Embed Size (px)
Citation preview

2/15/2017
1
BREAST CANCER PATHOLOGY
REPORTS
WHAT IS PATHOLOGY
• Pathology (from Greek pathos, feeling, pain, or suffering and ‘ology signifies the study of) is the study and diagnosis of a disease through examination of organs, tissue cells, and bodily fluids.
• The term encompasses both the medical specialty which uses tissues and bodily fluids to obtain clinically useful information, as well as scientific study of the disease process.
HISTORY OF PATHOLOGY
• The history of both experimental and medical pathology can be traced to the earliest application of the scientific method to the field of medicine, a development which occurred in Western Europe during the Italian Renaissance.
• Most early pathologists were practicing physicians or surgeons. Like other medical fields, pathology has become more specialized with time, and most pathologists today do not practice in other areas of medicine.
EARLY FAMOUS PATHOLOGIST
• No true documentation of autopsies performed before the renaissance age. (1325-1600)
• Antonio Benivieni (1443-1502) was the first physician to do anatomic dissection to determine the cause of death, he was Italian.
• Most famous gross pathologist
HOW MUCH EDUCATION IS NEEDED TO BECOME A PATHOLOGIST• Pathologists are physicians who diagnose and study diseases. They have significant educational
requirements that include completing medical school, residencies and possibly fellowships, along with earning a license. Medical programs require both classroom coursework and hands-on training. Pathologists must be precise, knowledgeable in science and able to work under pressure.
• 4 years of college, to get a bachelors degree. 4 years of medical school, to get the doctor of medicine (MD) degree. 4 or 5 years of residency (4 for anatomic pathology only, or 5 for combined anatomic/clinical pathology, the latter track being recommended) to become eligible to take the Board exams in pathology. Average income 2016 is $177,000.
HOW MANY DIFFERENT PATHOLOGY SPECIALTIES ARE THERE?• Anatomical pathology Radiation pathology
• Cytopathology Immunopathology
• Dermatopathology Molecular pathology
• Forensic pathology Hemapathology
• Histopathology Oral and maxillary pathology
• Neuropathology
• Pulmonary and renal pathology
• Surgical pathology
• Clinical pathology

2/15/2017
2
TOOLS OF THE PATHOLOGIST
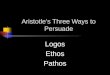
Zacharias Janssen and the first compound microscopeIn 1590
Zacharias Janssen was a Dutch spectacle-maker from Middelburg associated with the invention of the first optical telescope. Janssen is sometimes also credited for inventing the first truly compound microscope
British researchers from the University of Manchester helped develop the instrument which has broken all records for magnifying small objects using ordinary white light.The 'microsphere nanoscope is capable of examining objects as small as 50 nanometers across - 20 times smaller than the present limit for optical microscopesNanometer is one millionth of a millimeterHuman hair is one tenth of a millimeter
SURGICAL PATHOLOGIST
• Surgical pathology is the most significant and time-consuming area of practice for most anatomical pathologists. Surgical pathology involves the gross and microscopic examination of surgical specimens, as well as biopsies submitted by non-surgeons such as general internists, medical subspecialists, dermatologists, and interventional radiologists. Generally recognized sub-specialties of surgical pathology include the following:

2/15/2017
3
SURGICAL PATHOLOGIST
• The practice of surgical pathology allows for definitive diagnosis of disease (or lack thereof) in any case where tissue is surgically removed from a patient. This is usually performed by a combination of gross (i.e., macroscopic) and histologic (i.e., microscopic) examination of the tissue, and may involve evaluations of molecular properties of the tissue by immunohistochemistry or other laboratory tests.
• http://www.consumersresearchcncl.org
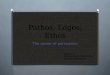
Gross examinationFrozen sectionFixation & EmbeddingHistopathologic examinationAncillary testingThe surgical pathology reportDirect consultation
Surgical pathology workflow
http://www.consumersresearchcncl.org/
TYPES OF BREAST PATHOLOGY REPORTS
Pathologist can read outside slides for patient’s who are requesting a second opinion
Pathologist can read specimen slides taken from FNA’s
Pathologist can read specimen’s taken by core biopsies
Pathologist can read specimen’s taken from segmental mastectomies
Pathologist can read specimen’s taken from mastectomies
WHY NOTTINGHAM?
• There are different "scoring systems" available for determining the grade of a breast cancer. One of these systems is the Nottingham Histologic Score system (the Elston-Ellis modification of Scarff-Bloom-Richardson grading system). In this scoring system, there are three factors that the pathologists take into consideration:
• the amount of gland formation ("differentiation" or how well the tumor cells try to recreate normal glands) differentiation is change/un-differentiation cells are not specialized.
• the nuclear features ("pleomorphism" or how "ugly" the tumor cells look)
• the mitotic activity (how much the tumor cells are dividing)
PATHOLOGY REPORTREPORTED BY PATHOLOGIST
• Presents a picture from the inside to better serve the case… • Reports must state the following• Specimen• Clinical History• Clinical Diagnosis• Gross Description• Microscopic Description• Special tests or markers• Summary or final Diagnosis
FNA BIOPSY PATHOLOGY READING
• Fine Needle Aspiration

