Embed Size (px)
Citation preview

1
بسم الله الرحمن الرحيمبسم الله الرحمن الرحيمEpidemiology & Epidemiology &
Control of Infectious diseasesControl of Infectious diseases
MalariaMalariaShahid Beheshti University of Shahid Beheshti University of
medical sciences, 2004medical sciences, 2004By: Hatami H. MD. MPHBy: Hatami H. MD. MPH

2
Definition Definition History History
Etiology Etiology

3
Definition of MalariaDefinition of Malaria
• Disease caused by Disease caused by a unicellular a unicellular protozoan protozoan PlasmodiumPlasmodium
• The The most importantmost important of the parasitic of the parasitic diseases of humansdiseases of humans
• Affecting Affecting > 1 billion> 1 billion people people
• Transmission in Transmission in 103 countries103 countries
• Causing Causing 1-3 million deaths1-3 million deaths each year each year

4
World's Deadliest Scourges
• Acute Respiratory Infections
• Diarrheal Diseases
• Tuberculosis
• Hepatitis B
• Malaria
• Measles
• Neonatal Tetanus
• AIDS
– 4,300,000
– 3,200,000
– 3,000,000
– 1-2,000,000
– 1,000,000
– 880,000
– 600,000
– 550,000
Infectious disease Annual deaths

5
History History
500_BC500_BC HippocratesHippocrates Clinical SymptomsClinical Symptoms
18801880 LaveranLaveran Blood StageBlood Stage
18981898 RossRoss Mosquito TransmissionMosquito Transmission
19481948 GarnhamGarnham Liver StageLiver Stage
Latin: “mal aria” Latin: “mal aria” = Bad air= Bad air association with swamp and association with swamp and
marshlandmarshland

6
History History • Most importantMost important of all tropical diseases of all tropical diseases
((WHOWHO))– Vast Vast morbiditymorbidity and and mortalitymortality
– 40% of world population at 40% of world population at riskrisk of of infectioninfection
– 300-500 million 300-500 million casescases >90% in sub- >90% in sub-Saharan AfricaSaharan Africa
– At least 1 million At least 1 million deathsdeaths per year per year
– Mostly Mostly African childrenAfrican children (75%) (75%)

7
• WWI WWI
– Almost 5,000 cases in Almost 5,000 cases in USUS Navy and Navy and MarinesMarines
– More than 100,000 cases in More than 100,000 cases in BritishBritish and and FrenchFrench soldiers soldiers
WWII
– 500,000 cases in US Army
– More than 110,000 cases in US Navy
History History

8
Resurgence of Malaria Resurgence of Malaria
• EcologicalEcological change change
• Breakdown of Breakdown of controlcontrol activities activities
• PoliticalPolitical events events
• Population Population movementmovement
• MarginalMarginal populations populations

9
Etiology Etiology
• Plasmodium protozoaPlasmodium protozoa– P. vivaxP. vivax
– P. ovaleP. ovale
– P. malariaeP. malariae
– P. falciparumP. falciparum

10
Plasmodium life cycle Plasmodium life cycle •Two phasesTwo phases
Extrinsic phaseExtrinsic phase In In AnophelesAnopheles – sexual – – sexual – definitivedefinitive
hosthost
Intrinsic phaseIntrinsic phase
In human –asexual – In human –asexual – intermediateintermediate hosthost

11
8-30 days
7-14 days

12
Severity dependent upon: Severity dependent upon: • SpeciesSpecies• ParasitaemiaParasitaemia• Health statusHealth status• Immunity Immunity
Pathogenesis Pathogenesis

13
Pathogenesis Pathogenesis Fever (Febrile paroxysm)Fever (Febrile paroxysm)
Many symptoms due Many symptoms due toto
– Erythrocyte break-down Erythrocyte break-down productsproducts
– parasite proteins parasite proteins

14
3 stages (paroxysm)3 stages (paroxysm)
• Pattern of fever (paroxysm):Pattern of fever (paroxysm):– 1- Cold stage1- Cold stage (shivers) (shivers)
– 2- Hot stage2- Hot stage (flush, rapid pulse) (flush, rapid pulse) severe headachesevere headache
joint pains, vomiting, diarrhoeajoint pains, vomiting, diarrhoea
– 3- Sweating stage3- Sweating stageprofuse sweating decrease in profuse sweating decrease in
Temperature exhaustionTemperature exhaustion
Pathogenesis Pathogenesis

