Embed Size (px)
Citation preview

1
Assistant-prof. V.Voloshyn
According:prof. Bodnar Ya.Ya.; prof. Sorokina I.V.; Frank Netter1

2
Haemoblastoses - there are the tumours of lymphoid and myeloid tissue
Haemoblastoses include leucosis and lymphadenomas
Leucosis (leukaemia) There is the system tumour disease of haemopoetic tissue with the obligatory defeat of red marrow and supplanting (substitution) of normal blood shoot.
Lymphadenomas – regional tumours of haemopoetic and/or lymphoid tissue.
2

3
3
Epidemiology. Hemoblastoses take 5 seat among all tumours of peoples. The 30% of all Haemoblastoses are formed by children to 5 years age.
Etiology. According to modern opinion leucosis arise up on mutational genetic basis. The question is about the specific mutations of haemopoetic cells, which lead to genes superactivating, that in a norm is responsible for their proliferation and differentiation. These genes obtained the name "prooncogenes” or cellular oncogenes, and is inalienable part of cellular genome, but at the same time have the hidden blastomogenic potencies. Surplus expression of them causes degeneration of marrow cells in leukemic.

4
Classification:
4
A) acute leucosis B) chronic leucosis:
undifferentiated Myelocyte orygin: myelocyticmyeloidalerytromyelosiserytraemia
true policytaemia (Vaquez-Osler's syndrome)
myeloblastic
lymphoblastic
plasmoblastic
monoblastic
erythroblastic Lymphocyte orygin: lympho-leukosis, skin lymphomatosis of Sezary paratroteinaemic:
a) myelomic diseasesb) primary macroglobulinaemia (Waldenstrom ) c) heavy chain (of Franklin)
megakarioblastic Monocyte orygin: a) monocyte leukosis b) hystiocytosis
I) Leucosis

5
Diagram of haemopoesis
5

6
1) lympho sarcoma: lymphocyte, prolymphocyte, lymphoblast, immunoblast, lymphoplasmocyte, African lymphoma (Burkitt's);
2) mycosis fungoides;3) Sezary's disease;4) reticulosarcoma;5) lymphogranulomatosis (Hodgkin's disease).
Classification: (continuation I)
II) Lymphomas — regional tumors:
6

7
Classification: (continuation III)
leukemic (tens and hundreds thousand leukosis cells per 1 microl);
subleukemic (not more that 15.000 — 25.000 per 1 microl);
leukopenic (leukocyte count is reduced but leukosis cells can be found);
aleukemic (leukosiscells in the blood are absent).
7

8
PATHOMORPHOLOGICAL SYNDROMES:
Pyoid bone marrow due to proliferation of the tumor cells (mature or immature, respectively) in the bone marrow with displacement of the red sprout. Macroscopically, bone marrow is grayish-whitish.
Leukoses infiltration of hemopoietic organs (bone marrow, spleen, lymphatic glands) at first, then of the other organs (mucous membranes, myocardium, kidneys, brain, etc., vessels).
The displacement of the red sprout of the bone marrow causes anemia.
Severe hemorrhagic syndrome in combination with anemia and destruction of the vascular walls with leukoses infiltration develop as a manifestation of thrombocytes formation in the bone marrow.
Necrotic tonsillitis, gingivitis develop due to leukoses infiltration of the oral mucosa and tonsils against the background of immunogenesis inhibition.
Secondary infection often accompanies the process, sepsis may develop.
Foci of extramedullary hemopoiesis develop in the liver, spleen, kidneys, lymphatic glands as compensatory adaptation reaction directed to restoration of the red sprout.
8

9
The acute undifferentiated leucosis
Leukemic infiltration of marrow, spleen, lymphonoduses, lymphoid follicles, vessels walls.
Necrotizing quinsy. Hemorragic syndrome
9

10
CLASSIFICATION IN SUBTYPES OF ACUTE MYELOPROLIFERATIVE DISEASES
FABClass
Subtype Name Abbreviation Proportion of Acute Myeloproliferative Diseases (%)
MO Acute myeloblasts leukemia, stem cell (i.e., minimal differentiation)
AML 3-5
M1 Acute myeloblasts leukemia without maturation
AML 15-20
M2 Acute myeloblasts leukemia with maturation
AML 25-30
M3 Acute promyelocytic leukemia APL 5-20
M4 Acute myelomonocytic leukemia AMML 20-30
M5 Acute monoblastic leukemia AMOL 2-9
M6 Acute erythroleukemia AEL 3-5
M7 Acute megakaryoblastic leukemia 3-12
10

11
Acute myeloblastic leucosis
Leukemic infiltration by the blastic cells of marrow, spleen, liver, kidneys, rarer lymphatic nodes.
Infiltration of mucuses and serosal membranes by the blastic cells: leukemic meningitis, leukemic pneumonitis, leukemic gastritis.
Hemorragic diathesis, bleeding, ulcerous-necrotic complications, sepsis.
11

12
Acute myelogenous leukemia
Leukemic infiltration of kidneys, Leukemic infiltration in bone marrow and spleen
12Skin infiltration

13
Acute Myelogenous Leukemia
Bone marrow biopsy specimen acute myelogenous leukemia (AML-M1). Diffuse immature myeloid hyperplasia with early maturation (chlorocetate esterase Stain; red cells = myeloid differentiation; AML-MO would show similar picture without red cells)
13
Blood smear of acute myelogenous leukemia (AML-M1)Immature myeloblasts, partly with
lymphoid appearance

