Embed Size (px)
Citation preview

1
DO COMMUNITY-BASED OUTREACH PROGRAMS REDUCE HIV RISK
BEHAVIORS AND HIV INFECTION?
Vietnam Ministry of Health and US Centers for Disease Control and Prevention
Workshop on Preventing HIV Transmission in Injection Drug Users and Other Vulnerable
Populations
Hanoi, September, 2003Sherry Deren, Ph.D., Richard Needle, Ph.D.,
and Dave Burrows, Ph.D.

What is Community-Based Outreach?
A strategy for providing health-related services by delivering the services to individuals in their own community, where they live or spend time (“reaching out” to the population”)
Outreach activities can include:• Education, giving information• Providing materials for health promotion• Reinforcing positive behavior change• Identifying service needs and providing
referrals• Recruitment for research or service projects
3
What are the Advantages of Conducting Community-Based Outreach with Injection
Drug Users (IDUs)?
• Can contact individuals who may not utilize institution-based services
• Can adapt outreach methods, information and services to different communities, populations and individuals
• Can influence social networks of drug users

4
Research Questions Regarding Effectiveness of Outreach Among IDUs
• Do outreach efforts contact hard-to-reach hidden populations of IDUs?
• Do IDUs who receive outreach services reduce their risk behaviors?
• Do communities with outreach services have lower rates of HIV infection?
• In communities where outreach services are associated with reductions in risk behaviors or infection rates, could there be other explanations for these findings?
5
Sources of Evidence-Based Information
• Review of published literature and program reports• Examination of data from multi-site and single site
studies• Searches supplemented by requests to GRN
members and other organizations to identify studies and reports of outreach efforts throughout the world
• Review of studies that examine alternative explanations for findings related to outreach

6
Criteria to Evaluate Scientific Causation (Sir Bradford Hill, 1966)
• Temporal Relationship- appropriate time sequence between intervention and outcomes
• Consistency of findings- similar associations are found by different investigators, in different populations, under different circumstances
• Strength of association between the intervention and the outcomes
• Specificity- association of intervention and outcome
• Plausibility- the association fits with previously existing knowledge
7
Evaluated Community-Based Outreach Models
• Indigenous Leader Outreach Model
• Community Health Outreach Worker Model
• National Institute on Drug Abuse Outreach Models
• Peer Driven Intervention
• Outreach in Natural Settings
• Kazan (RF) Outreach Model
• Wiebel et al, 1986
• Mid-City Consortium, 1986
• NIDA, 1987-1991, 1991-1998
• Broadhead et al., 1996
• Latkin et al., 1996
• Badrieva et al., 1999
8
Do Outreach Efforts Contact Hard-to-Reach Hidden Populations of IDUs?
• Among IDUs reached through outreach efforts, almost one-half had never been in drug treatment (Brown and Needle, 1994)
• Outreach is more likely to reach and refer higher risk IDUs (more sharing, more HIV positive) than those attending STD or VCT clinics (Rasmussen 2002)
• Reached higher risk IDUs (more recent drug use, more sharing) than those entering treatment from other sources (Dorsey et al., 1999)
• However, it is difficult to determine the proportion of the IDU population reached in communities, because good estimations of the size of this population are difficult to obtain

9
Do IDUs Who Receive Outreach Services Reduce Their Risk Behaviors?-Summary of Studies of Outreach-Based Programs
(Needle and Coyle, 1998, with updates)
Stopped injection use Reduced injection frequency Stopped/reduced sharing of
needles/syringes Stopped/reduced sharing of
other injection equipment Increased needle disinfection Increased condoms
10/11 17/18 18/22
9/13
10/16 17/19

10
Other Outcomes of Outreach Services: Referrals and Utilization of Services
• Entered drug treatment
• Reentry into drug treatment
• Increased uptake of VCT by high risk IDUs
• 8/9 studies
• Goldstein et al., 2001
• Rasmussen (2002), Dorsey et al., (1999)

11
Effectiveness of Outreach-based Strategies in Reducing Drug Use and Needle Practices
Behavioral OutcomeNumber of Findings
Median at
Baseline
Range of Change at Follow-up
Median Change at Follow-up
Stopped injecting drugs at time of follow-up
5 100% injected24% to 31% of IDUs stopped
injecting
26% of IDUs stopped injecting
Reduced drug injection frequency
773 injections per
month
11 to 62 fewer injections per
month
28 fewer injections per
month
Stopped/reduced reuse of needles/syringes
437% reused
syringes
14% to 43% fewer IDUs
reused syringes
19% fewer IDUs reused syringes
Stopped/reduced reuse of cookers, cotton, rinse water
467% reused equipment
16% to 34% fewer IDUs
reused equipment
27% fewer IDUs reused
equipment

