Embed Size (px)
Citation preview
1Folic acid inhibiting drugs
• Sulfonamides (sulfa drugs)– Early synthetic drugs– Metabolic antagonists, block folic acid biosynthetic
pathway– Folic acid needed for synthesis of nucleotides
• Selectively toxic: folic acid is a human vitamin– Failure to synthesize DNA bacteriostatic– Resistance common
• Mutation in enzyme easy• Reduced drug uptake also occurs
2trimethoprim
• Different structure, functions in same pathway– Inhibits different enzyme– Resistance also occurs from changed cell
permeability and altered enzyme
• Used in combinations with sulfonamides– Bactrim: sulfamethoxazole and trimethoprim– Synergistic to the point of being bactericidal– Decreased resistance by mutation from mutation
rate being the product of the two rates
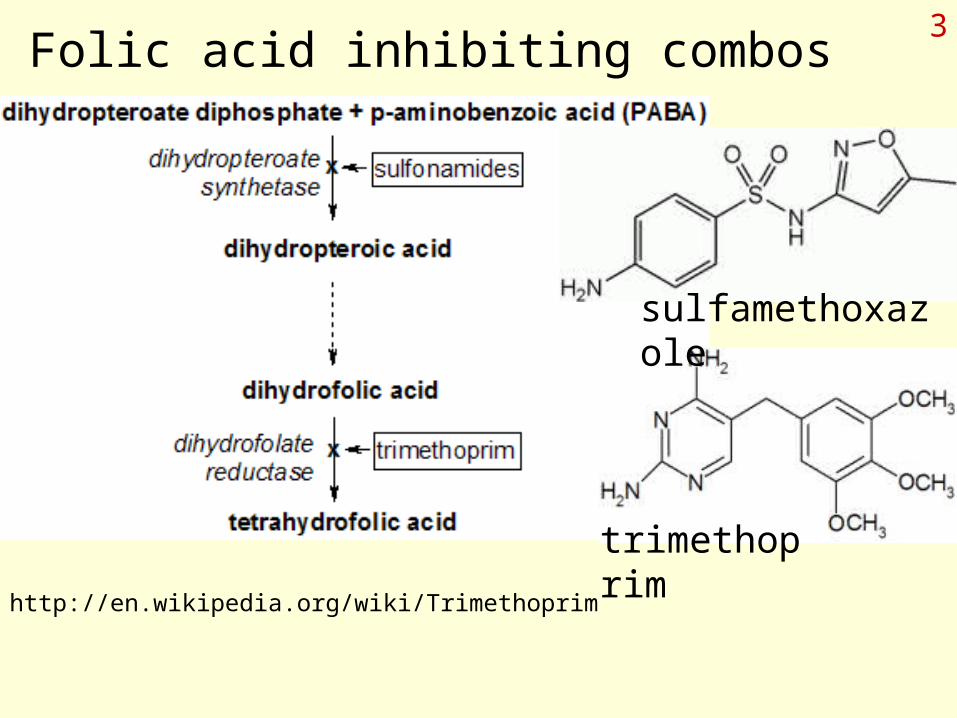
3Folic acid inhibiting combos
sulfamethoxazole
trimethoprim
http://en.wikipedia.org/wiki/Trimethoprim
4Pharmacokinetics and use
• Sulfa drug family generally administered orally– Great variation in disposition, half life – Mostly combos administered
• Wide variety of pathogens including non-bacterial• Treatment of opportunistic infections found with
HIV infection• Treatment of urinary tract infections• Treatment of some chronic respiratory infections
5Side effects of folate inhibitors
• Hypersensitivities including Stevens-Johnson syndrome– Severe reaction with extensive skin damage and
systemic effects
• Hematological effects including anemias, agranulocytosis, thrombocytopenia

