Embed Size (px)
Citation preview

1
Better Balance Coaching Research: Design and methodologies
Trine Wulff, Bispebjerg University Hospital, Copenhagen, Denmark
Agenda
1. Project vision
2. Intervention
3. Study design
4. Qualitative analyses (IPA etc): Today’s primary focus!
5. Quantitative analysis
6. Perspectives
7. Discussion

Better Balance Coaching Research: Design and methodologiesHandout, action research course participants, May 2009. Trine Wulff, Bispebjerg Hospital, Denmark
1. Project Vision: Promoting the engagement of older people in activities to prevent falls
4. Intervention phase. Coach/researcher made dense coach notes while executing study. Supervision system: Clinical supervisor and coach supervisor (ad hoc). Presentation of study for audiences, including reflective Q/A sessions. Coachee learning was challenged and verbalised in completion sessions
2. Development of intervention: Cyclic approach. Theories (fall prevention, geront., coaching, pos psych, health psych, etc), Coaching skills (CPCC educ incl. supervision, PLUS complement. methods), Interaction with target group (coachings, interviews, training partic. etc), Interaction with experts (clinicians, coaches, psychologists, health researchers), Development of coaching manual, templates and coachee handbook
8. Quantitative empirical material. 34 + 40 participants included. Participant testing and interviewing at baseline and 9 months. Self-reported no. of falls (1y), Data from primary care and hospitals, 9 months
7. Qualitative analyses (current plan, may be adjusted)
Analysis 1: Interpretative Phenomenological Analysis (Smith, Jarman, Osborn) added ”Working with mysteries and breakdown”(Alvesson, Kärreman). What incidences make elderly people being coached after fall accidents change health beliefs and/or health behaviours? Why do some elderly people being coached after fall accidents NOT change health beliefs and/or health behaviours? How do healthcare professionals impact health beliefs and health behaviours of elderly people being coached after fall accidents? Any mysteries, that can not be explained with current theories? (New theory to be generated…)
Analysis 2: How can coaching reduce fear of falling?
Analysis 3: How do elderly people being coached after fall accidents explain/justify their executed health behaviours?
9. Quantitative analysis. Number of fall incidents, hospital admissions and selected primary care services (emergency calls, delivered food, home services etc). Baseline: MMSE, social and drinking patterns, etc. Functional parameters relevant for fall prevention. Psychosocial parameters, QoL, Fear of falling, etc. Due to Type II error, no significant differences are expected
5. Qualitative focus. Qualitative interest intensified during intervention phase. Collecting qualitative material and acquiring qualitative analytical skills. Pilot analyses incl. feedback (discourse and hermeneutic approaches). Qualitative researchers suggesting different methods of analyses
6. Qualitative empirical material. 356 coaching sessions, 205 hours in totalDense coach notes from all sessions, plus additional notes/commentsTaping of approximately 75 sessions
3. Development of RCT study design. Max 6 months, max 10 hr’s, max 15 sessions: Home (2) and phone (13). Dimensioning: 2x60 part’s adequate based on hypothesis. Target: 2x90! 65+ y with fall history enrolled from hospital and training centres in Cph. Intervention: BB Coaching and usual care. Control: Usual care. Physiotherapists included and tested participants in a blinded manner
10. Project context. The coaching study is part of the project: “Better Balance – fall prevention among elderly people”, supported by the Danish Ministry of Health and Prevention. The project also includes a randomised, controlled trial of an integrated nurse approach as well as an analysis of the situation for elderly people who go to a hospital’s emergency department due to fall accidents. Contact person: Trine Wulff, Department of integrated health care, Bispebjerg University Hospital, email [email protected]

3
Project vision
Better Balance Coaching, Trine Wulff, 2009
Promoting the engagement of older people in activities to prevent falls
1. Promoting the engagement
2. of older people
3. in activities
4. to prevent falls

4
Background
• Falling is the most frequent accident among older people.
• Many falls lead to serious injuries. Falling doubles the risk of new falls.
• Specific training modalities are likely to prevent falls
• Older people are not motivated to participate in fall-preventive activities
• Down to 10% participation in interventions
• Low adherence/high drop out-rates
Better Balance Coaching, Trine Wulff, 2009