12
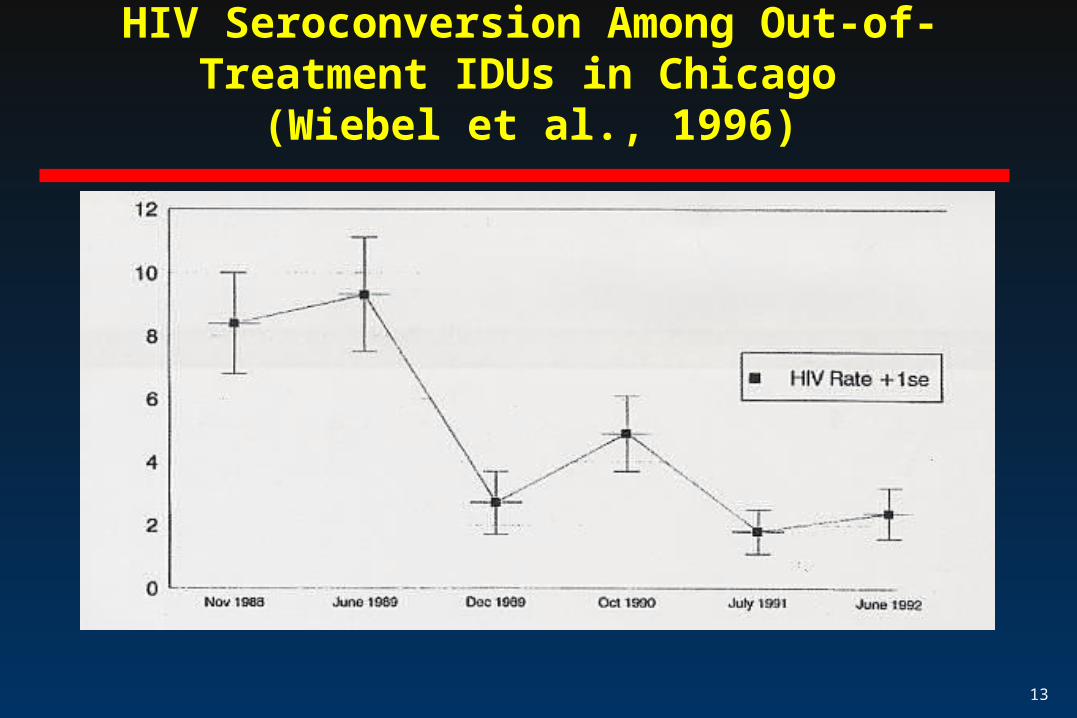
Changes in Risk Behaviors are Associated with Lower Rates of New HIV infections
(Wiebel et al., 1996)
• Multi-year study in Chicago, Illinois, USA• 6 waves, serological and behavioral data, 1988-92: 641
IDUs• Injection risk declined from 54%(Wave 1) to 14% (Wave 6)• Seroincidence declined from 8.4 (Wave 1) to 2.4 (Wave 6)• Injection risk only factor associated with HIV infection• Non-equivalent control group of IDUs-50% report needle risk
compared to 14% in the outreach group
13
HIV Seroconversion Among Out-of-Treatment IDUs in Chicago
(Wiebel et al., 1996)

14
Examination of Alternative Explanations for Research Findings Regarding Outreach
• Studies have shown that findings related to outreach are not due to other possible factors, such as:
- secular trends (Neaigus et al., 1990; Colón et al., 1995)
- impact of the research interview (Simpson et al., 1994)
15
Is Outreach Cost-Effective?
• Cost effectiveness estimates were developed for outreach-based interventions for IDUs in 8 U.S. communities (Pinkerton et al., 2000)
• To calculate cost effectiveness, the following were used:- estimated number of infections prevented- calculated savings in averted HIV/AIDS medical care costs
and quality-adjusted years of life- compared averted costs with the cost of implementing the
intervention• The interventions were cost-effective in all 8 communities
16
Outreach Works in Combination with Other Strategies
• Studies of “prevented epidemics” have found that the combination of outreach, access to sterile syringes and starting prevention activities early in an IDU epidemic can help prevent a large epidemic (Des Jarlais et al., 1998)
• In New York, the reduction in HIV seroprevalence (from approximately 50% to below 30%) and incidence (from approximately 13 to 1 per 100 person-years at risk) from the mid 1980s to the mid 1990s, suggest that large high-seroprevalence epidemic can be reversed by a combination of strategies, including outreach, access to sterile syringes, voluntary counseling and testing, and drug treatment services (Des Jarlais et al., 2002).

