Embed Size (px)
Citation preview

1AFRO Measles TAG – Nairobi 2-3 June 2015
MCV2 Introduction and the Second Year
of Life Contact
Lessons and way forward
Raoul KAMADJEUUNICEF ESARO
Meeting of the WHO AFRO Measles and Rubella Technical Advisory Group 2-3 June 2015, Nairobi (Kenya)

2AFRO Measles TAG – Nairobi 2-3 June 2015
Outline
1. Background on MCV2 2. MCV2 introduction into EPI - Status
update3. MCV2 performance4. Challenges o MCV2 introduction:
findings of MCV2 PIEs 5. Improving MCV2 coverage and way
forward6. Conclusion and questions to the TAG

3AFRO Measles TAG – Nairobi 2-3 June 2015
MCV2 - Background

4AFRO Measles TAG – Nairobi 2-3 June 2015
Measles and Rubella Elimination Goalsby WHO Region
2015 2015
20152012
20202020
2000 2010

5AFRO Measles TAG – Nairobi 2-3 June 2015
a major strategic approach to maintain high quality population immunity*
*Measles Elimination By 2020: A Strategy For The African Region - AFR/RC61/8 16 June 2011 (WHO AFRO)
“…The introduction of a second dose of measles immunization in RI in eligible countries”

6AFRO Measles TAG – Nairobi 2-3 June 2015
AFRO Measles TAG position on MCV2*TAG suggested criteria for MCV2 introduction:
‒ Achievement of MCV1 coverage >80%, maintained for at least three consecutive years using WHO/UNICEF best estimates of vaccine coverage; and
‒ Attainment of one of the two primary measles surveillance performance indicators for at least two consecutive years.”
*Report of the Second Meeting of the African Regional Measles Technical Advisory Group (TAG) – Recommendations (2008)

7AFRO Measles TAG – Nairobi 2-3 June 2015
WHO recommendation on MCV2 *
• All children should receive two doses of measles vaccine
• Minimum interval of one month between doses• MCV1 at 9 or 12 months• When MCV1 > 80% for 3 years then add MCV2 at:
‒ 15-18 months (if country has ongoing measles transmission)‒ school entry (option if near elimination)
• Very high coverage (>90%) needed with both doses‒ Mortality reduction: >90% national, >80% in every district‒ Elimination: >95% in every district
• School entry screening for vaccination status
*WHO Measles Vaccine Position Paper, WER Aug 2009 (http://www.who.int/wer/2009/wer8435.pdf)

8AFRO Measles TAG – Nairobi 2-3 June 2015
MCV2 introduction into EPI
AFRO Status update

9AFRO Measles TAG – Nairobi 2-3 June 2015
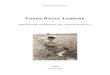
AFRO countries MCV2 status*
Introduced to date (19 Countries)
Planned introductions by end 2015 (5 Countries)
No introduction planned by 2015 (27)
Not applicable (Not AFRO)
• MCV2 as of May 2015: 19 countries (40%)
• MCV2 planned by end 2015: 5 (10%)
By the end of 2015, 24 countries (51% of AFRO countries) would have introduced MCV2 into their RI schedule
*As of May 205

10AFRO Measles TAG – Nairobi 2-3 June 2015
MCV2 introduction – MCV1 pre-introduction
All the countries introducing MCV2 have fulfilled the criteria of national MCV1 coverage ≥80% for 3 consecutive years and have sustained high MCV1 in the years preceding MCV2 introduction.
Country 2014 2013 2012 2011 2010 2009 2008 2007 2006
Botswana 94 94 94 94 94 94 94 94
Burkina Faso 82 87 89 92 94 94 94 88
Burundi 98 93 93 92 91 84 88 92
Capo Verde 91 91 96 97 97 96 95 94
Eritrea 96 98 99 99 99 97 97 95
Gambia 96 95 91 92 96 92 88 89
Kenya 93 93 87 86 88 90 80 77
Rwanda 97 97 97 95
Ghana 88 91 93 93 86 95 85
Sao Tome 91 92 91 92
Senegal 84 83 84 81 79 77 84 80
Tanzania 99 97 93 92 91 88 90 93
Zambia 80 82 83 96 90 87 93 85
MCV2 year of introduction MCV1 coverage 3 years pre-introduction
Data source: Official country reported coverage estimates – Access in May 2015