5
Recommendations for promoting the engagement of older people in fall preventive health care
1. Promoting the benefits fitting to a positive self-identity
2. Tailoring interventions to meet needs, preferences and capabilities of the individual
3. Encouraging confidence in self-management rather than dependence on professionals by giving older people an active role
Reference: ProFaNE (Prevention of Falls Network Europe) Work Package 4 – psychological aspects of falling
Better Balance Coaching, Trine Wulff, 2009

Better Balance Coaching Research: Design and methodologiesHandout, action research course participants, May 2009. Trine Wulff, Bispebjerg Hospital, Denmark
1. Project Vision: Promoting the engagement of older people in activities to prevent falls
4. Intervention phase. Coach/researcher made dense coach notes while executing study. Supervision system: Clinical supervisor and coach supervisor (ad hoc). Presentation of study for audiences, including reflective Q/A sessions. Coachee learning was challenged and verbalised in completion sessions
2. Development of intervention: Cyclic approach. Theories (fall prevention, geront., coaching, pos psych, health psych, etc), Coaching skills (CPCC educ incl. supervision, PLUS complement. methods), Interaction with target group (coachings, interviews, training partic. etc), Interaction with experts (clinicians, coaches, psychologists, health researchers), Development of coaching manual, templates and coachee handbook
8. Quantitative empirical material. 34 + 40 participants included. Participant testing and interviewing at baseline and 9 months. Self-reported no. of falls (1y), Data from primary care and hospitals, 9 months
7. Qualitative analyses (current plan, may be adjusted)
Analysis 1: Interpretative Phenomenological Analysis (Smith, Jarman, Osborn) added ”Working with mysteries and breakdown”(Alvesson, Kärreman). What incidences make elderly people being coached after fall accidents change health beliefs and/or health behaviours? Why do some elderly people being coached after fall accidents NOT change health beliefs and/or health behaviours? How do healthcare professionals impact health beliefs and health behaviours of elderly people being coached after fall accidents? Any mysteries, that can not be explained with current theories? (New theory to be generated…)
Analysis 2: How can coaching reduce fear of falling?
Analysis 3: How do elderly people being coached after fall accidents explain/justify their executed health behaviours?
9. Quantitative analysis. Number of fall incidents, hospital admissions and selected primary care services (emergency calls, delivered food, home services etc). Baseline: MMSE, social and drinking patterns, etc. Functional parameters relevant for fall prevention. Psychosocial parameters, QoL, Fear of falling, etc. Due to Type II error, no significant differences are expected
5. Qualitative focus. Qualitative interest intensified during intervention phase. Collecting qualitative material and acquiring qualitative analytical skills. Pilot analyses incl. feedback (discourse and hermeneutic approaches). Qualitative researchers suggesting different methods of analyses
6. Qualitative empirical material. 356 coaching sessions, 205 hours in totalDense coach notes from all sessions, plus additional notes/commentsTaping of approximately 75 sessions
3. Development of RCT study design. Max 6 months, max 10 hr’s, max 15 sessions: Home (2) and phone (13). Dimensioning: 2x60 part’s adequate based on hypothesis. Target: 2x90! 65+ y with fall history enrolled from hospital and training centres in Cph. Intervention: BB Coaching and usual care. Control: Usual care. Physiotherapists included and tested participants in a blinded manner
10. Project context. The coaching study is part of the project: “Better Balance – fall prevention among elderly people”, supported by the Danish Ministry of Health and Prevention. The project also includes a randomised, controlled trial of an integrated nurse approach as well as an analysis of the situation for elderly people who go to a hospital’s emergency department due to fall accidents. Contact person: Trine Wulff, Department of integrated health care, Bispebjerg University Hospital, email [email protected]

7
Intervention
Better Balance Coaching, Trine Wulff, 2009
1. Development of intervention
2. Intervention

8
Development of intervention: Cyclic approach
Better Balance Coaching, Trine Wulff, 2009
• Theories (fall prevention, gerontology, coaching, positive psychology, health psychology, etc), Coaching skills (CPCC education incl. supervision, PLUS complementary methods)
• Interaction with target group (coaching sessions, interviews, training participation etc)
• Interaction with experts (clinicians, coaches, psychologists, health researchers)
• Development of coaching manual, templates and coachee handbook

