Embed Size (px)
Citation preview

11
Best Practices in the Best Practices in the Prevention of Prevention of
Restraint/Seclusion (R/S)Restraint/Seclusion (R/S)
NYS OMH Forum: Preventing the Need for R/S NYS OMH Forum: Preventing the Need for R/S with Young and/or Mixed Age Children with Young and/or Mixed Age Children
October 6, 2009 Buffalo, New YorkOctober 6, 2009 Buffalo, New York
Beth Caldwell, Office of Technical Assistance Beth Caldwell, Office of Technical Assistance

22
Acknowledgements Acknowledgements • Substance Abuse and Mental Health
Services Administration (SAMHSA)• National Association of State Mental
Health Program Directors (NASMHPD) /Office of Technical Assistance (OTA)
• Kevin Ann Huckshorn (Commissioner of Delaware)
• Janice LeBel (MA DMH)• Staff and youth/families in successful
programs and family & youth advocates across the country

33
Brief Historical Overview Brief Historical Overview National S/R Reduction Initiative National S/R Reduction Initiative
• 1998: Hartford Courant Series • 1999: GAO Report (Congress) -
- NASMHPD MD S/R Report (Treatment Failure)
- CMS Rule changes (2001/06)• 2002/03: NASMHPD Training Curriculum created/
Training begins• 2003: New Freedom Commission Report
(Transformation)/ Independent projects support core strategies
• 2004 – 2007/2007 – 2010: SAMHSA funded 8-State Evaluations (total 16 States)

44
Framing the IssueFraming the Issue• The reduction of seclusion, restraint and coercive
practices requires a CULTURE CHANGE in our mental health treatment settings that results in far more than just reducing S/R (Huckshorn, 2006)
• This ‘Culture Change’ must be congruent with recovery and resiliency (transformation principles)
• Best practice core strategies have been identified
• However, practice and system change is slow and difficult… for many reasons…

55
Main Change Constructs (core beliefs that Main Change Constructs (core beliefs that provide a foundation) in Preventing Conflict, provide a foundation) in Preventing Conflict,
Violence and S/R useViolence and S/R use
• Leadership Principles for effective change• The Public Health Prevention approach• Use of Recovery/Resiliency Principles• Valuing Consumer/Families/Staff• Trauma Knowledge operationalized• Staying true to CQI Principles (the ability of staff
to be honest and take risks to assure that we learn from our mistakes)

J. LeBel
MA Pediatric Unit: Post-Visit S/R Use (JL)
0
20
40
60
80
100
120
Ju
l-00
Oct-00
Jan
-01
Ap
r-01
Ju
l-01
Oct-01
Jan
-02
Ap
r-02
Ju
l-02
NYNY
VisitVisit
MA Adolescent Unit: Post-Visit S/R UseMA Adolescent Unit: Post-Visit S/R Use (07/00-08/02)(07/00-08/02)
0
100
200
300
400
500
600
Ju
l-0
0
Oct-00
Jan
-01
Ap
r-0
1
Ju
l-0
1
Oct-01
Jan
-02
Ap
r-0
2
Ju
l-0
2
NYNY VisitVisit

7
Public Health Prevention Model
Tertiary
Primary
Seco
ndar
y

88
The Six Core StrategiesThe Six Core Strategies© to © to Prevent Violence and S/RPrevent Violence and S/R
(meet criteria to apply to be EBP)(meet criteria to apply to be EBP)
1) Leadership Toward Organizational Change
2) Use Data To Inform Practices
3) Develop Your Workforce
4) Implement S/R Prevention Tools
5) Actively recruit and include service users and families in all activities
6) Make Debriefing rigorous

99
SAMHSA SIG Six Core Strategy © Analysis/Statistical Strategy
Table 3: Number and percent of facilities by implementation phase at the end of the grant period (n=43). a.
Implementation Phase
b.
# of
Facilities
c.
% of
Facilities 1. Never Implemented 2 4.7% 2. Implementing, Did not Stabilize 7 16.3% 3. Stable Implementation 28 65.1% 4. Implementation followed by a
Decreased 5 11.6%
5. Implementation followed by Discontinuation
1 2.3
Preliminary Results