2/15/2017
4
FNA SET-UP U/S ROOM
FNA PROCEDUREFNA SPECIMEN
• FNA
– Samples can be obtained in under a minute.
– Full procedure times run approximately 10-15 minutes.
– If there is an on-site lab, preliminary results are available within 15 minutes, otherwise, full results take 3-5 business days. Some facilities only take one day depending on patient load.
FINE NEEDLE ASPIRATION
• FNA
– Indications
• Confirming a benign looking lesion.
• Determining malignancy of a node.
• When staging a known breast cancer and there are satellite lesions an FNA should be done to not get malignant cells in a large core bx, so FNA is more direct.
FINE NEEDLE ASPIRATION

2/15/2017
5
• FNA
– Contraindications
• Suspected malignant lesion
• Suspected invasive lobular carcinoma
• Some large fibroadenoma's/why?
FINE NEEDLE ASPIRATION
• Ultrasound Core Biopsy– A lesion is identified and targeted with the use of ultrasound.
– A large needle is then advanced to the site, where the needle is fired and the specimen is retrieved.
– This process is repeated until the physician is satisfied that the area has been properly sampled. Usually, this requires 3-6 cores.
– Or a needle with VAD is used, where the needle remains in place while the cores are acquired.
FINE NEEDLE ASPIRATION
• Ultrasound Core Bx– The goal is identical to stereotactic biopsies, to obtain a tissue sample for
the pathologist to determine histology and tumor markers.
– Ultrasound capabilities focus more on masses and distortion. Calcifications are hard to see, especially the micro size. Course calcs are easier seen.
ULTRASOUND CORE BIOPSY U/S CORE BX SET-UP
U/S CORE BX PROCEDURE10 Ga Core Needle with VAD
U/S CORE BX PROCEDURE18 Ga Core Needle

2/15/2017
6
U/S CORE BX SPECIMENFrom an 18Ga core needle
• Ultrasound Core Bx– Allotted room time is 30 minutes.
– Obtaining the cores takes, on average, 5 minutes. With remainder time spent positioning and localizing the lesion.
– Results are available in 3-5 business days.
ULTRASOUND CORE BIOPSY
• Ultrasound Core Bx– Indications
• Pt has a suspicious mammogram/ultrasound/MRI documenting a mass or asymmetry.
• Pt has a palpable lesion
ULTRASOUND CORE BIOPSY
• Ultrasound Core Biopsy– Contraindications
• Pt is taking heart medication (procedure is post-poned)
• Pt has already been diagnosed with breast ca in the same breast.
• Pt is unable to withstand the procedure due to high anxiety or refusal of biopsy do to maybe denial.
ULTRASOUND CORE BIOPSY
STEREOTACTIC BX SPECIMEN STEREOTACTIC BX SPECIMEN

2/15/2017
7
LUMPECTOMY/SEGMENTAL MASTECTOMY• Partial breast surgery removing the cancer cells and claiming clean margins

2/15/2017
8
MASTECTOMIES
• 6 different kind of mastectomies
TREATMENT OPTIONSURGICAL OPTIONS• Six types of mastectomies are….
• Simple/total mastectomies
• Modified radical mastectomies
• Radical mastectomies
• Partial mastectomies
• Subcutaneous/nipple sparing mastectomies
• Skin-sparing mastectomies
TREATMENT OPTIONSURGICAL OPTIONS• Women who choose mastectomies have many reasons.
• Peace of mind
• Avoid radiation
• If tumor is larger than 4cm
• If breast is too small to have a lumpectomy.
• If pt had prior radiation therapy to the same breast
• Presence of connective tissue diseases such as scleroderma, vasculitis, lupus
• If patient is pregnant
• Pt cannot commit to 5-7 weeks of radiation
TREATMENT OPTIONSURGICAL OPTIONS• To establish a standard for lumpectomy margins, the American Society for Radiation Oncology
(ASTRO) and the Society of Surgical Oncology (SSO) reviewed a number of studies. The groups issued new guidelines saying that clear margins, no matter how small as long as there was no ink on the cancer tumor, should be the standard for lumpectomy surgery. The guidelines also say that wider margins don’t lower the risk of recurrence any more than narrower margins.

