Embed Size (px)
Citation preview

1
Author: Klemp, Melissa, L Title: B Vitamin Supplementation in Treating Depression The accompanying research report is submitted to the University of Wisconsin-Stout, Graduate School in partial
completion of the requirements for the
Graduate Degree/ Major: MS Food and Nutritional Sciences
Research Advisor: Suejung Han, Ph.D.
Submission Term/Year: Spring, 2013
Number of Pages: 70
Style Manual Used: American Psychological Association, 6th edition
I understand that this research report must be officially approved by the Graduate School and that an electronic copy of the approved version will be made available through the University Library website
I attest that the research report is my original work (that any copyrightable materials have been used with the permission of the original authors), and as such, it is automatically protected by the laws, rules, and regulations of the U.S. Copyright Office.
My research advisor has approved the content and quality of this paper. STUDENT:
NAME Melissa Klemp DATE: 5-12-13
ADVISOR: (Committee Chair if MS Plan A or EdS Thesis or Field Project/Problem):
NAME Suejung Han DATE: 5-12-13
----------------------------------------------------------------------------------------------------------------------------- ----
This section for MS Plan A Thesis or EdS Thesis/Field Project papers only Committee members (other than your advisor who is listed in the section above) 1. CMTE MEMBER’S NAME: Carol Seaborn DATE: 5-10-13
2. CMTE MEMBER’S NAME: Patricia Knisley DATE: 5-10-13
----------------------------------------------------------------------------------------------------------------------------- ---- This section to be completed by the Graduate School This final research report has been approved by the Graduate School.
Director, Office of Graduate Studies: DATE:

2
Klemp, Melissa, L. B Vitamin Supplementation in Treating Depression
Abstract
Depression is a serious illness, negatively affecting quality of life mentally, physically, and
monetarily of many adults in the United States. Antidepressant medications are commonly
prescribed to treat symptoms of depression, but patient adherence rates to antidepressant
medications are often low due to negative side-effects, inefficacy, cost, and negative perceptions
regarding their use. Alternative and adjunct treatment therapies include vitamin supplement use.
B vitamins are considered in depression treatments because of positive impacts on certain
mechanisms in the body, including neurotransmitter and mood hormone pathways. This study
examined the effect of B vitamin supplementation on depressive symptoms. The study sample
consisted of 33 medicated and unmedicated adults living in the Menomonie, Wisconsin area.
Participants took a B vitamin supplement daily for 28 days. Presence of depressive symptoms
was assessed using the Center for Epidemiological Studies Depression Scale. Dietary
assessment of B vitamin intake was made by two, 24-hour food recalls. Results showed there
was a significant decrease in depressive symptoms from baseline (M = 31.4, SD = 9.6) and at
post-intervention (M = 18.9, SD = 10.4), t(32) = 7.08, p < .001. Depressive symptoms decreased
in participants regardless of medication status and dietary intake of B vitamins.

3
Table of Contents
.................................................................................................................................................... Page
Abstract ............................................................................................................................................2
List of Tables ...................................................................................................................................6
Chapter I: Introduction ....................................................................................................................7
Statement of the Problem .....................................................................................................9
Purpose of the Study ..........................................................................................................10
Assumptions of the Study ..................................................................................................10
Definition of Terms............................................................................................................10
Limitations of the Study.....................................................................................................12
Methodology ......................................................................................................................13
Chapter II: Literature Review ........................................................................................................14
Change Theory ...................................................................................................................14
Depression and Antidepressants ........................................................................................15
Depression and Supplements .............................................................................................16
B Vitamins .........................................................................................................................17
Thiamin (B1) ..........................................................................................................18
Riboflavin (B2) ......................................................................................................19
Niacin (B3).............................................................................................................20
Vitamin B5 (Pantothenic Acid) .............................................................................20
Vitamin B6 (Pyridoxine)........................................................................................20
Biotin (B7) .............................................................................................................22
Folate (B9) .............................................................................................................23

4
Vitamin B12 (Cobalamin)......................................................................................25
Present Study .....................................................................................................................26
Chapter III: Methodology ..............................................................................................................28
Subject Selection and Description .....................................................................................28
Instrumentation ..................................................................................................................28
Data Collection Procedures ................................................................................................30
Data Analysis .....................................................................................................................30
Limitations .........................................................................................................................31
Chapter IV: Results ........................................................................................................................32
Description of the Participants ..........................................................................................32
First Objective ...................................................................................................................33
Figure 1: Change in the participants CES-D depression score average from
baseline to post-intervention ..............................................................................................34
Second and Third Objectives and Gender ........................................................................34
Possible Side Effects .........................................................................................................36
Chapter V: Discussion ...................................................................................................................38
Discussion .........................................................................................................................38
Conclusions ........................................................................................................................43
Recommendations ..............................................................................................................43
References ......................................................................................................................................45
Appendix A: UW-Stout IRB Approval Letter ..............................................................................56
Appendix B: B Vitamin Study Participant Qualification Letter ....................................................57
Appendix C: Consent Form ...........................................................................................................58

5
Appendix D: Baseline Questionnaire.............................................................................................60
Appendix E: Post-Intervention Questionnaire ...............................................................................64
Appendix F: 24-Hour Food Recall Form .......................................................................................68
Appendix G: B Vitamin Supplement Used in Study .....................................................................69
Appendix H: Participant Study Instructions ..................................................................................70

6
List of Tables Table 1: Participant Body Mass Index (BMI)………..…………………………………32
Table 2: Participant Alcohol Intake Frequency…………..……………………………..33
Table 3: Participant Adequacy of Dietary Intake of B Vitamins.…………………….…35

7
Chapter I: Introduction
According to the Centers for Disease Control and Prevention (2011), depression affects
one in every ten adults in the United States, with an associated $150 billion in direct and indirect
medical and employment costs. Depression affects quality of life not only mentally, but
physically as well by negatively impacting numerous other ailments such as arthritis, obesity,
and diabetes (Centers for Disease Control and Prevention, 2011). Ten billion dollars’ worth of
antidepressants were prescribed in 2010 (Insel, 2011), but patient adherence to antidepressant
treatment using medications is often as low as 25% (Kikuchi, Uchida, Suzuki, Watanabe, &
Kashima, 2011). The negative side effects caused by antidepressant use are a major contributing
factor to the low adherence rates, and nearly 74% of respondents of a large internet survey
reported experiencing side effects (Kikuchi et al., 2011). Patient attitude towards antidepressants
is another contributing factor to adherence rates, and a negative attitude toward antidepressants
has been associated with more missed days of taking a prescribed antidepressant medication
(Chakraborty, Avasthi, Kumar, & Grover, 2009).
Over 50% of the United States (U.S.) adult population uses dietary supplements (Gahche
et al., 2011), and supplement use among people being treated for depression is very common
(Silvers, Woolley, & Hedderley, 2006). One in three older adults that have been diagnosed with
depression or bipolar disorder takes an herbal or nutritional compound (Keaton et al., 2009).
Studies on the effects of various supplements on symptoms of depression have revealed
conflicting results, and there is limited research on most supplements (Nguyen et al., 2009).
There is a specific lack of research on B vitamins and their effect on symptoms of depression,
although deficiencies of various B vitamins have been associated with psychiatric disorders,
including depression (Hvas, Svend, Bech, & Nexø, 2004; Sachdev et al., 2005). Most studies
focus on blood serum correlations of some of the B vitamins and depression, and a few of those

8
studies included B vitamin supplementation, but sufficient randomized double-blind placebo
controlled trials are lacking (Bender, 1984; Nguyen et al., 2009).
The use of dietary supplements to treat depression needs to be studied for efficacy as an
alternative or as an enhancement therapy to current antidepressant drug therapies. Since people
experience negative side effects from antidepressant drugs and have negative perceptions
regarding their use, the use of supplements in place of or in conjunction with antidepressants
could reduce patient experience of the negative antidepressant side effects, and could increase
overall treatment compliance. Attitudes towards supplement use appear to be favorable, since a
study by Silvers et al. (2006) found that 63% of their subjects with depression were taking
supplements, and 80% of their subjects who took antidepressant medications also took a
supplement, although the reasons for supplement use were not discussed. A large telephone
survey found that 73% of participants used any type of supplement, 85% took a
multivitamin/multimineral supplement, and 77% took a single ingredient or a specialized vitamin
supplement (Timbo, Ross, McCarthy, & Lin, 2006). Only four percent of participants reported
an adverse event that they associated with taking a supplement (Timbo, et al., 2006).
Studies in several countries show correlations between depression and B vitamin
deficiencies (Kim et al., 2008; Nguyen et al., 2009; Skarupski, et al., 2010; Tolmunen et al.,
2004), including studies since 2009, the year that 51 countries mandated folic acid grain
fortification laws (Berry, Bailey, Mulinare, Bower, & Dary, 2010). Low blood serum levels of
folate and low dietary intake of folate in particular show an association with depression in
studies, but there is a question as to whether this evidence applies to the United States
population, as folic acid fortification of grain foods has been mandated since 1998 (Skarupski, et
al., 2010). Research has shown that on average, red blood cell folate concentrations have

9
increased 57% in the United States population since grain fortification (Dietrich, Brown, &
Block, 2005). Despite that increase, less than 10% of women of childbearing age meet the
recommendations for red blood cell folate concentrations, and dietary intake of folate has not
increased for women over age 60 (Dietrich et al., 2005). There is enough evidence to warrant
further investigation into the positive effects B vitamin supplementation may have on symptoms
of depression, because although there is B vitamin food fortification, dietary intake of the B
vitamins may still be low in some populations (Dietrich et al., 2005; Nguyen et al., 2009).
Overall, little research or trials have been conducted in the United States addressing associations
between B vitamin deficiencies and depression, or the efficacy of B vitamin supplementation on
depression, or how B vitamins in the diet may play a role in depression.
Statement of the Problem
Several studies have concluded that further research needs to be undertaken on alternative
therapies for the treatment of depression based on positive preliminary findings (Nguyen et al.,
2009). Natural health magazine articles, internet blogs, anecdotal conversations, and other
popular media describe of the benefits of B vitamins in reducing or eliminating symptoms of
depression, yet little research exists. There are insufficient human subject trials using B vitamins
to treat symptoms of depression, which makes it difficult for health care practitioners to make
informed decisions when treating their patients using B vitamins as an alternative therapy. An
assessment of the effectiveness of B vitamin supplementation to reduce symptoms of depression
in adults could be helpful to ascertain if B vitamins should be considered as adjunct therapy for
people already taking antidepressant medications, or for people who are unable or unwilling to
take antidepressant medications.