1010
Most Successful Child/Adolescent Most Successful Child/Adolescent State MH Initiative in the USAState MH Initiative in the USA
MA: 2001 – 2009 33 hospital & RTF type programs
• Mechanical Restraint: <91% (2010 to eliminate)
• Hours Decreased: <60%• Medication Restraint: < 80%• Staff Injuries: < 61.53%

1111
Next Steps for MA: CW/JJ/ED Next Steps for MA: CW/JJ/ED Residential Programs Residential Programs (JL)(JL)
In 2008:
• 65,000 episodes of restraint
• More than 2,300 injuries to youth
• Approximately 1,900 injuries to staff
December/2009 Kick-off

1212
Most Potent MA Most Potent MA ProviderProvider Actions Actions (JL)(JL)
PreparationPreparation
• Hired or identified passionate, leaders with caregiving experience & perspective
• Built a strong team of co-leaders/champions
• Organized around a model of care: explained why & how
• Prepared to re-examine everything
• Understood it was a process, not simply a task and implemented in a step-wise fashion

1313
Most Potent MA Provider Actions Most Potent MA Provider Actions (JL)(JL)
ImplementationImplementation
• Increased supervision and mentoring (i.e. hands-on presence by leadership)
• Hired to the vision and expectation
• Changed their orientation/training/policies & procedures
• Helped staff who did not agree with new culture to find their “gifts & graces”“gifts & graces”
• Never wavered from vision: patient & tenacious

1414
Specific MA Provider ExamplesSpecific MA Provider Examples
• Boston University IRTP (adolescent)
• Cambridge Child Assessment Unit

15
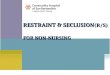
Boston Medical Center Intensive Residential Treatment Program
Total Seclusion, Restraint & Injury Episodes09/00 - 05/07
0
10
20
30
40
50
60
70
80
Se
p-0
0
Ja
n-0
1
Ma
y-0
1
Se
p-0
1
Ja
n-0
2
Ma
y-0
2
Se
p-0
2
Ja
n-0
3
Ma
y-0
3
Se
p-0
3
Ja
n-0
4
Ma
y-0
4
Se
p-0
4
Ja
n-0
5
Ma
y-0
5
Se
p-0
5
Ja
n-0
6
Ma
y-0
6
Se
p-0
6
Ja
n-0
7
Ma
y-0
7
Significant Periods
SR
& I
nju
ry E
pis
od
es
SR Episodes
Kid Injury
Staff Injury
St

1616
How did BU do it? How did BU do it? (JL)(JL)
• Hired senior experienced leaders who were parents (very hands on – 1 of top 3 leaders always on the floor)
• Implemented Glenn Saxe’s Trauma Systems Treatment
• ““We started talking a lot!”We started talking a lot!” Many more staff meetings to organize around shared vision and values. “After “After that – we all knew what we were doing and why.”that – we all knew what we were doing and why.”
• Built a team & empowered staffempowered staff to create change:– Hired to new vision, expected & managed turnover– Shift focus to “pre-escalation”– No more nurses station – “Lost” mechanical restraints– Moved away from point – level system

1717
How did BU do it? How did BU do it? (JL)(JL)
• New mechanisms to create culture change:
– Pre-admit expectation re: safety plan
– Family partnership & program as familyprogram as family: it’s all about relationships, creating expectations & nurture, nurture, nurturenurture, nurture, nurture
– Crisis plan program plan tx plan
– New medical record: pulls for daily tracking of triggers & strategies
• ““S/R is just not an option.” “Staff now believe … I S/R is just not an option.” “Staff now believe … I can leave and this will continue.”can leave and this will continue.”