2/15/2017
9
TREATMENT OPTIONSURGICAL OPTIONS• The more breast tissue removed, the more likely it is there will be a change in the shape of the
breast afterward. If the breasts look very different after surgery, you might be able to have some type of surgery to improve the way the breast looks. Sometimes surgery is done on the other breast so the breasts look more alike. You should talk with your doctor before surgery to get an idea of how your breasts are likely to look afterward and to learn what your options might be.
WHAT DOES THIS MEAN?• FDA REQUIRED DISCLAIMER: The immunohistochemical, immunofluorescence, or in-situ hybridization
test included in report, were developed and their performance characteristics determines by either propath laboratory, North Texas Pathology Laboratories, Lakeview Pkwy, or Nacogdoches Medical Center. These test have not been cleared or approved by the US Food and Drug Administration (FDA). The FDA has determined that such clearance or approval is not necessary. These tests are used for clinical purposes, and should not be regarded as investigational or for research. Results should be interpreted with caution given the possibility of false negative results. Propath is certified under the clinical laboratory improvement amendments of 1988 as qualified to perform high complexity clinical laboratory testing.
• The information contained in this e-mail message may be privileged, confidential, and/or protected from disclosure. This e-mail message may contain protected health information (PHI); dissemination of PHI should comply with applicable federal and state laws. If you are not the intended recipient, or an authorized representative of the intended recipient, any further review, disclosure, use, dissemination, distribution, or copying of this message or any attachment (or the information contained therein) is strictly prohibited. If you think that you have received this e-mail message in error, please notify the sender by return e-mail and delete all references to it and its contents from your systems.
OLD DAYS….
• No malignant cells identifiedNo malignant cells identified. Benign ductal epithelial cells present 11/02/98
Screened screened by:NPC Verified by: , M.D.#754(Electronic Signature)
• COMMENT:Not applicableFellow/Staff: MHK/NCSR: 3 S
• SPECIMEN:Breast, Left Upper Inner Quadrant, Ultrasound-guided FNA
• GROSS DESCRIPTION:0.7 cm. nodule, 11 o'clock position, 8 cm. from nipple
• SNOMED CODES:M-00110 P-0000A T-04050Division of Pathology and Laboratory Medici
OLD DAYS…..
• (A) LEFT BREAST SUPERIOR MEDIAL MARGIN:Breast parenchyma, no tumor present.(B) REEXCISION OF BREAST SCAR AND TUMOR BED:Breast parenchyma with focal ductal epithelial hyperplasia andfibroadenomatoid changes.Fibrosis, foreign body giant cell reaction, granulation tissuefat necrosis consistent with previous biopsy site.No residual tumor present.Skin with suture granuloma. (C) DEEP MARGIN AND LEFT BREAST:Skeletal muscle, no tumor present
• 10/1998
FNA’S

2/15/2017
10
• Preprocedure Diagnosis:
• History of breast carcinoma
•
• Postprocedure Diagnosis:
• Unchanged
• Indication:
• Aspiration of a recurrent left breast seroma is requested for symptomatic relief.
• Title of Procedure:
• Percutaneous Image-Guided Seroma Aspiration
• IMPRESSION:
• Operative Findings:
• Successful percutaneous image-guided aspiration of approximately 80 mL of fluid from the left breast seroma.
•
• Consent: The procedure, risks, indications and alternatives were explained. All questions were answered and informed consent was obtained.
•
• I have reviewed the History and Physical dictated by the Mid-Level Practitioner/Fellow.
•
• Sedation/Anesthesia:
• None.•
• Procedure in Detail:
• A time out was performed prior to the start of the procedure and the correct patient, procedure, presence of consent, site, and side were confirmed with all members of the team.
• The patient was placed supine on the examination table and limited ultrasound performed of the left breast. This demonstrated a large seroma, consistent with the diagnostic ultrasound. The area was then prepped and draped in a sterile manner. Local
• anesthesia was administered with 1% lidocaine.
• An 18-gauge Chiba needle was then advanced under ultrasound guidance into the seroma. Approximately 80 mL of serous fluid was aspirated with no significant residual. The needle was then removed and hemostasis achieved.
• Additional Comments: None.
•
• Estimated Blood Loss: Minimal.
•
• Specimens Removed: Palliative only
•
• Immediate Complications: None.
MASTECTOMY PATHOLOGY READINGSurgical Pathology ReportFile under: Pathology******* MODIFIED REPORT - REVIEW ADDENDUM SECTION *******DIAGNOSIS(A) RIGHT AXILLARY SENTINEL LYMPH NODE #1, EXCISIONAL BIOPSY:MICROMETASTASIS PRESENT IN ONE OF ONE LYMPH NODE (0/1).IMMUNOHISTOCHEMICAL STAIN FOR PANCYTOKERATIN HIGHLIGHTS TUMOR.TUMOR FOCUS MEASURES 0.3 CM IN GREATEST SINGLE SLIDE DIMENSION. (SEE COMMENT 1)(B) RIGHT AXILLARY NONSENTINEL LYMPH NODE #1, EXCISIONAL BIOPSY:One lymph node, no tumor present (0/1).(C) RIGHT AXILLARY SENTINEL LYMPH NODE #2, EXCISIONAL BIOPSY:Two lymph nodes, no tumor present (0/2).Immunohistochemical stains for pancytokeratin are negative for metastatic carcinoma.(D) RIGHT AXILLARY SENTINEL LYMPH NODE #3, EXCISIONAL BIOPSY:One lymph node, no tumor present (0/1).Immunohistochemical stain for pancytokeratin is negative for metastatic carcinoma.(E) RIGHT BREAST, TOTAL MASTECTOMY:FOCI OF INVASIVE DUCTAL CARCINOMA, NOTTINGHAM HISTOLOGIC GRADE 2 (MODERATELYDIFFERENTIATED).
EXTENSIVE DUCTAL CARCINOMA IN SITU (DCIS), LOW TO INTERMIEDIATE TO HIGH-GRADE, CRIBRIFORM,PAPILLARY, MICROPAPILLARY, SOLID PATTERNS WITH ASSOCIATED COMEDONECROSIS ANDMICROCALCIFICATIONS. (SEE COMMENT 2)FOCI OF INVASIVE CARCINOMA MEASURES FROM 0.1 CM TO 1.2 CM IN LARGEST SINGLE SLIDEDIMENSION.MARGINS ARE WIDELY FREE, INVASIVE AND IN SITU CARCINOMA ARE PRESENT AT LEAST 1.0 CM FROMMARGIN.No lymphovascular invasion identified.Biopsy site changes present adjacent to invasive and in situ carcinoma.NIPPLE, INFILTRATING CARCINOMA PRESENT PREDOMINANTLY IN THE DERMIS AND FOCALLY IN THEEPIDERMIS.NIPPLE, DCIS INVOLVING DUCTS.Skin, no tumor present.Skeletal muscle, no tumor present.Nine lymph nodes, no tumor present (0/9).
(F) RIGHT AXILLARY SENTINEL LYMPH NODE #4, EXCISIONAL BIOPSY:One lymph node, no tumor present (0/1).Immunohistochemical stain for pancytokeratin is negative for metastatic carcinoma.COMMENT1) In specimen A, a minute focus of tumor is present in the H&E stained slide. Deeper levels are submitted forimmunohistochemical stain and highlight a 0.3 mm focus of tumor. The tumor is not evident in the frozen section slides.2) In specimen E, the DCIS is extensive and is present in the lower outer quadrant and lower importation of the specimen, anarea measuring at least 4.5 x 4.0 x 3.0 cm.Collected: 11/15/2013 Pathologist: Accession: S-13-090519Received: 11/15/2013 11:27 Case type: Surgical CasePage 2 of 4Surgical Pathology ReportFile under: PathologyThere is a spectrum of DCIS ranging from low grade micropapillary to higher grade solid and cribriform patterns withcomedonecrosis.CTA/elk