9
Intervention
Better Balance Coaching, Trine Wulff, 2009
1. Use of Better Balance Coaching method: Integrative health coaching model with elements from coaching, e.g. positive psychology-principles and cognitive coaching, as well as health psychology
2. Coaching period: Max 6 months
3. Coaching time: Max 10 hours
4. Number of sessions: Max 15 sessions: Home (2) and phone (13).
5. Intervention phase: Coach/researcher made dense coach notes while executing study. Supervision system: Clinical supervisor and coach supervisor (ad hoc). Presentation of study for audiences, including reflective Q/A sessions. Coachee learning was challenged and verbalised in completion sessions

10
Case: Gudrun
Better Balance Coaching, Trine Wulff, 2009
• Coachee: 73 year old divorced woman living alone in her private apartment• Latest job: Responsible for a restaurant in a Famous Deer Garden• Network: Children, grandchildren and a competent bridge partner…• Has lost weight: From 70 to 46 kg. Dislikes artificial protein drinks,fat food, etc.• Was recently hospitalized due to functional decline• Has been falling a number of times in her apartment • Outpatient collaboration with Geriatrics Department to unravel any underlying
diseases explaining her fall tendency• Thanked no to suggested participation in balance training at the hospital
Coaching aims/targets defined in the beginning of the collaboration:
• I wish… my back pain was decreased, I had more strength in my arms, and I ate more vegetables.
• If I succeed, I will be able to… become more mobile, get more energy and bring my rollator in the bus
• If I am able to do that, my life is better, because… I can choose to get new impressions: Deer Garden, Tivoli, Zoo, etc

Better Balance Coaching Research: Design and methodologiesHandout, action research course participants, May 2009. Trine Wulff, Bispebjerg Hospital, Denmark
1. Project Vision: Promoting the engagement of older people in activities to prevent falls
4. Intervention phase. Coach/researcher made dense coach notes while executing study. Supervision system: Clinical supervisor and coach supervisor (ad hoc). Presentation of study for audiences, including reflective Q/A sessions. Coachee learning was challenged and verbalised in completion sessions
2. Development of intervention: Cyclic approach. Theories (fall prevention, geront., coaching, pos psych, health psych, etc), Coaching skills (CPCC educ incl. supervision, PLUS complement. methods), Interaction with target group (coachings, interviews, training partic. etc), Interaction with experts (clinicians, coaches, psychologists, health researchers), Development of coaching manual, templates and coachee handbook
8. Quantitative empirical material. 34 + 40 participants included. Participant testing and interviewing at baseline and 9 months. Self-reported no. of falls (1y), Data from primary care and hospitals, 9 months
7. Qualitative analyses (current plan, may be adjusted)
Analysis 1: Interpretative Phenomenological Analysis (Smith, Jarman, Osborn) added ”Working with mysteries and breakdown”(Alvesson, Kärreman). What incidences make elderly people being coached after fall accidents change health beliefs and/or health behaviours? Why do some elderly people being coached after fall accidents NOT change health beliefs and/or health behaviours? How do healthcare professionals impact health beliefs and health behaviours of elderly people being coached after fall accidents? Any mysteries, that can not be explained with current theories? (New theory to be generated…)
Analysis 2: How can coaching reduce fear of falling?
Analysis 3: How do elderly people being coached after fall accidents explain/justify their executed health behaviours?
9. Quantitative analysis. Number of fall incidents, hospital admissions and selected primary care services (emergency calls, delivered food, home services etc). Baseline: MMSE, social and drinking patterns, etc. Functional parameters relevant for fall prevention. Psychosocial parameters, QoL, Fear of falling, etc. Due to Type II error, no significant differences are expected
5. Qualitative focus. Qualitative interest intensified during intervention phase. Collecting qualitative material and acquiring qualitative analytical skills. Pilot analyses incl. feedback (discourse and hermeneutic approaches). Qualitative researchers suggesting different methods of analyses
6. Qualitative empirical material. 356 coaching sessions, 205 hours in totalDense coach notes from all sessions, plus additional notes/commentsTaping of approximately 75 sessions
3. Development of RCT study design. Max 6 months, max 10 hr’s, max 15 sessions: Home (2) and phone (13). Dimensioning: 2x60 part’s adequate based on hypothesis. Target: 2x90! 65+ y with fall history enrolled from hospital and training centres in Cph. Intervention: BB Coaching and usual care. Control: Usual care. Physiotherapists included and tested participants in a blinded manner
10. Project context. The coaching study is part of the project: “Better Balance – fall prevention among elderly people”, supported by the Danish Ministry of Health and Prevention. The project also includes a randomised, controlled trial of an integrated nurse approach as well as an analysis of the situation for elderly people who go to a hospital’s emergency department due to fall accidents. Contact person: Trine Wulff, Department of integrated health care, Bispebjerg University Hospital, email [email protected]

