Embed Size (px)
Citation preview

1
ChenMed Care Model: Creating Change and Transformation in General Practice
November , 6th, 2014

2
Average per capita health care costs by number of chronic
conditions
Source: Medical Expenditure Panel Survey, 2006
Chronic conditions drive health care spending, especially in Medicare
Medicare spending for patients with 5+ chronic conditions
1987
1997
2002
0% 10% 20% 30% 40% 50% 60% 70% 80%
52%
65%
76%

3
Who we are: Privately held, primary care-led physician group
Our focus: Low to moderate income adults > 55 with multiple chronic conditions in urban areas. Typical patient searches for a PCP every 18 months, often considered “frequent flyers” by other health systems.
Care model: 400-450 patients per PCP; on-site Rx, focus on culture, patient relationships, decision making, customized information technology, intensive care coordination
Scale: Designed to scale quickly; Growth from 5 centers in Miami market in 2010E to 36 centers in 8 markets at 2013E . 40+k risk lives in 2014.
Payment: Global risk adjusted capitation from Medicare Advantage plans
Snapshot of ChenMed

4
This approach is fundamentally different
ChenMed Typical ACO
Population focus
Low to moderate income MA population
Commercial insurance, multiple types
Payor Primarily one, capitated
Multiple, FFS economics still preeminent
Strategy Start with getting
doctor-patient relationship right
Evidence based guidelines, operational
processes
Governance Primary care led Complex, multi-specialty, multi-facility
Ability to scale High Low
Upfront integration challenges
Low High
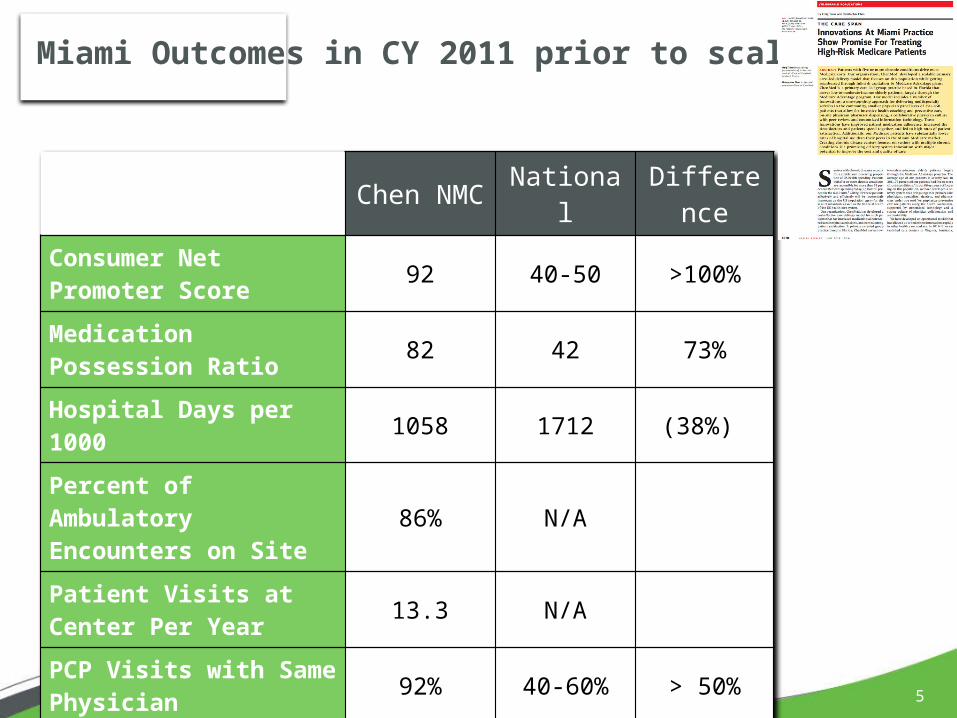
5
Chen NMC National Difference
Consumer Net Promoter Score 92 40-50 >100%
Medication Possession Ratio 82 42 73%
Hospital Days per 1000 1058 1712 (38%)
Percent of Ambulatory Encounters on Site
86% N/A
Patient Visits at Center Per Year 13.3 N/A
PCP Visits with Same Physician 92% 40-60% > 50%
Miami Outcomes in CY 2011 prior to scaling

