Embed Size (px)
Citation preview

1
1MPI for Biological Cybernetics
2Stanford University3Werner Reichardt Centre for Integrative Neuroscience
Eberhard Karls University Tuebingen
Epidural ECoG Online Decoding of Arm Movement Intention in Hemiparesis
M. Gomez-Rodriguez1,2 M. Grosse-Wentrup1
J. Peters1 G. Naros3 J. Hill1 B. Schölkopf1 A. Gharabaghi3
ICPR Workshop in Brain Decoding, August 2010

2
BCI for Neurorehabilitation
A Brain Computer Interface (BCI) for neurorehabilitation of:Hemiparetic syndromes due to cerebrovascular, traumatic or tumor-related brain damage.
may outperform traditional therapy → Hebbian rule-based [1]
1. Instantaneous feedback:Synchronize subject’s attempt and feedback
2. High accuracy:User’s control of the BCI
3. High specificity:To focus on specific areas of the cortex
4. Limited invasiveness
Challenges

3
EECoG for Neurorehabilitation
BCI with Epidural Electrocorticography (EECoG) may be a promising tool for neurorehabilitation.
Instantaneous feedback: Delays in the order of ms.
Why EECoG for neurorehabilitation?
High accuracy: On-line decoding of arm movement intention.High specificity: Greater spatial resolution over motor cortex.
Limited invasiveness: Safer alternative to intraparenchymal electrodes or subdural devices.
Previous studies [2, 3]: Off-line real movement and motor imagery classification and real movement direction decoding using subdural ECoG with epileptic patients.
In our work:On-line movement attempt classification using epidural ECoG with a stroke patient.
4
Outline
We present a Case Study (one patient) of a BCI with Epidural Electrocorticography (EECoG):
1. Experimental Setup:Human subject, task and recording
2. Methods:Signal processing and on-line decoding techniques
3. Results:Spatial and frequency features and classification performance
4. Conclusions
5
Experimental Setup
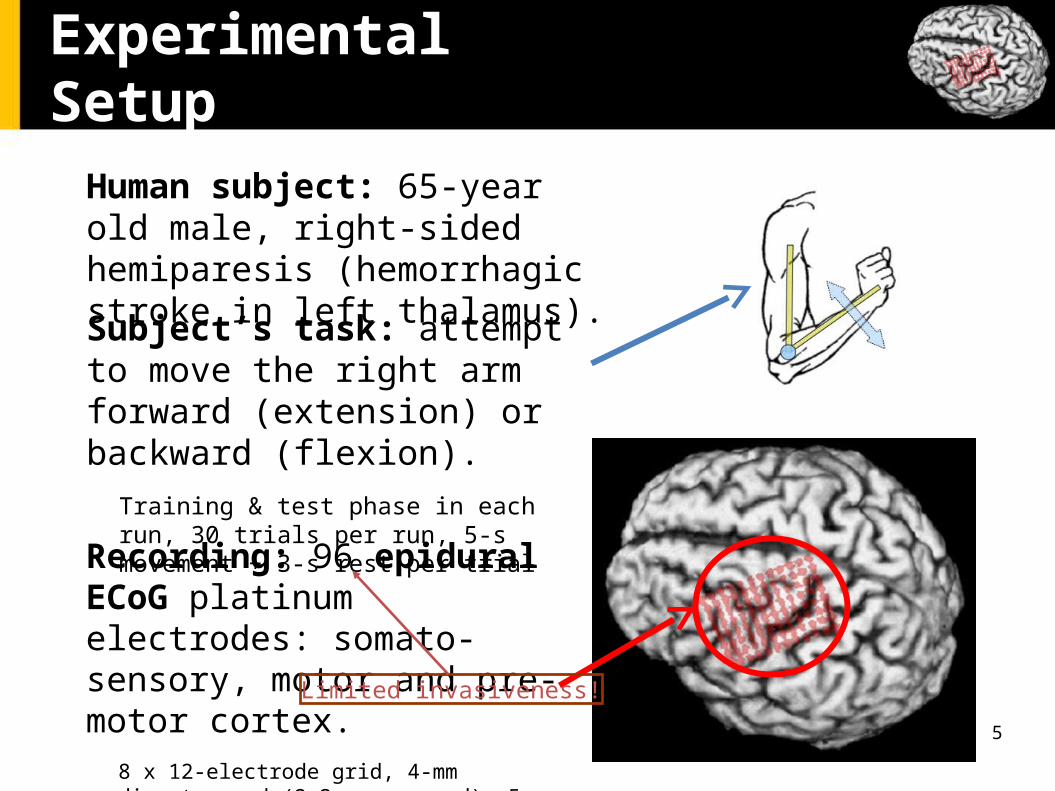
Recording: 96 epidural ECoG platinum electrodes: somato-sensory, motor and pre-motor cortex.
8 x 12-electrode grid, 4-mm diameter pad (2.3 mm exposed), 5-mm interelectrode distance.
Human subject: 65-year old male, right-sided hemiparesis (hemorrhagic stroke in left thalamus).
Subject’s task: attempt to move the right arm forward (extension) or backward (flexion).
Training & test phase in each run, 30 trials per run, 5-s movement + 3-s rest per trial
Limited invasiveness!

6
Methods (Signal Processing)
Common-Average Reference (CAR), band-pass filtering (2-115Hz) & notch filtering (50 Hz power-line).
Average power spectral densities over 2Hz frequency bins for each electrode are used as features. Welch’s method over overlapping incrementally bigger time
segments each 5-s movement or 3-s resting periods.
Larger segments → Less noise and more reliable estimates. Shorter segments → Necessary for on-line feedback.

