Embed Size (px)
Citation preview

JSM Dentistry
Cite this article: Goldberg M (2019) 1-2- Pediatric Dental Development Pulp Biology, Defense Cells and Inflammation. JSM Dent 7(1): 1118.
Central
*Corresponding authorMichel Goldberg, Professor Emeritus. Paris Cité University, Department of Oral Biology, Faculty of Fundamental and Biomedical Sciences, INSERM UMR-S 1124. 45 rue des Saints Pères 75006, Paris, France, Tel : 33 6 62 67 67 09 ; Email: [email protected]
Submitted: 19 September 2019
Accepted: 20 November 2019
Published: 23 November 2019
ISSN: 2333-7133
Copyright© 2019 Goldberg M
OPEN ACCESS
Keywords•Pulp cells; Pulpoblasts; Angiogenic; Dentin
innervation; apoptosis
Review Article
1-2- Pediatric Dental Development Pulp Biology, Defense Cells and InflammationMichel Goldberg*Department of Oral Biology, Paris Cité University, France
Abstract
Pulp cells biology includes sensitive and sensory-motor nerves, blood vessels and a inflammatory vascular network (T-lymphocytes, B-lymphocytes, dendritic cells, NK cells. Fibroblasts (or pulpoblasts) are linked by intercellular junctions (desmosomes and gap-junctions). After migration from the inner pulp toward the periphery, pulpoblasts are transferred toward the outer pulp border. The cells are renewed after they underwent functional apoptosis. Angiogenesis, neuronal differentiation, inflammatory cells, constitute the bulk of pulp cells. The dental pulp extracellular matrix components include collagen and non-collagenous molecules. Non-carious and carious lesions are the major non-genetic events leading to pulp degradation.
I-PULP CELLS BIOLOGY The outer layers of the pulp are located
• Beneath the mantle dentin (specifically in the crown),
• Whereas the superficial cell free and cell rich zones are situated both in crown and in roots.
They constitute cell layers (odontoblasts and Höhl cell layers) implicated in primary and secondary dentin formation. They are concerned by the synthesis, secretion and configuration of the peripheral dentins.
The dental pulp contains pulpoblasts (or pulpocytes) [1], that are the major cell components. In the central pulp, nerves are arising from the apex (as branches of the Vth cranial nerve, also named trigeminal nerve). Two branches are innervating the dental pulp and dentin. One is sensitive (the maxillary nerve) and the other sensory-motor (the mandibular nerve). The third branch is issued from the trigeminal ganglion and innervates the upper third of the face. It is the ophthalmic branch of Willis.
They fan out in the outer part of the pulp (Raschkov plexus). They are connected to the basal part of odontoblasts, pass between the lateral membranes and crosses intercellular junctions. They penetrate into the predentin and inside dentin tubules (up to the inner 150µm). Blood vessels (arterioles, venules and capillaries) built a vascular network. In addition cells implicated in the inflammatory response are identified as T-lymphocytes, B-lymphocytes forming clusters, dendritic cells, and NK cells. In human deciduous teeth, HLA-DR+, CD68+, and factor XIIIa are also present.
Fibroblasts (or pulpoblasts) are elongated cells, whith small stellated dendritic processes establishing contact between cells.
Desmosome-like and gap junctions tightly connect pulp cells. They contribute to form a continuous network. The intercellular matrix is occupied by the ground substance filling enlarged spaces. Pulp cells migrate from the central part toward pulp periphery, beneath the odontoblast layer, where no (or very few) fibroblastic apoptotic cells are detected. Pulpoblasts migration implicate a continuous transfer from the central part of the pulp toward the periphery. They are subjacent to odontoblasts and Höhl’s cells. They slide in the pulp. Intercellular junctions are instrumental in connecting cells, and migrating from the inside of the pulp, toward the periphery. This keep a continuous flow of newly-formed cells to the outer part of the pulp, where they become ultimately apoptotic [2]. The cell migration was demonstrated in the pulp of essential fatty acids deprived rats (EFAD) [3].
Pulp fibroblasts are implicated in the synthesis of collagens and non-collagenous extracellular matrix proteins. The rough endoplasmic reticulum and Golgi apparatus are implicated in these processses. Lysosomes within the cytoplasm participate to the cell degradation and re-uptake of the ground substance.
PULP CELL RENEWAL • Primary dentine refers to the dentin formed by actively
secreting odontoblasts during the crown formation.
• Secondary dentine is used for describing the physiological dentin that is continuously deposited after completion of root formation.
The secretory function of odontoblasts is tempered by autophagy, a housekeeping process that degrades some of the secretory intracellular components to preserve the functionality of these long-lived post-mitotic cells and to ensure their survival

Goldberg M (2019)Email: [email protected]
JSM Dent 7(1): 1117 (2019) 2/9
Central
during starvation, stress, or cell injury. The less actively secreting odontoblasts that produce secondary dentin are characterized by the presence of autophagic vacuoles and increasing deposition of intracellular lipofuscin
• The tertiary dentine contained irregular dentinal tubules that appeared to be disconnected with those present in the secondary dentin. However, observation of serial sections indicated that the tubules from the tertiary dentin are always continuous with the tubules of secondary dentin [4].
Odontoblasts and cells of the Höhl layer (identifed as pre-odontoblastic cells) are post-mitotic cells and they do not renew. In contrast with pulp fibroblasts, they are getting older but apparently stay alive. During the secondary dentin formation and located in a decreasing pulp chamber volume, the number of odontoblasts is slowly reduced. Odontoblast layers are starting with 3 to 4 rows of cells, and becomes gradually thinner. Ultimately, only one single layer of flattened cells remains. The so-called Höhl’s cell layer constitute probabily replacement cells and they differentiate into odontoblast-like cells
In contrast, dental pulp stem cells (DPSCs) take origin in the apical region (also named stem cells from the apical papilla, or SCAP cells) [5].