11AFRO Measles TAG – Nairobi 2-3 June 2015
MCV2 introduction – status update
• 10 out of the 19 countries (52%) have introduced MVC2 with GAVI support. • A PIE was conducted in 5 countries with MCV2 introduction date > 2012• MCV2 is in most cases provided at 18 months of age. Few exceptions to this rules are
Senegal and Seychelles. • Three countries are providing MR as MCV2 while 4 countries are providing MMR
CountriesYear of
introduction Vaccine for MCV2 visit Age of administrationSupport for introduction PIE (Year)
1 Algeria 2000 M (MMR from 2015)6 years (18 months from 2015) with MMR1 at 11
months SELF 2 Lesotho 2000 M 18 months SELF 3 Seychelles 2000 MMR 6 yrs (MCV1 at 15 months) SELF 4 South Africa 2000 M/MMR 12-15-18 months SELF 5 Swaziland 2002 M 18 months SELF 6 Mauritius 2003 M 18 months SELF 7 Capo Verde 2009 MMR 18 months SELF 8 Eritrea 2012 M 18 months +GAVI 20159 Gambia 2012 M 18 months +GAVI
10 Ghana 2012 M 18 months +GAVI 201311 Botswana 2013 M 18 months +GAVI 12 Burundi 2013 M 18 months +GAVI 201413 Kenya 2013 M 18 months SELF 201514 Sao Tome 2013 MR 18 months +GAVI 15 Zambia 2013 M 18 months +GAVI 201416 Burkina Faso 2014 M 18 months +GAVI 17 Rwanda 2014 M 12 months +GAVI 18 Senegal 2014 MR 15 months +GAVI 19 Tanzania 2014 MR 18 months +GAVI

12AFRO Measles TAG – Nairobi 2-3 June 2015
MCV2 performance

13AFRO Measles TAG – Nairobi 2-3 June 2015
MCV2 performance
*Data source: Official country reported coverage estimates – Access in May 2015** Not yet officially reported by the country
MCV2 > 80% MCV2 60 - 80% MCV2 < 60% No data Country Year of MCV2 introduction MCV2 20141 Algeria 2000 1002 Lesotho 2000 543 Seychelles 2000 984 South Africa 2000 815 Swaziland 2002 896 Mauritius 2003 857 Capo Verde 2009 798 Eritrea 2012 69**9 Gambia 2012 73
10 Ghana 2012 6711 Botswana 2013 8512 Burundi 2013 6013 Kenya 2013 25**14 Sao Tome 2013 7115 Burkina Faso 2014 16 Rwanda 2014 7717 Senegal 2014 1318 Tanzania 2014 4419 Zambia 2014 33
MCV2 coverage < 80%: 12 including 5 with MCV2<60%

14AFRO Measles TAG – Nairobi 2-3 June 2015
ALG BWA BFA BDI CPV ERI GAM GHA KEN LSO MUS SEN SYC SWZ ZAF TZN ZMB RWA0
10
20
30
40
50
60
70
80
90
100
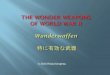
Year 3 Year 2 Year 1
MCV2 performance in early introduction*
*Data source: Official country reported coverage estimates – Access in May 2015
80%
MCV2 coverage at Year 1, Year 2 and Year 3 post introduction

15AFRO Measles TAG – Nairobi 2-3 June 2015
DZA (2000)
SYC (2000)
BWA (2013)
LSO (2000)
SWZ (2002)
ZAF (2000)
MUS (2003)
CPV (2009)
RWA (2014)
STP (2013)
ERI (2012)
GMB (2012)
GHA (2012)
BDI (2013)
TZA (2014)
ZMB (2013)
KEN (2013)
SEN (2014)
-10% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
MCV1 - MCV2 dropout rate 2014*
*Data source: WHO/UNICEF reported National Immunization Coverage 2014
Drop out rate (%)
20%

16AFRO Measles TAG – Nairobi 2-3 June 2015
MCV2 coverage trend in “early introducers” (2004 to 2013)
201320122011201020092008200720062005200430
40
50
60
70
80
90
100
ZAF
LSO
MUS
DZA
SWZ
SYC
Some countries were able to achieve and maintain high coverage early in MCV2 introduction

17AFRO Measles TAG – Nairobi 2-3 June 2015
Challenges to MCV2 introduction and uptake
Key summary findings of PIEs

18AFRO Measles TAG – Nairobi 2-3 June 2015
MCV2 Post Introduction EvaluationsPurpose• to evaluate the impact of introduction on
country’s immunization program• To rapidly identify problems needing correction
PIE to be conducted 6 – 12 months following the introduction (WHO Recommendation)
Assessment conducted at all levels of the health system by a team of experts (national and internationals) using adapted tools

19AFRO Measles TAG – Nairobi 2-3 June 2015
PIE – programmatic areas assessed
Planning and
process
Advocacy,
comm, soc mob
Training and
Knowledge of HCW
Service delivery
, recordin
g, reportin
g
Monitoring and supervi
s.
Cold chain,
vaccine mgt and logistic
Sustain. and
finance
Injection safety
and waste
disposal
Monitoring of AEFI

20AFRO Measles TAG – Nairobi 2-3 June 2015
MCV2 PIEs implementation statusYear Done Planned2013 • Ghana (MCV2, PCV, RV) (August, 19 months
after introduction)2014 • Burundi (MCV2, RV) (June, 17 months after
introduction)• Zambia (MCV, PCV, RV – combined with EPI
and in-depth surveillance review) (July, 12 months after introduction)
2015 • Eritrea (MCV2, RV) (Feb, 31 months after introduction)
• Kenya (MCV2, RV) (May, 22 months after introduction)
• Senegal• Gambia• Tanzania