15
AnaemiaAnaemia• Haemolytic Haemolytic • Usually most severe in Usually most severe in P. falciparumP. falciparum
HepatosplenomegalyHepatosplenomegaly• Begins in early acute infectionBegins in early acute infection• Spleen may be very enlarged in chronic Spleen may be very enlarged in chronic
malaria after repeated infectionsmalaria after repeated infections
JaundiceJaundiceUsually Usually mildmild but may be but may be severesevere in in P. falciparumP. falciparum due to liver damage due to liver damage
Pathogenesis Pathogenesis

16
Abiotic and Biotic Factors Abiotic and Biotic Factors influencing malariainfluencing malaria
• AbioticAbiotic• Increased Increased temperaturetemperature• An increase in An increase in greenhousegreenhouse gases gases
• BioticBiotic• An increase in An increase in parasitesparasites• An increase in An increase in mosquitoesmosquitoes• Increase in human Increase in human populationpopulation

17
Movement of
People
Human / Insect
Interactions
Population
Growth
Increased
Breeding
Sites
Increased
Temperature
Increased
Precipitation
Changes in
Land Use
Increase in
Resistance
Increase in
Mortality
Spread of
Malaria
Increase in the
Dispersion of
Mosquitoes and parasite
Increased Chance
of Susceptibility
Climate
Change
Factors influencing malariaFactors influencing malaria

18
Descriptive Descriptive epidemiology epidemiology
and and
occurrenceoccurrence

19
1 -Incubation Period1 -Incubation Period
Prepatent period Prepatent period (I.P of parasitemia)(I.P of parasitemia)
The time from infection to the The time from infection to the appearance of parasites in the appearance of parasites in the blood (blood (usually 7-10 days)usually 7-10 days)
Incubation periodIncubation periodThe time from infection to the The time from infection to the appearance of symptoms (14 days)appearance of symptoms (14 days)

20
– P. falciparumP. falciparum 7-14 days7-14 days
– P. vivax 8-14 daysP. vivax 8-14 days
– P. ovale 8-14 daysP. ovale 8-14 days
– P. malariae 7-30 daysP. malariae 7-30 days
–By blood transfusion is shorter By blood transfusion is shorter
Incubation PeriodIncubation Period

21
2- Natural course 2- Natural course • RelapseRelapse
– HypnozoitesHypnozoites - dormant phase in - dormant phase in P. vivaxP. vivax and and P. ovaleP. ovale
– RelapseRelapse - reactivation of the infection - reactivation of the infection via hypnozoitesvia hypnozoites
• RecrudescenceRecrudescence – Parasitaemia falls below detectable levels and then Parasitaemia falls below detectable levels and then
later increases to a patent parasitaemia (later increases to a patent parasitaemia (P. malariae)P. malariae)

22
Natural course Natural course
P. vivaxP. vivax• If untreated, usually lasts for 2-3 If untreated, usually lasts for 2-3
months with months with diminishingdiminishing frequency and intensity of frequency and intensity of paroxysmsparoxysms
• 50% experience a 50% experience a relapserelapse in a few in a few weeks to 5 years after the initial weeks to 5 years after the initial illness.illness.

23
Natural course Natural course
P. ovaleP. ovale• SimilarSimilar to to P vivaxP vivax infections infections
• Are usually Are usually less severeless severe
• Often Often resolvesresolves without treatment. without treatment.

24
Natural course Natural course
P. malariaeP. malariae• AsymptomaticAsymptomatic for a much longer for a much longer
period of time period of time
• RecrudescenceRecrudescence is common is common
• It often is associated with a It often is associated with a nephroticnephrotic syndromesyndrome
• Possibly resulting from deposition of Possibly resulting from deposition of antibody-antigen complexantibody-antigen complex upon the upon the glomeruli.glomeruli.

25
Natural course Natural course
P. falciparumP. falciparum• The most The most malignantmalignant form of malaria form of malaria • Not limitedNot limited to RBCs of a particular age to RBCs of a particular age• The highest level of The highest level of parasitemiaparasitemia• Vascular obstructionVascular obstruction due to its ability to due to its ability to
adhere to endothelial cell wallsadhere to endothelial cell walls• CCerebralerebral malaria, malaria, pulmonarypulmonary edema, edema,
rapidly developing rapidly developing anemiaanemia, and , and renalrenal problems.problems.

26
Natural course Natural course Classic paroxysm :Classic paroxysm :• Begins with shivering and chillsBegins with shivering and chills• Lasts 1-2 hoursLasts 1-2 hours• Followed by a high feverFollowed by a high fever Finally, Finally, • The patient experiences excessive The patient experiences excessive diaphoresisdiaphoresis• Body temperature drops to normal or Body temperature drops to normal or below normal.below normal.

