. I 5 guess you would probably want sort of extreme phenotypes, 6 those with no GI disorder or those with one phenotype or 7 the other so that you get a maximal chance of finding 8 something. 9 QUESTION: You're right. Most of the work done 10 on FD is with Felicia Axelrod. I do think there might be 11 an advantage to get other points of view and other people 12 working on it. Just as with Mass General working on the 13 gene, they later on saw that the way they grow their 14 samples had a big impact. And I think they were only able 15 to see that once another group had come to a finding as
16 well. So I think there's always room for extra people. 17 DR. BIAGGIONI: No, and we actually do that. 18 We've done that in the past. I think Felicia has worked 19 with us on other things, with David, and with Max, with a 20 lot of people in the field. 21 DR. GOLDSTEIN: I have an open invitation. Any 22 patient over the age of 18 with FD I'd be very interested 23 in finding out whether the sympathetic innervation of the 24 heart really is there or not. I think it's very doable 25 and I'd be happy to do it. 0225 1 DR. AXELROD: Well, I think that's really a very 2 important point. I want to address two things. 3 One about modified genes. I think as Dr. 4 Peltzer eloquently described, even within the same family, 5 you have two children who have very, very different kinds 6 of courses, and other families where there has been more 7 than one child affected, the same kind of thing has 8 happened where you don't exactly see the same disease 9 expression, but there's modification within there. So we 10 have to assume that there are some modifying genes, and I 11 think Dr. Hirschhorn also tried to alert us to this 12 possibility. And the search for modifying genes is 13 probably going to help us explain disease variability. 14 I think collaborative studies are really 15 important. What I said in my introduction, this hopefully 16 will be the fruit of this kind of conference, and I think 17 this is the spirit of this kind of a conference. 18 Dr. Goldstein has been wonderful. He actually 19 has studied one of our patients, the sympathetic 20 innervation of the heart in one patient already, and we 21 hope that other patients will cooperate. When they had 22 trepidations, I came down to the NIH and held the hand of 23 the patient so they wouldn't be as frightened of Dr. 24 Goldstein. 25 (Laughter.) 0226 1 DR. AXELROD: Yes, a very scary man. 2 (Laughter.) 3 DR. AXELROD: No, but I think if Vanderbilt has 4 some good ideas and other institutions have some good 5 ideas, that would help patients, I don't want people to 6 think that I will not cooperate or encourage my patients 7 or even just stand by to hold their hands. 8 DR. PELTZER: There's one interesting thing with 9 the variation. There is one case of identical twins that 10 both have FD, and they actually have a different 11 presentation. They are not identical in their 12 presentation. So absolutely looking for other genetic 13 factors is important, but there clearly are some 14 environmental factors that are impacting on the disease as 15 well. 16 DR. GOLDSTEIN: We'll open it up to questions on 17 any topic from this session. 18 I have a question for Italo. If in PAF there's 19 a denervation and yet the patients have significant supine 20 hypertension, other than the low baroreflex sensitivity,

21 what else comes to mind about why that would be? 22 DR. BIAGGIONI: I think we're just starting to 23 try to find out. So when you look at what maintains blood 24 pressure or what maintains blood pressure under a 25 relatively narrow limit, obviously the autonomic nervous 0227 1 system is important, renin is important, and there are 2 several other things. These patients have taught us that 3 nitric oxide is also very, very important. So this is a 4 compound that is produced by the cells lining blood 5 vessels. In normal subjects, if you block that, you 6 increase blood pressure by 10, 15, 20 points. But that is 7 misleading because that is a normal subject with a normal 8 autonomic nervous system. So every time you try to 9 increase blood pressure, the autonomic nervous system will 10 try to reduce it. If you block autonomic function, then 11 nitric oxide, then blocking nitric oxide increases blood 12 pressure by 30, 40, or 50 points. So this is obviously 13 one good candidate that we're looking at, but we're just 14 starting those studies. 15 DR. GOLDSTEIN: Yes, I was wondering. I was 16 thinking along the same lines, but also in terms of 17 treatment, if there were a way rapidly to interfere with 18 nitric oxide synthase, then given the possibility that the 19 PAF patients have supine hypertension because of some 20 endothelial dysfunction, let's say, maybe you can exploit 21 that and allow their blood pressure to increase by 22 basically blocking that nitric oxide synthase temporarily 23 when they want to be up. 24 DR. BIAGGIONI: Right. 25 DR. ADLER: Suzanne Adler from Melbourne, 0228 1 Australia. 2 A question for Dr. Ando. Can you comment on the 3 use of L-threoDOPS in the patients with amyloidotic 4 polyneuropathy? 5 DR. ANDO: Yes. That was very effective for 6 also static hypotension with elevation of the basal blood 7 pressure. As I said in my presentation, severe diarrhea 8 simultaneously occurs usually. So that chemical compound 9 was effective for treating diarrhea partially. 10 DR. GOLDSTEIN: For those who don't know, 11 L-threoDOPS is one of the four stereoisomers of DOPS. 12 DOPS, dihydroxyphenylserine, basically is an amino acid, 13 looks exactly like DOPA, except just as DOPA gets turned 14 into dopamine, L-DOPS gets turned into norepinephrine. 15 So, L-DOPS is being used as a kind of a norepinephrine 16 prodrug in several forms of autonomic failure and is 17 virtually curative in dopamine betahydroxylase deficiency 18 where this is essentially reversing the defect. 19 DR. ANDO: Yes. The very useful artificial 20 precursor compound of norepinephrine is converted in the 21 plasma in 3 or 4 hours after administration. However, in 22 FAP patients, severe diarrhea with sometimes tablet in the 23 stool. So we made a nasal application for FAP patients. 24 DR. ADLER: What's the time of onset of action 25 given intranasally?