2/15/2017
11
PATHOLOGIC STAGE BASED ON PATHOLOGY MATERIAL REVIEWED IN THIS ACCESSIONPrimary tumor: pT1a but focal involvement of epidermisRegional lymph nodes: pN1miDistant metastases: pMx(American Joint Committee on Cancer, 7th Edition, 2010)GROSS DESCRIPTION(A) RIGHT AXILLARY SLN #1, COUNT 3400 – A 2.1 x 1.6 x 0.7 cm possible lymph node, serially sectioned. Submittedentirely.SECTION CODE: A1-A3, one possible lymph node, serially sectioned, submitted for frozen section diagnosis as wellas permanent evaluation. SJ/tlc*FS/DX: NO TUMOR PRESENT. CTA/elk(B) RIGHT AXILLARY NON-SENTINEL LYMPH NODE #1 – Received fresh is a yellow-tan single lymph node (1 x 1 x 0.5 cm).The specimen is bisected and entirely submitted in cassette B. ML/tlc*FS/DX: NO TUMOR PRESENT. CTA/elk
(C) RIGHT AXILLARY SLN #2, COUNT 600 – Two possible lymph nodes, 0.6 x 0.5 x 0.5 cm and 0.8 x 0.4 x 0.4 cm.Specimen is submitted entirely.SECTION CODE: C1, one possible lymph node, bisected, submitted for frozen section diagnosis as well aspermanent evaluation; C2, one possible lymph node bisected and submitted for frozen section diagnosis as well as permanentevaluation. SJ/tlc(D) RIGHT AXILLARY SENTINEL LYMPH NODE, COUNTS 330 – Received fresh is a yellow-tan lymph node (2 x 1 x 0.8cm). The specimen is serially sectioned and entirely submitted in cassette D. ML/tlc(E) RIGHT TOTAL MASTECTOMY PLUS NODES, SS- SUPERIOR, LS – LATERAL – A mastectomy specimen (35 x 21 x 6.5cm) oriented by the surgeon with a short stitch marking superior and a long stitch marking lateral. The specimen is surfaced byan oval-shaped portion of unremarkable, light tan skin (34 x 30 cm). The areolar is 3.5 cm in greatest diameter and the nippleis 1.6 cm in greatest diameter revealing a light gray, crusty nodule (0.3 cm in greatest diameter). The specimen was inked andserially sectioned from lateral to medial into eleven slices (nipple present on slice 5).On inferior of slice 4, an ill-defined, light gray and tan lesion (2.2 x 1.5 x 1.1 cm) surrounded by extensive areas offibrotic appearance. The lesion is located at 16 cm from superior, 3.4 cm from deep, 4.3 cm from the inferior resection marginsCollected: 11/15/2013 Pathologist: Accession: S-13-090519
Surgical Pathology ReportFile under: Pathologyand 2.8 cm from the skin. X-rays were requested confirming the lesion on slice 4 with a metal clip associated within the lesionon slice 4 and adjacent areas of interest on slices 3 (most lateral) and 5. X-rays also reveal suspicious calcifications on centralof slice 6. No other gross or radiological abnormalities were revealed. Remaining breast parenchyma was approximately 65%adipose tissue and 35% fibrous changes. Twenty-one possible lymph nodes were dissected from the axillary tail ranging from0.2 to 3 cm in greatest dimension.INK CODE: Blue – superior; orange – inferior; black – deep.SECTION CODE: E1, base of the nipple; E2, rest of the nipple from slice 5; E3, upper outer quadrant on slice 3; E4-E6, lateral to lesion, slice 3; E7, superior margin to the lesion on slice 4; E8, skin anterior to the lesion, slice 4; E9-E15, lesionon slice 4 (E9 correspond to metal clip site and E10, mirror to E9); E15, deep margin to the lesion, slice 4; E16, inferior marginto the lesion, slice 4; E17, area below the nipple on slice 5; E18-E21, medial to the lesion, slice 5, submitted from anterior todeep; E22, suspicious calcification with skin on slice 6; E23, E24, suspicious calcification on slice 6; E25, adjacent tosuspicious calcification most medial on slice 7; E26, upper inner quadrant on slice 7; E27, upper quadrant on slice 9; lymphnodes are submitted as follows: E28, one lymph node; E29, one lymph nodes; E30, two possible lymph
(F) RIGHT AXILLARY SENTINEL LYMPH NODE #4, COUNTS 220 – Received fresh is a yellow-tan single lymph node (0.4 x0.4 x 0.2 cm). The specimen is bisected and entirely submitted in cassette F. ML/tlcBIOMARKER TESTINGE6CLINICAL HISTORYNone given.SNOMED CODEST-D04050, M-85003"Some tests reported here may have been developed and performance characteristics determined by Pathology and Laboratory Medicine.These tests have not been specifically cleared or approved by the U.S. Food and Drug Administration."Entire report and diagnosis completed by: MD 10650 Nov 21, 2013Surgical PathologyReportDepartment of Pathology, Box 85Tel: 713-792-3205 Fax: 713-794-46301037898Collected: 11/15/2013 Pathologist: Accession: S-13-090519Received: 11/15/2013 11:27 Case type: Surgical Case
DIFFERENT TYPE OF MASTECTOMY