27
Natural course Natural course Classic paroxysm :Classic paroxysm :• Many patients may have Many patients may have several small fever spikes a dayseveral small fever spikes a day
• Maintain a Maintain a high index of suspicionhigh index of suspicion for for malaria in any patient exhibiting any malaria in any patient exhibiting any malarial malarial symptomssymptoms and having a and having a history of travel to endemic areas history of travel to endemic areas

28
Natural course Natural course Classic paroxysm :Classic paroxysm :
Less common symptoms Less common symptoms include the following:include the following:• Anorexia and lethargyAnorexia and lethargy• Nausea and vomitingNausea and vomiting• DiarrheaDiarrhea• HeadacheHeadache

29
Natural course Natural course PhysicalPhysical: :
•TachycardiaTachycardia• FeverFever• HypotensionHypotension• Signs of anemiaSigns of anemia• SplenomegalySplenomegaly

30
Natural course Natural course Laboratory finding Laboratory finding
• Normochromic, normocytic Normochromic, normocytic anemiaanemia• WBCWBC count is normal but in count is normal but in severe malaria may be raisedsevere malaria may be raised• ESRESR and and CRPCRP are high are high • the the plateletplatelet count is reduced count is reduced

31
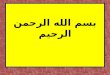
40.6
55.5
3.9
0
10
20
30
40
50
60
1001-4500 4501-10500 10501-30000
Patients with malaria admitted Patients with malaria admitted in Sina hospital Kermanshahin Sina hospital Kermanshah
WBC countWBC count

32
4/7-11/938%
12-HI62%
Patients with malaria admitted Patients with malaria admitted in Sina hospital Kermanshahin Sina hospital Kermanshah
HEMOGLOBINEHEMOGLOBINE

33
99.5 99
6355.8
47
28.4 24 2414.412.5 10 8.7
2.4 1.90102030405060708090
100
feve
r
chill
s
head
ache
swea
ting
vom
iting
mya
lgia
ab . pain no
sea
cons
tipat
ion
blac
k ur
ine
diar
rhea
arth
ralg
ia
ches
t pai
n
epis
taxi
a
Patients with malaria admitted Patients with malaria admitted in Sina hospital Kermanshahin Sina hospital Kermanshah
symptomssymptoms

34
82.6
57.2
37.2
26 25 21.5
7.2 4.3 0.50102030405060708090
feve
r
sple
nom
egal
ia
tach
ypne
a
pale
ness
jund
ice
tach
ycar
dia
hepa
tom
egal
ia
herp
es l
.p . o . ed
ema
Patients with malaria admitted Patients with malaria admitted in Sina hospital Kermanshahin Sina hospital Kermanshah
signssigns

35
Complications Complications • Coma (Coma (cerebral malariacerebral malaria) ) • SeizuresSeizures• Renal failureRenal failure• Hemoglobinuria (Hemoglobinuria (blackwater feverblackwater fever) ) • Noncardiogenic pulmonary edema Noncardiogenic pulmonary edema • Profound hypoglycemiaProfound hypoglycemia• Lactic acidosisLactic acidosis• HemolysisHemolysis• Bleeding (Bleeding (coagulopathycoagulopathy))

36
Complications / ComaComplications / Coma• Altered Altered mental statusmental status, or multiple , or multiple seizuresseizures with with P P falciparumfalciparum• Cerebral malaria is the Cerebral malaria is the most common causemost common cause of of deathdeath in malaria patients in malaria patients• If untreated, is If untreated, is lethallethal• Even with treatment, 15% of children and 20% Even with treatment, 15% of children and 20% of adults who develop cerebral malaria dieof adults who develop cerebral malaria die• The symptoms of cerebral malaria are The symptoms of cerebral malaria are similar to those of toxic encephalopathysimilar to those of toxic encephalopathy

37
Complications of Complications of P. falciparumP. falciparum
OrganOrgan SymptomsSymptoms MisdiagnosisMisdiagnosis
Stomach & Stomach & intestinesintestines
Vomiting & Vomiting & diarrhoeadiarrhoea
Gastric flu, choleraGastric flu, cholera
BrainBrain Deliria, coma, Deliria, coma, convulsionsconvulsions
Encephalitis, Encephalitis, meningitismeningitis
Kidneys Kidneys Renal failure Renal failure haemoglobinuriahaemoglobinuria
NephritisNephritis
LiverLiver Jaundice & feverJaundice & fever HepatitisHepatitis
LungsLungs Pulmonary Pulmonary oedemaoedema

38
Host immune Host immune responseresponse
• In high transmission areas In high transmission areas 5-6yr 5-6yr childchild immune to lethal disease, immune to lethal disease, AdultsAdults usually mild flu-like episodesusually mild flu-like episodes
• IgGIgG limits parasitaemia limits parasitaemia
• ButBut suppressed by suppressed by pregnancypregnancy, , severe illnesssevere illness, immunosuppressive , immunosuppressive drugsdrugs

39
Host immune Host immune responseresponse
• Both Both humoralhumoral immunity and immunity and cellularcellular immunity are necessary immunity are necessary for protectionfor protection
• The The mechanismmechanism of each are of each are incompletely understoodincompletely understood
• Premunition ??Premunition ??