18
0
10
20
30
40
50
60
70
80
90
100
Jan-01 Jul-01 Jan-02 Jul-02 Jan-03 Jul-03 Jan-04 Jul-04 Jan-05 Jul-05 Jan-06 Jul-06 Jan-07 Jul-07
Significant Periods
# E
pis
od
es p
er 1
000
Pat
ien
t D
ays
Cambridge Hospital
Unit Type Average
Cambridge CAU
SR Episodes per 1000 patient days

1919
How did Cambridge do it? How did Cambridge do it? (JL)(JL)
• Adopted Ross Greene’s Collab. Problem-Solving model – Changed orientation from pathology to skill deficit: skill deficit:
“Kids do well, if they can”“Kids do well, if they can”• Created a strong, like-minded driven team• Significant increase in training & supervision • Every policy/procedure/practice was up for grabs, no
sacred cows• Invited families in: no visiting hours, spend the night, join
us!• Encouraged staff creativity & empowerment

2020
How did Cambridge do it? How did Cambridge do it? (JL)(JL)
ABC’s:• Arts & crafts• Backrubs• Cooking activities• Distraction• Empathy• Finding out what they like
and doing it with them• Giving kids space when the
need it
SPACE techniques:• Saving face (kids need
dignity respected)• Paying attention to their
ideas & solutions• Allowing children space to
calm/regroup on their timetable
• Collaboration rather than uni-lateral decision making
• Encouraging master by providing choices

2121
Words of Wisdom
from MA Child or Mixed Age Serving
Program Leaders

2222
Bev Presson, Metro West Medical Bev Presson, Metro West Medical Center; Child Development UnitCenter; Child Development Unit
• Get rid of naysayers! Invite staff not on board to leave. They have talents to be used else where. Have authentic responses with staff to get engagement out in the open. Are you on board?
• Saying sorry works. It assists the child to be released from shame and move toward exploring their own behavior
• Shame runs deep at an early age. Tone is important. Get rid of harsh tomes and laugh more. Allow children to know that your unit is one where they can make mistakes and practice new skills.
• It isn’t rocket science it’s about kindness. Keep it simple. • It gets down to listening to the child’s story. There is truth. • Becoming mindful of our own response and regulating
response to aggression.

2323
Ralph Buonopone, McLean-Ralph Buonopone, McLean-Franciscan C/A Inpatient (mixed)Franciscan C/A Inpatient (mixed)
• Staff take turns & trust each other• Don’t use rewards/consequences when relationships
will work better• Allow mistakes – don’t treat every mistake as a major
infraction• Start with empathy• Instill hope and optimism• Slow down – ritual and routine are more effective than
limits and consequences• Increase structure and increase choices (yoga, Tai
Chi, meditation, music, relaxation, bowling, origami, medicine balls, stationary bikes, etc., etc.)

2424
Children’s Hospital – Bader 5Children’s Hospital – Bader 5• Complementary Treatments:
– Massage (allows teaching about reducing stress)– Reiki (part of treatment plan – esp. severe
anxiety/panic disorder & eating disorders)– Sensory (activities, materials, room)– Deep relaxation techniques– Therapeutic Dogs
• Physical Activities (running group, baseball, kickball, walking, stationary bicycle, yoga, etc.)
• Lots of recreation and art• Relaxed approach (hold hands when walking, tuck-
in bed time rituals – including back rubs)

2525
MA Top Tips from Providers MA Top Tips from Providers (JL)(JL)
• Encourage flexible “out of the box” thinking. It is not not win or lose… win or lose… but how can we help?but how can we help?
• Have frequent forums for staff to openly express feelings so they don’t act these out on youth
• Instill hope and optimism no matter whatno matter what
• If a youth doesn’t succeed 80% of time, break expectations into smaller steps until they have achieved goals
• When you take away a tool, you have to put another one in its place

2626
MA Top Tips from Providers MA Top Tips from Providers (JL)(JL)
• Praise staff & youth for good work and celebrate often!
• Keep goals brief, focused & involve youth & families
• Make it fun and use humor
• Use complementary therapies – massage, Reiki, yoga, relaxation, visualization, positive affirmations, spiritual needs
• Reframe behavioral descriptions to be more strength-based
– “Wandering” halls is now “grazing for sensory input”“grazing for sensory input”
– “Needy” is now “understandably in need of staff “understandably in need of staff attention”attention”
• Show them “the data!”Show them “the data!”