10
Purpose of the Study
The purpose of this research is to investigate the effectiveness of B vitamin
supplementation in reducing symptoms of depression. The following research questions were
asked:
1. Does B vitamin supplementation decrease symptoms of depression?
2. Does B vitamin supplementation decrease symptoms of depression in people in who
take antidepressants yet still experience symptoms of depression?
3. Does dietary intake of B vitamins affect the efficacy of B vitamin supplementation in
reducing symptoms of depression?
Assumptions of the Study
It was assumed that the participants in the study responded accurately to the pre- and
post-depression questionnaire, and that they accurately listed the number of supplements not
consumed for the purpose of assessing compliance. It was assumed that the two 24-hour food
diaries were completed accurately by each participant, including the estimates of portion sizes. It
was also assumed that the participants understood and adhered to the study’s qualifications of
participation.
Definition of Terms
The following terms have been given operational definitions for the purpose of this study.
B vitamins. B vitamins refer to any combination of two or more of the following eight B
vitamins, unless specifically stated: B1 (thiamin), B2 (riboflavin), B3 (niacin), B5 (pantothenic
acid), B6 (pyridoxine), B7 (biotin), B9 (folic acid), and B12 (cobalamin). The B vitamin
supplement given to participants in the study included all of the above eight vitamins. In the
body, B vitamins play vital roles in various body functions and pathways, including the

11
metabolism of the neurotransmitters serotonin, dopamine, epinephrine, and norepinephrine,
which are linked to mood.
Depression. The American Psychiatric Association (2000) characterizes depression as a
depressed or sad mood, diminished interest in activities which used to be pleasurable, weight
gain or loss, physical agitation or restlessness, slowing of physical or mental activity, fatigue,
inappropriate guilt, difficulties concentrating, as well as recurrent thoughts of death. Five or
more of the above symptoms must be present for a continuous period of at least two weeks to be
assumed to have a major depressive episode. If those depressive symptoms interfere with
functioning significantly, then a major depressive disorder diagnosis is given. The subjects in
this study did not need to have received a health care practitioner’s diagnosis of depressive
disorder to participate.
Food fortification. Food fortification (or enrichment) is the addition of vitamins and/or
minerals to a food, to deliberately increase the content of those vitamins and minerals in the
food, often for the purpose of restoring the vitamins and minerals lost during processing that
were originally in the whole food. Generally, vitamins and minerals added during fortification
are not as bioavailable as those in the whole food. White flour is stripped of vitamins and
minerals, and enriched flour is white flour that has had those vitamins and minerals replaced. In
order for a label to claim “enriched flour,” it must meet the Food and Drug Administration
guidelines for a minimum amount of the B vitamins thiamin, riboflavin, niacin and folic acid.
Many companies that make processed cereals, breads, and other grain products commonly fortify
their foods with the B vitamins thiamin, riboflavin, niacin, vitamin B6, folic acid, and vitamin
B12.

12
Serotonin. Serotonin is a neurotransmitter found mainly in the central nervous system
and gastrointestinal tract that is involved in vasoconstriction and the regulation of mood, sleep,
appetite and memory.
Selective serotonin reuptake inhibitors (SSRIs). SSRIs are medications typically used
as antidepressants that act to increase the amount of available serotonin in the brain by blocking
the reabsorption of serotonin. SSRIs are used to treat depression, anxiety disorders, and some
personality disorders.
Supplements. Supplements refer specifically to dietary supplements. Dietary
supplements are vitamins, minerals, herbs, or other botanical substances taken in addition to the
usual diet in the form of pills, capsules, powders, or liquids.
Limitations of the Study
Limitations of the study included the self-reported accuracy of the participants’ two 24-
hour food diaries. The software used to analyze the diets, Food Processor, has an extensive
database, but still has limitations in available food choices. Individual participants’ ability to
absorb the various B vitamins was not measured or taken into account, which was beyond the
scope of this study. Also beyond the scope of this study was assessing biochemical B vitamin
status and markers in the participants. There are possible participant life situations or other
unknown variables that could have affected the results. The study population was a convenience
sample, recruited in the Menomonie, Wisconsin area via advertisements on the University of
Wisconsin-Stout’s campus and posters placed in the community. Finally, there was no placebo
group with which to compare the treatment group.

13
Methodology
Participants took a B vitamin supplement daily for 28 days. Their depressive symptoms
were assessed at baseline and at the end of the study using the Center for Epidemiologic Studies
Depression (CES-D) scale. Two 24-hour food diaries were taken to assess their dietary intake of
B vitamins. The data collected was analyzed using the Statistical Program for Social Sciences
(SPSS) software.

14
Chapter II: Literature Review
The purpose of this research was to investigate the effectiveness of B vitamin
supplementation in reducing symptoms of depression, so that health care practitioners and
patients have more treatment options available to them. There is a correlation between
deficiencies in some B vitamins and depression but there is a gap in studies evaluating the
effectiveness on their treatment of depression (Bender, 1984; Rao, Kumar, Raman, Sivakumar,
& Pandey, 2008; Sanchez-Villegas et al., 2009). Another reason to explore B vitamins is
because these supplements are increasingly being touted in natural health magazine articles,
internet blogs, and anecdotal conversations as having benefits that relieve symptoms of
depression, yet little research exists.
Change Theory
In 1962, Everett Rogers (2003) first described Change Theory, in which he sought an
explanation for how, when, and why change comes about. He explained that new ideas must go
through five stages of acceptance, and that an idea may be accepted or rejected during any of the
stages: awareness, interest, evaluation, trial, and adoption. People adopt new ideas at different
rates and tend to accept them the most readily if the change is uncomplicated, easily fits into
their life, and shows obvious improvement. The treatment of disease has developed over time
following much this same action. By some means, a subject is first made aware to researchers,
health practitioners, and/or the public. If an interest is expressed, current knowledge on the
subject is evaluated. If the findings are reasonable, trials with the new treatment are undertaken.
If results are favorable, the new treatment may be adopted, often by certain communities before
extending itself to the general public. Interest and knowledge on the topic of utilizing B vitamins
in the treatment of depression has been expressed, and trials have been undertaken. It is still in

15
the inconclusive stage, and this study seeks to assess the efficacy of taking a B vitamin
supplement to treat symptoms of depression. If results show that B vitamin supplementation
reduces symptoms of depression, recommendations will be made for further evaluation and trials
of using B vitamins to treat symptoms of depression, to determine if this treatment option should
be adopted into our health care system.
Depression and Antidepressants
There are several reasons for exploring and researching alternative depression treatments.
By 2020, depression is projected to be the second largest health burden worldwide (Sado et al.,
2009). In low socio-economic populations, the purchase of and adherence to antidepressant
drugs is low (Hansen et al., 2004), so there is a need for less expensive options. Patients often
experience negative side effects of antidepressants with the most common including headache,
nausea, drowsiness, fatigue, dry mouth, constipation, diarrhea, anorexia, insomnia, tremors,
vertigo, sexual dysfunction, anxiety, flu-like symptoms, sweating, and weight gain (Kikuchi et
al., 2011). Men report more side effects than women, and whether a symptom is reported or not
depends on the type of side effect (Kikuchi et al., 2011). Sexual dysfunction is the side effect
least reported to physicians, particularly by women, and less personal side effects, such as dry
mouth, are reported more frequently (Kikuchi et al., 2011). This shows that patients may
discontinue their prescribed medications for side effects unreported to physicians, but it may not
necessarily mean they do not want to receive treatment for their depression. People experiencing
unpleasant side effects from antidepressant medications may be willing to try an alternate
therapy that may not have unpleasant side effects.
Treatment-resistant depression is found in more than one third of all people being treated
for depression, and over 50% of people who positively respond to antidepressant medications do

16
not experience full remission (Souery, Papakostas, & Trivedi, 2006). There is a possibility that
treatment-resistant patients may have vitamin deficiencies (Kate, Grover, & Agarwal, 2010; Rao
et al., 2008). Patients resistant to drug treatment that were found to be deficient in vitamin B12
were given a B12 supplement in conjunction with the drug therapy, and the effectiveness of the
antidepressants increased with the B12 supplementation (Kate et al., 2010; Rao et al., 2008).
With B12 supplementation, the antidepressant effectiveness increased enough that the
medication dosage was slowly reduced, and some medications were eventually stopped (Kate et
al., 2010; Rao et al., 2008). Attitudes toward antidepressants also play a role in their use for
treatment of depression. People over age 40 tend to have a more negative view of
antidepressants, and men have a more negative view of antidepressants than women
(Chakraborty et al., 2009), so younger populations and women may be more likely to adhere to
alternative therapy.
Depression and Supplements
Few studies are available on usage and attitudes toward dietary supplements in treating
depression. However, nearly three-quarters of the adult U.S. population have used supplements
for unnamed reasons, and few have experienced adverse effects from taking supplements (Timbo
et al., 2006), so it is likely attitudes towards supplement use is favorable. Research is limited,
but it appears that around 30% of the U.S. population has tried a supplement to treat unnamed
major illnesses instead of using prescribed medication (Timbo et al., 2006). Dietary supplements
taken by people with depression are varied and are usually taken for other physical ailments,
such as fish oil for arthritis (Silvers et al., 2006). In one study, both men and women who had
previously been diagnosed with depression were more likely to take a vitamin supplement than
people without depression (Zhao et al., 2011).

17
Little research has been conducted regarding drug-nutrient interactions with
antidepressants, yet one study showed that 80% of participants were taking both a supplement
and an antidepressant (Silvers et al., 2006). The most commonly consumed supplements were
multivitamin and mineral supplements at 81%, and vitamin B complexes at 36% (Silvers et al.,
2006). Sixteen percent to 18% of older adults with depression use a dietary supplement,
although the purpose for supplement use was not discussed (Kales, Blow, Welsh, & Mellow,
2004; Silvers et al., 2006). Older adults often take a combination of medications, and in a study
of older adults with major depression and/or bipolar disorder, 20% preferred to use an herbal or
nutritional supplement over medication, and 16% believed supplements were safer to use than
prescribed medications (Keaton et al., 2009). An herbal or nutritional supplement was used daily
by 18% of the participants, and 26% used a supplement weekly (Keaton et al., 2009). This
shows that some older adults may be more receptive to alternative depression treatments.
Gender may also play a role in treatment choices, as women with depression use dietary
supplements more often than men (Silvers et al., 2006; Zhao et al., 2011).
B Vitamins
B vitamins are most abundant in the diet in meat and animal products, especially organ
meats, and for many people in fortified foods (Mahan, Escott-Stump, Raymond, & Krause,
2012). Many plant foods contain varying amounts of the different B vitamins, especially
legumes, whole grains, yeast, and green leafy vegetables (Mahan et al., 2012). Vitamin B12 is of
concern for vegans, because B12 is only available from animal sources (Mahan et al., 2012).
Vegans and vegetarians with low animal product intake require a B12 supplement to prevent B12
deficiencies (Mahan et al., 2012). Older adults also sometimes require B12 supplementation

18
because of reduced production of intrinsic factor in the stomach, an important protein which is
needed to utilize B12, and overall lower food consumption (Mahan et al., 2012).
B vitamins are essential for the metabolism of carbohydrates, proteins, and fats, as well
as serving as coenzymes necessary for the generation of energy (Mahan et al., 2012). Many B
vitamins are essential for growth, tissue respiration, appetite and digestive function, and healthy
nerves (Mahan et al., 2012). Some serve as antioxidants, and some aid in the formation and
repair of DNA (Mahan et al., 2012). Deficiencies of several B vitamins cause problems with the
central nervous system, including neurological problems (Mahan et al., 2012). Not many human
subject trials have been completed using B vitamins to treat depression, and most of those studies
do not use a single B vitamin, but rather a combination of a few B vitamins that often include
other vitamins or minerals. The various B vitamins are considered in depression because of their
impact in certain mechanisms in the body that are linked to depression.
Thiamin (B1). Thiamin deficiencies are associated with depression in both animals and
humans (Zhang et al., 2013). In studies involving rats, thiamin deficiency leads to depressive-
like symptoms, which were evaluated by using standard tests such as forced swimming, activity
in open spaces, and movement during tail suspension (Nikseresht et al., 2012). Low serum
levels of thiamin were associated with higher incidence of depressive symptoms in a population
of older Chinese adults (Zhang et al., 2013). In a population of hospitalized older adults, thiamin
deficiencies were associated with depression, as well as Alzheimer’s disease, cardiac failure,
falls, and furosemide use (Pepersack et al., 1999). Supplementation of thiamin, along with zinc
and magnesium, improved depressive symptoms in rats that had been depression-induced using
the depressant drug reserpine (Nikseresht et al., 2012).