12
Study design
Better Balance Coaching, Trine Wulff, 2009
• Dimensioning: 2 x 60 participants adequate, based on hypothesis
• Target: 2 x 90 participants
• Result: 34 + 40 participants (Type II error)
• People aged 65+ with fall history enrolled from hospital and training centres in Copenhagen
• Intervention: Better Balance Coaching and usual care
• Control: Usual care
• Physiotherapists included and tested participants in a blinded manner

Better Balance Coaching Research: Design and methodologiesHandout, action research course participants, May 2009. Trine Wulff, Bispebjerg Hospital, Denmark
1. Project Vision: Promoting the engagement of older people in activities to prevent falls
4. Intervention phase. Coach/researcher made dense coach notes while executing study. Supervision system: Clinical supervisor and coach supervisor (ad hoc). Presentation of study for audiences, including reflective Q/A sessions. Coachee learning was challenged and verbalised in completion sessions
2. Development of intervention: Cyclic approach. Theories (fall prevention, geront., coaching, pos psych, health psych, etc), Coaching skills (CPCC educ incl. supervision, PLUS complement. methods), Interaction with target group (coachings, interviews, training partic. etc), Interaction with experts (clinicians, coaches, psychologists, health researchers), Development of coaching manual, templates and coachee handbook
8. Quantitative empirical material. 34 + 40 participants included. Participant testing and interviewing at baseline and 9 months. Self-reported no. of falls (1y), Data from primary care and hospitals, 9 months
7. Qualitative analyses (current plan, may be adjusted)
Analysis 1: Interpretative Phenomenological Analysis (Smith, Jarman, Osborn) added ”Working with mysteries and breakdown”(Alvesson, Kärreman). What incidences make elderly people being coached after fall accidents change health beliefs and/or health behaviours? Why do some elderly people being coached after fall accidents NOT change health beliefs and/or health behaviours? How do healthcare professionals impact health beliefs and health behaviours of elderly people being coached after fall accidents? Any mysteries, that can not be explained with current theories? (New theory to be generated…)
Analysis 2: How can coaching reduce fear of falling?
Analysis 3: How do elderly people being coached after fall accidents explain/justify their executed health behaviours?
9. Quantitative analysis. Number of fall incidents, hospital admissions and selected primary care services (emergency calls, delivered food, home services etc). Baseline: MMSE, social and drinking patterns, etc. Functional parameters relevant for fall prevention. Psychosocial parameters, QoL, Fear of falling, etc. Due to Type II error, no significant differences are expected
5. Qualitative focus. Qualitative interest intensified during intervention phase. Collecting qualitative material and acquiring qualitative analytical skills. Pilot analyses incl. feedback (discourse and hermeneutic approaches). Qualitative researchers suggesting different methods of analyses
6. Qualitative empirical material. 356 coaching sessions, 205 hours in totalDense coach notes from all sessions, plus additional notes/commentsTaping of approximately 75 sessions
3. Development of RCT study design. Max 6 months, max 10 hr’s, max 15 sessions: Home (2) and phone (13). Dimensioning: 2x60 part’s adequate based on hypothesis. Target: 2x90! 65+ y with fall history enrolled from hospital and training centres in Cph. Intervention: BB Coaching and usual care. Control: Usual care. Physiotherapists included and tested participants in a blinded manner
10. Project context. The coaching study is part of the project: “Better Balance – fall prevention among elderly people”, supported by the Danish Ministry of Health and Prevention. The project also includes a randomised, controlled trial of an integrated nurse approach as well as an analysis of the situation for elderly people who go to a hospital’s emergency department due to fall accidents. Contact person: Trine Wulff, Department of integrated health care, Bispebjerg University Hospital, email [email protected]