40
• Sickle cellSickle cell– Glutamic acidGlutamic acid replaced by replaced by valisevalise in in
haemoglobin (Hb)haemoglobin (Hb)– Change in Hb conformation/Change in Hb conformation/reduced reduced
oxygen carryingoxygen carrying– HeterozygotesHeterozygotes - - 80-90% protection80-90% protection
against severe malariaagainst severe malaria– HomozygotesHomozygotes – usually die before 30yrs – usually die before 30yrs
Host immune response Host immune response Non-immune protectionNon-immune protection

41
Host immune Host immune responseresponse
• ThalassemiaThalassemia– Defective synthesis of Hb chainsDefective synthesis of Hb chains
• Duffy blood group antigensDuffy blood group antigens– Fy/Fy (Duffy negative) Fy/Fy (Duffy negative) – Erythrocyte plasma membrane Erythrocyte plasma membrane
receptor not expressedreceptor not expressed– P. P. vivaxvivax cannot enter erythrocytes cannot enter erythrocytes– Resistance to lethal Resistance to lethal P. P. falciparumfalciparum
Non-immune protectionNon-immune protection

42
• Malaria occurs in over Malaria occurs in over 103 countries103 countries and territoriesand territories
• Central and South Central and South AmericaAmerica, , HispaniaHispania (Haiti and Dominican (Haiti and Dominican Republic), Republic), AfricaAfrica, the , the Indian Indian subcontinentsubcontinent, , Southeast AsiaSoutheast Asia, and , and the the Middle East. Middle East.
3 - Geographical distribution3 - Geographical distribution

43
Geographical distributionGeographical distribution
p. f
p. vp. v
p. Vp. f
p. Vp. f
p. Vp. f
p. m
p. o

44
12260130
5288916
105223 1123290
2000000
4000000
6000000
8000000
10000000
12000000
14000000
Africa Asia Americas Oceanis
Geographical distributionGeographical distribution

45
Parasitemia rate or palpable spleen Parasitemia rate or palpable spleen rates in children 2-9 years of age :rates in children 2-9 years of age :
• HypoendemicHypoendemic < 10% < 10%• Mesoendemic 11-50%Mesoendemic 11-50%• Hyperendemic 51-75%Hyperendemic 51-75%• Holoendemic > 75%Holoendemic > 75%
Endemicity Endemicity

46
Malaria in IranMalaria in Iran
• Sistan-Baluchestan, Sistan-Baluchestan, • Fars, Fars, • Boshehr, Boshehr, • Khuzestan, Khuzestan, • Ilam, Ilam, • Lorestan, Lorestan, • Charmahal, and Bakhtiari; Charmahal, and Bakhtiari; • Kerman; Kerman; • Hormozgan. Hormozgan.

47
Malaria in IranMalaria in Iran
• Strong malaria control programStrong malaria control program• There has been a decreasing trend in recent yearsThere has been a decreasing trend in recent years• 16% out of the total population live in non-16% out of the total population live in non-
malarious areasmalarious areas• 66% lived in areas freed from malaria66% lived in areas freed from malaria• 12% in areas with sporadic transmission Mostly 12% in areas with sporadic transmission Mostly
P.vivaxP.vivax, , • 6% in areas of continuous transmission with a 6% in areas of continuous transmission with a
high proportion of high proportion of P.falciparumP.falciparum..

48
Malaria in IranMalaria in Iran
• During 1997, During 1997, 38,76638,766 were found to were found to be positivebe positive
• 22%22% were due to were due to P. falciparumP. falciparum
• 22 22 fatalitiesfatalities were reported. were reported.