19
Thiamin may be involved in depression or other psychiatric issues due to its function in
the nitrergic system, which plays a role in neuroendocrine responses (Reis, Saad, Camargo,
Elias, & Antunes-Rodrigues, 2010). Thiamin is specifically involved in the synthesis of
serotonin, a neurotransmitter thought to contribute to a sense of happiness and well-being
(Mahan et al., 2012). Studies have been done on rats induced with thiamin deficiency, and
alterations in their serotonin function occurred (Mousseau, Raghavendra-Rao, & Butterworth,
1996). Thiamin-deficient rats exhibited a successful reduction in depressive symptoms by
treatment with either serotonin or the antidepressant medication fluoxetine, an SSRI (Onodera,
Ogura, & Kisara, 1981). Thiamin deficiency appears to decrease the uptake of serotonin, and
when rats were supplemented with thiamin, serotonin uptake increased (Plaitakis, Nicklas, &
Berl, 1978). The research conducted regarding thiamin and its role with serotonin has only been
studied in rats. Overall, little research has been conducted on thiamin and its involvement in
depression, and there do not appear to be human trials using thiamin to treat depression.
Riboflavin (B2). Low riboflavin intake was associated with depressive symptoms in
adolescent girls, but not adolescent boys (Murakami, Miyake, Sasaki, Tanaka, & Arakawa,
2010). Low serum levels of riboflavin were associated with depression in a study with female
nurses (Naghashpour, Amani, Nutr, Nematpour, & Haghighizadeh, 2011), and riboflavin may
reduce symptoms of postpartum depression (Miyake et al., 2006). Therefore, it would appear
that low riboflavin status is associated with depression in women but not in men. However, the
research conducted was only on female populations except for one study with adolescents that
looked at dietary correlations. There do not appear to be trials using riboflavin to treat
depression, but the mechanism for its action in depression may be its involvement in activating
vitamin B6 and folate (Mahan et al., 2012), the importance of which is discussed below.

20
Niacin (B3). There are few sources and no randomized controlled trials for using niacin
to treat depression, and the small amount of literature available on niacin and depression is from
approximately six decades ago (Prousky, 2010). However, there is enough evidence that niacin
may widen the blood vessels in the brain, allowing for increased circulation which in turn may
reduce depression (Prousky, 2010). Niacin is linked to serotonin through tryptophan, an
essential amino acid (Mahan et al. 2012). Tryptophan is needed to synthesize serotonin, but is
also the substrate necessary for the synthesis of niacin for use in the body (Mahan et al. 2012).
Niacin supplementation could potentially reduce the need for tryptophan’s conversion to niacin,
and allow it instead to be used for the creation of serotonin. If niacin is supplemented in the
form of niacinamide, the flushing that sometimes happens with increased niacin intake in the
form of nicotinic acid is avoided (Prousky, 2010).
Vitamin B5 (Pantothenic Acid). There is little to no research, and no trials using
vitamin B5 in the treatment of depression, although it is included in most B complex
supplements. True B5 deficiency in humans is rare, but when found, so is depression (Mahan et
al., 2012).
Vitamin B6 (Pyridoxine). Vitamin B6 is a coenzyme involved in the tryptophan-
serotonin pathway, and deficiency of serotonin in the brain can cause depression (Williams et al.,
2005). B6 is also involved in the synthesis and metabolism of the neurotransmitter γ-
aminobutyric acid (GABA), low levels of which are associated with anxiety and depression
(Guilloux et al., 2011; Möhler, 2012). Rats with diets deficient in vitamin B6 have reduced
levels of GABA (Bayoumi, Kirwan, & Smith, 1972). In one study, the amount of serotonin and
GABA in the hypothalamus of B6-deficient rats was significantly lower than in control rats
(Paulose, Dakshinamurti, Packer, & Stephens, 1988). When the B6-deficient rats were given B6

21
supplements, their serotonin and GABA levels in the hypothalamus returned to normal (Paulose
et al., 1988). The B6 deficient rats also had significantly higher blood serum levels of
epinephrine and norepinephrine than the control rats, and when the rats were given B6
supplementation the serum levels of those hormones returned to normal (Paulose et al., 1988).
Vitamin B6 is involved in the synthesis and metabolism of the hormone and neurotransmitters
called the catecholamines, which include dopamine, epinephrine and norepinephrine (Mahan et
al., 2012). The catecholamines act on the sympathetic nervous system invoking the “fight or
flight” response and high levels are associated with stress and hypertension (Laverty, 1978).
They are involved in mood and behavior, and dopamine is specifically used in the pleasure-
reward system of the brain (Depue & Collins, 1999). As evidenced in the rat study described
above, B6 is not only needed to synthesize the catecholamines, it is also needed to catabolize the
catcholamines to prevent excess accumulations.
Vitamin B6 is also involved in homocysteine metabolism (Williams et al., 2005).
Homocysteine is a marker of inflammation and promotes oxidative stress, and high levels in the
body are associated with vascular disease, depression, and can affect neurotransmitter function
(Folstein et al., 2007; Sachdev et al., 2005). Vitamin B6 is needed to convert homocysteine to
cysteine, thereby reducing homocysteine levels, so a connection of B6 to depression may also be
involved by this mechanism (Folstein et al., 2007; Williams et al., 2005).
Research has shown that different population types with low B6 intake have higher
incidence of depression including adolescents, older adults, and women with hormone-related
depression such as premenstrual syndrome and premenstrual dysphoric disorder (Murakami et
al., 2010; Skarupski, et al., 2010; Williams et al., 2005). A large study involving predominantly
middle-aged men and women showed that B6 intake had no correlation with depression

22
(Sánchez-Villegas et al., 2009); however a low blood plasma of B6 has been associated with
depression (Hvas, Svend, Bech, & Nexø, 2004). There are few trials using B6 to treat symptoms
of depression. In stroke patients, incidence of major depression is high, and one study found that
although the decrease in the prevalence of major and minor depression in stroke patients who
received a supplement of B6, folate, and B12 was nonsignificant, it did significantly lower the
odds of experiencing a major depressive episode (Almeida et al., 2010).
Vitamin B6 supplementation has been found useful in treating depression in pre-
menopausal women (Williams et al., 2005), and it may be useful in treating depression in women
who take oral contraceptives (Wilson, Bivins, Russell, & Bailey, 2011). A side-effect of oral
contraceptive use for some women is depression, which may be due in part because oral
contraceptives negatively impact vitamin B6 status (Wilson et al., 2011). Abnormal tryptophan
metabolism occurs in women taking oral contraceptives, and studies have shown that high doses
of B6 supplementation corrected the problem (Aly, Donald, & Simpson, 1971; Luhby et al.,
1971).
Biotin (B7). Biotin deficiency in humans is extremely rare because it is widely available
in foods and is produced by intestinal flora (Mahan et al., 2012). No dietary references have
been established because there has not been enough research to set such standards (Mahan et al.,
2012). The amount of biotin the intestinal flora produces and is used by the body is still
unknown, and there are differences in the bioavailability of biotin in foods (Mahan et al., 2012).
In the few recorded human cases of biotin deficiencies there was depression (Mahan et al.,
2012). In cases of people who have a genetic defect of biotin enzymes, there are serious
neurological problems (Mahan et al., 2012).

23
Folate (B9). Folate is involved in the synthesis and metabolism of the neurotransmitters
and the mood hormones which include serotonin, epinephrine, norepinephrine and dopamine
(Sachdev et al., 2005; Sanchez-Villegas et al., 2009). Folate also plays an important part in
homocysteine metabolism, helping to synthesize methionine from homocysteine (Folstein et al.,
2007; Sachdev et al., 2005). Like B6, there may be a link to depression by folate’s role in
reducing circulating homocysteine levels (Folstein et al., 2007; Sachdev et al., 2005).
Studies involving folate and depression conflict, but most literature points to an
association between low dietary intake and low blood serum levels of folate and depression
(Miller, 2008). To illustrate, one study found that there was no association between dietary
folate intake and depression in older adults (Skarupski, et al., 2010), but a separate study found
the opposite results (Payne et al., 2009). Low dietary intake of folate in adolescents was
associated with depression (Murakami et al., 2010), as well as in a large sample of adult
Japanese workers (Koichi, et al., 2012). Sanches-Villegas et al. (2009) found that low dietary
intake of folate was associated with depression in men but not women. Low serum folate and
low red blood cell folate levels are often associated with depression; however, there is some
literature that shows no association with low serum folate (Dimopoulos et al., 2007; Morris,
Trivedi, & Rush, 2008; Ng, Feng, Niti, Kua, & Yap, 2009; Nguyen et al., 2009; Sachdev et al.,
2005; Tiemeier et al., 2002).
In a study with Guatemalan women, an association was found between low red blood cell
levels of folate and depression, and both daily and weekly supplementation of folate with
vitamin B12, iron and zinc reduced symptoms of depression, but the trial was not placebo-
controlled (Nguyen et al., 2009). It is also likely that supplementation of folate can help reduce
incidence of depression after stroke (Almeida et al., 2010). There are few other human trials

24
using folate to treat depression, but there are some animal models. Folic acid successfully
treated depression in mice (Brocardo, Budni, Kaster, Santos, & Rodrigues, 2008). Depression-
induced rats were given different treatments and then performed a series of tests to determine a
reduction in depression (El-Sisi, 2011). The tests showed that a combination of omega-3 plus
folate and B12, or an antidepressant medication plus the B vitamins, had a greater reduction of
depressive symptoms than just the omega-3 supplementation, B vitamins, or antidepressant
medication alone (El-Sisi, 2011). This shows that using the B vitamins as an adjunct treatment
could be very effective.
The type of antidepressant being used by the patient may be an important consideration in
the decision to supplement. In the rat study mentioned above, the antidepressant fluoxetine was
used (El-Sisi, 2011), and one study found that patients had a poor response to fluoxetine when
red blood cell folate levels were low (Fava, Borus, Alpert, & Nierenberg, 1997). However, a
different study found that red blood cell folate status had no bearing on the efficacy of fluoxetine
in patients, and instead found a worse response to the antidepressant nortriptyline if patients had
low red blood cell folate levels (Beaglehole, Luty, Mulder, Kennedy, & Joyce, 2007). People
with low serum levels of folate have a significantly lower response to selective serotonin re-
uptake inhibitors (SSRIs) to treat depression than in people with higher levels of serum folate,
and individuals experience higher incidence of relapse (Alpert, Silva and Pouget, 2003; Miller,
2008; Papakostas, 2004). Despite the evidence that folate could play an important role in
treating depression, there have been very few human trials.
Vitamin B12 (Cobalamin). Like folate and vitamin B6, vitamin B12 is also involved in
the synthesis and metabolism of the neurotransmitters and mood hormones serotonin,
epinephrine, norepinephrine and dopamine (Sachdev et al., 2005; Sanchez-Villegas et al., 2009).