In vitro functional studies showed that dental pulp cells from unerupted molars displayed extensive osteo-dentinogenic potential but were unable to differentiate into chondrocytes and adipocytes. Dental pulp from erupted molars displayed a reduced number of cells. In vitro functional assays demonstrated the ability of a small fraction of cells to differentiate into odontoblasts, osteoblasts, adipocytes and chondrocytes.
Cell adhesion molecules are cell surface glycoproteins involved in diverse biological processes such as cell adhesion, cell recognition, control of cell division and migration, differentiation, and morphogenesis. Cell adhesion molecules are classified into four protein families: the cadherins, the integrins, the selectins, and the immunoglobulin superfamily proteins.
Cadherins make up a large superfamily that can be divided into classical, desmosomal, protocadherins, seven transmembrane, and FAT-like cadherins. Epithelial, Neuronal, and Placental cadherins represent the most well characterized classical cadherins [6]. Cadherins are linked with the actin cytoskeletal filaments and connected to actin-based adherens junctions. The connection to cytoskeletal proteins is crucial for efficient cell-cell adhesion. Changes in cadherin expression or function correlate with the onset of processes that control cell migration and differentiation. Intercellular junctions support that connections between pulp cells are determinant for the sliding and migration of pulp cells. Pulp cells differentiate into odontoblast-like cells, which start secretion and deposition of the reparative dentin matrix. High levels of stem cell factor (SCF) are acting as an agent of recruitment. This effect was accompanied by cytoskeletal re-arrangement.
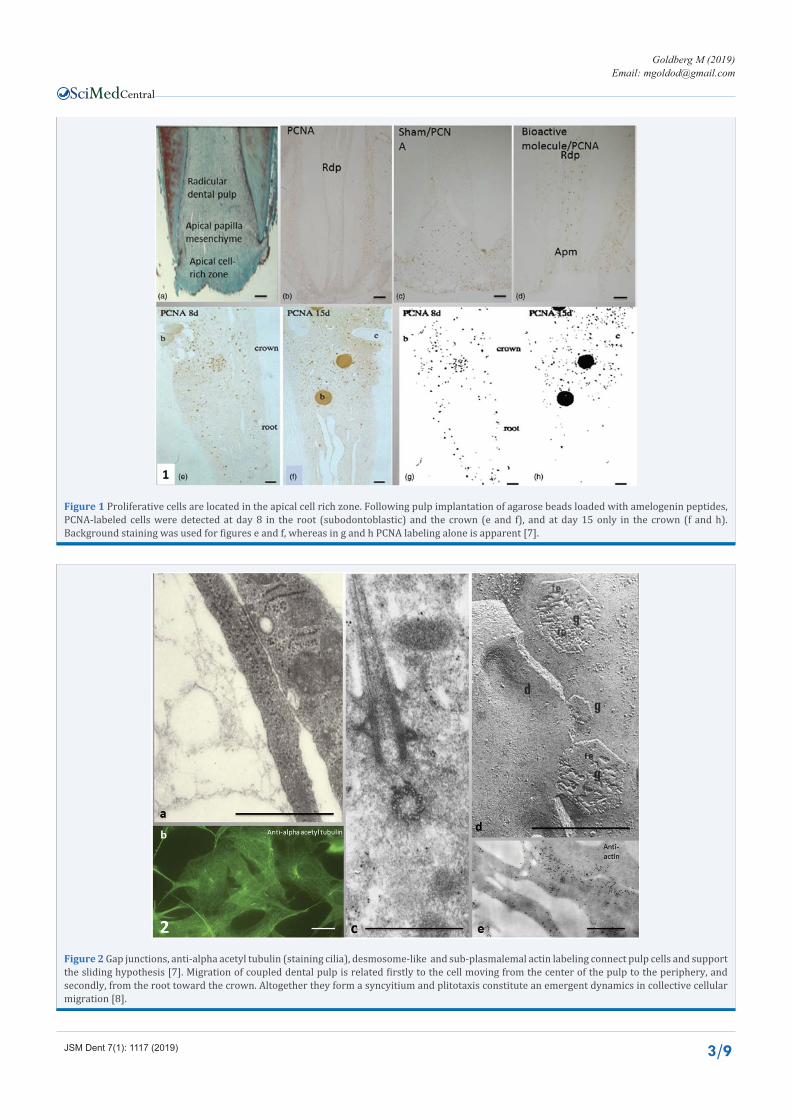
Hirata [7], have shown that PCNA–positive cells migrate at day 8, from the central part of the radicular pulp toward the sub-odontoblastic cell layer. Later, 15 days after implantation of beads
loaded with amelogenin-peptides, they are present only in the coronal pulp and totally lacking in the root. The time difference suggests that the radicular cells migrate, sliding from the root to the crown. This phenoenon, characterized as plithotaxis, govern pulp healing and regeneration.