17
Global Diffusion of Community-Based Outreach Programs for IDUs
• North America-U.S., and most countries in Western Europe reached large numbers of IDUs
• Asia and Pacific-Australia and New Zealand, Bangladesh, have reached large majority of IDUs
• Central and Eastern Europe-very few countries reaching majority of IDUs-some exceptions
• Latin America- Brazil and Argentina • Africa and Middle East—no programs reported
18
Community-Based Outreach in Madras, India(Kumar, Mudaliar and Daniels,1998)
• Street recruitment of two groups IDUs (outreach and control) in two different locations
• Outreach group received information, risk reduction supplies and referrals by recovering drug users
• Control group did not receive outreach services• 18 month follow-up, outreach group reports fewer
injection risk behaviors, but no changes in sexual risk behaviors

19
Summary of Findings on Community-Based Outreach
• Reaches high-risk populations • Results in reductions in risk behaviors and reduction in
seroconversions• Outreach referrals lead to increases in utilization of
other services (e.g., drug abuse treatment, VCT) • Cost effectiveness established

20
Limitation of Findings
• Most of the published studies on effectiveness are based on data from the United States
• Data for comparative analysis of implementation of outreach strategies are limited
21
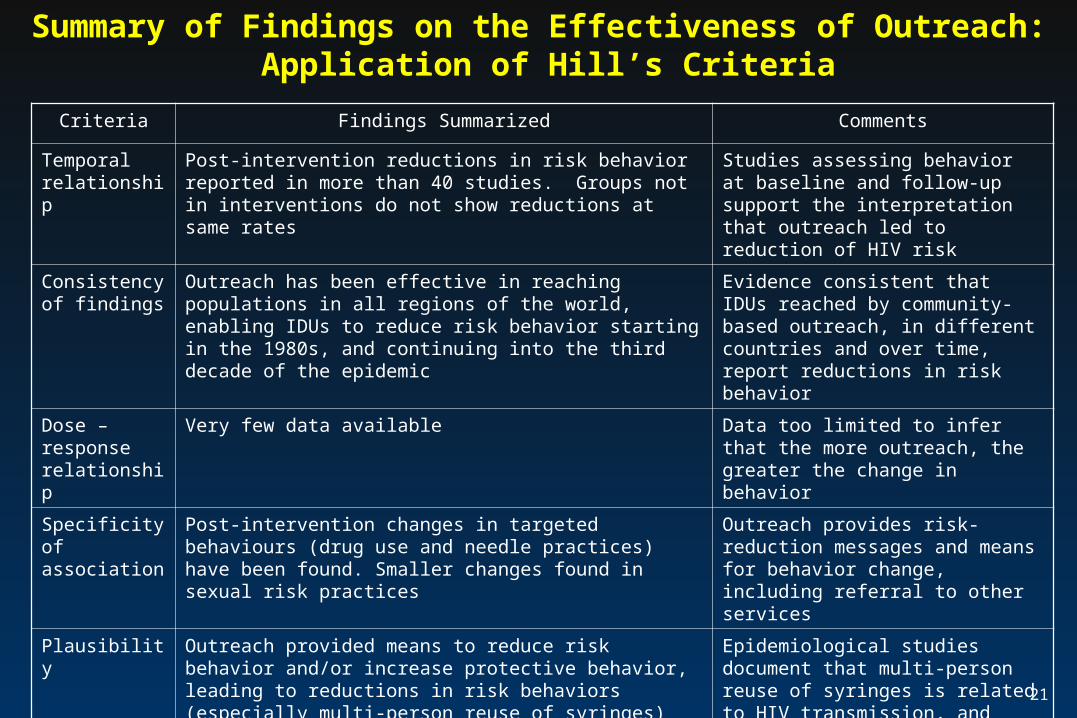
Summary of Findings on the Effectiveness of Outreach: Application of Hill’s Criteria
Criteria Findings Summarized Comments
Temporal relationship
Post-intervention reductions in risk behavior reported in more than 40 studies. Groups not in interventions do not show reductions at same rates
Studies assessing behavior at baseline and follow-up support the interpretation that outreach led to reduction of HIV risk
Consistency of findings
Outreach has been effective in reaching populations in all regions of the world, enabling IDUs to reduce risk behavior starting in the 1980s, and continuing into the third decade of the epidemic
Evidence consistent that IDUs reached by community-based outreach, in different countries and over time, report reductions in risk behavior
Dose –response relationship
Very few data available Data too limited to infer that the more outreach, the greater the change in behavior
Specificity of association
Post-intervention changes in targeted behaviours (drug use and needle practices) have been found. Smaller changes found in sexual risk practices
Outreach provides risk-reduction messages and means for behavior change, including referral to other services
Plausibility Outreach provided means to reduce risk behavior and/or increase protective behavior, leading to reductions in risk behaviors (especially multi-person reuse of syringes) and in incidence of HIV transmission
Epidemiological studies document that multi-person reuse of syringes is related to HIV transmission, and evaluation studies of outreach indicate that outreach enables IDUS to reduce HIV risk and transmission
22
Conclusions
• Evidence-based findings meet criteria for scientific causality
• Need to implement on broader international scale
• Need for more countries to publish evidence-based studies on effectiveness of community-based outreach