6Polymyxins
www.cas.astate.edu/ draganjac/AndreaHausman.html
Cyclic peptides of amino acids and amino butyric acid.
“R” is a long hydrophobic tail.
Source: Bacillus polymyxa
Polymyxins interact with OM of Gram negatives, causing leakage of periplasmic enzymes, damage cell membrane.
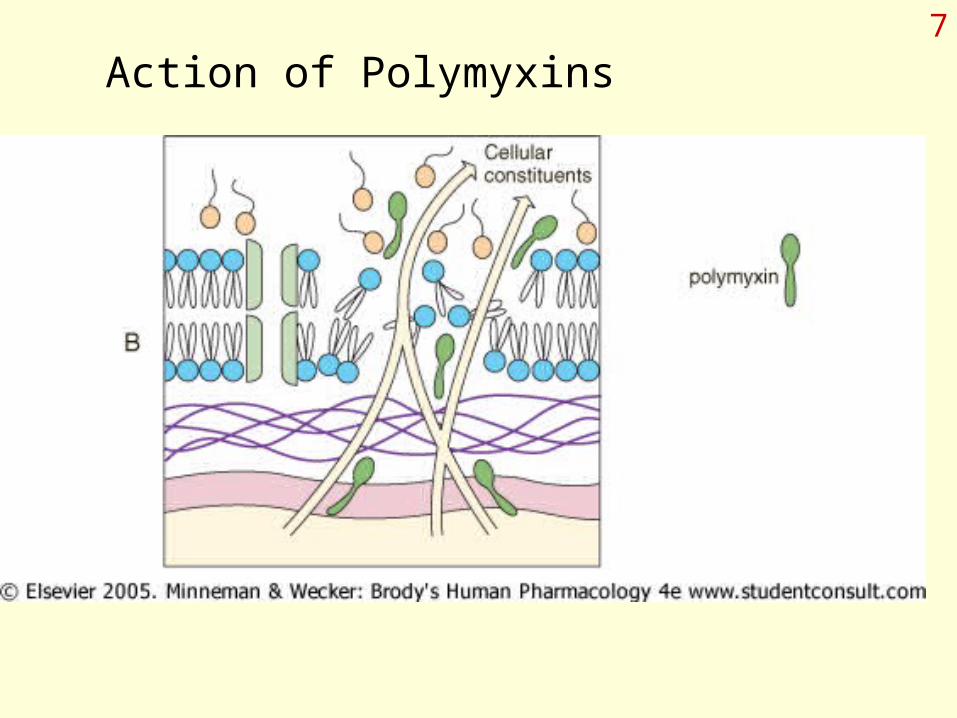
7
Action of Polymyxins

8Polymyxins
• Can be used iv with caution
• Toxicity primarily nephro- and neurotoxicity– Expected to have low selective toxicity because of
detergent effects on cell membranes.
• Typically administered topically along with neomycin and bacitracin– Combination covers cell wall inhibition, protein
synthesis inhibition, and membrane attack– Effective against Gram positives and negatives
9Fluoroquinolones
• Based on older drug nalidixic acid
• Became familiar to public during anthrax scares
• Inhibit the action of Topoisomerases including Type 2 (includes gyrase) and Topo..ase IV– Bacterial DNA is negatively supercoiled; these
enzymes introduce or remove supercoiling and are required for relieving coiling stress during DNA replication.
– Inhibition results in cell death due to release of DNA w/ double strand breaks.
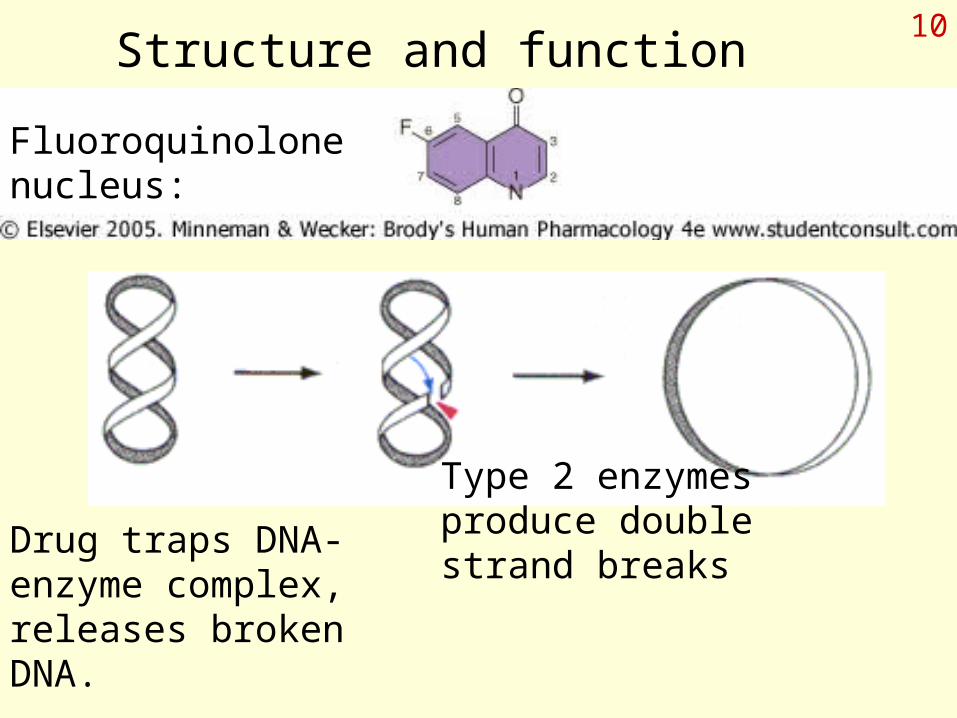
10Structure and function
Fluoroquinolone nucleus:
Type 2 enzymes produce double strand breaks
Drug traps DNA-enzyme complex, releases broken DNA.
11Pharmacokinetics and clinical use
• Fluoroquinolones can all be given orally– Most can also be administered iv
• Most have fairly long half-life in the body (e.g. >4 hours), good penetration into compartments
• Mostly renal excretion
• Active against a wide range of bacteria– Urinary tract and STDs– Tough to kill bacteria– Biowarfare agents (anthrax, plague, tularemia)