2/15/2017
12
• DIAGNOSIS
• (A) LEFT AXILLA, SENTINEL LYMPH NODE #1, EXCISION:
• MICROMETASTASIS IN ONE OUT OF THREE LYMPH NODES.
• THE LARGEST TUMOR DEPOSIT MEASURING 1.5 MM IN DIAMETER.
• No extranodal extension present.
• (B) LEFT BREAST, LOW AXILLARY LYMPH NODES, NIPPLE SPARING MASTECTOMY:
• INVASIVE DUCTAL CARCINOMA, INTERMEDIATE NUCLEAR GRADE, NOTTINGHAM HISTOLOGIC GRADE 2 (MODERATELY DIFFERENTIATED), TWO FOCI IN CLOSE DISTANCE, MEASURING 3.2 CM AND 0.5 CM IN MAXIMUM DIMENSIONS, RESPECTIVELY, ASSOCIATED WITH BIOPSY SITE CHANGES.
• ASSOCIATED DUCTAL CARCINOMA IN SITU (DCIS), INTERMEDIATE NUCLEAR GRADE, PAPILLARY, MICROPAPILLARY AND CRIBRIFORM PATTERNS, WITHOUT NECROSIS.
• No lymphovascular invasion identified.
• INVASIVE CARCINOMA SEEN AT THE SHAVED AREOLAR NIPPLE COMPLEX MARGINS AT 12 O’CLOCK AND 6 O’CLOCK REGIONS AND 1 MM AWAY FROM THE CLOSEST ANTERIOR TISSUE EDGE IN THE OUTER UPPER BREAST. (SEE COMMENT)
• The remaining resection margins free of invasive carcinoma or DCIS.
• Mild fibrocystic changes present, including fibroadenomatoid changes and fibrosis.
• Seven lower axillary lymph nodes, no tumor present (0/7).
(C) LEFT BREAST, ADDITIONAL ANTERIOR MARGIN, EXCISION:Benign breast tissue, no tumor present.(D) LEFT BREAST, TISSUE AT BASE OF NIPPLE, EXCISION:Benign breast tissue, no tumor present.(E) LEFT BREAST, BASE OF NIPPLE MARGIN #2, EXCISION:Benign breast tissue, no tumor present.(F) LEFT BREAST, ADDITIONAL LATERAL TISSUE, EXCISION:Predominantly benign fibroadipose tissue, no tumor present.(G) LEFT BREAST, FINAL INFERIOR MARGIN, EXCISION:Benign breast tissue, no tumor present.(H) LEFT BREAST, SKIN EDGE, EXCISION:Skin, no tumor present.mast
(A) RIGHT SOFT TISSUE, CORE NEEDLE BIOPSY:METASTATIC OSTEOCHONDROMATOUS MALIGNANCY, HIGH GRADE (SEECOMMENT)COMMENTImmunohistochemical stains performed at ---- show that the tumor cells arepositive for SOX-9, SATB2 and pankeratin(rare cells) and are negative for GATA-3. Ki-67 highlights a proliferation index of30%.Microscopically, the tumor has features of a high grade chondroblasticosteosarcoma but in view of the patient’s history thismost likely represents a metastasis from this patient’s known metaplastic breastcarcinoma with osteosarcomatous component.
STEREOTACTIC PATHOLOGY REPORT