14
Lymphoblastic leucosis
Lymphoblasts infiltration of marrow, lymphatic nodes, thymus gland, spleen, intestine, kidneys
Thymomegaly Spleenomegaly
14

15
Acute megakaryoblastic leukemia
15

16
Acute erythroblastic leukemia
16
Acute erythroblastic leukemia (AML-M6). Blood smear with immature erythroblastic cells (arrows)

17
Complications and causes of death
hemorrhage to vital organs (brain); ulcerative necrotic and septic
complications (sepsis).
17

18
DISTINCTIVE FEATURES OF ACUTE AND CHRONIC LEUKAEMIAS
Bone marrow and blood picture (In acute leukoses the blasts are observed, in chronic leukoses the mature cells are found).
Leukemic failure (hiatus leucemicus) characterizes acute leukoses. It is sharp increase of blast count and single mature elements while transitional forms are absent.
Sharp enlargement of the spleen, liver, kidneys and lymphatic glands characterizes chronic leukoses while in chronic leukoses it is less marked. The spleen can weigh 6—8 kg, the liver 5—6 kg.
18

19
19

20
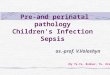
Chronic myelosis
Blastic crises Pyoid marrow. Gray-red blood. Hepatomegalia. Spleenomegaly Myelocytes
infiltration of lymphoid organs.
20

21
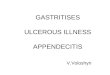
Chronic Myelogenous Leukemia
Blood smear. Showing increased number of metamyelocytes and myelocytes (arrow)
21
Blood marrow smear. Mild increase in myelocytes and myeloblasts and decreased erythropoiesis (arrows)

22
Chronic Myelogenous Leukemia
22
a)Myelomonocytic variant of chronic myelogenous leukemia (CMoML). Immature monocytoid cells (arrow)
b) Bone marrow smear of CMoML. Increased number of monocytoid cells (neutral anaphthyl esterase reaction for monocytes): brown cells (arrow)

23
Chronic lympholeucosis
Leukemic infiltrates takes place in marrow, lymphatic nodes, spleen and liver
Blastic crises are possible
Marrow is red Spleenomegaly A liver and kidneys are
increased Hemorrhages Pneumonias 23

24
Paraproteinaemic leucosis. Myeloma (1.2.b.2.a)
24

25
25

26
26

27
myelomas (chronic, lymphocyte, paraproteinemic group)
1) plasmocyte,2) plasmoblast,3) polymorphocellular,4) small-cell.
27
1) diffuse,2) diffuse nodular,3) multiple nodular.
Morphological forms:

28
Lymphadenomas
Regional tumours diseases of haemopoetic and lymphatic tissue.
Lymphomas include lymphosarcoma,
Sezary's illness, Hodgkin's illness
28

29
Lymphosarcoma
29

30
non-Hodgkin lymphoma (NHL).
Lymphoplasmacytoid non-Hodgkin lymphoma (NHL). Showing a mixture of lymphocytes, plasmacytoid cells and occasional immunoblast (arrow; Giemsa stain)
Follicular non-Hodgkin lymphoma (FCC) (follicular center cell lymphoma). Showing nodular, partly follicular, structure with a mixed small and large cell population (Giemsa stain)
30

31
Follicular center cell lymphoma. With predominant large cells. The follicular may be still discernable or completely lost (H& E stain)
Large cell immunoblastic non-Hodgkin lymphoma. Showing predominance of immunoblasts (arrow) with some plasmacytoid features (PAS stain)
non-Hodgkin lymphoma
31

32
Non-Hodgkin lymphoma
32
Infiltration of maxilla (Burkitt)
Burkitt-type non-Hodgkin lymphoma (here classical Burkitt lymphoma). Showing densely packed lymphoblasts with scattered histiocytes containing nuclear debris (starry sky pattern; arrow)

33
Infiltration of femur marrow (immunoblastic)
Non-Hodgkin lymphoma
33

34
Non-Hodgkin lymphoma
34 Non-Hodgkin Lymphomas, Gross View
Non-Hodgkin lymphoma. Infiltration of stomach (immunoblastic). Non-Hodgkin lymphoma. Infiltration of spleen (follicular)

35
CLINICO-MORPHOLOGICAL CLASSIFICATION
35
variant 1: with prevail of lymphoid tissue (lymphohistiocyte);variant 2: nodular sclerosisvariant 3: mixed-cell;variant 4: with inhibition of lymphoid tissue.
HODGKIN'S DISEASE (HD)

36
Lymphogranulomatosis (Hodgkin's)
36

37
HD
37
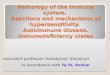
HODGKIN'S DISEASE HODGKIN'S DISEASE
Gross infiltration of spleen in Hodgkin disease (HD)
Gross infiltration of spine in Hodgkin disease (HD)

38
HD
38
HODGKIN'S DISEASE HODGKIN'S DISEASE
Lymphocyte-predominant type of Hodgkin disease. With only occasional Hodgkin and Reed-
Sternberg cells (arrows)(HD)
Mixed cellularity type of Hodgkin disease. With mixed population of lymphocytes, histiocytes (which may show epithelioid features), eosinophils, Hodgkin and Reed-Sternberg cells (arrows)

39
HD
39
Nodular sclerosis type (C1) of Hodgkin disease. With paracortical atrophy, fibrosis, and typical lacunar-type Hodgkin and Reed-Sternberg cells (arrow)
Lymphocyte-depleted type of Hodgkin disease.
Showing predominance of atypical histiocytoblasts with many Hodgkin and
Reed-Sternberg cells (arrows)

40
Thank you for attention!
40