14
Qualitative analyses
Better Balance Coaching, Trine Wulff, 2009
1. Qualitative focus
2. Qualitative empirical material
3. Qualitative analyses (current plan, may be adjusted)

15
Qualitative focus
Better Balance Coaching, Trine Wulff, 2009
• Qualitative interest intensified during intervention phase
• Collecting qualitative material and acquiring qualitative analytical skills
• Pilot analyses incl. feedback (discourse and hermeneutic approaches)
• Qualitative researchers suggesting different methods of analyses

16
Qualitative empirical material
Better Balance Coaching, Trine Wulff, 2009
• 356 coaching sessions, 205 hours in total
• Dense coach notes from all sessions, plus additional notes/comments
• Taping of approximately 75 sessions

17
Qualitative analyses(current plan, may be adjusted)
Better Balance Coaching, Trine Wulff, 2009
Project team collaborates with Susanne Reventlow on the qualitative analyses!
Analysis 1: Interpretative Phenomenological Analysis/IPA (Smith, Jarman, Osborn) added ”Working with mysteries and breakdown”(Alvesson, Kärreman).
• What incidences make elderly people being coached after fall accidents change health beliefs and/or health behaviours?
• Why do some elderly people being coached after fall accidents NOT change health beliefs and/or health behaviours?
• How do healthcare professionals impact health beliefs and health behaviours of elderly people being coached after fall accidents?
• Any mysteries, that can not be explained with current theories? (New theory to be generated…)
Analysis 2: How can coaching reduce fear of falling?
Analysis 3: How do elderly people being coached after fall accidents explain/justify their executed health behaviours?

18
What is IPA?(Interpretative Phenomenological Analysis)
Better Balance Coaching, Trine Wulff, 2009
Aim of IPA
• Explore participant’s view of the topic (phenomenological approach)
• Make sense of participant’s experiences/beliefs, based on the researcher’s personal interaction with – and interpretation of – the empirical data (interpretative approach)
• Health psychology relevance: Focus on connections between verbal report, cognition and physical state.
• Example: Explore how older people having experienced fall accidents may talk and act differently related to their health conditions.
ReferenceSmith JA, Jarman M, Osborn M (1999) Doing Interpretative Phenomenological Analysis. In Murray M, Chamberlain K (eds), Qualitative health psychology, theories and methods. London: Sage, 218-40.

19
IPA process (guideline)
Better Balance Coaching, Trine Wulff, 2009
1. Repeated reading of 1st transcript: Free notes in left margin2. Right margin: Emerging theme titles (key words)3. List of emerging themes: Look for connections, clustering4. Check connections, themes in transcripts: What is the person saying?
(Phenomenological) What is your understanding? (interpretative)5. Master list of themes, some themes may be deleted 6. Repeat 1-5 for the next transcripts, look at each transcript “afresh” (but
primed to certain aspects of the data…)7. Identify shared themes. You may choose your own strategy!8. Analyze shared themes by examining selected transcripts again, focusing
on extracts related to identified themes.9. What constitutes the shared aspects of the participants’ experience in
relation to the general theme?10. Search for patterns, connections and tensions by using diagrams, notes,
idea discussions, etc11. Write themes up to a narrative account

20
Better Balance Coaching IPA process
Better Balance Coaching, Trine Wulff, 2009
1. Creating 1 page-summaries of all coaching collaborations2. Repeated reading of summaries: What are the coachees saying and doing? What is my under-
standing? Other interesting findings? Focus on health-related conversations. Free notes in left margin
3. Categorization of coachees based on mental and physical capacities, etc4. Emerging theme titles and mysteries/breakdowns (key words) with reference to specific coachees5. Clustering of emerging themes6. Check connections, themes in summaries, sometimes combined with the underlying empirical
material: What are the coachees saying and doing? What is my understanding (interpretation)?7. Master list of shared themes. Discussions with co-researchers (C Hendriksen, S Reventlow).8. Repeat 2-6 from other perspectives. Example: Researcher interpretation, all coachees: Based on
coachee statements and actions, what would bring or brings in real life engagement/extraordinary value to coachee in relation to their coaching targets? (Blue Ocean Strategy-inspired approach)
9. Adapted master list based on 8, with identified shared themes. 10. Clustering of coachees in 5 sub-groups, based on shared themes.11. Analyze shared themes for prioritized groups by coding/examining selected empirical material again,
focusing on extracts related to identified themes. What are the coachees saying and doing? What is my understanding?
12. What constitutes the shared aspects of the groups’ experience in relation to the general theme?13. Search for patterns, connections and tensions* (*TW looks for mysteries and breakdown) by using diagrams,
notes, idea discussions, etc14. Write themes up to a narrative account