25
Vitamin B12 also has a relationship with homocysteine, acting as an enzymatic cofactor to
convert homocysteine to methionine (Folstein et al., 2007; Sachdev et al., 2005). In much the
same way as B6 and folate, B12 may be another link to depression via its action in reducing
circulating homocysteine levels (Folstein et al., 2007; Sachdev et al., 2005).
Studies involving B12 and depression are conflicting. An association between low B12
intake and depression was found in women, but not in men (Sanchez-Villegas et al., 2009).
Higher dietary intakes of B12 appear to be protective of depressive symptoms in older adults
(Skarupski, et al., 2010), but no association between B12 intake and depression was found in
adolescents (Murakami et al., 2010). Studies showed that low serum B12 levels were associated
with symptoms of depression (Dimopoulos et al., 2007; Ng et al., 2009; Tiemeier et al., 2002),
but one study did not find this correlation (Sachdev et. al., 2005). In a group of disabled older
women, deficiency in serum B12 was associated with double the risk of severe depression
(Penninx et al., 2000).
As studies previously mentioned have shown, supplementation with B12 may be
effective at reducing symptoms of depression (El-Sisi, 2011; Nguyen et al., 2009). There are
case studies of treatment-resistant depression that when an underlying B12 deficiency was
discovered, improvement was shown with B12 supplementation (Kate et al., 2010; Milanlioğlu,
2011; Rao et al., 2008). In patients being treated with SSRIs, higher serum B12 levels were
associated with better treatment outcomes (Hintikka, Tolmunen, Tanskanen, & Viinamäki,
2003). Severe fatigue and depression after stroke is associated with B12 deficiency, and may be
alleviated with B12 supplementation (Almeida et al., 2010; Huijts, Duits, Staals, & van
Oostenbrugge, 2012). However, in a randomized double-blind placebo-controlled trial, no
improvement in depressive symptoms was achieved with B12 supplementation (Hvas, Juul,

26
Lauritzen, Nexø, & Ellegaard, 2004). There is a lack of trials using B12 to treat depression, and
the majority of research with B12 has focused on other psychiatric and neurological disorders
rather than depression.
Present Study
The review of the literature shows a strong correlation between B vitamin deficiencies
and depression, yet there have been few trials conducted that use B vitamins to treat symptoms
of depression. In the United States specifically, there has been little research and very few trials
conducted on using B vitamins to treat symptoms of depression, yet depression is a growing
healthcare burden. For this research, the following questions were asked:
1. Does B vitamin supplementation decrease symptoms of depression?
H1: B vitamin supplementation will decrease symptoms of depression. As seen in
the literature review, there is a trend is towards improvement of depressive
symptoms with B vitamin supplementation. B vitamins show an interrelated
relationship, but the previously conducted trials only use one to three of the B
vitamins, which may explain the conflicted findings. Since this study uses a B
vitamin supplement that includes all of the B vitamins, an improvement in
depressive symptoms is expected.
2. Does B vitamin supplementation decrease symptoms of depression in people who take
antidepressants yet still experience symptoms of depression?
H1: B vitamin supplementation will decrease symptoms of depression in people
who take antidepressants yet still experience symptoms of depression. The few
case studies available on treatment-resistant depression with B vitamin

27
supplementation show a favorable outcome, therefore an improvement of
depressive symptoms is expected.
3. Does dietary intake of B vitamins affect the efficacy of B vitamin supplementation in
reducing symptoms of depression?
H1: There will be a reduction of depressive symptoms in people regardless of
adequate or inadequate B vitamin intake. The Dietary Reference Intakes for B
vitamins are for a healthy population, and people suffering from depression are not
considered part of a healthy population. It is likely that some people living in the
United States who suffer from depression consume adequate dietary B vitamins
because of B vitamin fortification in foods otherwise low in B vitamins. The
previously conducted trials do not assess their participants’ dietary B vitamin
intake, but the overall trend is towards improvement in depressive symptoms with B
vitamin supplementation. Therefore, an increase in depressive symptoms is
expected even in participants that have adequate intake of B vitamins.
In the literature review, research showed that sometimes there were gender differences in
correlations and response to B vitamin supplementation, so gender was considered as a
supplementary analysis. Participant smoking status and alcohol consumption data were collected
as potential modifying factors, because both activities deplete B vitamins in the body. To
determine the population distribution of Body Mass Index (BMI), participant height and weight
were measured to calculate BMI. Finally, participants were asked about possible side effects to
the B vitamin supplementation, since the side effects of antidepressants are a major deterrent to
their adherence.

28
Chapter III: Methodology
The purpose of this research was to investigate the effectiveness of B vitamin
supplementation in reducing symptoms of depression. This chapter describes the study
methodology including subject selection and description, instrumentation, data collection
procedures and analyses used. The study limitations are also discussed.
Subject Selection and Description
This research study was reviewed and approved by the University of Wisconsin-Stout
Institutional Review Board of Human Subjects (Appendix A). All subject participation was
voluntary. Participants were recruited via an email sample of 50% of students and staff at the
University of Wisconsin-Stout, using a computer randomized email list made available from the
Planning, Assessment, Research and Quality office on the UW-Stout campus. Participants were
also recruited via advertisements placed on campus and in the community. After initial contact,
potential subjects were sent a letter via email to see if they qualified (Appendix B). Participant
exclusions included pregnant and nursing women, those already regularly taking B vitamin
supplements, those diagnosed with mental health conditions other than depression, and those
with metabolic conditions or medication use that prevented B vitamin usage. Participants
diagnosed with an anxiety issue along with their depression were included, but those with severe
psychopathology issues were excluded.
Instrumentation
All participants signed a consent to participate form (Appendix C). Each participant
received a subject number, obtained using an online random number generator. The Center for
Epidemiologic Studies Depression (CES-D) scale was used to assess depression. The validity
and reliability of the CES-D in assessing depression has been documented and utilized in
numerous studies (Radloff, 1977). The CES-D has a scoring range from 0 to 60, with higher

29
scores indicating more severe symptoms of depression. A score ≥ 16 on the CES-D is
considered indicative of clinically significant depression. A questionnaire was created with
Qualtrics using the questions from the CES-D as well as questions about medication usage, age,
gender, alcohol consumption, and smoking status (Appendix D). The CES-D was administered
again via Qualtrics at the end of the intervention, and the questionnaire included areas for
participant comments on potential side effects, and to record the amount of any remaining
supplements (Appendix E). Two 24-hour food diaries were taken to assess usual B vitamin
intake. Participants were given a form to fill out for the food diaries, created and adapted from
various samples (Appendix F). Participant height and weight was taken using the equipment in
UW-Stout’s Nutrition Assessment Lab, to calculate BMI and enter into the diet analysis software
Food Processor.
The B vitamin supplement given to the participants to consume was a complex called
Glycogenics®, developed and manufactured by Metagenics, Inc., and formulated to promote
bioavailability of the B vitamins (Appendix G). Per tablet, Glycogenics® contains the B
vitamins: thiamin (as thiamin mononitrate) 14 mg; riboflavin 16 mg; niacin (as niacinamide and
niacin) 200 mg; pantothenic acid (as D-calcium pantothenate) 75 mg; vitamin B6 (as pyridoxine
HCl) 22 mg; biotin 250 mcg; folate (as folic acid and L-5-methyltetrahydrofolate) 400 mcg;
vitamin B12 (as cyanocobalamin) 250 mcg. Glycogenics® also contains other ingredients to
promote B vitamin absorption: vitamin C (as ascorbic acid) 125 mg; choline (as choline
bitartrate) 100 mg; inositol 94 mg; para-aminobenzoic acid (PABA) 15 mg. There are also
inactive ingredients to form the capsule and coating. Glycogenics® is formulated to exclude:
wheat, gluten, soy protein, animal and dairy products, nuts, tree nuts, fish, crustacean shellfish,
colors, artificial sweeteners, and preservatives. Because the supplement contains some of the B

30
vitamins in pharmacological doses, the company chooses to sell their products only to licensed
or certified health care practitioners.
Data Collection Procedures
Data collection was conducted from February 7, 2013 to March 11, 2013. Participants
arrived by appointment to UW-Stout’s Nutrition Assessment Lab. After signing the informed
consent form, participants completed the CES-D questionnaire and demographic questions via
Qualtrics using the Nutrition Assessment Lab computer. Next height and weight were measured,
and their 24-hour food diary was collected. Finally, participants were given a 28-day supply of
B vitamins with instructions (Appendix H). Participants took one tablet daily for 28 days.
Participants returned to the Nutrition Assessment Lab by appointment 28 days later, where they
completed the CES-D questionnaire and were able to leave comments, again via Qualtrics using
the Nutrition Assessment Lab computer. A second 24-hour food diary was collected. The
participants were asked to bring any unused tablets to the final appointment to assess
compliance. Three participants were unable to make the last in-person appointment, so they
completed the final questionnaire online from their personal computers.
Data Analysis
The Statistical Program for Social Sciences (SPSS) version 19.0 was used to analyze the
data. A paired samples t-test was conducted to determine if there was a significant difference
between the participants’ baseline CES-D scores and post-intervention CES-D scores. A
univariate ANOVA was conducted to assess if there were differences in the reduction of
depressive symptoms between the medicated and unmedicated participants, between participants
with dietary inadequacy in six or more B vitamins versus those with dietary inadequacy in two or
fewer B vitamins, and between male and female participants. Participant gender, age, height and

31
weight were entered into the diet analysis software Food Processor, which was used to determine
individual B vitamin needs and to analyze the B vitamin content of subjects’ diets. The program
compared participants’ estimated nutrient needs with actual consumption to assess whether their
dietary intake of the B vitamins was adequate or inadequate based on reference standards.
Limitations
The self-reported two 24-hour food diaries may be a study limitation, as participants may
have over or underreported the amount and types of foods consumed. More nutrition counseling
strategies could have been employed to increase the accuracy of the food diaries. However, it
would have required more of the participants’ time. Twenty-four hour food recalls and food
diaries are considered more accurate than Food Frequency Questionnaires (FFQs) in assessing
average food intake (Schatzkin et al., 2003), and requiring more food records up to the entire
length of the study rather than just the two sample days obtained would have given a more
accurate diet history. However, studies generally limit the amount of food recalls or diaries
taken to no more than three days because of the time consuming nature of the data entry
involved, and in fact are more apt to use FFQs (Schatzkin et al., 2003). Although Food
Processor has an extensive database, it has limitations in available food choices, and the
researcher may not have always chosen a correct representative food item.
Individual participants’ ability to absorb the various B vitamins was not measured or
taken into account, which was beyond the scope of this study. Also beyond the scope of this
study was assessing biochemical B vitamin status and markers in the participants. There are
possible participant life situations or other unknown variables that could have affected the
results. There was no placebo group with which to compare the treatment group, so it is
unknown how much of the results are due to the effect of the B vitamin supplement.