2/15/2017
13
• A) LEFT BREAST, 9 O'CLOCK, STEREOTACTIC CORE BIOPSY:
• DUCTAL CARCINOMA IN SITU, HIGH GRADE, MICROPAPILLARY, SOLID AND CRIBRIFORM TYPES, WITH
• COMEDONECROSIS AND ASSOCIATED MICROCALCIFICATIONS.
• Sclerosed atypical intraductal papilloma with associated microcalcifications.
• Florid usual ductal hyperplasia.
• GROSS DESCRIPTION
• (A) LEFT BREAST 9 O'CLOCK – Consists of six fibrofatty cores, ranging from 1.5 to 2.4, four of the cores are received in a
• pink cassette.
• SECTION CODE: A1-A2, each contain two cores from cassette; A3, two additional cores. BM/tlc
• BIOMARKER TESTING
• Primary
• Tumor Block: A1
• CLINICAL HISTORY
• None given.
• SNOMED CODES
• T-04050, M-85002, M-80570
• "Some tests reported here may have been developed and performance characteristics determined by Pathology and Laboratory Medicine.
• DOB: 4/2/1949 Age: 67 Sex: F
• Physician: B
• Collected: 5/6/2016 Pathologist: Accession: S-16-026754
• Received: 05/06/2016 15:02 Case type: Surgical Biopsy
• Page 2 of 2
• Surgical Pathology Report
• File under: Pathology
• Specimens Involved
• Specimens: A: left breast 9:00
• Immunohistochemical staining is performed in our lab on a representative paraffin-embedded section.
• Block: A1
• Estrogen Receptor
• Antibody clone: 6F11 (Novacastra)
• Positive 10 - 100% Low Positive 1-9%
• Estrogen Receptor Results: Positive
• Estrogen Receptor Percent Staining: 100%
• Estrogen Receptor Staining Intensity: Strong
• Progesterone Receptor
• Antibody clone: PgR1294 (DAKO)
• Positive 10 - 100% Low Positive 1-9%
• Progesterone Receptor Results: Positive
• Progesterone Receptor Percent Staining: 95%
• Progesterone Receptor Staining Intensity: Strong
SPECIMENS
FootnoteBreast specimens used for determining prognostic / predictive markers arefixed in formalin for at least 6 hours and generally less than 48 hours, butformalin fixation exceeds 48 hours on holidays and weekends.If the specimen has been fixed for longer than 72 hours, a negative Her 2immunohistochemical (IHC) result may theoretically represent a falsenegative, although studies have shown that specimens can be fixed for aslong as 2 weeks without affecting IHC staining results. Therefore, anegative result should be verified by additional tests on alternative samplesif appropriate. Reference Arber et al. Appl. Immunohistochem. Mol Morp2005; 13; 283-286.
PATHOLOGY REPORT SEGMENTAL
• With Addendum
Collected: 4/9/2013 Accession: S-13-028336Received: 04/09/2013 17:06 Case type: Surgical CasePage 1 of 5Surgical Pathology ReportFile under: Pathology******* MODIFIED REPORT - REVIEW ADDENDUM SECTION *******DIAGNOSIS(A) BREAST, LEFT, SEGMENTAL MASTECTOMY AT 10 O'CLOCK:Sclerosed fibroadenoma with stromal calcifications.Predominantly fibrofatty tissue.Additional deeper sections pending to investigate second, smaller site of calcifications in slice #5 will be reported as anaddendum(B) BREAST, LEFT, SEGMENTAL MASTECTOMY AT 6 O'CLOCK:VIABLE RESIDUAL INVASIVE CARCINOMA PRESENT IN TREATED TUMOR BED (SEE COMMENT).TUMOR BED MEASURES 3.5 x 2.6 CM.TUMOR CELLULARITY IS 40%.DUCTAL CARCINOMA IN SITU IS MINIMALLY PRESENT (1%).RESIDUAL INVASIVE CARCINOMA MEASURES 3.5 CM IN GREATEST EXTENT.INVASIVE CARCINOMA IS LESS THAN 0.1 CM TO SUPERIOR AND POSTERIOR MARGINS FROM MIDSPECIMEN TO MEDIAL MARGIN.Ductal carcinoma in situ is present 0.2 cm to inferior margin at medial aspect.Invasive carcinoma is 0.5 cm to anterior margin.LYMPHOVASCULAR INVASION IDENTIFIED
(C) BREAST, LEFT 6 O'CLOCK, ADDITIONAL SUPERIOR MARGIN:INVASIVE CARCINOMA PRESENT.Invasive carcinoma is 0.7 cm to new superior margin.Ductal hyperplasia without atypia.(D) BREAST, LEFT 6 O'CLOCK, ADDITIONAL MEDIAL MARGIN:Benign breast tissue.Negative for carcinoma.(E) BREAST, LEFT 6 O'CLOCK, ADDITIONAL POSTERIOR MARGIN:Benign breast tissue.Negative for carcinoma.(F) LYMPH NODE, LEFT AXILLA, SENTINEL LYMPH NODE #1:One lymph node, negative for carcinoma (0/1).(G) BREAST, LEFT 10 O'CLOCK, ADDITIONAL ANTERIOR AND INFERIOR MARGIN:Predominantly fibrofatty tissue.Negative for carcinoma.