21
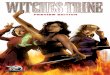
Example of coding process
Better Balance Coaching, Trine Wulff, 2009
Coach. Regarding becoming more mobile, and getting more energy and so on. How do you think this has been going?
Gudrun. Well, I think it is still progressing. Now, I get a lot of Vitamins and so on.
Coach. RightGudrun. I don’t want to weigh much more. Coach. No. So it is not just any*…. You do not want to become
BIG, if you can say it that way. Are you satisfied with your present weight?
Gudrun. Yes. Very, very satisfied. Because, I also have this osteoarthritis in my feet.
Coach. Yes.Gudrun. And I am feeling very good around not weighing too much.
Coach. Yes. So there is a balance for you, a limit for how much
weight you shall gain?Gudrun. Yes I think so..
* Hospital recently recommended her to put on some extra kilo’s
(Source: Gudrun, completion session, paragraphs 196-221 in analysis memo)
Gudrun’s understanding of her goal achievement
In progress, correlates with activities
Relates energy and gained
weight. Has now reached personal target
Considers potential side-effects if continuing
Dislikes feeling overweight
Emerging theme titles
Health-related activities
Satisfied with achievement
Considers implications before following hospital’s advice
Guided by personal health understanding

Better Balance Coaching Research: Design and methodologiesHandout, action research course participants, May 2009. Trine Wulff, Bispebjerg Hospital, Denmark
1. Project Vision: Promoting the engagement of older people in activities to prevent falls
4. Intervention phase. Coach/researcher made dense coach notes while executing study. Supervision system: Clinical supervisor and coach supervisor (ad hoc). Presentation of study for audiences, including reflective Q/A sessions. Coachee learning was challenged and verbalised in completion sessions
2. Development of intervention: Cyclic approach. Theories (fall prevention, geront., coaching, pos psych, health psych, etc), Coaching skills (CPCC educ incl. supervision, PLUS complement. methods), Interaction with target group (coachings, interviews, training partic. etc), Interaction with experts (clinicians, coaches, psychologists, health researchers), Development of coaching manual, templates and coachee handbook
8. Quantitative empirical material. 34 + 40 participants included. Participant testing and interviewing at baseline and 9 months. Self-reported no. of falls (1y), Data from primary care and hospitals, 9 months
7. Qualitative analyses (current plan, may be adjusted)
Analysis 1: Interpretative Phenomenological Analysis (Smith, Jarman, Osborn) added ”Working with mysteries and breakdown”(Alvesson, Kärreman). What incidences make elderly people being coached after fall accidents change health beliefs and/or health behaviours? Why do some elderly people being coached after fall accidents NOT change health beliefs and/or health behaviours? How do healthcare professionals impact health beliefs and health behaviours of elderly people being coached after fall accidents? Any mysteries, that can not be explained with current theories? (New theory to be generated…)
Analysis 2: How can coaching reduce fear of falling?
Analysis 3: How do elderly people being coached after fall accidents explain/justify their executed health behaviours?
9. Quantitative analysis. Number of fall incidents, hospital admissions and selected primary care services (emergency calls, delivered food, home services etc). Baseline: MMSE, social and drinking patterns, etc. Functional parameters relevant for fall prevention. Psychosocial parameters, QoL, Fear of falling, etc. Due to Type II error, no significant differences are expected
5. Qualitative focus. Qualitative interest intensified during intervention phase. Collecting qualitative material and acquiring qualitative analytical skills. Pilot analyses incl. feedback (discourse and hermeneutic approaches). Qualitative researchers suggesting different methods of analyses
6. Qualitative empirical material. 356 coaching sessions, 205 hours in totalDense coach notes from all sessions, plus additional notes/commentsTaping of approximately 75 sessions
3. Development of RCT study design. Max 6 months, max 10 hr’s, max 15 sessions: Home (2) and phone (13). Dimensioning: 2x60 part’s adequate based on hypothesis. Target: 2x90! 65+ y with fall history enrolled from hospital and training centres in Cph. Intervention: BB Coaching and usual care. Control: Usual care. Physiotherapists included and tested participants in a blinded manner
10. Project context. The coaching study is part of the project: “Better Balance – fall prevention among elderly people”, supported by the Danish Ministry of Health and Prevention. The project also includes a randomised, controlled trial of an integrated nurse approach as well as an analysis of the situation for elderly people who go to a hospital’s emergency department due to fall accidents. Contact person: Trine Wulff, Department of integrated health care, Bispebjerg University Hospital, email [email protected]