49
Malaria in Iran / RegionsMalaria in Iran / Regions1.Regions to the north of the Zagros range 1.Regions to the north of the Zagros range
• Annual Parasite Incidence (Annual Parasite Incidence (APIAPI) ) in this area was in this area was 0.140.14 per 1,000 in per 1,000 in 19971997
• About About 77%77% of the malaria cases of the malaria cases were were importedimported from abroad or the from abroad or the south eastern part of the countrysouth eastern part of the country

50
Malaria in Iran / RegionsMalaria in Iran / Regions2.Regions to the south of the Zagros range2.Regions to the south of the Zagros range
• API was reported to be 0.18 per API was reported to be 0.18 per 1,0001,000
• 48%48% were classified as were classified as importedimported..

51
Malaria in Iran / RegionsMalaria in Iran / Regions3.The south eastern corner of Iran3.The south eastern corner of Iran
• Consists of Consists of SistanSistan and and BuluchistanBuluchistan Province, Province, HormozganHormozgan Province and the Province and the tropical part of tropical part of KermanKerman Province Province
• A combined population of approximately A combined population of approximately 3 million3 million is considered to be a is considered to be a refractoryrefractory malaria regionmalaria region
• API was reported to be API was reported to be 8.74 per 1,0008.74 per 1,000 populationpopulation

52
Malaria in Iran / RegionsMalaria in Iran / Regions3.The south eastern corner of Iran (2)3.The south eastern corner of Iran (2)
• It is It is more difficult to controlmore difficult to control than than elsewhere in Iranelsewhere in Iran
• DrugDrug resistance resistance of of P.falciparumP.falciparum
• Vector resistanceVector resistance to insecticides to insecticides
• ImportationImportation of malaria, mostly of malaria, mostly P.falciparumP.falciparum, from Afghanistan , from Afghanistan
and, to a lesser extent, Pakistan. and, to a lesser extent, Pakistan.

53
4 - Timeline trend4 - Timeline trend
• PandemicsPandemics
• EpidemicsEpidemics
• OutbreaksOutbreaks
• SeasonalitySeasonality

54
Seasonality Seasonality • Summer,Summer,
• Autumn,Autumn,
• SpringSpring

55
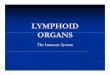
Spring20%
Summer57%
Automn21%
winter2%
seasonal distribution of malaria, seasonal distribution of malaria, Kermanshah 1988-99Kermanshah 1988-99

56
5 – Age,5 – Age, Gender, Gender,
Occupation,Occupation, Social conditions Social conditions

57
• AgeAge: :
• All ages are affected by malariaAll ages are affected by malaria
• MortalityMortality is very high in children is very high in children younger than 5 yearsyounger than 5 years
• SexSex::
• Males and females are affected Males and females are affected equally. equally.

58
25.1
74.9
0
20
40
60
80
Female Male
Sex distribution of malaria, Sex distribution of malaria, Kermanshah 1988-99Kermanshah 1988-99

59
6- Predisposing factors / 6- Predisposing factors / Pregnancy Pregnancy
• Especially Especially primigravidprimigravid women women
• 10 times more likely to contract 10 times more likely to contract Severe malariaSevere malaria
• Pregnant women with Pregnant women with P. P. vivaxvivax & & falciparumfalciparum are at high risk for are at high risk for severe malariasevere malaria

60
• Has a Has a shorter courseshorter course, often rapidly , often rapidly progressing to progressing to severesevere malaria malaria
• HypoglycemiaHypoglycemia, , seizuresseizures, severe , severe anemiaanemia, , and and sudden deathsudden death
• Much less likely to develop Much less likely to develop renalrenal failure, failure, pulmonary edemapulmonary edema, or , or jaundicejaundice
• Commonly Commonly recoverrecover from malaria, even from malaria, even severe malaria, much faster than adultssevere malaria, much faster than adults
Predisposing factors / Pediatrics Predisposing factors / Pediatrics

61
7 – Susceptibility and Resistance7 – Susceptibility and Resistance
• Tolerance in highly endemic • Duffy negatives • Sickle cell trait

62
8 – Secondary attack rate8 – Secondary attack rate
Period of Period of communicabilitycommunicability
•Untreated patients may be a Untreated patients may be a source of mosquito infection source of mosquito infection for :for :
•More the 3 years in malariaeMore the 3 years in malariae• 1-2 years in vivax1-2 years in vivax• 1 year in falciparum1 year in falciparum• The mosquito remains The mosquito remains
infective for lifeinfective for life

63
9 - Transmission9 - Transmission
Transmission requires complex Transmission requires complex interaction between:interaction between:
Humans, Humans,
Mosquitoes, Mosquitoes,
Parasites, and Parasites, and
Local environmentLocal environment