32
Chapter IV: Results
The purpose of this research was to investigate the effectiveness of B vitamin
supplementation in reducing symptoms of depression. Participants in this study took a B vitamin
supplement for 28 days, and their depressive symptoms were assessed at baseline and at the end
of the study. This chapter includes participant demographics and the results of data analyses.
Description of the Participants
There were 35 participants at the start of the study. One participant discontinued the
study due to possible negative side effects, and one subject failed to complete the final
questionnaire. The 33 participants that completed the study were students and staff at UW-Stout.
There were 21 females (63.6%) and 12 males (36.4%). Participant age range was from 19 to 63
years (M = 28.3, SD = 13.7), with a median age of 21 years. Participant BMI range was from
17.9 to 49.0 kg/m2 (M = 28.4, SD = 8.3). Table 1 shows the percentages of participants that fell
into the different BMI categories.
Table 1
Participant Body Mass Index (BMI)
BMI Category Frequency (N=33) Percentage
< 18.5 Underweight 1 3.0%
18.5 - 24.9 Normal 13 39.4%
25.0 - 29.9 Overweight
30.0 - 39.9 Obese
≥ 40.0 Morbid obese
7
7
5
21.2%
21.2%
15.2%

33
Twenty-four of the participants (72.7%) were not taking antidepressant medications and
nine participants (27.3%) were taking antidepressant medications which included: Bupropion
(Wellbutrin), Citalopram, Fluoxetine (Prozac), Nortriptyline, Sertraline (Zoloft), and
Venlafaxine. There were four smokers (12.1%) and 29 nonsmokers (87.9%). Frequency of
alcohol consumption by the participants is shown in Table 2.
Table 2
Participant Alcohol Intake Frequency
Alcohol Consumption Frequency (N=33) Percentage
Almost every day 1 3.0%
5 or 6 days a week 0 0.0%
3 or 4 days a week
Once or twice a week
Once or twice a month
Less than once a month
0
9
10
13
0.0%
27.3%
30.3%
39.4%
First Objective
The first objective of this research was to investigate if B vitamin supplementation may
reduce symptoms of depression in people. Participant CES-D scores were used to assess
symptoms of depression. The range of participant CES-D scores at baseline was 15 to 52 (M =
31.4, SD = 9.6). One subject had a baseline score of 15, which is less than the generally used
cut-off score of 16 that indicates clinically significant depression. A score of 16 was not
necessary for the purpose of this study, because a diagnosis or screening for clinical depression
was not needed to participate in this study. A paired samples t-test was conducted to compare

34
0
5
10
15
20
25
30
35
Baseline Post-Intervention
CES
-D S
core
31.4 (9.6)a
18.9 (10.4)b
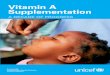
participant baseline CES-D scores with their post-intervention CES-D scores. There was a
significant decrease in participant CES-D scores from baseline (M = 31.4, SD = 9.6) and at post-
intervention (M = 18.9, SD = 10.4), t(32) = 7.08, p < .001 (Figure 1). The effect size, d, was
1.23, a large effect. The hypothesis that B vitamin supplementation would decrease symptoms
of depression was supported by this finding.
Figure 1. Change in the participants CES-D depression score average from baseline to post-
intervention; a < b, p < .001.
Second and Third Objectives and Gender
The second objective of this research was to determine if B vitamin supplementation
reduced symptoms of depression in people who take antidepressant medication, but still
experience symptoms of depression. The third objective of this research was to determine if
dietary intake of B vitamins affected the efficacy of B vitamin supplementation in reducing
symptoms of depression. A supplementary analysis of this research was to determine if there

35
were gender differences in the reduction of symptoms of depression. A univariate ANOVA was
conducted on these three variables.
There was no significant difference in the reduction of CES-D scores between the
medicated (N = 9; M = -9.22, SD = 8.64) and unmedicated (N = 24; M = -13.62, SD = 10.49)
participants, F (1, 32) = .603, p = .445, showing that both groups experienced a similar reduction
in symptoms of depression. This finding supports the hypothesis that B vitamin supplementation
would decrease symptoms of depression in people who take antidepressants yet still experience
symptoms of depression.
Table 3 shows the frequencies of adequate or inadequate participant dietary consumption
of each B vitamin.
Table 3
Participant Adequacy of Dietary Intake of B Vitamins
B Vitamin Adequate Intake Inadequate Intake
B1 (thiamin) 19 (57.6%) 14 (42.4%)
B2 (riboflavin) 20 (60.6%) 13 (39.4%)
B4 (niacin)
B5 (pantothenic acid)
B6 (pyridoxine)
B7 (biotin)
B9 (folic acid)
B12 (cobalamin)
26 (78.8%)
11 (33.3%)
18 (54.5%)
11 (33.3%)
14 (42.4%)
22 (66.7%)
7 (21.2%)
22 (66.7%)
15 (4.55%)
22 (66.7%)
19 (57.6%)
11 (33.3%)
Note: N =33

36
Eleven participants (33.3%) had inadequate intake of six or more of the B vitamins, and
22 participants (66.7%) had inadequate intake of two or fewer of the B vitamins. There was no
significant difference in the reduction of depressive symptoms between the group inadequate in
six or more B vitamins (M = -14.18, SD = 4.05) and the group inadequate in two or fewer of the
B vitamins (M = -11.55, SD = 12.03), F (1, 32) = .058, p = .811, showing that both groups
experienced a similar reduction in symptoms of depression regardless of their dietary B vitamin
intake.
There was no significant difference in the reduction of depressive symptoms between
women (M = -12.67, SD = 9.58) and men (M = -12.00, SD = 11.35), F (1, 32) = .007, p = .936,
showing that both groups experienced a similar reduction in depressive symptoms. This finding
supports the hypothesis that there would be a reduction of depressive symptoms in people
regardless of adequate or inadequate B vitamin intake.
Possible Side Effects
One participant dropped out of the study due to experiencing possible negative side
effects from taking the B vitamin supplement. The participant said that it was “excruciatingly
difficult to focus on anything” and experienced a “mild depressive breakdown.” The participant
also felt “weird, high, and light-headed.” However, while these mental symptoms were going
on, the participant was very physically calm, as fidgeting by bouncing a leg, tapping fingers, etc.,
was usual, and instead was able to be “content with sitting still.” The participant gets depressive
episodes approximately four or five times per year, but there is usually a trigger for them. The
participant thought the B vitamin supplement was the most likely trigger, although a second
possibility was that around the same time the participant stopped a usual exercise routine.

37
The final questionnaire asked participants if they had noticed any positive or negative
effects during the study. Nine participants (27.3%) reported experiencing negative effects:
digestive or stomach issues (n = 2); nausea or heightened gag reflex (n = 3); felt more depressed
(n = 1); increased appetite (n = 1); and sleep difficulties (n = 2). Twenty-five participants
(75.8%) reported experiencing positive side effects: increased energy (n = 11); improved
mood/outlook (n = 16); smiled more (n = 1); more assertive (n = 1); fewer crying spells (n = 1);
desire for exercise (n = 1); desire for healthier foods (n = 1); easier to wake up in the morning (n
= 4); decreased appetite (n = 2); more alert/clear-headed (n = 3); and increased desire to eat
breakfast (n = 1). Neutral comments were that some disliked the taste of the supplement, some
experienced yellower urine, and some stated they were going to continue B vitamin
supplementation on their own because of the perceived benefits.

38
Chapter V: Discussion
The purpose of this research was to investigate the effectiveness of B vitamin
supplementation in reducing symptoms of depression. This chapter includes a discussion of the
research, conclusions, and recommendations.
Discussion
The first hypothesis of this research was that B vitamin supplementation would decrease
symptoms of depression. The results support this hypothesis showing a significant decrease in
depressive symptoms with a large effect size, with an average 12.5 point drop in scores on the
CES-D scale, after participants took a B complex vitamin for 28 days. Previous research showed
a trend towards a decrease in depressive symptoms with higher B vitamin intake or blood serum
values as well as with B vitamin supplementation, but there was also opposing research. The
data may conflict because the studies looked at three or fewer B vitamins, sometimes with the
addition of other vitamins or minerals. As the literature review explored, the mechanisms of the
B vitamins are often connected. An example is that riboflavin is needed to activate vitamin B6
and folate, yet trials with vitamin B6 and/or folate supplementation do not include riboflavin, nor
was riboflavin status assessed. A search of the EBSCO, PubMed, and Google Scholar databases
revealed no animal or human subject trials using a B complex supplement to treat symptoms of
depression. The B vitamin supplement used in this research gave the full complement of B
vitamins, which was unlike other similar research, and may be why a positive effect was found.
The results here show that larger, placebo-controlled trials using a B complex supplement are
warranted to further investigate B vitamins in treating depression.
Care was taken to avoid confounding factors, beginning with the participant exclusions as
shown in Appendix B, which included the exclusion of participants that had ever been diagnosed

39
with a mental illness other than depression. A few participants also had anxiety issues, and they
were included in the study because anxiety and depression are closely linked (Dobson, 1985).
Participants had to be able to read and understand the English language, because the
questionnaires and instructions were given in English. To participate, it was not necessary to
have received a diagnosis of depression from a health care practitioner because not everyone
with a mental health problem seeks professional help, especially young people (Wilson, 2007).
Young people are even less likely to seek professional help if their symptoms are depressive, and
if they are male (Wilson, 2007). Therefore, because this research was conducted on a college
campus with a demographic population that is less likely to seek professional treatment for
depression, a medical diagnosis of depression was not necessary to participate. The CES-D
questionnaire was used to assess depression, because as described in the methods chapter it is a
reliable and valid tool commonly used in research studies.
Other potential confounding factors accounted for were smoking status and frequency of
alcohol consumption. Cigarette smoking causes depletion in the body of all of the B vitamins
(Gabriel et al., 2006), so participants were asked “Do you smoke?” on the first questionnaire
(Appendix D). Since only 4 participants smoked, it is unlikely that smoking status influenced
the results. Participants were also asked about their alcohol consumption on the first
questionnaire, because in the body, alcohol inhibits the absorption of B vitamins, particularly
thiamin (Mahan et al., 2012). Alcohol also inhibits B vitamin use in the body, increases vitamin
excretion, and causes the destruction of some, particularly folic acid (Mahan et al., 2012). As
shown in the results section, there was only one participant who drank nearly every day,
followed by a gap in frequency until “once or twice a week,” with the majority of participants

40
(69.7%) consuming alcohol “once or twice a month” or less. Therefore, it is unlikely that
frequency of alcohol consumption influenced the results.
Although it was explained to each participant during the first appointment that it was
possible no effects would occur to prevent bias, it is uncertain how many subjects experienced
positive results because they expected it. The major weakness of this study is that there was no
placebo group with which to compare the treatment group, the same weakness encountered in
most of the available research on B vitamin supplementation in treating depression. However,
the results showed a large effect size, so it is likely the improvement in depressive symptoms
was not due to participant expectation. The large effect size in this study, d = 1.23, is much
larger than the no more than moderate effect size found in most depression studies which have a
Cohen’s d range of 0.19 to 0.51 (Chang et al., 2006; Cuijpers, Smit, Bohlmeijer, Hollon, &
Andersson, 2010; Okumura & Sakamoto, 2011). In depression studies that have a placebo
group, on average, 30% of the participants in the placebo group experience positive effects, and
50% of the participants in the treatment group experience positive effects (Walsh, Seidman,
Sysko, & Gould, 2002). In this study, over 50% of the participants experienced a significant
reduction in their depressive symptoms, although that does not exclude the possibility that the
results were due to participant expectations.
The second hypothesis of this research was that B vitamin supplementation would
decrease symptoms of depression in people who take antidepressants yet still experience
symptoms of depression. This hypothesis was supported because results of this study found that
there was no difference in the reduction of depressive symptoms between medicated and
unmedicated groups. Individuals described in the literature review case studies were able to
reduce the dosage of their medications or the number of antidepressants taken with B vitamin

41
supplementation. This study showed that there was no interaction between medications and B
vitamin supplementation, so B vitamins may not only work well for some patients as an adjunct
therapy to antidepressants, but may be successful in treating depression when used alone. The
bulk of research in treatment-resistant depression found on the EBSCO, PubMed, and Google
Scholar databases focuses on dosage and drug substitution rather than possible nutrition
connections, but as explored in the literature review, some case studies have shown treatment
improvement following a nutrition intervention.
The third hypothesis of this research was that there would be a reduction of depressive
symptoms in people regardless of adequate or inadequate B vitamin intake. This hypothesis was
supported because results showed that there was a similar reduction in depressive symptoms
between participants with adequate dietary intake of B vitamins and those with inadequate B
vitamin intake. Despite grain fortification in the United States, only four participants had
adequate dietary intake for all of the B vitamins. Overall participant diet quality was poor, but
even in participants that had healthier, balanced diets, dietary adequacy in all of the B vitamins
was not achieved. Adequacy in all of the B vitamins was only achieved by participants who ate
a large quantity of food, much more than their recommended caloric intake. This shows that a B
vitamin supplement may be a viable option, because for many people, it is easier to take a pill
than transform the entire diet to meet their B vitamin needs while not exceeding their caloric
requirements. This is especially important to consider in patients with vegan and vegetarian
diets, and those with poor quality diets, which may be lower in B vitamins. It is also possible
that some people with depression have an underlying problem with the utilization of B vitamins,
so that dietary intake of B vitamins may not be sufficient, and a supplement is needed.