0229 1 DR. ANDO: Time of what? 2 DR. ADLER: How quickly does it work given 3 intranasally versus orally? 4 DR. ANDO: Eight times a day or so makes sense 5 for FAP patients' therapy. 6 DR. ADLER: And a question to you and also 7 perhaps to Dr. Biaggioni. Do you think there's a role for 8 a trial of L-threoDOPS in familial dysautonomia related 9 postural hypotension? 10 DR. GOLDSTEIN: Oh, yes, if you can get the 11 drug. 12 DR. ALDER: If you can get the drug. If one is 13 persistent, one might. Do you think it's worth a try? 14 DR. BIAGGIONI: Well, I think, Dr. Kaufmann, 15 perhaps you might want to elaborate a little bit on that. 16 You have some experience with using that drug in other 17 patients with autonomic failure. 18 DR. KAUFMANN: I don't have a lot to say. David 19 already summarized it. This is a very interesting drug. 20 It's a synthetic precursor of norepinephrine. And the 21 first group that used it was David and Italo and another 22 group in Europe for patients with DBH deficiency, with 23 dopamine beta-hydroxylase, which David is going to talk 24 about tomorrow. 25 We were lucky enough to have the compound and we 0230 1 still use it. So we did a trial together also with David 2 and with Roy Freeman from Boston in patients with multiple 3 system atrophy and with pure autonomic failure, and it was 4 dramatically effective. It was very, very good. 5 So in familial dysautonomia, I cannot tell you. 6 I have very little, the same as was said before. All the 7 patients with familial dysautonomia I have seen were when 8 I went doing rounds at NYU with Felicia, and a few that 9 were upset with Felicia that came to Sinai. 10 (Laughter.) 11 DR. KAUFMANN: And I understood why they were 12 upset with Felicia because anybody would be upset with 13 them. They were very difficult patients. So I think it 14 would be interesting to try. 15 DR. GOLDSTEIN: Felicia, have you ever given the 16 stuff to an FD patient? 17 DR. AXELROD: (Inaudible.) 18 DR. BIAGGIONI: When we used it, it was not 19 commercially available, and I think we bought it through 20 Sigma Chemical Company for oral use, and it was like $50 a 21 dose. So without support from a drug company, it would be 22 very difficult to do. 23 DR. KAUFMANN: (Inaudible.) 24 DR. BIAGGIONI: Right, it's not as effective. 25 So it will be $100 per dose. 0231 1 DR. STEWART: Julian Stewart, Valhalla, New 2 York, for Dr. Biaggioni. 3 A comment about blood pressure variability. In 4 my experience, whenever heart rate variability became

5 essentially monotonous, blood pressure variability went 6 haywire. My thought was -- and perhaps you can answer 7 whether it's your thought as well -- is that on a beat- 8 to-beat basis, the heart rate may serve a role in 9 compensating for wide swings in blood pressure. What do 10 you think? 11 DR. BIAGGIONI: Yes, of course, right. 12 DR. STEWART: That's it. 13 DR. BIAGGIONI: Yes. 14 (Laughter.) 15 DR. STEWART: So that when you have no 16 baroreflex transfer, for example, you're going to see wide 17 swings in blood pressure generally speaking. 18 DR. BIAGGIONI: Right. 19 DR. STEWART: As you do in baroreflex failure. 20 DR. BIAGGIONI: Right. 21 DR. GOLDSTEIN: I think what he's trying to say 22 is that the issue of sympathetic regulation being measured 23 by the effects of trimethaphan on the power spectral 24 analysis of systolic pressure may be influenced or even 25 determined by a concurrent baroreflex regulation of pulse 0232 1 rate, and trimethaphan is eliminating both parasympathetic 2 and sympathetic postganglionic traffic. 3 DR. STEWART: I see the same thing in patients 4 with changes in baroreflex gain so that as the gain falls 5 down, the blood pressure variability -- as the heart rate 6 becomes monotonous, blood pressure variability almost 7 invariably skyrockets, for whatever reason. 8 DR. BIAGGIONI: Can I ask a question to Dr. 9 Ando? Do your patients have supine hypertension? 10 DR. ANDO: Basically no, but after 11 administration of L-threoDOPS ________, supine 12 hypertension sometimes occurs. Basically no. 13 QUESTION: A couple of years ago, I did ask 14 someone at the center -- I forgot who -- on FD Day about 15 L-DOPS because I read such great stuff about it, but at 16 the time I think someone didn't hear about it and someone 17 did, but they were afraid that when the blood pressure in 18 FDers go up during a crisis, that the L-DOPS might push it 19 over the top and that might be a problem. 