12Toxicity
• Usual wide variety of side effects
• GI disturbance including C. difficile problems
• Hypersensitivity with rashes
• Some degree of neuro- and hepatotixicity
• Damage to cartilage in developing individuals (i.e. children).
• Elevated theophylline levels!
13Chapter 49: anti-mycobacterial agents
• Mycobacterium– M. tuberculosis: cause of tuberculosis
• Chronic lung disease– M. avium complex (MAC)
• Environmental opportunist– M. leprae: Hansen’s disease aka leprosy

14Challenges to treatment
• Chronic diseases, require long term treatment
• Socio-economic groups– Homeless and poor least likely to continue therapy,
breeds resistance
• Combination therapy required because of developing resistance
• Bacteria grow intracellularly– Drug must reach target
• Uncontrolled, contagious infections in immunocompromised
15Selected info on drugs
• Mixture of synthetic drugs and antibiotics
• Orally administered as befits long term care– 6 to 9 months of treatment
• Typical drugs:– Isoniazid, ethambutol, rifampicin, pyrazinamide– Include many different modes of action– Some target the unique cell wall consisting of
mycolic acids covalently attached to PG
16Antifungal drugs
• Fungi are eukaryotes, thus removing targets of 70S ribosomes and PG.– Major target: fungal cell membrane– Other drugs target cell wall, nuclear division, and
nucleic acid synthesis
• Except for superficial infections, serious disease rarely occurs in healthy individual– Systemic, serious disease in immunocompromised
• Older drugs powerful, but more toxic– Amphotericin B, Nystatin, etc.
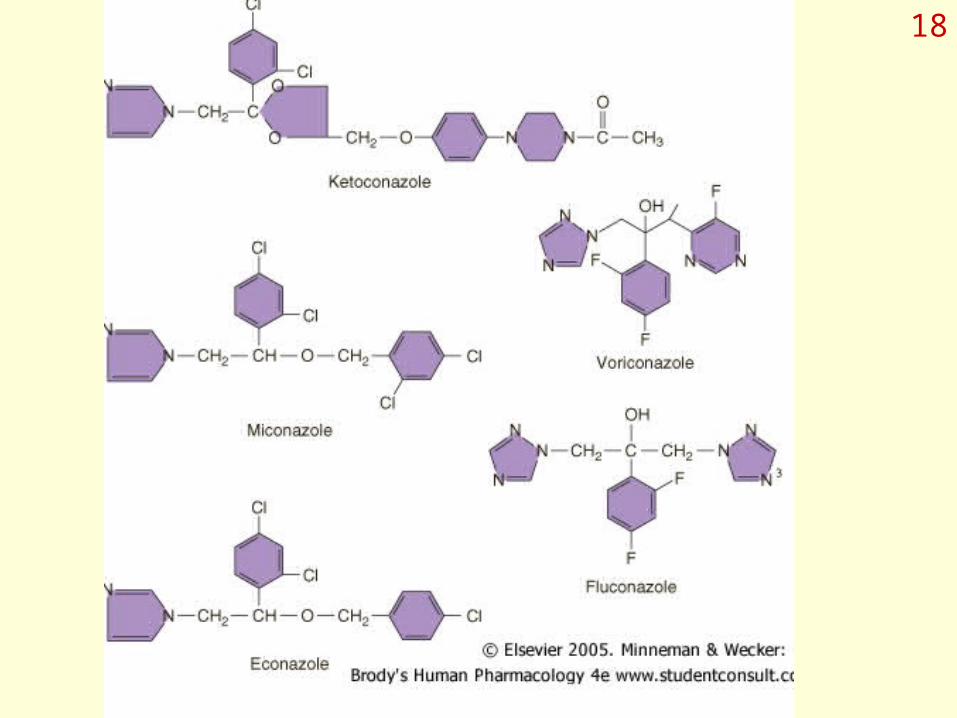
17Azoles, Allylamines, Tolnaftate
• Azoles:Fluconazole, ketoconazole, miconazole– Inhibit enzyme in ergosterol pathway, compromising
cell membranes– Some oral, some topical, some iv
• Dependent on absorption properties
• Terbinafine: allylamine marketed as Lamisil– Concentrated in hair and nails
• Various azoles, terbinafine, and tolnaftate sold for treatment of superficial infections, OTC
18




















![acid dexaexilcolic,acid folic ]n dezvoltarea creer nn.pdf](https://img.pdfslide.us/doc/110x75/577cb57f1a28aba7118d31d3/acid-dexaexilcolicacid-folic-n-dezvoltarea-creer-nnpdf.jpg)