42
The dietary reference standards are for healthy people, and people with depression do not
fall into that category. Each person has a unique metabolism and genetic make-up, and it is
possible that some people do not adequately utilize the B vitamins available to them and need a
pharmacological dose of one or more of the vitamins, as opposed to simply meeting reference
standards. All of the B vitamins used in the study were given in doses well above the
Recommended Dietary Allowance (RDA), except for folate (at 100% RDA) and biotin (at 83%
RDA) (see Appendix G). It may be possible that some people who experience depression cannot
meet the quantity of B vitamins needed from the diet because there is an underlying metabolic
issue that requires a higher B vitamin intake. Metabolic implications are seen in the varying
positive and negative effects reported by the participants, such as increased or decreased
appetite, increased energy, easier to wake up, etc. Although the effects may not be due to the B
vitamin supplementation, upon reviewing the importance of B vitamins in human metabolism
and the literature specifically regarding depression, it is quite possible there is an underlying
metabolic insufficiency in some people for some of the B vitamins. Assessing the body’s
efficiency in metabolizing the B vitamins in the depressed person would be an interesting area
for further research. It should be noted that unlike in a study setting, each person is unique and
may not require supplements of all of the B vitamins, or could use a lower dose and still
experience positive effects. Individual adjustment is especially true if someone is experiencing
both positive and negative effects. An example in this study is that some people experienced
improved mood at the same time as experiencing sleep problems. It is possible that a lower dose
would avoid the sleep problems.

43
Conclusions
Overall, there is evidence that B vitamins play a role in depression and supplementation
may help alleviate symptoms of depression, but there is little research on B vitamins in the
treatment of depression, and the research that exists is conflicting. This research suggests that B
vitamin supplementation may reduce depressive symptoms in people whether medicated or
unmedicated, as both groups had a significant reduction in depressive symptoms. It also
significantly reduced symptoms of depression in people regardless of dietary B vitamin intake,
so people with a variety of eating patterns may equally benefit from B vitamin supplementation.
Some of the research explored in the literature review showed a response difference between
men and women, but this study found no difference in the reduction of depressive symptoms
between men and women.
Recommendations
The literature lacks human trials using B vitamins to treat symptoms of depression,
particularly placebo-controlled trials. This research shows that resources would be well used to
conduct randomized, placebo-controlled trials using B vitamins to treat depression. Since
associations between low B vitamin intake and depression were found in adolescents, trials
should be conducted to assess a safe alternative to antidepressant use in children, since many
antidepressants are not approved for use in children.
Health care professionals should consider B vitamin supplementation in patients who are
unwilling or unable to take antidepressants, or are responding poorly to traditional treatments.
As shown in the literature review, many people have a favorable opinion of supplement use. In
addition, many people who use antidepressant medications experience negative side effects, or
do not respond well to treatment. The bulk of research in treatment-resistant depression focuses

44
on dosage and drug substitution rather than possible nutrition connections, yet nutrition research
shows that nutrition intervention positively impacts treatment outcomes in people with
depression. In the article Folate and depression—a neglected problem (2007), author Simon
Young illuminates this fact, and proposes that simple, inexpensive treatments such as folate
supplementation are available to aid in treating depression yet are simply not being explored.
Another area for future research is to assess if there is a difference in the effectiveness of
vitamin B supplementation in reducing symptoms between mild, moderate, and severe
depression. Due to the small sample size in this study, this area was not analyzed, but future
research with a larger sample size could take this into account.
Community or college campus nutrition efforts in how nutrition can help people cope
with depression could be beneficial, because young people are not inclined to seek professional
help. Efforts should also be geared at making mental health practitioners aware of the
association between nutrition and depression. More studies and conclusive evidence could lead
to the incorporation of the nutrition connection in mental illness in the education curriculum of
mental health care practitioners.

45
References
Almeida, O. P., Marsh, K., Alfonso, H., Flicker, L., Davis, T. M., & Hankey, G. J. (2010). B‐
vitamins reduce the long‐term risk of depression after stroke: The VITATOPS‐DEP trial.
Annals of Neurology, 68(4), 503-510.
Alpert, M., Silva, R. R., & Pouget, E. R. (2003). Prediction of treatment response in geriatric
depression from baseline folate level: Interaction with an SSRI or a tricyclic
antidepressant. Journal of Clinical Psychopharmacology, 23(3), 309-313.
Aly, H. E., Donald, E. A., & Simpson, M. H. (1971). Oral contraceptives and vitamin B6
metabolism. The American Journal of Clinical Nutrition, 24(3), 297-303.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental
disorders (4th ed.). Washington, DC: American Psychiatric Association.
Bayoumi, R. A., Kirwan, J. R., & Smith, W. R. D. (1972). Some effects of dietary vitamin B6
deficiency and 4‐deoxypridoxine on γ‐aminobutyric acid metabolism in rat brain. Journal
of Neurochemistry, 19(3), 569-576.
Beaglehole, B., Luty, S. E., Mulder, R. T., Kennedy, M. A., & Joyce, P. R. (2007). Low red cell
folate levels are associated with poor response to nortriptyline in major depression. Acta
Neuropsychiatrica, 19(3), 204-207. doi:10.1111/j.1601-5215.2007.00215.x
Bender, D. A. (1984). Review: B vitamins in the nervous system. Neurochemistry International,
6(3), 297-321.
Berry, R. J., Bailey, L., Mulinare, J., Bower, C., & Dary, O. (2010). Fortification of flour with
folic acid. Food & Nutrition Bulletin, 31(Supplement 1), 22S-35S.

46
Brocardo, P. S., Budni, J., Kaster, M. P., Santos, A. R., & Rodrigues, A. L. S. (2008). Folic acid
administration produces an antidepressant-like effect in mice: Evidence for the
involvement of the serotonergic and noradrenergic systems. Neuropharmacology, 54(2),
464.
Centers for Disease Control and Prevention. (2011). An estimated 1 in 10 U.S. adults report
depression. Retrieved from http://www.cdc.gov/Features/dsDepression/
Chakraborty, K., Avasthi, A., Kumar, S., & Grover, S. (2009). Attitudes and beliefs of patients
of first episode depression towards antidepressants and their adherence to treatment.
Social Psychiatry and Psychiatric Epidemiology, 44, 482–488.
Chang, A. E., Ganz, P. A., Hayes, D. F., Kinsella, T., Pass, H. I., Schiller, J. H., Stone, R. M., &
Strecher, V. (2006). Oncology: An evidence-based approach. New York, NY: Springer
Science + Business Media.
Cuijpers, P., Smit, F., Bohlmeijer, E., Hollon, S. D., & Andersson, G. (2010). Efficacy of
cognitive–behavioural therapy and other psychological treatments for adult depression:
Meta-analytic study of publication bias. The British Journal of Psychiatry, 196(3), 173-
178.
Depue, R. A., & Collins, P. F. (1999). Neurobiology of the structure of personality: Dopamine,
facilitation of incentive motivation, and extraversion. Behavioral and Brain Sciences,
22(3), 491-517.
Dietrich, M., Brown, C. J., & Block, G. (2005). The effect of folate fortification of cereal-grain
products on blood folate status, dietary folate intake, and dietary folate sources among
adult non-supplement users in the United States. Journal of the American College of
Nutrition, 24(4), 266-74.

47
Dimopoulos, N., Piperi, C., Salonicioti, A., Psarra, V., Gazi, F., Papadimitriou, A., . . .
Kalofoutis, A. (2007). Correlation of folate, vitamin B12 and homocysteine plasma levels
with depression in an elderly Greek population. Clinical Biochemistry, 40(9/10), 604-
608. doi: 10.1016/j.clinbiochem.2007.01.007
Dobson, K. S. (1985). The relationship between anxiety and depression. Clinical Psychology
Review, 5(4), 307-324.
El-Sisi, S. F. (2011). Evaluation of the antidepressant like effect for some natural supplements
against reserpine induced behavioral depression in mice. New York Science Journal,
4(10), 93-104.
Fava, M., Borus, J. S., Alpert, J. E., & Nierenberg, A. A. (1997). Folate, vitamin B₁₂, and
homocysteine in major depressive disorder. American Journal of Psychiatry, 154, 426-
428.
Folstein, M., Liu, T., Peter, I., Buel, J., Arsenault, L., Scott, T., & Qiu, W. (2007). The
homocysteine hypothesis of depression. American Journal of Psychiatry, 164(6), 861-
867.
Gabriel, H. E., Crott, J. W., Ghandour, H., Dallal, G. E., Choi, S. W., Keyes, M. K., . . . Mason,
J. B. (2006). Chronic cigarette smoking is associated with diminished folate status,
altered folate form distribution, and increased genetic damage in the buccal mucosa of
healthy adults. The American Journal of Clinical Nutrition, 83(4), 835-841.
Gahche, J., Bailey, R., Burt, V., Hughes, J., Yetley, E., Dwyer, J. Picciano, M. F., McDowell,
M., & Sempos, C. (2011). Dietary supplement use among U.S. adults has increased since
NHANES III (1988–1994). NCHS Data Brief, No. 61. Retrieved from:
http://www.cdc.gov/nchs/data/databriefs/db61.pdf

48
Guilloux, J. P., Douillard-Guilloux, G., Kota, R., Wang, X., Gardier, A. M., Martinowich, K., . . .
Sibille, E. (2011). Molecular evidence for BDNF-and GABA-related dysfunctions in the
amygdala of female subjects with major depression. Molecular Psychiatry, 17(11), 1130-
1142.
Hansen, D. G., Vach, W., Rosholm, J-U., Søndergaard, J., Gram, L. F., & Kragstrup, J. (2004).
Early discontinuation of antidepressants in general practice: Association with patient and
prescriber characteristics. Family Practice, 21(6), 623-629.
Hintikka, J., Tolmunen, T., Tanskanen, A., & Viinamäki, H. (2003). High vitamin B12 level and
good treatment outcome may be associated in major depressive disorder. BMC
Psychiatry, 3(1), 17.
Hvas, A. M., Juul, S., Lauritzen, L., Nexø, E., & Ellegaard, J. (2004). No effect of vitamin B-12
treatment on cognitive function and depression: A randomized placebo controlled study.
Journal of Affective Disorders, 81(3), 269-273.
Hvas, A. M., Svend, J., Bech, P., & Nexø, E. (2004). Vitamin B6 level is associated with
symptoms of depression. Psychotherapy and Psychosomatics, 73, 340–343.
Huijts, M., Duits, A., Staals, J., & van Oostenbrugge, R. J. (2012). Association of vitamin B12
deficiency with fatigue and depression after lacunar stroke. Public Library of Science
One, 7(1), 1-3. doi:10.1371/journal.pone.0030519
Insel, T. (2011). Antidepressants: A complicated picture. The National Institute of Mental
Health, National Institutes of Health, U.S. Department of Health and Human Services.
Retrieved from http://www.nimh.nih.gov/about/director/2011/antidepressants-a-
complicated-picture.shtml