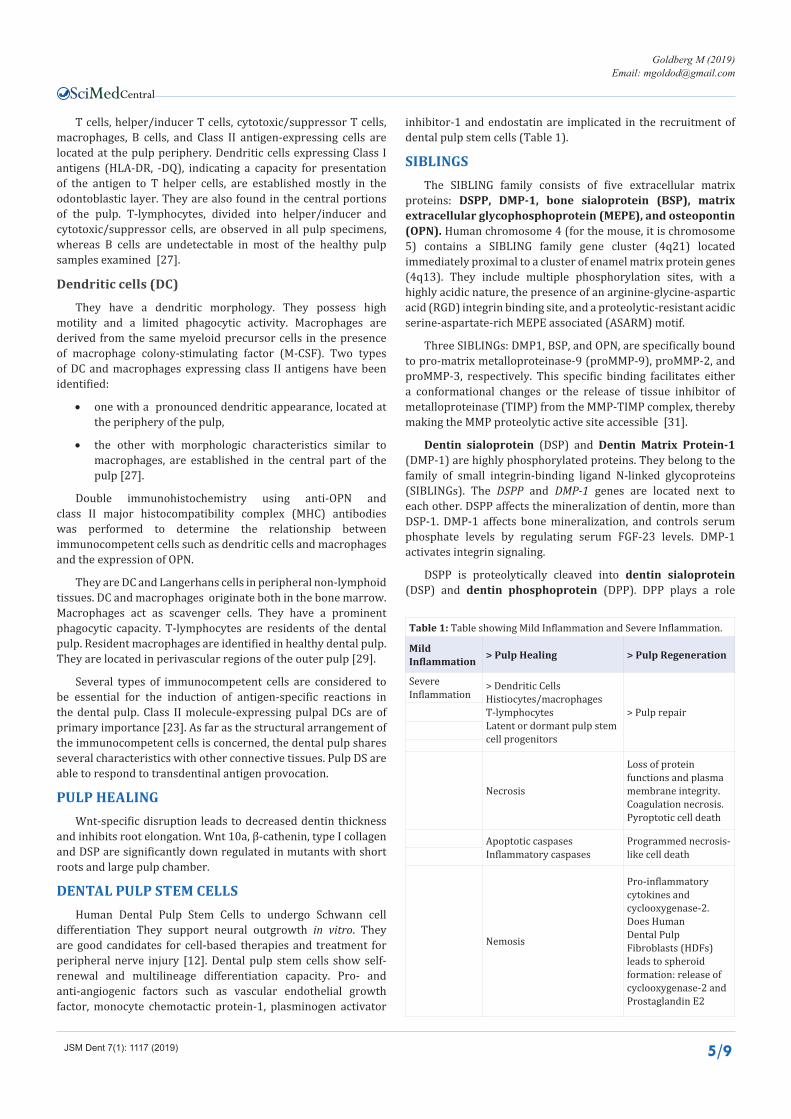
It has also been shown that once in the crown part, a continuous row of pulp cells migrate toward the outer part of the pulp, where they becomes apoptotic. Therefore, new cells issued from the center of the crown are involved in the replacement of fragmented apoptotic cells, as demonstrated by the effects induced by fatty acids deficiency [3] (Figure 1and 2).
ANGIOGENESIS Arterioles enters in the pulp via apical and accessory foramina.
The primary feeding arterioles divide into secondary and terminal arterioles. Pre-capillaries are in continuity with capillaries. They form loops of terminal capillaries and vascularize areas of about 100 to 150µm. Following post-capillaries, collecting venules merge into larger venules and exit from the pulp via the apex.
In the root, capillaries display a continuous fisher-like arrangement, in contrast with the loops seen in the coronal pulp. Intercellular junctions of the desmosome and gap-like type regulate the pulpal circulation (vasoconstriction and vasodilatation), according to Takahashi [9].
Shunt (or bypass) microvessels are observed in the pulp feeding individual areas of microcirculation. Anastomoses are also observed, linking arterioles to venules and/or venules to venules. U-turn loops are observed, bypassing the capillary bed. α-Smooth muscle actin was detected from the late bell stage up to the early root formation, preceding eruption. Runx2 positive cells overlap with the α−SMA positive area. In mature tissue, α-SMA is localized on the pericytes. Actin is specifically expressed in the dental follicle. Intercellular junctions are of the gap type, with discontinuities in the basement membrane.
Lymph vascularization is regulated by vascular endothelial growth factors (VEGF-C and D) and their receptors. Lymph capillaries are missing in the coronal and middle regions of the pulp, but extensively present in the apical region. Lymph collected in interstitial tissue is drained toward the apex via lymph capillaries. The lymph captured by unsealed endothelial cells flows in the apical direction toward the lymph node chains located in the neck.
NEURAL MARKERSNerves arise from the nerves main trunks of the Vth cranial
pair (primarily the maxillary and mandibular nerves), and spread in the direction of tooth buds. When the dental lamina is forming, a stage where tooth buds are underdeveloped, the dental nerves ingrow into the tooth buds. At the bell and cap stages, small nerve bundles enter the mesenchyme [10]. The nerves fan out and colonize the mesenchymal pulp. Located below the primordium area, they innervate the dental papilla. There is a relationship between the nerve sprouting and neural induction playing part of the initiation of odontogenesis. Nerves form a plexus. Innervation of the follicle is followed by nerve development within the papilla during tooth early maturation. Nerves enter the dental papilla
Goldberg M (2019)Email: [email protected]
JSM Dent 7(1): 1117 (2019) 3/9
Central
Figure 1 Proliferative cells are located in the apical cell rich zone. Following pulp implantation of agarose beads loaded with amelogenin peptides, PCNA-labeled cells were detected at day 8 in the root (subodontoblastic) and the crown (e and f), and at day 15 only in the crown (f and h). Background staining was used for figures e and f, whereas in g and h PCNA labeling alone is apparent [7].
Figure 2 Gap junctions, anti-alpha acetyl tubulin (staining cilia), desmosome-like and sub-plasmalemal actin labeling connect pulp cells and support the sliding hypothesis [7]. Migration of coupled dental pulp is related firstly to the cell moving from the center of the pulp to the periphery, and secondly, from the root toward the crown. Altogether they form a syncyitium and plitotaxis constitute an emergent dynamics in collective cellular migration [8].

Goldberg M (2019)Email: [email protected]
JSM Dent 7(1): 1117 (2019) 4/9
Central
when the crown formation reach completness [11]. DPSCs already express neural markers enhancing and guiding axonal outgrowth [12].
During tooth development, Nerve Growth Factor (NGF) and brain-derived neurotrophic factor (BDNF) were detected in the dental papilla/pulp of post-natal rats. Neurotrophin 3 and 4 were predominantly epithelial. Glial cell line-derived neurotrophic factor was mainly mesenchymal, observed in the odontoblast layer and subodontoblastic zone [13]. The physical confinement of dental pulp and its innervation within the tooth, and the high incidence of polymodal A-delta and C-fibers in pulp and dentin allow to study the neuroinflammatory interactions.