23
Quantitative analysis
Better Balance Coaching, Trine Wulff, 2009
Quantitative empirical material• 34 + 40 participants included• Participant testing and interviewing at baseline and 9 months• Self-reported no. of falls (1 year)• Data from primary care and hospitals, 9 months
Quantitative analysis• Number of fall incidents• hospital admissions and selected primary care services (emergency
calls, delivered food, home services etc)• Baseline: MMSE, social and drinking patterns, etc. • Functional parameters relevant for fall prevention. • Psychosocial parameters, QoL, Fear of falling, etc. • Due to Type II error, no significant differences are expected

24
Perspectives
Better Balance Coaching, Trine Wulff, 2009
• Communication of findings to relevant health professionals (articles etc):
How do we promote the engagement of older people in activities to prevent falls? (or… in self-concordant health-related activities)
• What works – and why and for which sub-groups? • What does not work and why?
• Educational model teaching the principles, and targeting relevant health professionals: Hospitals and primary care ?? (not included in project)

Better Balance Coaching Research: Design and methodologiesHandout, action research course participants, May 2009. Trine Wulff, Bispebjerg Hospital, Denmark
1. Project Vision: Promoting the engagement of older people in activities to prevent falls
4. Intervention phase. Coach/researcher made dense coach notes while executing study. Supervision system: Clinical supervisor and coach supervisor (ad hoc). Presentation of study for audiences, including reflective Q/A sessions. Coachee learning was challenged and verbalised in completion sessions
2. Development of intervention: Cyclic approach. Theories (fall prevention, geront., coaching, pos psych, health psych, etc), Coaching skills (CPCC educ incl. supervision, PLUS complement. methods), Interaction with target group (coachings, interviews, training partic. etc), Interaction with experts (clinicians, coaches, psychologists, health researchers), Development of coaching manual, templates and coachee handbook
8. Quantitative empirical material. 34 + 40 participants included. Participant testing and interviewing at baseline and 9 months. Self-reported no. of falls (1y), Data from primary care and hospitals, 9 months
7. Qualitative analyses (current plan, may be adjusted)
Analysis 1: Interpretative Phenomenological Analysis (Smith, Jarman, Osborn) added ”Working with mysteries and breakdown”(Alvesson, Kärreman). What incidences make elderly people being coached after fall accidents change health beliefs and/or health behaviours? Why do some elderly people being coached after fall accidents NOT change health beliefs and/or health behaviours? How do healthcare professionals impact health beliefs and health behaviours of elderly people being coached after fall accidents? Any mysteries, that can not be explained with current theories? (New theory to be generated…)
Analysis 2: How can coaching reduce fear of falling?
Analysis 3: How do elderly people being coached after fall accidents explain/justify their executed health behaviours?
9. Quantitative analysis. Number of fall incidents, hospital admissions and selected primary care services (emergency calls, delivered food, home services etc). Baseline: MMSE, social and drinking patterns, etc. Functional parameters relevant for fall prevention. Psychosocial parameters, QoL, Fear of falling, etc. Due to Type II error, no significant differences are expected
5. Qualitative focus. Qualitative interest intensified during intervention phase. Collecting qualitative material and acquiring qualitative analytical skills. Pilot analyses incl. feedback (discourse and hermeneutic approaches). Qualitative researchers suggesting different methods of analyses
6. Qualitative empirical material. 356 coaching sessions, 205 hours in totalDense coach notes from all sessions, plus additional notes/commentsTaping of approximately 75 sessions
3. Development of RCT study design. Max 6 months, max 10 hr’s, max 15 sessions: Home (2) and phone (13). Dimensioning: 2x60 part’s adequate based on hypothesis. Target: 2x90! 65+ y with fall history enrolled from hospital and training centres in Cph. Intervention: BB Coaching and usual care. Control: Usual care. Physiotherapists included and tested participants in a blinded manner
10. Project context. The coaching study is part of the project: “Better Balance – fall prevention among elderly people”, supported by the Danish Ministry of Health and Prevention. The project also includes a randomised, controlled trial of an integrated nurse approach as well as an analysis of the situation for elderly people who go to a hospital’s emergency department due to fall accidents. Contact person: Trine Wulff, Department of integrated health care, Bispebjerg University Hospital, email [email protected]