2/15/2017
14
PATHOLOGIC STAGE BASED ON PATHOLOGY MATERIAL REVIEWED IN THIS ACCESSIONPrimary tumor: y pT2Regional lymph nodes: sn y pN0Collected: 4/9/2013 Pathologist: Accession: S-13-028336Received: 04/09/2013 17:06 Case type: Surgical CasePage 2 of 5Surgical Pathology ReportFile under: PathologyDistant metastases: y pMx(American Joint Committee on Cancer, 7th Edition, 2010)COMMENTPrognostic evaluation of residual cancer burden (RCB) is calculated using the RCB index of Symmanset al. (W. FraserSymmans, Florentia Peintinger, Christos Hatzis, Radhika Rajan, Henry Kuerer, Vicente Valero, Lina Assad, Anna Poniecka,Bryan Hennessy, Marjorie Green, Aman U. Buzdar, S. Eva Singletary, Gabriel N. Hortobagyi, and Lajos Pusztai, “ Measurementof Residual Breast Cancer Burden to Predict Survival After Neoadjuvant Chemotherapy”, 2007, J ClinOncol 25:4414-4422). Thispatient’s RCB index is2.134, corresponding to an RCB-II prognosis category and based on tumor bed dimensions of 35 by 26 mm,cellularity of residual viable carcinoma estimated as 40%, estimated 1% of residual tumor burden is due to ductal carcinoma in situ, and no
Specimen Type: Excision with wire-guided localizationLaterality: LeftTumor Site: 6 o’clockSize of Invasive Component: 3.5 cmHistologic Type: Invasive Ductal CarcinomaHistologic Grade : IIITubule Formation Score: 3Nuclear Pleomorphism Score: 3 (cannot exclude treatment effect)Mitotic Score: 3Total Nottingham Score: 9DCIS: PresentPathologic Staging (pTNM) see aboveMargins: Final Margins NegativeExtent of Margin Involvement for Invasive Carcinoma: N/AExtent of Margin Involvement for DCIS: N/AVenous/Lymphatic (Large/Small Vessel) Invasion (V/L): PresentLymph Node Sampling: Sentinel Lymph NodeNumber of Sentinel Lymph Nodes Sampled: 1
Number Of Non-Sentinel Lymph Nodes Sampled: 0Number Of Lymph Nodes with Macrometastases 0Number Of Lymph Nodes with Micrometastases 0Number Of Lymph Nodes with Isolated Tumor Cells 0Number of Lymph Nodes without Tumor Cells Identified 1Prognostic marker studies were previously reported (see S12-65931)Collected: 4/9/2013 Pathologist: Accession: S-13-028336Received: 04/09/2013 17:06 Case type: Surgical Case
Surgical Pathology ReportFile under: Pathology(A) LEFT BREAST 10 O'CLOCK CALCIFICATIONS, SHORT STITCH SUPERIOR, LONG STITCH LATERAL - An orientedleft breast segmental mastectomy that has overall dimensions of 6.5 x 4.2 x 2.5 cm. The specimen is oriented with a doubleshort stitch that marks the superior margin and double long stitch that marks the lateral margin. The specimen is seriallysectioned medial to lateral in eight consecutive cross sections to reveal approximately 75% yellow adipose tissue and 25%gray-white fibrous tissue. Radiographs reveal microcalcifications present in slice 5 as well as slice 9. No definite mass ispalpated or visualized. No lymph nodes are present.INK CODE: Blue - superior margin; green - inferior margin; yellow - anterior margin; black - posterior margin; red -medial and lateral margins.SECTION CODE: A1, medial margin, perpendicular section; A2, anterior inferior margin, perpendicular section, slice 4;A3, posterior inferior margin, perpendicular section, slice 4; A4, superior margin, perpendicular sections, slice 5; A5, midsection to include anterior and posterior margins, perpendicular section; A6, most inferior margin, perpendicular sections, slice5; A7, superior one-half margin, perpendicular section, slice 6; A8, inferior one-half margin, perpendicular sections, slice 6; A7,
lice 9 to include microcalcifications; A8, entire lateral margin, perpendicular section. DA/elk*IOA/DX: CALCIFICATIONS IDENTIFIED IN LATERAL 1/3 OF SPECIMEN AND ARE PRESENT ATANTERIOR/INFERIOR MARGIN. MEE/tlc(B) LEFT BREAST, 6 O'CLOCK - A portion of fibrofatty tissue measuring 7.0 x 5.5 x 4.0 cm with a short stitch marking thesuperior aspect and a long stitch at lateral. There are two wires emanating from the specimen. The specimen is inked andsubsequently sliced into seven slices from medial to lateral. Inking is as per the standard protocol which is blue - superior,green - inferior, medial and lateral - red, anterior - yellow and posterior black. Upon sectioning, the tumor is identified in slices 2and 3 measuring 2.6 x 1.7 x 1.0 cm. It abuts the superior and posterior margins at the medial aspect. It grossly approachesthe anterior margin at 5.0 mm. The inferior margin is greater than 1.0 cm. MEE/elkSECTION CODE: B1, B2, medial margin, perpendicular section; B3-B5, entire slice 2, superior to inferior includingmargins, perpendicular section; B6-B9, entire slice 3 to include margins, perpendicular sections; B10-B15, entire slice 4 toinclude margins, superior to inferior in consecutive order; B16, B17, superior two thirds to include slice 5 to include margins,perpendicular section; B18, lateral margin, perpendicular section. DA/elk*IOA/DX: TUMOR ABUTS SUPERIOR/POSTERIOR MARGINS NEAR MEDIAL ASPECT. MEE/tlc
(C) LEFT BREAST, 6 O'CLOCK ADDITIONAL SUPERIOR MARGIN, CLIPS MARKS TRUE MARGIN -Fatty breast tissue (3.4x 1.9 x 1.1 cm). There is a clip on one side. Serial sectioning of the specimen reveals a yellow lobulated breast tissue.INK CODE: Black ink - true margin.SECTION CODE: C1-C4, specimen serially sectioned and entirely submitted. ED/elk(D) LEFT BREAST, 6 O'CLOCK, ADDITIONAL MEDIAL MARGIN, CLIPS MARKS TRUE - Fatty tissue (3.6 x 2.2 x 1.1 cm).There is a clip on one side of the specimen that designating the true margin. Serial sections of the specimen reveals lobulatedyellow fatty tissue.INK CODE: Black ink - true margin.SECTION CODE: D1-D4, specimen serially sectioned and entirely submitted.(E) LEFT BREAST, 6 O'CLOCK, ADDITIONAL POSTERIOR MARGIN, CLIP MARKS TRUE MARGIN -Fatty tissue (3.6 x 1.9x 0.9 cm). There is a clip on one side designating true margin. Serial sectioning of the specimen reveals lobulated fatty yellowtissue.INK CODE: Black ink - true margin.