Dental pulp stem cells expressed some adipogenic, myogenic, neurogenic, osteogenic (osteonectin, osteocalcin, osteopontin, Runx-2, and type I collagen) and chondrogenic markers. Embryonic stem cell markers were also identified. The differentiation potential of human natal dental pulp and human bone marrow mesenchymal stem cells to adipogenic, osteogenic, chondrogenic, myogenic and neurogenic was confirmed [14].
Seventy to eighty per cent of the pulpal axons are unmyelinated. Intradental A- and C-fibres are activated by extrenal stimuli. A-fibres are responsible for the sensitivity of dentin. Aβ- and Aδ–fibres indicate that they belong to the same functional group. Intradental C-fibres are activated only if functional stimuli reach the pulp proper [15].
Axonal transport of radioactive 3H proline was followed by radioautography. Numerous myelinated and unmyelinated axons formed a few terminal branches in the roots but primarily branched in the crown to form the peripheral plexus of Raschkow and terminate as free endings in the odontoblast layer, and as far as 120μm in the inner part of dentinal tubules. The transported protein was confined to sensory axons and endings. Odontoblasts and dentin matrix were not significantly labeled. Dentinal sensory nerve endings in primate teeth can be profuse, sparse, or absent, depending on the location and structure of dentin and the adjacent pulp. When dentin is innervated, the tubules were straight and contained odontoblast processes. The predentin is wide. Odontoblast cell bodies are relatively columnar, with an adjacent cell-free zone and pulpal nerve plexus [16].
PULP INFLAMMATION - DEFENSE CELLSInflammation is a prerequisite for pulp healing, pulp necrosis
includes pyroptosis, apoptosis, and nemosis, with a series of events ahead of regeneration. Immunocompetent cells are recruited in the apical part. They slide along the root and migrate toward the crown. Due to the high alkalinity of the capping agent, pulp cells proliferate and initiate mineralization. After direct capping, pulp fibroblasts become odontoblast-like cells producing type I collagen, alkaline phosphatase, and SPARC/osteonectin. Molecules of the SIBLING family, matrix metalloproteinases, vascular and nerve mediators are also implicated in the formation of a reparative dentinal bridge, osteo or orthodentin closing the pulp exposure.
Inflammatory and/or noninflammatory processes contribute to produce a reparative dentinal bridge closing the pulp exposure, with minute canaliculi and large tunnel defects [17].
INFLAMMATORY AND IMMUNOCOMPETENT PULP CELLS
Inflammatory cells include pulpal dendritic cells, histiocytes/macrophages and T-lymphocytes. Lymphocytes are classified as B- or T- lymphocytes. T-lymphocytes involve cells, such as helper/inducer T-cells (CD4+) and cytotoxic/suppressor T-cell (CD8+). The B-lymphocytes are rare or lacking in the normal pulp. During the early inflammatory reaction phase, B-lymphocytes are present, and they increase in number. In contrast, the T-lymphocytes are revealed by immunostaining both in normal and inflammed pulps. Lymphocytes are found as normal resident cells.
The dendritic cell family migrates from the bone marrow to the pulp. Macrophages are scavengers cells displaying phagocytic capacities. Dendritic cells (DC) are concentrated at the periphery of the coronal pulp. They are members of the class I and II major histocompatibility complex (MHC).
Resident macrophages appear at perivascular locations. Non-resident macrophages and monocytes constitute minor macrophage populations. Mast cells containing histamine, leukotrienes and palatet-activating factors are implicated in immediate hypersensitivity reaction.
Melanocytes arise from the neural crest cell population. Melanocytes are elongated dendritic cells with specific organelles, called melanosomes, which contain all components required for melanin biosynthesis. Polymorphonuclear leukocytes are mostly involved in the capture and degradation of bacteria [18].
Dental pulp stem cells have a great potential in regenerative medicine [19,20]. They differentiate in vitro toward the melanocytic lineage. These cells show morphological and molecular features of melanocytes. DPSCs cultured in MEM differentiate into melanocytes at considerably slower rate than those cultured in DMEM [21,22].
B-lymphocytes produce antibodies against specific antigens following blast formation, proliferation, and maturation into plasma cells [23]. T-lymphocytes are divided into T-helper cells (CD4+) and cytotoxic T-cells (CD8+). When CD4+ are activated, T-lymphocytes are identified according the recognition of membrane-bound T-cell receptors.
CD4+T-lymphocytes are further classified into Th1 and Th2 cells. Th1 produce interleukin and interferon gama. Undifferentiated cells participate in dentin and pulp regeneration. The expression of DSPP, Cbfa1, and collagen types I and III in pulp is currently considered: DSPP is expressed mostly by odontoblast cells [24]. The transcriptional factor Cbfa1 is expressed in mouse dental pulp clonal cell lines [25]. Both type I and III collagen are produced by pulp fibroblasts, whereas collagens type III, V, VI have been actually identified in the pulp [26].
Antigen-presenting cells (APC)
The Major Histocompatibility Complex (MHC) region encodes transplantation class I and class II molecules. Dendritic cells, macrophages, B-lymphocytes, endothelial cells, and various epithelial and mesenchymal cells are constitutive or inducible cells expressing Class II MHC molecules.
Goldberg M (2019)Email: [email protected]
JSM Dent 7(1): 1117 (2019) 5/9
Central
T cells, helper/inducer T cells, cytotoxic/suppressor T cells, macrophages, B cells, and Class II antigen-expressing cells are located at the pulp periphery. Dendritic cells expressing Class I antigens (HLA-DR, -DQ), indicating a capacity for presentation of the antigen to T helper cells, are established mostly in the odontoblastic layer. They are also found in the central portions of the pulp. T-lymphocytes, divided into helper/inducer and cytotoxic/suppressor cells, are observed in all pulp specimens, whereas B cells are undetectable in most of the healthy pulp samples examined [27].