26
Discussion
Better Balance Coaching, Trine Wulff, 2009

27
Action research relevance
Better Balance Coaching, Trine Wulff, 2009
• Action research-like programme development
• Action research and coaching similarities
• Action research relevance in analysis phase
• TW’s dual roles: Programme inventor, coach and evaluator

28
Handout, delivered to participants
Better Balance Coaching, Trine Wulff, 2009

Better Balance Coaching Research: Design and methodologiesHandout, action research course participants, May 2009. Trine Wulff, Bispebjerg Hospital, Denmark
1. Project Vision: Promoting the engagement of older people in activities to prevent falls
4. Intervention phase. Coach/researcher made dense coach notes while executing study. Supervision system: Clinical supervisor and coach supervisor (ad hoc). Presentation of study for audiences, including reflective Q/A sessions. Coachee learning was challenged and verbalised in completion sessions
2. Development of intervention: Cyclic approach. Theories (fall prevention, geront., coaching, pos psych, health psych, etc), Coaching skills (CPCC educ incl. supervision, PLUS complement. methods), Interaction with target group (coachings, interviews, training partic. etc), Interaction with experts (clinicians, coaches, psychologists, health researchers), Development of coaching manual, templates and coachee handbook
8. Quantitative empirical material. 34 + 40 participants included. Participant testing and interviewing at baseline and 9 months. Self-reported no. of falls (1y), Data from primary care and hospitals, 9 months
7. Qualitative analyses (current plan, may be adjusted)
Analysis 1: Interpretative Phenomenological Analysis (Smith, Jarman, Osborn) added ”Working with mysteries and breakdown”(Alvesson, Kärreman). What incidences make elderly people being coached after fall accidents change health beliefs and/or health behaviours? Why do some elderly people being coached after fall accidents NOT change health beliefs and/or health behaviours? How do healthcare professionals impact health beliefs and health behaviours of elderly people being coached after fall accidents? Any mysteries, that can not be explained with current theories? (New theory to be generated…)
Analysis 2: How can coaching reduce fear of falling?
Analysis 3: How do elderly people being coached after fall accidents explain/justify their executed health behaviours?
9. Quantitative analysis. Number of fall incidents, hospital admissions and selected primary care services (emergency calls, delivered food, home services etc). Baseline: MMSE, social and drinking patterns, etc. Functional parameters relevant for fall prevention. Psychosocial parameters, QoL, Fear of falling, etc. Due to Type II error, no significant differences are expected
5. Qualitative focus. Qualitative interest intensified during intervention phase. Collecting qualitative material and acquiring qualitative analytical skills. Pilot analyses incl. feedback (discourse and hermeneutic approaches). Qualitative researchers suggesting different methods of analyses
6. Qualitative empirical material. 356 coaching sessions, 205 hours in totalDense coach notes from all sessions, plus additional notes/commentsTaping of approximately 75 sessions
3. Development of RCT study design. Max 6 months, max 10 hr’s, max 15 sessions: Home (2) and phone (13). Dimensioning: 2x60 part’s adequate based on hypothesis. Target: 2x90! 65+ y with fall history enrolled from hospital and training centres in Cph. Intervention: BB Coaching and usual care. Control: Usual care. Physiotherapists included and tested participants in a blinded manner
10. Project context. The coaching study is part of the project: “Better Balance – fall prevention among elderly people”, supported by the Danish Ministry of Health and Prevention. The project also includes a randomised, controlled trial of an integrated nurse approach as well as an analysis of the situation for elderly people who go to a hospital’s emergency department due to fall accidents. Contact person: Trine Wulff, Department of integrated health care, Bispebjerg University Hospital, email [email protected]