20 DR. BIAGGIONI: I guess we need to understand 21 better why they have these crises. Well, let me rephrase 22 that. I would need to understand better. Perhaps 23 somebody knows. But if it is driven by the dopamine or 24 epinephrine or dopamine being converted to norepinephrine, 25 you're going to be competing with the same receptors. So 0233 1 I'm not sure if it's going to make it worse. 2 DR. GOLDSTEIN: I think a lot depends on whether 3 there's denervation. That's crucial because if there is 4 denervation, then you could argue that with a crisis, the 5 L-DOPS isn't really going to make that much of a 6 difference, but if there is innervation, then the L-DOPS 7 would be converted to norepinephrine. Norepinephrine 8 could be taken up into those existing terminals, and the 9 norepinephrine could be released during sympathetic
10 stimulation. And that would be dangerous. So I think a 11 lot depends on whether there's really denervation or not. 12 I wanted to mention -- remember back when I was 13 talking about the five components of the autonomic nervous 14 system -- I think it's really crucial to find out if 15 during these crises there actually is a high plasma 16 epinephrine level because it sounds to me like a lot of 17 the findings could be explained by a combination of 18 epinephrine and receptors that are super-sensitive. 19 DR. AXELROD: There isn't. That's been done. 20 There's high dopamine during crisis and some patients 21 actually have some high norepinephrine, which we believe 22 is converted from the dopamine because it's seen with 23 longer crises. When the crises last a long time, then you 24 see a lot of hyperglycemia, hypertension, you see the 25 norepinephrine go up, but the epinephrine is not up. 0234 1 DR. GOLDSTEIN: I've been confused by that 2 dopamine story because I know if you infuse dopamine into 3 normal volunteers to produce these levels of dopamine -- 4 granted, they're 10 times normal -- there's no hemodynamic 5 effect. In order to see an increase in blood pressure 6 with infused dopamine, you have to have a concentration in 7 a range of about 3,000 picograms per ml. That doesn't 8 happen, not even during a crisis. 9 DR. AXELROD: (Inaudible.) 10 DR. MAAYAN: I'm just saying that for the same 11 amount of dopamine, because receptors of dysautonomic 12 patients are hypersensitive, they're reacting much more. 13 DR. AXELROD: Actually that was also done by 14 Weiser and myself in a microcirculation study with the 15 laser Doppler, and we actually demonstrated 16 hypersensitivity of the adrenoreceptors. So they could 17 bind to -- 18 DR. GOLDSTEIN: To dopamine? 19 DR. AXELROD: -- other catecholamines. I mean, 20 the dopamine can bind to that as well. 21 DR. GOLDSTEIN: Did you find that there was an 22 effect of dopamine on the -- 23 DR. AXELROD: We did not use dopamine. 24 DR. GOLDSTEIN: -- flowmetry? 25 DR. AXELROD: No, we didn't use dopamine during 0235 1 the microcirculation studies. We used norepinephrine. 2 DR. GOLDSTEIN: Right. The adrenoreceptors I'm 3 sure could be up-regulated, but the issue is what dopamine 4 is doing. 5 Yes, go ahead. 6 DR. ADLER: The crisis is such an awful part of 7 dysautonomia. Given that we have more technology now to 8 look at catecholamine chemistry and dynamics, it might be 9 worthwhile devising a protocol where we actually look at 10 what happens during crisis using all modalities in a 11 monitored lab, because we really are in the dark knowing 12 what drugs to blocks, to treat when we go into crisis. 13 The drugs we use for day-to-day staying upright and not 14 falling dizzy are the opposite to what you might want to

15 have around when you're having crisis. So we need to look 16 at short-acting agents, we need to look at alternative 17 routes of delivery, sublingual, intranasal, whatever. 18 Parents are capable. They can even given subcutaneous 19 injections if there was a drug that was appropriate. So I 20 think it's time to probably work out another protocol for 21 a study for crisis, and I'm sure we could find lots of 22 volunteers. 23 DR. GOLDSTEIN: Thank you. 24 All right. I think we'll call it a day. Thanks 25 everybody. 0236 1 (Applause.) 2 (Whereupon, at 4:25 p.m., the meeting was 3 recessed, to reconvene at 8:30 a.m., Friday, October 4, 4 2002.) 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25