64
TransmissionTransmission• All 4 species are transmitted All 4 species are transmitted
through the through the bitebite of an infected of an infected female female AnophelesAnopheles
• Via a blood Via a blood transfusiontransfusion, , needleneedle stick injury, stick injury, sharingsharing of needles by of needles by infected drug addicts organ infected drug addicts organ transplantationtransplantation
• CongenitallyCongenitally between mother and between mother and fetus fetus

65
TransmissionTransmission
• The mosquito must survive for The mosquito must survive for > 7 days > 7 days
• At temperature <16-18°C At temperature <16-18°C sporogony is not completed and sporogony is not completed and transmission does not occurtransmission does not occur

66
Anopheles in Iran Anopheles in Iran • A. superpictusA. superpictus
• A. sacharoviA. sacharovi
• A. stephensi A. stephensi
• A. d’thaliA. d’thali
• A. fluviatilisA. fluviatilis
• A. maculipenisA. maculipenis

67
Prevention Prevention andand
ControlControl

68
Prevention and ControlPrevention and Control• Primary Prevention:Primary Prevention:
Prevention of disease in “well” Prevention of disease in “well” individualsindividuals
• Secondary Prevention:Secondary Prevention: Identification and intervention Identification and intervention
in early stages of diseasein early stages of disease
Tertiary Prevention:Tertiary Prevention: Prevention of further Prevention of further
deterioration, reduction in deterioration, reduction in complicationscomplications

69
1 - Primary prevention 1 - Primary prevention
1)1) Personal protectionPersonal protection2)2) Chemoprophylaxis Chemoprophylaxis 3)3) VaccinationVaccination4)4) Vector controlVector control

70
Primary prevention Primary prevention Personal protectionPersonal protection
• Avoidance of Avoidance of exposureexposure to to mosquitoes at their peak mosquitoes at their peak feeding timesfeeding times
• Use of insect Use of insect repellentsrepellents (DEET 10-35%)(DEET 10-35%)
• Use of Use of bed netsbed nets

71
Anti malarial drugs
Drug UsageMefloquine
Atovaquone-proguanil
Doxycycline
Chloroquine
Used in areas where chloroquine resistant malaria has been reported
As alternative to mefloquine or doxycycline
As alternative to mefloquine or ato.-prog.
Used in areas where chloroquine resistant malaria has not been reported

72
Primary prevention Primary prevention Chemoprophylaxis (1)Chemoprophylaxis (1)• Depends on knowledge of local Depends on knowledge of local
patterns of:patterns of:• Drug Drug sensitivitysensitivity & Resistance & Resistance• Likelihood of Likelihood of acquiringacquiring
malarial infectionmalarial infection

73
• When there is uncertainty, drugs When there is uncertainty, drugs effective against resistant effective against resistant p. falciparum should be usedp. falciparum should be used
• Mefloquie Mefloquie • Atovaquone-proguanilAtovaquone-proguanil• Doxycycline Doxycycline • Primaquine Primaquine
• Chemoprophylaxis is never Chemoprophylaxis is never entirely reliableentirely reliable
Chemoprophylaxis (2) Chemoprophylaxis (2)

74
Chemoprophylaxis (3) Chemoprophylaxis (3) Pregnant womenPregnant women
• If travelling to malarious areas If travelling to malarious areas should be should be warnedwarned
• In endemic areas they should In endemic areas they should receive receive prophylaxisprophylaxis : :
• ChloroquineChloroquine 300 mg weekly alone or with 300 mg weekly alone or with proguanilproguanil 200 mg daily) or . . .200 mg daily) or . . .

75
Chemoprophylaxis (4) Chemoprophylaxis (4) Children Children
• Children borne to Children borne to non immune non immune mothersmothers in endemic areas in endemic areas
• Intermittent prophylaxisIntermittent prophylaxis

76
Chemoprophylaxis (5) Chemoprophylaxis (5) Travelers Travelers
• Should start taking anti malarial drugs Should start taking anti malarial drugs at least at least 1 week before1 week before departure departure
• Should continue for Should continue for 4 weeks after4 weeks after has has left the endemic arealeft the endemic area
• If If atovaquone-proguanilatovaquone-proguanil or or primaquineprimaquine has been taken, only for has been taken, only for 1 week1 week after after departure departure

77
Chemoprophylaxis (6) Chemoprophylaxis (6) Mefloquine Mefloquine
• 250250 mg weekly in adults mg weekly in adults • Is choice for much of the Is choice for much of the tropicstropics • Effective against Effective against MDRMDR f. malaria f. malaria• Well Well toleratedtolerated• Mild Mild nauseanausea, dizziness, . . . , dizziness, . . . • During pregnancy is uncertain During pregnancy is uncertain