Dendritic cells (DC)
They have a dendritic morphology. They possess high motility and a limited phagocytic activity. Macrophages are derived from the same myeloid precursor cells in the presence of macrophage colony-stimulating factor (M-CSF). Two types of DC and macrophages expressing class II antigens have been identified:
• one with a pronounced dendritic appearance, located at the periphery of the pulp,
• the other with morphologic characteristics similar to macrophages, are established in the central part of the pulp [27].
Double immunohistochemistry using anti-OPN and class II major histocompatibility complex (MHC) antibodies was performed to determine the relationship between immunocompetent cells such as dendritic cells and macrophages and the expression of OPN.
They are DC and Langerhans cells in peripheral non-lymphoid tissues. DC and macrophages originate both in the bone marrow. Macrophages act as scavenger cells. They have a prominent phagocytic capacity. T-lymphocytes are residents of the dental pulp. Resident macrophages are identified in healthy dental pulp. They are located in perivascular regions of the outer pulp [29].
Several types of immunocompetent cells are considered to be essential for the induction of antigen-specific reactions in the dental pulp. Class II molecule-expressing pulpal DCs are of primary importance [23]. As far as the structural arrangement of the immunocompetent cells is concerned, the dental pulp shares several characteristics with other connective tissues. Pulp DS are able to respond to transdentinal antigen provocation.
PULP HEALING Wnt-specific disruption leads to decreased dentin thickness
and inhibits root elongation. Wnt 10a, β-cathenin, type I collagen and DSP are significantly down regulated in mutants with short roots and large pulp chamber.
DENTAL PULP STEM CELLSHuman Dental Pulp Stem Cells to undergo Schwann cell
differentiation They support neural outgrowth in vitro. They are good candidates for cell-based therapies and treatment for peripheral nerve injury [12]. Dental pulp stem cells show self-renewal and multilineage differentiation capacity. Pro- and anti-angiogenic factors such as vascular endothelial growth factor, monocyte chemotactic protein-1, plasminogen activator
inhibitor-1 and endostatin are implicated in the recruitment of dental pulp stem cells (Table 1).
SIBLINGSThe SIBLING family consists of five extracellular matrix
proteins: DSPP, DMP-1, bone sialoprotein (BSP), matrix extracellular glycophosphoprotein (MEPE), and osteopontin (OPN). Human chromosome 4 (for the mouse, it is chromosome 5) contains a SIBLING family gene cluster (4q21) located immediately proximal to a cluster of enamel matrix protein genes (4q13). They include multiple phosphorylation sites, with a highly acidic nature, the presence of an arginine-glycine-aspartic acid (RGD) integrin binding site, and a proteolytic-resistant acidic serine-aspartate-rich MEPE associated (ASARM) motif.
Three SIBLINGs: DMP1, BSP, and OPN, are specifically bound to pro-matrix metalloproteinase-9 (proMMP-9), proMMP-2, and proMMP-3, respectively. This specific binding facilitates either a conformational changes or the release of tissue inhibitor of metalloproteinase (TIMP) from the MMP-TIMP complex, thereby making the MMP proteolytic active site accessible [31].
Dentin sialoprotein (DSP) and Dentin Matrix Protein-1 (DMP-1) are highly phosphorylated proteins. They belong to the family of small integrin-binding ligand N-linked glycoproteins (SIBLINGs). The DSPP and DMP-1 genes are located next to each other. DSPP affects the mineralization of dentin, more than DSP-1. DMP-1 affects bone mineralization, and controls serum phosphate levels by regulating serum FGF-23 levels. DMP-1 activates integrin signaling.
DSPP is proteolytically cleaved into dentin sialoprotein (DSP) and dentin phosphoprotein (DPP). DPP plays a role
Table 1: Table showing Mild Inflammation and Severe Inflammation.
Mild Inflammation > Pulp Healing > Pulp Regeneration
Severe Inflammation
> Dendritic Cells Histiocytes/macrophages T-lymphocytes Latent or dormant pulp stem cell progenitors
> Pulp repair
Necrosis
Loss of protein functions and plasma membrane integrity. Coagulation necrosis. Pyroptotic cell death
Apoptotic caspases Inflammatory caspases
Programmed necrosis-like cell death
Nemosis
Pro-inflammatory cytokines and cyclooxygenase-2. Does Human Dental Pulp Fibroblasts (HDFs) leads to spheroid formation: release of cyclooxygenase-2 and Prostaglandin E2

Goldberg M (2019)Email: [email protected]
JSM Dent 7(1): 1117 (2019) 6/9
Central
in initiation and maturation of dentin mineralization. Distinct roles of DSP and DPP indicate that DSP is regulating initiation of dentin mineralization, while DPP is involved in the maturation of mineralized dentin [32]. DSP and DMP-1 are both cleaved into two protein chains. The N-terminal region is formed by proteoglycans that contain chondroitin sulfate chains, and the C-terminal region is highly phosphorylated.
Dmp-1 is an acidic phosphorylated extracellular matrix protein mapped to mouse chromosome 5q21 and human chromosome 4q21/22. DNA sequence analysis revealed that DMP1 is rich in aspartic acid, glutamic acid, and serine, and has numerous potential phosphorylation sites for casein kinases I and II. DMP1 has a potential RGD cell attachment sequence and chondroitin sulfate chains attached to the NH2-terminal. Although also expressed in bone, this protein is mostly odontoblast-specific.