27
MA Top Tips: Sensory/Sensory

2828
MA Top Tips: > Physical Activity/Play MA Top Tips: > Physical Activity/Play (JL)(JL)
• Trauma impacts capacity for joy (Panksepp, 1993 & 1998)
• Activating Play-Joy SystemPlay-Joy System promotes socialization, brain development & maturation of frontal cortical executive processes (Panksepp, 2004)
• Positive behavioral states take practice (Wolff, 1987)
• Decrease in left-hemisphere activation (verbal skills) suggests trauma survivors need another way to communicate their experiences, such as right-right-hemisphere “body-oriented therapies” hemisphere “body-oriented therapies”
(van der Kolk, 2004)

2929
““Traumatized individuals need toTraumatized individuals need tohave experiences that directlyhave experiences that directly
contradict the emotionalcontradict the emotional helplessness and physicalhelplessness and physicalparalysis that accompanyparalysis that accompanytraumatic experiences.”traumatic experiences.”
Bessel Van der Kolk, 2004Bessel Van der Kolk, 2004

30
MA Top Tips: AnimalsGoing to the Dogs (JL)
““These dogs are worth These dogs are worth
their weight in gold … their weight in gold …
they work faster than any they work faster than any
therapist or drug I’ve seen.”therapist or drug I’ve seen.”(Benedetti, 2006)
• NEADS dogs• Prison-Puppy Program graduates
– Bruin & Bogie

3131
MA Top Tips: What’s the Point? MA Top Tips: What’s the Point? (JL)(JL)
• Coercive tool to teach compliance
• Lack of evidence base to support use(Mohr & Pumariega, 2004)
• Critically re-examining point & level systems statewide
• Consultation & revision underway
• Moving to natural & logical consequences & making amends

3232
Priority Training for Staff to Priority Training for Staff to Prevent R/S & Promote Prevent R/S & Promote
Youth-guided Care: Moving Youth-guided Care: Moving from Control to Collaboration from Control to Collaboration
(> choice for all ages)(> choice for all ages)
NYC Youth Advocate NYC Youth Advocate RecommendationsRecommendations

3333

3434
Other Youth Recommendations Other Youth Recommendations JLJL
• Use of sensory strategies • Peer leadership/support• Youth ‘really’ involved in own treatment• Home like environments• More individual time with staff• Staff: strong communication & listening skills (e.g.,
body language, tone - not threatening, disrespectful, unfair or judgmental
• Lots of activities (e.g., sports, art, music).• Appropriate physical contact• Eliminate the use of point and level systems

3535
Researched Best Practices in Researched Best Practices in Achieving Positive Outcomes Achieving Positive Outcomes
with Children/Adolescentswith Children/Adolescents• Family-driven Care (i.e. CFT/Wraparound)• Youth-guided Care (i.e. > youth voice/choice)• Practices based on System of Care Values
(strength-based, individualized, C & LC, flexible)
• Responsiveness to Developmental Age• Trauma Informed Care • Emerging Science of Sensory Modulation• Specific EBP’s (e.g., MST, CBT’s - DBT)

3636
Do/Are Your Children Ever?Do/Are Your Children Ever?
• Appear guarded and anxious
• Difficult to re-direct, reject support
• Highly emotionally reactive
• Have difficulty “settling” after outbursts
• Hold onto grievances
• Not take responsibility for behavior
• Make the same mistakes over and over • (Hodas, 2004: Trauma)

3737
Understand Normal Understand Normal Developmental Stages Developmental Stages
& Each Child’s & Each Child’s Developmental HistoryDevelopmental History
(Fosterparentscope Curriculum, 1993)