78
Chemoprophylaxis (7) Chemoprophylaxis (7) Atovaquone-proguanil Atovaquone-proguanil • 250/100250/100 mg once daily mg once daily• Very well Very well toleratedtolerated• Fewer adverseFewer adverse effects effects • Effective against all types of malaria Effective against all types of malaria • May be discontinued May be discontinued 1 week1 week after after
departuredeparture• Insufficient data on safety in Insufficient data on safety in pregnancypregnancy

79
Chemoprophylaxis (8) Chemoprophylaxis (8) Doxycycline Doxycycline
• 100 mg daily100 mg daily• Effective alternative to mefloquine Effective alternative to mefloquine • Well tolerated Well tolerated • May cause May cause vulvovaginal thrushvulvovaginal thrush, ,
diarrhoeadiarrhoea, , photosensitivityphotosensitivity• Can not be used by Can not be used by childrenchildren < 8 years < 8 years• Can not be used by Can not be used by pregnantpregnant women women

80
Chemoprophylaxis (9) Chemoprophylaxis (9) Chloroquine Chloroquine
• Drug of choice for drug-sensitive p. f. Drug of choice for drug-sensitive p. f. and the other human species and the other human species
• Resistant p. vivax in :Resistant p. vivax in :• Eastern AsiaEastern Asia• OceaniaOceania• Central and South AmericaCentral and South America
Resistant p. falciparum in :Resistant p. falciparum in :• Many parts of the worldMany parts of the world

81
Chemoprophylaxis (10) Chemoprophylaxis (10) Chloroquine Chloroquine
• Safe in Safe in pregnancypregnancy • RetinopathyRetinopathy if for more than 5 years if for more than 5 years• AmodiaquineAmodiaquine is associated with a is associated with a
high risk of agranulocytosis high risk of agranulocytosis

82
Chemoprophylaxis (11) Chemoprophylaxis (11) Primaquine Primaquine
• 30 mg30 mg daily daily• Effective in prevention of Effective in prevention of DR malariaDR malaria• Abdominal painAbdominal pain• Oxidant hemolysisOxidant hemolysis • Should not give to Should not give to G6PDDG6PDD persons persons• Should not give to Should not give to pregnantpregnant & & neonateneonate

83
Current programmesCurrent programmes
• Roll Back Malaria global partnership (Roll Back Malaria global partnership (WHOWHO))• Mosquito breeding sites: Mosquito breeding sites: Draining, Draining,
insecticide against larvaeinsecticide against larvae• House spraying:House spraying: Newer insecticides Newer insecticides• Insecticide-treated bed netsInsecticide-treated bed nets: : AnophelesAnopheles
bite at nightbite at night• Chemotherapy:Chemotherapy: Artemisinin-based Artemisinin-based
combination therapies (ACTs)combination therapies (ACTs)• VaccinesVaccines: Poor results to date: Poor results to date

84
2 - 2 - Secondary Prevention:Secondary Prevention:
IdentificationIdentification
AndAnd
interventionintervention
in early stages of in early stages of diseasedisease

85
DiagnosisDiagnosis
• Blood smearsBlood smears – Most common methodMost common method– Giemsa stainGiemsa stain
SerodiagnosisSerodiagnosis Immune response for years after Immune response for years after
disappearance of the parasitedisappearance of the parasite Used mostly for returning western Used mostly for returning western
travellers.travellers.

86
Specific treatmentSpecific treatment
P. vivax, P. ovale, P. malariae P. vivax, P. ovale, P. malariae and chloroquine-susceptible P. and chloroquine-susceptible P. falciparum :falciparum :
• 600 mg base chloroquine PO initially, 600 mg base chloroquine PO initially,
• followed by an additional 300 mg base followed by an additional 300 mg base 6 hr later, and again 6 hr later, and again
• On days 2 and 3 On days 2 and 3

87
Specific treatmentSpecific treatment
Chloroquine-resistant P. falciparum Chloroquine-resistant P. falciparum Drugs of choice Drugs of choice
QuinineQuinine sulfate 650 mg every 8 hr × 3–7 d sulfate 650 mg every 8 hr × 3–7 dplusplusDoxycyclineDoxycycline 100 mg bid × 7 d 100 mg bid × 7 dororQuinineQuinine followed by followed by FancidarFancidar, 3 tablets on , 3 tablets on the last day of quinine treatment the last day of quinine treatment