Biglycan (Bgn) and Decorin (Dcn) are major small leucine rich repeat proteoglycans (SLRPs) found in dentin. Bone morphogenetic protein 1 (BMP-1) cleave full-length DMP-1 and DSPP proteins into two proteins. Meprin A, a member of the astacin family, can cleave the DSPP precursor protein to generate DPP. The functions of DSPP and DMP-1 are mainly dependent on their phosphorylated C-terminal protein region. Active BMP-1, which is processed by furin convertase, cleaves full-length DSPP and DMP-1.
ENDOGENOUS METALLOPROTEINASES AND MEMBRANE-TYPE MMPS
MMPs are a family of 23 mammalian enzymes, which degrade all extracellular matrix proteins. Dentin also contains MMP activity, as well as collagenase (MMP-8), and gelatinases (MMP-2 and MMP-9). Cathepsins B and L cleave non-helical telopeptide extensions of the collagen fibres, and cathepsin K cleaves collagen in the triple helical region.
MMPs are divided into 5 groups: collagenases (MMP-1, -8, -13, 18), gelatinases (MMP-2 and MMP-9), stromelysins (MMP -3, -7, -10, -11, -12), membrane-type MMPs (MMP-14, -15, -16, -17) and MMP-20 (also called enamelysin) implicated in the degradation of amelogenins [34,35].
The degradation of collagens and other extracellular matix components is regulated by MMPs. Gelatinase A (MMP-2, or type IV collagenase : 72kDa) and gelatinase B (MMP-9) are cuting the collagen fibers into two parts (1/4 th and ¾ th). MMP2 removes the collagen telopeptides from the ends of helical collagens. It becomes a better substrate for casein kinase II after a limited proteolysis with MMP-2. The MMPs are produced as latent proenzymes, and can be inhibited by specific tissue inhibitors of metalloproteinases.
MMP-8 can cleave the collagen fibres into two large fragments. Cathepsin K splits both helical and telopeptide regions. Cathepsins B and L cleave the non-helical telopeptides estensions of collagens, whereas cathepsin K cleaves the collagen at the triple helical region. Lysosomal cystein cathepsins degrade type I collagen, laminin, fibronectin and proteoglycans [36,37].
The enzymes can be divided into two structurally distinct subgroups, the membrane-type and secreted MMPs. The secreted MMPs include interstitial collagenases which degrade fibrillar collagens, and elastases with high activity against gelatin and type IV collagen.
Genetically distinct MT-MMPs have been identified. These enzymes (except MMP- 17, which is glycosyl-phosphatidyl-inositol anchored) are singlepass type I membrane proteins with an extracellular N terminus containing the catalytic domain and a short C-terminal cytoplasmic domain. MMP-14 was first identified as a cellular receptor and activator. Both MT1-MMP and MT2- MMP (MMP-15) have activity against a variety of ECM proteins [38].
III-PULP CELLS APOPTOSIS Apoptosis is an important morphogenetic event both in
embryology and during the post-natal life. Comparison of the odontoblasts activity within the pulp of deciduous versus permanent teeth supports that the deciduous teeth presented a reduced layer of odontoblasts, and greater apoptotic cells. Odontoblats of deciduous teeth have a predominant pro-apoptotic phenotype.
The transient co-localizations of c-Jun N-terminal Kinase (JNK) and C-Jun with Heat Shock Protein 70 (HSP70) are involved in pulp cells stress-induced apoptosis [39]. The association of JNK and anti-apoptotic HSP was established with pulp apoptosis. After injury, HSP70 migrates from the nucleus to the cytoplasm. The cysteine cathepsins proteases initiate and promote apoptotic signaling [40]. Apoptosis has been observed in early morphogenesis, during mineralized tissue formation, and during tooth eruption. The appearance of apoptotic cells detected by TUNEL and the presence of apoptotic bodies correlates with caspase-3 activation. Apoptotic bodies result from the cytoplasmic blebing and subsequently, the destruction of the nuclei. Macrophages and dendritic cells eliminate cells fragments (apoptotic bodies) [2].
IV- INFLAMMATORY PROCESSESNon-infectious pulp degradation was reviewed by Imfeld
[41]. The terms ‘abfraction’ and ‘abrasion’ describe lesions found in cervical margins. Mechanical destruction of cusps and abrasion may be due to grinding and other mechano-chemical factors [42]. Erosion, abrasion, and attrition are due to excessive horizontal toothbrushing. Abfraction have another etiology and involves occlusal stress. The theory of abfraction is based primarily on analyses demonstrating stress concentration at the cervical area. Tribocorrosion is a wear process in which corrosion and abrasion act simultaneously or successively. However, the destruction of dental tissues is mostly related to the carious decay and some reactions are resulting from the degradative processes due to bacteria.
CARIOUS DECAYDental caries is related to the local destruction of dental
hard tissues by acidic by-products from bacterial fermentation of dietary carbohydrates [43]. All types of microorganisms are not equally able to ferment carbohydrates. Looking for the major

Goldberg M (2019)Email: [email protected]
JSM Dent 7(1): 1117 (2019) 7/9
Central
caries pathogens, it was noted that in patients with excellent oral hygiene there is virtually no ‘plaque’ on the tooth surfaces, but carious lesions are present. Streptococcus Mutans (SM) may be below the detection level. Relatively high proportions of SM may persist on tooth surfaces without caries progression while caries may develop also in the absence of these species and therefore, caries are not a classical infectious disease [44].
Endogenous bacteria produce weak organic acids as a by-product of metabolism of fermentable carbohydrates. These acids cause local falls of pH values below a critical value resulting in demineralisation of tooth. This process leads either to cavitation within the tooth or to the repair and reversal of the lesion, or to the maintenance of the status quo. Remineralisation is frequent, especially when the pH of the biofilm is restored by saliva acting as a buffer. The acids produced include lactic, acetic, formic and propionic, dissolving the mineral of teeth [45]. Many of the functions of the salivary proteins have been established together with the protective role of saliva in the reversal or arrestment of the caries process.