21AFRO Measles TAG – Nairobi 2-3 June 2015
MCV2 PIEs Key findingsProgrammatic areas
Key findings
Service delivery, integration, reducing missed opportunities
• Strategies to reach children > 9 months not planned• Strategies for vaccination in second year of life not
established• Opportunities to link MCV2 with other child health
activities >1 year not fully explored• Strategies for defaulters tracing not in place• Lack of clarity when zero-dose children come in for
MCV2.• Knowledge of HCW sub-optimal (training for MCV2 not
given sufficient attention since it is “an old vaccine”)

22AFRO Measles TAG – Nairobi 2-3 June 2015
MCV2 PIEs Key findingsProgrammatic areas
Key findings
Demand creation
• Provision of immunization service > 1 year new to care takers
• Sub-optimal knowledge of EPI clients on MCV2 and immunization activities > 1 year
• Demand creation activities limited• Opportunities to increase demand creation exist
but are not fully harnessed (health education during EPI sessions/antenatal visits, health visits, mass media, etc..)

23AFRO Measles TAG – Nairobi 2-3 June 2015
MCV2 PIEs Key findingsProgrammatic areas
Key findings
Monitoring of doses/coverage/dropout
• Unstable population figures• Target population for MCV2 new to the program and
not widely understood• Recording of MCV doses still a challenge• Monitoring of MCV2 not fully established
‒ Poor recording of MCV2 doses‒ Monitoring of MCV2 at all levels not established‒ High MCV1-MCV2 dropout rates observed
(reflecting low MCV2 coverage) but not monitored ‒ Impact of MCV2 introduction on vaccine
utilization/wastage is not systematically monitored

24AFRO Measles TAG – Nairobi 2-3 June 2015
Improving MCV2 coverage
Way forward

25AFRO Measles TAG – Nairobi 2-3 June 2015
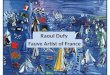
Modeling MCV2 impact – Theoretical model
• Changes in susceptible population by level of MCV2 coverage in a theoretical population with a birth cohort of 500,000, assuming MCV1 coverage 80% at 9 months maintained over time.
• At coverage 70%, 80% and 90% it will take 9, 13 and 22 years respectively for the population of susceptible to accumulate above the birth cohort
Y1 Y2 Y3 Y4 Y5 Y6 Y7 Y80
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
900,000
1,000,000
1,100,000
1,200,000
1,300,000
1,400,000
No MCV2MCV1 = 80%Assumed constant over years
MCV2 = 50%
MCV2 = 40%
MCV2 = 70%
MCV2 = 80%
MCV2 = 60%
MCV2 = 90%
Birth cohort
MCV SIAs
Susceptible accumulated above birth cohort – Recommended time for measles SIA

26AFRO Measles TAG – Nairobi 2-3 June 2015
Way forward to improve MCV2 performance
1. Institution of a pre-MCV2 introduction readiness assessment/planning tool developed by WHO/UNICEF?
2. WHO-AFRO to institute reporting on dropout between MCV1 and MCV2 as key performance indicator (to be reported in feedback bulletin and included in monitoring charts ) for countries with MCV2
3. WHO and UNICEF to conduct additional operational research on strategies/best practices to improve MCV2 coverage around: service delivery, demand creation and integration with 2nd year of life activities

27AFRO Measles TAG – Nairobi 2-3 June 2015
Way forward to improve MCV2 performance
4. Sharing lessons learned and best practice from other countries to inform MCV2 introduction and performance
5. Changing EPI target age from the historic 9 months (0-11 months) to under 2 or under 5 years
6. Monitoring the implementation of PIEs recommendations

28AFRO Measles TAG – Nairobi 2-3 June 2015
Conclusion and questions to the TAG

29AFRO Measles TAG – Nairobi 2-3 June 2015
Conclusion• 19 countries in WHO/AFRO Region (40%) have
introduced MCV2 into their RI schedule, with more countries planning to introduce MCV2 in the near future
• Concerns remain over low performance of MCV2 and appropriate actions should be taken to improve MCV2 performance
• Not all countries have exploited MCV2 introduction to make policy and practice changes to increase MCV1 and MCV2 coverage

30AFRO Measles TAG – Nairobi 2-3 June 2015
Questions to the TAG on MCV21. Is it time the TAG revisit its MCV2 introduction
criteria that were set in 2008 (coverage criteria, surveillance criteria)?
2. Should WHO institutes a pre-introduction assessment (6, 8 months prior to MCV2 introduction?)
3. Should AFRO countries institute universal school entry MCV checks and referral when there is not evidence of 2 doses of MCV?

31AFRO Measles TAG – Nairobi 2-3 June 2015
Thank you