88
Specific treatmentSpecific treatmentChloroquine-resistant P. falciparum Chloroquine-resistant P. falciparum AlternativesAlternativesQuinineQuinine followed by followed by clindamycinclindamycin 900 mg tid × 5 days 900 mg tid × 5 days
ororMefloquineMefloquine 1250 single dose 1250 single doseororHalofantrineHalofantrine 500 mg every 6 hr × 3 doses, repeat 1 500 mg every 6 hr × 3 doses, repeat 1 wk laterwk laterororAtovaquoneAtovaquone 1000 mg daily × 3 d plus proguanil 1000 mg daily × 3 d plus proguanil 400 mg daily × 3 d 400 mg daily × 3 d

89
Specific treatmentSpecific treatmentChloroquine-resistant P. falciparum Chloroquine-resistant P. falciparum AlternativesAlternativesoror
AtovaquoneAtovaquone 1000 mg daily × 3 d plus 1000 mg daily × 3 d plus doxycyclinedoxycycline 100 mg bid × 3 days100 mg bid × 3 days
oror
ArtesunateArtesunate 4 mg/kg daily × 3 d plus 4 mg/kg daily × 3 d plus mefloquinemefloquine 1250 single dose (750 mg followed 12 hr later by 1250 single dose (750 mg followed 12 hr later by 500 mg) 500 mg)

90
Specific treatmentSpecific treatment
Parenteral regimensParenteral regimens• Quinidine gluconate 10 mg /kg loading Quinidine gluconate 10 mg /kg loading
dose (max 600 mg) in normal saline dose (max 600 mg) in normal saline infused slowly over 1–2 hr, followed by infused slowly over 1–2 hr, followed by
• Continuous infusion of 0.02 mg/kg/min Continuous infusion of 0.02 mg/kg/min until patient is able to begin oral until patient is able to begin oral treatment treatment

91
Specific treatmentSpecific treatment
OrOr
QuinineQuinine dihydrochloride 20 mg salt/kg dihydrochloride 20 mg salt/kg loading dose in 5% dextrose over 4 hr, loading dose in 5% dextrose over 4 hr, followed by 10 mg salt/kg over 2–4 hr followed by 10 mg salt/kg over 2–4 hr every 8 hr (max 1800 mg/d) until every 8 hr (max 1800 mg/d) until patient is able to begin oral treatment patient is able to begin oral treatment
ArtemetherArtemether 3.2 mg/kg intramuscularly, 3.2 mg/kg intramuscularly, then 1.6 mg/kg daily × 3 d then 1.6 mg/kg daily × 3 d

92
Specific treatmentSpecific treatment
Prevention of Relapse Due to Prevention of Relapse Due to P. Vivax or P. Ovale P. Vivax or P. Ovale
Primaquine phosphate 15.3 mg Primaquine phosphate 15.3 mg base per day PO for 14 daysbase per day PO for 14 days
oror
45 mg base per week × 8 wk 45 mg base per week × 8 wk

93
Drug resistanceDrug resistance
• Particular to Particular to P. falciparumP. falciparum but spreading to other but spreading to other speciesspecies
• Resistance to Resistance to chloroquinechloroquine most widespread but also most widespread but also newer drugsnewer drugs

94
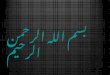
Chloroquine-resistant P. falciparumChloroquine-sensitive malaria
Chloroquine-resistant Chloroquine-resistant P. falciparumP. falciparum, 1995, 1995
CDC
200 million clinical cases annually

95
Artemisinin Artemisinin or Qinghaosu ("ching-how-soo")or Qinghaosu ("ching-how-soo")
• Active principal of Chinese medicinal Active principal of Chinese medicinal herb herb Artemisia annua. - Artemisia annua. - used to treat used to treat fevers in China for more than 1000 fevers in China for more than 1000 years.years.
– Terpinoid active anti-malarial Terpinoid active anti-malarial constituents isolated in 1971. constituents isolated in 1971.
- artesunate artemether and arteether- artesunate artemether and arteether
– Activated by parasite-digested haem – Activated by parasite-digested haem – free radical formed that kills free radical formed that kills PlasmodiumPlasmodium..
– Short half-life.Short half-life.
– Used in combination with other drugs. Used in combination with other drugs.

96
3 - 3 - Tertiary Prevention:Tertiary Prevention:
• Treatment of complications Treatment of complications

97
Sources :
• Control of communicable diseases, 2000• Nicholas J. White, Joel G. Breman, Malaria and Babesiosis in Harrison’s principles of internal medicine, 16th ed. 2005• Mandell 2000• BSL 2014, Parasites and Pathogens of Man, Dr Ron Stanley• Nicole T. McCadie, The Impact of Global The Impact of Global Change on the Spread of MalariaChange on the Spread of Malaria