More than 300 bacterial species are components of the oral microflora. However, only few species are able to invade and infect the root canal space. Studies on the microbiology of primary dental caries in human indicate the role of the SM in the initiation of caries of smooth surfaces and fissures of crowns, and suggest a potent role in inducing root surface caries [46].
Molecular/genetic studies of implicated bacteria isolated from humans, indicate that SM spread vertically, mostly from mothers to their children. The tooth surface selectively adsorbs various acidic glycoproteins (mucins) from the saliva, contributing to the formation of the acquired enamel pellicle (AEP), which varies in thickness from 0.1 to 3µm, and contains a high number of sulfate and carboxyl groups.
Data provide evidences that SM are human odontopathogens. As such, dental caries is a diagnosable and treatable infection. Colonization by SM occurs after tooth eruption, and if the fissures are colonized in their depths, the decay may be inevitable. However, if this colonization is delayed until the fissure depths are occupied by other bacteria, the carious decay will not occur or its occurrence will be greatly reduced. This understanding of the ecology of SM suggests treatment strategies. The surfaces of the mineralized dental tissues are coated by a pellicle to which the microbial cells attach. The colonizers generate a matrix of exopolymer within which cells grow.
However, the carious decay results from the pellicle and plaque associated to bacteria implicated in the colonization of tooth surfaces.
REFERENCES1. Baume LJ. The biology of pulp and dentine: a historic,
terminologitaxonomic; histologic- biochemical, embryonic and clinical survey. In Monographs in Oral Science. 1980; 8: 1-220.
2. Vermelin L, Lécolle S, Septier D, Lasfargues J-J, Goldberg M. Apoptosis in human and rat dental pulp. Euro J Oral Sci. 1996; 104: 547-553.
3. Vermelin L, Ayanoglou Ch, Septier D, Carreau JP, Bissila-Mapahou P, Goldberg M. Effects of essential fatty acid deficiency on rat molar pulp cells. Eur J Oral Sci. 1995; 103: 219-224.
4. Ricucci D, Loghin S, Lin LM, Spangberg LSW, Tay FR. Is hard tissue formation in the dental pulp after the death of the primary odontoblasts a regenerative or a reparative process? J Dent. 2014; 42: 1156-1170.
5. Sonoyama W, Liu Y, Yamaza T, Tuan RS, Wang S, Shi S, et al. Characterization of apical papilla and its residing stem cells from human immature permanent teeth-a pilot study. J Endod. 2008; 34: 166-171.
6. Heymann R, About I, Lendahl U, Franquin JC, Öbrink B, Mitsiadis TA. E- and N-cadherin distribution in developing and functional human teeth under normal and pathological conditions. Am J Pathol. 2002; 160: 2123-2133.
7. Hirata A, Dimitrova-Nakov S, Djole SX, Ardila H, Baudry A, Kellermann O, et al. Plithotaxis, a collective cell migration, regulates the sliding of proliferating pulp cells located in the apical niche. Connective Tissue Res. 2014; 55: 68-72.
8. Trepat X, Fredberg JJ. Plithotaxis and emergent dynamics in collective cellular migration. Trends Cell Biol. 2011; 21: 638-646.
9. Takahashi K. Vascular architecture of dog pulp using corrosion resin cast examined under a scanning electron microscope. J Dent Res. 1985; 64: 579 -584.
10. Pearson AA. The early innervation of the developing deciduous teeth. J Anat. 1977; 123: 563-577.
11. Mohamed SS, Atkinson ME. A histological study of the innervation of developing mouse teeth. J Anat. 1983; 136: 735-749.
12. Martens W, Sanen K, Georgiou M, Struys T, Bronckaers A, Ameloot M, et al. Human dental pulp stem cells can differentiate into Schwann cells and promote and guide neurite outgrowth in an aligned tissue-engineered collagen construct in vitro. FASEB J. 2014; 28: 1634-1643.
13. Nosrat CA, Fried K, Ebendal T, Olson L. NGF, BDNF, NT3, NT4 and GDNF in tooth development. Eur J Oral Sci. 1998; 106: 94-99.
14. Karaöz E, Dogan BN, Aksoy A, Gacar G, Akyuz S, Ayhan S, et al. Isolation and in vitro characterisation of dental pulp stem cells from natal teeth. Histochem Cell Biol. 2010; 133: 95-112.
15. Narhi M, Jyvasjarvi E, Virtanen A, Huopaniemi T, Ngassapa D, Hirvonen T. Role of intradental A- and C-type nerve in dental pain mechanisms. Proc Finn Dent Soc. 1992; 88: 507-516.
16. Byers MR, Dong WK. Autoradiographic location of sensory nerve endings in dentin of monkey teeth. Anat Rec. 1983; 205: 441-454.
17. Goldberg M, Njeh A, Uzunoglu E. Is pulp inflammation a prerequisite for pulp healing and regeneration? Mediators of inflammation. 2015; 2015: 1-11.
18. Goldberg M. Superficial and deep carious lesions. Chapter 9 In Understanding Dental Caries (M. Goldberg ed.) Springer Int Publishing Switzerland. 2016 : 85-96.
19. Huang GTJ, Yamaza T, Shea L, Djouad F, Kuhn NZ, Tuan RS, et al. Stem/progenitor cell-mediated de novo regeneration of dental pulp with newly deposited continuous layer of dentin in an in vivo model Tissue Engineering Part A. 2010 ; 16: 605-615.
20. Tatullo M, Marrelli M, Shakesheff KM, White LJ. Dental pulp stem cells: function, isolation and applications in regenerative medicine. J Tissue Eng reg Med. 2015; 9: 1205-1216.
21. Paino F, Ricci G, De Rosa A, D’Aquino R, Laino L, Pirozzi G, et al. Ecto-mesenchymal stem cells from dental pulp are committed to differentiate into active melanocytes. Eur Cells Mat. 2010; 20: 2 9 5 - 3 0 5.