6
Designing the operations of a focused factory
One-stop shopping enhances coordination, collaboration, convenience, and compliance
Reproducible layout resembles an Ambulatory ICU• Primary care doctors lead the care team and do not have
private offices• Onsite specialists to encourage physician to physician dialogue • Onsite supportive services for convenience• Capacity to keep patients out of hospital (e.g., IV Antibiotics,
Diuresis)
Door-to-doctor transportation to our clinical sites improves access to care

7
Focus creates the potential for strategic design
▪ Hire staff who are passionate about this patient segment with right skills
▪ Engineer tighter integration and links in every process
▪ Test multiple changes in different markets
▪ Streamlined organizational governance
▪ > 70% of Medicare costs driven by patients with > 4 conditions
▪ Changes in outcomes can be measured in months
Faster change cycles
Impact easier to measure
Payor collaboration
▪ JV allows for rationalization of care programs between payor and provider (e.g., analytics, care coordination, specialized programs)
▪ Don’t focus on fee for service demands
▪ Operational challenges dramatically reduced
Specialized staff and processes
Reduces complexity

8
Manage across
transitions
▪ Build in continuity where possible; hospitalist follows patients to first follow-up visit
▪ PCP and NP joint SNF decision-making
▪ Initial home assessment
▪ Interdisciplinary weekly team meetings by center
Design around access
▪ One stop shop – most patients within 7 miles ; transportation
▪ On-site physician drug dispensing
▪ Wellness focused activities on-site
▪ Not looking to be a complete multi-specialty group, but invite external specialists on-site as feasible and practical
Build up care team
▪ Nurse case manager, social worker, transitions team
▪ Developing medical assistants as coaches
▪ Qualitative judgment – the worry index
▪ Develop relationships with trusted specialists over time
Integrating primary care decisions around the patient

9
Physician culture is critical to get care right “from the inside out”

10
Building the right culture requires changing mindsets and behaviors
Role-modeling
Behavior and mindset shifts
Developing talent and skills
Reinforcing with formal mechanisms
Fostering understanding and convictions
The McKinsey influence model
“I see superiors, peers, and subordinates behaving in the new way”
“I know what is expected of me – I agree with it, and it is meaningful
“I have the skills and competencies to behave in the new way”
“The structures, processes, and systems reinforce the change in behavior I am being asked to make”
• Changes in mindsets and behaviors need to happen at all levels of the organization, starting with
– Front-line physicians
– Clinical team
– Physician leadership
• None of the changes in behaviors and mindsets can be mandated or dictated – each will require a coordinated set of influencing tactics to ensure traction in the organization

11
CMS risk scores
Real-time internal HEDIS Metrics
Real-time patient flow metrics (i.e. wait times)
Comprehensive outpatient clinical data, digitized and scanned
• Hospital Admissions & Readmissions
• Real-time inpatient clinical data
Claims Data• Part A• Part B• Part D
MRANet Promoter Scores / Customer Feedback
Predictive Modeling data from Envita and Humana
Providing a suite of tools to optimise decision making in the exam room

12
Using Visualization Tools to help a Physician Manage Her Panel of 450 High Risk patients

13
A care timeline is used to integrate claims, referrals and hospital data for high cost case management

14
Dash2Go

15
▪ 3 times a week review of patient care by the physician group
▪ Transparent review of outcomes with all physicians
▪ Entire team owns the relationship
▪ Relationship evolves over time
▪ >85% of the touch-points
Focus on the patient
relationship
Physician decision-making
▪ Selection and culture
▪ Decision support at point of care
▪ Positive incentives – the “tuned” patient panel
Convenience matters
▪ Redesigned system of on-site physician drug dispensing dramatically improves adherence
▪ On-site behavioral health model coordination
Communication
▪ Coordination of care
▪ Specialist – PCP communication in person
▪ Team conferences
What are the key drivers of success in integrated care?





