49
Kales, H. C., Blow, F. C., Welsh, D. E., & Mellow, A. M. (2004). Herbal products and other
supplements: Use by elderly veterans with depression and dementia and their caregivers.
Journal of Geriatric Psychiatry & Neurology, 17(1), 25-31.
Kate, N., Grover, S., & Agarwal, M. (2010). Does B12 deficiency lead to lack of treatment
response to conventional antidepressants? Psychiatry (Edgmont), 7(11), 42–44.
Keaton, D., Lamkin, N., Cassidy, K. A., Meyer, W. J., Ignacio, R. V., Aulakh, L., . . . Sajatovic,
M. (2009). Utilization of herbal and nutritional compounds among older adults with
bipolar disorder and with major depression. International Journal of Geriatric
Psychiatry, 24, 1087–1093.
Kikuchi, T., Uchida, H., Suzuki, T., Watanabe, K., & Kashima, H. (2011). Patients’ attitudes
toward side effects of antidepressants: An internet survey. European Archives of
Psychiatry and Clinical Neuroscience, 261, 103–109.
Kim, J. M., Stewart, R., Kim, S. W., Yang, S. J., Shin, I. S., & Yoon, J. S. (2008). Predictive
value of folate, vitamin B12 and homocysteine levels in late-life depression. The British
Journal of Psychiatry, 192(4), 268-274.
Koichi, M., Yixuan, S., Nay Chi, H., Akizumi, T., Hideki, H., Norito, K., . . . Takuro, S. (2012).
Folate intake and depressive symptoms in Japanese workers considering SES and job
stress factors: J-HOPE study. BMC Psychiatry, 12(1), 33-40. doi:10.1186/1471-244X-12-
33
Laverty, R. (1978). Catecholamines: Role in health and disease. Drugs, 16(5), 418-440.
Luhby, A. L., Brin, M., Gordon, M., Davis, P., Murphy, M., & Spiegel, H. (1971). Vitamin B6
metabolism in users of oral contraceptive agents. I. Abnormal urinary xanthurenic acid
excretion and its correction by pyridoxine. American Journal of Clinical Nutrition, 24,
684–693.

50
Mahan, L. K., Escott-Stump, S., Raymond, J. L., & Krause, M. V. (2012). Krause's food & the
nutrition care process (13th ed.). St. Louis, Mo.: Elsevier/Saunders.
Milanlioğlu, A. (2011). Vitamin B12 deficiency and depression. Journal of Clinical and
Experimental Investigations, 2(4), 455-456.
Miller, A. L. (2008). The methylation, neurotransmitter, and antioxidant connections between
folate and depression. Alternative Medicine Review, 13(3), 216-226.
Miyake, Y., Sasaki, S., Tanaka, K., Yokoyama, T., Ohya, Y., Fukushima, W., . . . Hirota, Y.
(2006). Dietary folate and vitamins B12, B6, and B2 intake and the risk of postpartum
depression in Japan: The Osaka Maternal and Child Health Study. Journal of Affective
Disorders, 96(1), 133-138.
Möhler, H. (2012). The GABA system in anxiety and depression and its therapeutic potential.
Neuropharmacology, 62(1), 42-53. doi: 10.1016/j.neuropharm.2011.08.040
Morris, D. W., Trivedi, M. H., & Rush, A. (2008). Folate and unipolar depression. Journal of
Alternative & Complementary Medicine, 14(3), 277-285. doi: 10.1089/acm.2007.0663
Mousseau, D. D., Raghavendra Rao, V. L., & Butterworth, R. F. (1996). Alterations in serotonin
parameters in brain of thiamin‐deficient rats are evident prior to the appearance of
neurological symptoms. Journal of Neurochemistry, 67(3), 1113-1123.
Murakami, K., Miyake, Y., Sasaki, S., Tanaka, K. & Arakawa, M. (2010). Dietary folate,
riboflavin, vitamin B-6, and vitamin B-12 and depressive symptoms in early adolescence:
The Ryukyus Child Health Study. Psychosomatic Medicine, 72(8), 763-8. doi:
10.1097/PSY.0b013e3181f02f15
Naghashpour, M., Amani, R., Nutr, R., Nematpour, S., & Haghighizadeh, M. H. (2011).
Riboflavin status and its association with serum hs-CRP levels among clinical nurses
with depression. Journal of the American College of Nutrition, 30(5), 340-7.

51
Ng, T. P., Feng, L., Niti, M., Kua, E. H., & Yap, K. B. (2009). Folate, vitamin B12,
homocysteine, and depressive symptoms in a population sample of older Chinese adults.
Journal of the American Geriatrics Society, 57(5), 871-876.
Nguyen, P. H., Grajeda, R., Melgar, P., Marcinkevage, J., DiGirolamo, A. M., Flores, R., &
Martorell, R. (2009). Micronutrient supplementation may reduce symptoms of depression
in Guatemalan women. Organo Oficial de la Sociedad Latinoamericana de Nutrición,
59(3), 278-286.
Nikseresht, S., Etebary, S., Karimian, M., Nabavizadeh, F., Zarrindast, M., & Sadeghipour, H.
(2012). Acute administration of Zn, Mg, and thiamin improves postpartum depression
conditions in mice. Archives of Iranian Medicine, 15(5), 306-311.
Okumura, Y., & Sakamoto, S. (2011). Statistical power and effect sizes of depression research in
Japan. Psychiatry and clinical neurosciences, 65(4), 356-364.
Onodera, K., Ogura, Y., & Kisara, K. (1981). Characteristics of muricide induced by thiamine
deficiency and its suppression by antidepressants or intraventricular serotonin.
Physiology & Behavior, 27(5), 847-853.
Papakostas, G. I., Petersen, T., Mischoulon, D., Ryan, J. L., Nierenberg, A. A., Bottiglieri, T.,
. . . Fava, M. (2004). Serum folate, vitamin B12, and homocysteine in major depressive
disorder, part 1: predictors of clinical response in fluoxetine-resistant depression. The
Journal of Clinical Psychiatry, 65(8), 1090-1095.
Paulose, C. S., Dakshinamurti, K., Packer, S., & Stephens, N. L. (1988). Sympathetic stimulation
and hypertension in the pyridoxine-deficient adult rat. Hypertension, 11(4), 387-391.

52
Payne, M. E., Jamerson, B. D., Potocky, C. F., Ashley-Koch, A. E., Speer, M. C., & Steffens, D.
C. (2009). Natural food folate and late-life depression. Journal of Nutrition for the
Elderly, 28(4), 348-358.
Penninx, B. W., Guralnik, J. M., Ferrucci, L., Fried, L. P., Allen, R. H., & Stabler, S. P. (2000).
Vitamin B12 deficiency and depression in physically disabled older women:
Epidemiologic evidence from the Women’s Health and Aging Study. American Journal
of Psychiatry, 157(5), 715-721.
Pepersack, T., Garbusinski, J., Robberecht, J., Beyer, I., Willems, D., & Fuss, M. (1999).
Clinical relevance of thiamine status amongst hospitalized elderly patients. Gerontology,
45(2), 96-101.
Plaitakis, A., Nicklas, W. J., & Berl, S. (1978). Thiamine deficiency selective impairment of the
cerebellar serotonergic system. Neurology, 28(7), 691-691.
Prousky, J. E. (2010). Vitamin B3 for depression: Case report and review of the literature.
Journal of Orthomolecular Medicine, 25(3), 137-147.
Radloff, L. S. (1977). The CES-D scale: A self-report depression scale for research in the general
population. Applied Psychological Measurement, 1(3), 385-401.
Rao, N. P., Kumar, N. C., Raman, B. R. P., Sivakumar, P. T., & Pandey, R. S. (2008). Role of
vitamin B12 in depressive disorder — a case report. General Hospital Psychiatry, 30,
185–186.
Reis, W. L., Saad, W. A., Camargo, L. A., Elias, L. L. K., & Antunes-Rodrigues, J. (2010).
Central nitrergic system regulation of neuroendocrine secretion, fluid intake and blood
pressure induced by angiotensin-II. Behavioral & Brain Functions, 6, 64-71. doi:
10.1186/1744-9081-6-64.

53
Rogers, E. (2003). Diffusion of innovations (5th ed.). New York, NY: The Free Press: Simon &
Schuster, Inc.
Sachdev, P. S., Parslow, R. A., Lux, R., Salonikas, C., Wen, W., Naidoo, D., Christensen, H., &
Jorm, A. F. (2005). Relationship of homocysteine, folic acid and vitamin B12 with
depression in a middle-aged community sample. Psychological Medicine, 35(4), 529-
538.
Sado, M., Knapp, M., Yamauchi, K., Fujisawa, D., So, M., Nakagawa, A., Kikuchi, T., & Ono,
Y. (2009). Cost-effectiveness of combination therapy versus antidepressant therapy for
management of depression in Japan. Australian & New Zealand Journal of Psychiatry,
43(6), 539-547.
Sánchez-Villegas, A., Doreste, J., Schlatter, J., Pla, J., Bes-Rastrollo, M., & Martínez-
González, M. A. (2009). Association between folate, vitamin B6 and vitamin B12 intake
and depression in the SUN cohort study. Journal of Human Nutrition and Dietetics, 22,
122–133.
Schatzkin, A., Kipnis, V., Carroll, R. J., Midthune, D., Subar, A. F., Bingham, S., . . . Freedman,
L. S. (2003). A comparison of a food frequency questionnaire with a 24-hour recall for
use in an epidemiological cohort study: Results from the biomarker-based Observing
Protein and Energy Nutrition (OPEN) study. International Journal of Epidemiology,
32(6), 1054-1062.
Silvers, K. M., Woolley, C. C., & Hedderley, D. (2006). Dietary supplement use in people being
treated for depression. Asia Pacific Journal of Clinical Nutrition, 15(1), 30-34.

54
Skarupski, K. A., Tangney, C., Li, H., Ouyang, B., Evans, D. A., & Morris, M. C. (2010).
Longitudinal association of vitamin B-6, folate, and vitamin B-12 with depressive
symptoms among older adults over time. American Journal of Clinical Nutrition, 92,
330-335.
Souery, D., Papakostas, G. I., & Trivedi, M. H. (2006). Treatment-resistant depression. Journal
of Clinical Psychiatry, 67, 16.
Tiemeier, H., Ruud van Tuijl, H., Hofman, A., Meijer, J., Kiliaan, A. J., & Breteler, M. M. B.
(2002). Vitamin B12, folate, and homocysteine in depression: The Rotterdam Study.
American Journal of Psychiatry, 159, 2099-2101.
Timbo, B. B., Ross, M. P., McCarthy, P. V., & Lin, C. T. (2006). Dietary supplements in a
national survey: Prevalence of use and reports of adverse events. Journal of the American
Dietetic Association, 106(12), 1966.
Tolmunen, T., Hintikka, J., Ruusunen, A., Voutilainen, S., Tanskanen, A., Valkonen, V. P., . . .
Salonen, J. T. (2004). Dietary folate and the risk of depression in Finnish middle-aged
men. Psychotherapy and Psychosomatics, 73(6), 334-339.
Walsh, B. T., Seidman, S. N., Sysko, R., & Gould, M. (2002). Placebo response in studies of
major depression. Journal of the American Medical Association, 287(14), 1840-1847.
Williams, A-L., Cotter, A., Sabina, A., Girard, C., Goodman, J. & Katz, D. L. (2005). The role
for vitamin B-6 as treatment for depression: A systematic review. Family Practice, 22,
532–537.
Wilson, C. J. (2007). When and how do young people seek professional help for mental health
problems?. The Medical Journal of Australia, 187(Supplement), S35-S39.