22. Arpornsuwan T, Sriwai W, Sritanaudomchai H, Roytrakul S. Using

Goldberg M (2019)Email: [email protected]
JSM Dent 7(1): 1117 (2019) 8/9
Central
Oral and Colon Cancer Cells for Studying the Anticancer Properties of Antimicrobial Peptides. Methods Mol Biol. 2017; 1548: 345-357.
23. Jontell M, Okiji T, Dahlgren U, Bergenholtz G. Immune defense menchanisms of the dental pulp. Crit Rev oral Biol Med. 1998 ; 9 : 179-200.
24. MacDougall M, Simmons D, Luan X, Nydegger J, Feng J, Gu TT. Dentin phosphoprotein and dentin sialoprotein are cleavage products expressed from a single transcript coded by a gene on human chromosome 4. J Biol Chem. 1997; 272: 835-842.
25. Priam F, Ronco V, Locker M, Bourd K, Bonnefoix M , Duchêne T, et al. New cellular models for tracking the odontoblast phenotype. Arch Oral Biol. 2005: 50: 271-277.
26. Veis A, Goldberg M. Pulp extracellular matrix. In M. Goldberg (ed) The dental pulp Springer Verlag Berlin Heidelberg 2014; 35-46.
27. Jontell M, Gunraj M, Bergenholtz G. Immunocompetent cells in normal dental pulp. J Dent Res. 1987; 66: 1149-1153.
28. Jontell M, Bergenholtz G, Scheynius A, Ambrose W. Dendritic cells and macrophages expression class II antigens in the normal rat incisor pulp. J Dent Res. 1988; 67: 1263-1266.
29. Cooper PR, Holder MJ, Smith AJ. Inflammation and regeneration in the dentin-pulp complex: a double-edged sword. J Endod. 2014; 40: S46-51.
30. Suzuki S, Haruyana N, Nishimura F, Kulkarni AB. Dentin sialophosphoprotein and dentin matrix protein-1: two highly phosphorylated proteins in mineralized tissues. Archs Oral Biol. 2012; 57: 1165-1174.
31. Suzuki S, Sreenath T, Haruyama N, Honeycutt C, Terse A, Cho A, et al. . Dentin sialoprotein and dentin phosphoprotein have distinct roles in dentin mineralization. Matrix Biol. 2009; 28: 221-229.
32. Tjäderhane L, Palossari H, Wahlgren J, Larmas M, Sorsa T, Salo T. Human odontoblast culture method : the expression of collagen and matrix metalloproteinases (MMPs). Adv Dent Res. 2001; 15: 55-58.
33. Sulkala M, Larmas M, Sorsa T, Salo T, Tjäderhane L. The localization of
matrix metalloproteinase-20 (MMP-20, enamelysis) in mature human teeth. J Dent Res. 2002; 81: 603-607.
34. Tersariol ILS, Geraldelt S, Minciotti CL, Nascimento FD, Pääkkönen V, Martins MT, et al. Cysteine Cathepssins in human dentin-pulp complex. J Endod. 2010; 36: 475-481.
35. Nascimento FD, Minciotti CL, Geraldeli S, Carriho MR, Pashley DH, Tay FR, et al. Cysteine Cathepsins in human carious dentin. J Dent Res. 2011; 90: 506-511.
36. Zhou Z, Apte SS, Soininen R, Cao R, Baaklini GY, Rauser RW, et al. Impaired endochondral ossification and angiogenesis in mice deficient in membrane-type matrix metalloproteinase I. PNAS. 2000; 97: 4052-4057.
37. Kitamura C, Ogawa Y, Nishihara T, Morotomi T, Terashita M. Transient co-localization of c-Jun N-terminal Kinase and c-Jun with heat Shock Protein 70 in pulp cells during apoptosis. J Dent Res. 2016; 82: 91-95.
38. Matalova E, Svandova E, Tucker AS. Apoptotic signaling in mouse odontogenesis. OMICS A J Int Biol. 2O12; 16: 60-70.
39. Imfeld T. Dental erosion, definition, classification and links. Eur J Oral Sci. 1996; 104: 151-155.
40. Bartlett DW, Shah P. A critical review of non-carious cervical (wear) lesions and the role of abfraction, erosion, and abrasion. J Dent Res. 2016; 85: 306-312.
41. Selwitz RH, Ismail AI, Pitts NB. Dental caries Lancet. 2007; 369: 51-59.
42. Fejerskov O. Changing paradigms in concepts on dental caries: consequences for oral health care. Caries Res. 2004; 38: 182-191.
43. Featherstone JBD. Dental caries: a dynamic disease process. Aus Dental J. 2008; 53: 286-291.
44. Loesche WJ. Role of Streptococcus mutans in human dental decay. Microbiol Rev. 1986; 50: 353-380.
45. Tanzer JM, Livingston J, Thompson AM. The microbiology of primary dental caries in human. J Dental Edu. 2001; 65: 1028-1037.
46. Trepat X, Fredberg JJ. Plithotaxis and emergent dynamics in collective cellular migration. Trends Cell Biol. 2011; 21: 638-646.

Goldberg M (2019)Email: [email protected]
JSM Dent 7(1): 1117 (2019) 9/9
Central
Goldberg M (2019) 1-2- Pediatric Dental Development Pulp Biology, Defense Cells and Inflammation. JSM Dent 7(1): 1118.
Cite this article




















![Cobourne [1999] the Genetic Control of Early Odontogenesis](https://img.pdfslide.us/doc/110x75/577cd66a1a28ab9e789c508c/cobourne-1999-the-genetic-control-of-early-odontogenesis.jpg)




![Muscle Innervation Chart II[1]](https://img.pdfslide.us/doc/110x75/55241db64a7959da488b45f0/muscle-innervation-chart-ii1.jpg)