7
Methods (On-line Decoding)
On-line classification (every 300ms) between movement and resting using spectral features:
Visual on-line feedback is provided
A linear support vector machine (SVM) is generated on-line after a training period (15 seconds of each condition)
8
Results (Spatial and Spectral Features)
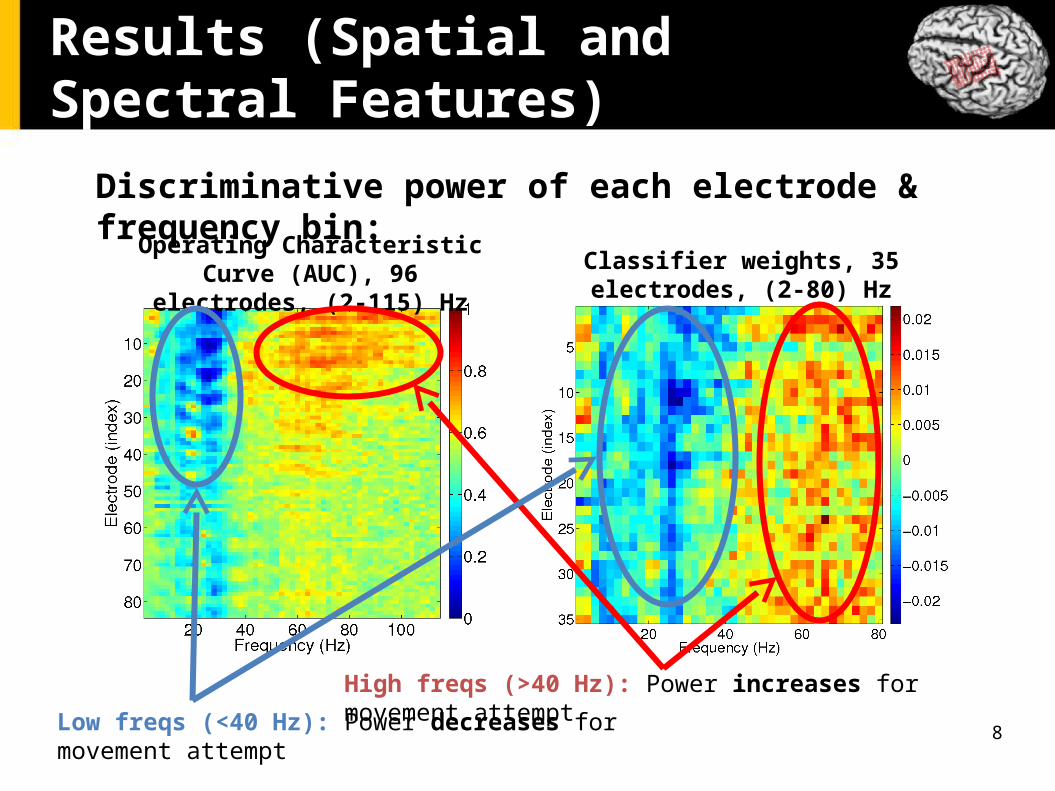
Discriminative power of each electrode & frequency bin:
Operating Characteristic Curve (AUC), 96 electrodes, (2-115) Hz Classifier weights, 35 electrodes, (2-80)
Hz
Low freqs (<40 Hz): Power decreases for movement attempt
High freqs (>40 Hz): Power increases for movement attempt

9
Results (Spatial and Spectral Features)
To see discriminative power of each spatial location better:Average AUC for each electrode over:
Low freqs (2 - 40 Hz) High freqs (40 - 80 Hz)
High Specificity!

10
Results (Performance)
On-line decoding of movement intention based on different frequency bands: (2, 40), (40, 80) and (2, 80) Hz
High Accuracy!
11
Conclusions
We showed the feasibility of epidural ECoG for BCI-based rehabilitation devices for hemiparetic patients
Future work (in progress): EECoG on-line decoding + haptic feedback provided by a robot arm guiding
patient’s arm: See already workshop paper at SMC’10 [4] on robot-based haptic feedback using EEG on-line
decoding on healthy subjects.
Instantaneous feedback: delay of 300 ms.
High accuracy: > 85 % in arm movement intention decoding.High specificity: Cortical reorganization caused by the stroke.
Limited invasiveness

12
References
[1] T. H. Murphy, and D. Corbett. Plasticity during stroke recovery: from synapse to behaviour. Nature Review Neuroscience 2009, 10-12, 861-872.
[2] T. Pistohl, T. Ball, A. Schulze-Bonhage, A. Aertsen, and C. Mehring. Prediction of arm movement trajectories from ECoG-recordings in humans. Journal of Neuroscience Methods 2008, Vol. 167-1, 105-114
[3] G. Schalk, J. Kubanek, K.J. Miller, N.R. Anderson, E.C. Leuthardt, J.G. Ojemann, D. Limbrick, D. Moran, L.A. Gerhardt, and J.R. Wolpaw. Decoding two-dimensional movement trajectories using electrocorticographic signals in humans. Journal of Neural Engineering 2007, 4-264.
[4] M. Gomez-Rodriguez, J. Peters, J. Hill, B. Schölkopf, A. Gharabaghi, and M. Grosse-Wentrup. Closing the Sensorimotor Loop: Haptic Feedback Facilitates Decoding of Arm Movement Imagery. SMC Workshop in Shared-Control for BMI, 2010.