3838
Common Emotional, Social and Common Emotional, Social and Cognitive Consequences Cognitive Consequences
of Abuse and Neglectof Abuse and Neglect• May display thinking patterns that are typical of a
younger child, including egocentric perspectives, lack of problem-solving ability, and inability to organize and structure thoughts.
• May be unable to concentrate on school work, and may not be able to conform to the structure of a school setting. The child may not have developed basic problem-solving and may have considerable difficulty in academics.
• May be suspicious and mistrustful of adults or overly solicitous, agreeable, and manipulative, and may not turn to adults for comfort and help when in need.
(Fosterparentscope Curriculum, 1993)

3939
Common Emotional, Social and Common Emotional, Social and Cognitive Consequences Cognitive Consequences
of Abuse and Neglectof Abuse and Neglect• May not respond to positive praise and attention or
may excessively seek adult approval and attention. • May feel inferior, incapable, and unworthy around
other children; may have difficulty making friends, feel overwhelmed by peer expectations for performance, may withdraw from social contact, and may be scapegoated by peers.
• May experience damage to self-esteem from denigrating or punitive messages from an abusive parent or lack of positive attention in a neglectful environment.
• May behave impulsively, have frequent emotional outbursts, and be unable to delay gratification.
(Fosterparentscope Curriculum, 1993)

4040
Recommendations: Recommendations: Successful Administrators from 4 Successful Administrators from 4
Child or Mixed-age Programs Child or Mixed-age Programs • Leadership• Data to Inform Practice• Workforce Development• Primary Prevention
Tools• Family-driven/Youth-
guided Care• Debriefing• Other: Individualize!!!!!!
• 5 +++ (all levels)• 5 (in beginning)• 5 ++• 4/5
• 4/5
• 5 +++
• 5+++

4141
EXTREME PERSISTENCEEXTREME PERSISTENCE
Resiliency-based mental health service providers:• “recognize that needs can be complex, that
change is sometimes very difficult to achieve”;• Promotes “extreme persistence” and creative
adaptations in delivery of services,• “changing the plan (our approach) instead of
rejecting (blaming) the youth” or familyJohn VanDenBerg, 2002

4242
Most Frequently Identified Most Frequently Identified ChallengesChallenges
• Culture Change/Philosophy Shift– Kick-off– Value-driven persistent leadership– Training/training/training – Supervision/mentoring– Unit-based meetings regularly – Staff empowered/valued – part of all workgroups
• Sustaining Initiative– Celebrate success– All staff meetings– Newsletter/story boards– Empower staff to keep learning and implementing new ideas– Video of staff and consumers sharing why they like the new culture of
prevention/support versus the old culture of control/restraint

4343
““You never change things You never change things by fighting existing reality. by fighting existing reality.
To change something, To change something, build a new model build a new model
that makes the that makes the old model obsolete.”old model obsolete.”
- Buckminster Fuller- Buckminster Fuller

4444
First step in prevention? First step in prevention? Develop a Plan!Develop a Plan!
• TO START: Facility leaders must develop a S/R Prevention/Reduction Action Plan
Action Plan FrameworkPrevention-Based ApproachContinuous Quality Improvement PrinciplesIndividualized for the Facility or Agency (based on
population – i.e. developmental age)Adopt/adapt Six Core Strategies ©

4545
The Six Core StrategiesThe Six Core Strategies© to Prevent © to Prevent Violence and S/RViolence and S/R
1) Leadership Toward Organizational Change
2) Use Data To Inform Practices
3) Develop Your Workforce
4) Implement S/R Prevention Tools
5) Actively recruit and include service users and families in all activities
6) Make Debriefing rigorous

4646
And for those skeptics out there…

4747
Training CommentsTraining Comments

4848
Contact InformationContact Information
Beth Caldwell
413-644-9319
Janice LeBelJanice LeBel617-626-8085