55
Wilson, S., Bivins, B., Russell, K., & Bailey, L. (2011). Oral contraceptive use: Impact on folate,
vitamin B6, and vitamin B12 status. Nutrition Reviews, 69(10), 572-583. doi:
10.1111/j.1753-4887.2011.00419.x
Young, S. N. (2007). Folate and depression—a neglected problem. Journal of Psychiatry &
Neuroscience, 32(2), 80.
Zhang, G., Ding, H., Chen, H., Ye, X., Li, H., Lin, X., & Ke, Z. (2013). Thiamine nutritional
status and depressive symptoms are inversely associated among older Chinese adults. The
Journal of Nutrition, 143(1), 53-58.
Zhao, G., Ford, E. S., Li, C., Greenlund, K. J., Croft, J. B., & Balluz, L. S. (2011). Use of folic
acid and vitamin supplementation among adults with depression and anxiety: A cross-
sectional, population-based survey. Nutrition Journal, 10, 102.

56
Appendix A December 6, 2012 Melissa Klemp Psychology UW-Stout RE: “B Vitamin Supplementation in Treating Depression” Dear Melissa, In accordance with Federal Regulations, your project, “B Vitamin Supplementation in Treating Depression” was reviewed on 12/5/2012, by a member of the Institutional Review Board and was approved under Expedited Review through 12/4/2013. If your project involves administration of a survey or interview, please copy and paste the following message to the top of your survey/interview form before dissemination: If you are conducting an online survey/interview, please copy and paste the following message to the top of the form: “This research has been approved by the UW-Stout IRB as required by the Code of Federal regulations Title 45 Part 46.” Responsibilities for Principal Investigators of IRB-approved research:
1. No subjects may be involved in any study procedure prior to the IRB approval date or after the expiration date. (Principal Investigators and Sponsors are responsible for initiating Continuing Review proceedings.)
2. All unanticipated or serious adverse events must be reported to the IRB. 3. All protocol modifications must be IRB approved prior to implementation, unless they are
intended to reduce risk. 4. All protocol deviations must be reported to the IRB. 5. All recruitment materials and methods must be approved by the IRB prior to being used. 6. Federal regulations require IRB review of ongoing projects on an annual basis.
Thank you for your cooperation with the IRB and best wishes with your project. Should you have any questions regarding this letter or need further assistance, please contact the IRB office at 715-232-1126 or email [email protected]. Sincerely,
Susan Foxwell Research Administrator and Human Protections Administrator, UW-Stout Institutional Review Board for the Protection of Human Subjects in Research (IRB)

57
Appendix B
Do I qualify for the B vitamin study?
You do not have to be diagnosed with depression by a health care practitioner to
participate in this study.
You MUST be :
At least 18 yrs old
Experiencing symptoms of depression
It’s OK to be on medications or to have used medications
Able to read and understand the English language
You must NOT:
Be pregnant or nursing
Currently take B vitamin supplements
Have a medical condition that prevents B vitamin supplement usage
Currently take a medication that prevents B vitamin supplement usage
Have been diagnosed with a mental illness other than depression
Have been hospitalized for a mental illness including depression within the
last 10 years.
Depressive symptoms may vary for different people, but often include the
following:
Diminished interest in activities which used to be pleasurable
Weight gain or loss
Physical agitation or restlessness
Slowing of physical or mental activity; fatigue
Inappropriate guilt
Difficulties concentrating
Recurrent thoughts of death

58
Appendix C
Consent to Participate In UW-Stout Approved Research
Title: B Vitamin Supplementation in Treating Depression
Research Sponsor: Suejung Han, Ph.D. [email protected] 715-232-2645
Investigator: Melissa Klemp, BA [email protected] 920-737-1561
Description: The purpose of this study is to assess if B vitamin supplementation decreases symptoms of depression in people. The purpose is also to assess if B vitmain supplementation decreases symptoms of depression in people who take antidepressants yet still experience symptoms of depression. As a participant, you will be asked to orally consume one vitamin B complex tablet per day, for 28 days. On the day you pick up your supplements, you will fill out a questionnaire, and your height and weight will be taken. After 28 days, you will return to take a final questionairre. We ask that you write down everything you ate and drank for a 24 hour period the day before you receive the tablets, and again the day before the final questionnaire. Risks and Benefits: There are no more risks involved in this study than those ordinarily encountered in daily life. A potential benefit is that you may experience a reduction in depressive symptoms. Your participation benefits society by offering more information about using B vitamin supplementation in treating depression. Time Commitment and Incentive: The trial begins February 7, 2013 and ends March 8, 2013. You will meet with the researcher approximately 20 minutes at the start of the trial, and approximately 10 minutes at the end of the trial. A $50 Wal-Mart gift card will be given at the end of the trial to two participants whose names will be randomly drawn. Confidentiality: Your name will not be included on any documents. This informed consent will not be kept with any of the other documents completed with this project. We do not believe that you can be identified from any of this information. Your information will be assigned a code number that is unique to this study. The list connecting your name to this number will be kept in a locked file and only the researcher and Research Sponsor will be able to access it. When the study is completed and the data have been analyzed, the list linking participants’ names to study numbers will be destroyed. Study findings will be presented only in summary form and your name would not be used in any report. Right to Withdraw: Your participation in this study is entirely voluntary. You may choose not to participate without any adverse consequences to you. Should you choose to participate and later wish to withdraw

59
from the study, you may discontinue your participation at this time without incurring adverse consequences. IRB Approval: This study has been reviewed and approved by The University of Wisconsin-Stout's Institutional Review Board (IRB). The IRB has determined that this study meets the ethical obligations required by federal law and University policies. If you have questions or concerns regarding this study please contact the Investigator or Advisor. If you have any questions, concerns, or reports regarding your rights as a research subject, please contact the IRB Administrator. Investigator: Melissa Klemp Phone: 920-737-1561 E-mail: [email protected]
IRB Administrator Sue Foxwell, Director, Research Services 152 Vocational Rehabilitation Bldg. UW-Stout Menomonie, WI 54751 715.232.2477 [email protected]
Advisor: Suejung Han, Ph.D. Phone: 715-232-2645 E-mail: [email protected] Statement of Consent: By signing this consent form you agree to participate in the project entitled, “B Vitamin Supplementation in Treating Depression.” _________________________________________________ Signature Date

60
Appendix D
Baseline Questionnaire
Q1 Enter your participant ID number: Q2 I was bothered by things that usually don’t bother me. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q3 I did not feel like eating; my appetite was poor. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q4 I felt that I could not shake off the blues even with help from my family or friends. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q5 I felt that I was just as good as other people. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q6 I had trouble keeping my mind on what I was doing. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q7 I felt depressed. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q8 I felt that everything I did was an effort. Rarely or none of the time (less than 1 day)

61
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q9 I felt hopeful about the future. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q10 I thought my life had been a failure. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q11 I felt fearful. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q12 My sleep was restless. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q13 I was happy. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q14 I talked less than usual. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q15 I felt lonely. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)

62
Most or all of the time (5-7 days)
Q16 People were unfriendly. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q17 I enjoyed life. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q18 I had crying spells. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q19 I felt sad. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q20 I felt that people dislike me. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q21 I could not get “going.” Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q22 How old are you?

63
Q23 Do you currently take any medications to treat depression? Yes
No
Q23a If so, please list which depression medications: Q24 How frequently do you drink alcohol? Almost every day
5 or 6 days a week
3 or 4 days a week
Once or twice a week
Once or twice a month
Less than once a month
Q25 Do you smoke? Yes
No
Q26 Your gender is: Male
Female

64
Appendix E
Post-intervention Questionnaire
Q1 Enter your participant ID number: Q2 I was bothered by things that usually don’t bother me. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q3 I did not feel like eating; my appetite was poor. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q4 I felt that I could not shake off the blues even with help from my family or friends. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q5 I felt that I was just as good as other people. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q6 I had trouble keeping my mind on what I was doing. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q7 I felt depressed. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q8 I felt that everything I did was an effort. Rarely or none of the time (less than 1 day)

65
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q9 I felt hopeful about the future. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q10 I thought my life had been a failure. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q11 I felt fearful. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q12 My sleep was restless. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q13 I was happy. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q14 I talked less than usual. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q15 I felt lonely. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)

66
Most or all of the time (5-7 days)
Q16 People were unfriendly. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q17 I enjoyed life. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q18 I had crying spells. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q19 I felt sad. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q20 I felt that people dislike me. Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q21 I could not get “going.” Rarely or none of the time (less than 1 day)
Some or a little of the time (1-2 days)
Occasionally or a moderate amount of time (3-4 days)
Most or all of the time (5-7 days)
Q22 Did you notice any positive effects from the B vitamins? Yes
No
Q22a What positive effects did you notice?

67
Q23 Did you notice any negative effects from the B vitamins? Yes
No
Q23a What negative effects did you notice? Q24 If you have other comments, write them here. Q25 How many B vitamins do you have left?

68
Appendix F
Subject # _______________
24-Hour Diet Recall
Please be as specific as possible. Include all beverages, condiments, and portion sizes. An example has been filled in.
Time/Meal Food Item and Method of Preparation Amount Eaten
Breakfast Kashi Blackberry Hills Cereal 1 cup Milk 1 cup Banana, medium 1 whole

69
Appendix G
B vitamin supplement used in study
Contents of Glycogenics®
Ingredient Amount Per Tablet % Daily Value
Vitamin C (as ascorbic acid) 125 mg 208%
Thiamin (as thiamin mononitrate) 14 mg 933%
Riboflavin 16 mg 941%
Niacin (as niacinamide and niacin) 200 mg 1000%
Vitamin B6 (as pyridoxine HCl) 22 mg 1100%
Folate (as folic acid and L-5-
methyltetrahydrofolate) 400 mcg 100%
Vitamin B12 (as cyanocobalamin) 250 mcg 4167%
Biotin 250 mcg 83%
Pantothenic Acid (as D-calcium pantothenate) 75 mg 750%
Choline (as choline bitartrate) 100 mg *
Inositol 94 mg *
para-Aminobenzoic Acid (PABA) 15 mg *
Note: *Daily Value not established.

70
Appendix H
Participant Study Instructions
B vitamin supplementation in treating depression trial
Instructions
Starting tomorrow morning, take one capsule daily, for 28 days. You may take it
with or without food.
If you forget to take it in the morning, you may take it later in the day or before
bed.
If you don’t remember to take the capsule at all one day, start again the next
morning with just one. You will return any unused capsules at your next and
final appointment time.
Please store capsules away from heat and light. (Keeping them in the paper bag
is sufficient to prevent light).
One more 24 hour food intake is needed from you. Attached is a form for you to
fill in on a day convenient for you and bring to your appointment. If you do not
bring this to your appointment, we will do a 24 hour food recall with you at that
time.
Your appoint time is ____________________________________ Your participant number is _______________________