2/15/2017
15
(F) LEFT AXILLARY SENTINEL LYMPH NODE #1, BLUE, IN VIVO; 11, EX VIVO 69 - A single irregular piece of fibrofattytissue measuring 4.5 x 1.8 x 0.9 cm. Grossly, there appears to be a thin, pink-red rim of lymphoid tissue at the periphery andgrossly is suggestive of a fatty replaced lymph node which will be entirely submitted in consecutive order.SECTION CODE: F1FS-F11FS, one serially sectioned fatty replaced lymph node in consecutive order. DA/elkCollected: 4/9/2013 Pathologist: Accession: S-13-028336Received: 04/09/2013 17:06 Case type: Surgical CasePage 4 of 5Surgical Pathology ReportFile under: Pathology*FS/DX: ONE LYMPH NODE, NEGATIVE FOR CARCINOMA. MEE/tlc(G) LEFT BREAST 10 O'CLOCK, ADDITIONAL ANTERIOR AND INFERIOR MARGIN, CLIPS MARKS TRUE ANTERIORMARGIN - Fatty breast tissue (3.4 x 2.2 x 1.1 cm). There is a clip designating the true margin. Serial sectioning of thespecimen reveals lobulated yellow fatty tissue.INK CODE: Black ink - true margin.
BIOMARKER TESTINGPrimaryTumor Block: B3CLINICAL HISTORYNone given.SNOMED CODES"Some tests reported here may have been developed and performance characteristics determined by Pathology and Laboratory Medicine.These tests have not been specifically cleared or approved by the U.S. Food and Drug Administration."Entire report and diagnosis completed by: Mary MD, PhD 11608 Apr 15, 2013DOB: 1/4/1963 Age: 50 Sex: FPhysician: Henry Collected: 4/9/2013 Pathologist: Accession: S-13-028336Received: 04/09/2013 17:06 Case type: Surgical Case
ADDENDUMThis modified report is being issued to report additional diagnostic information.Deeper levels of Section A5 from the Left Breast Segmental Mastectomy at 10 o’clock were examined for calcifications inaddition to those already reported (see above). None were identified and the diagnosis is unchanged.Entire report and diagnosis completed by: Mary E. MD, PhD 11608 Apr 16, 2013
HAVE A HAPPY NEW YEAR