Embed Size (px)
Citation preview

1 |
Methods for costing NCD prevention and control
Methods for costing NCD prevention and control
Workshop on Country Perspectives on Workshop on Country Perspectives on Decision Making for control of chronic diseasesDecision Making for control of chronic diseases
Institute of Medicine of the National Academies July 19-21, 2011Institute of Medicine of the National Academies July 19-21, 2011
Karin Stenberg, Department of Health Systems FinancingKarin Stenberg, Department of Health Systems Financing

2 |
AcknowledgementsAcknowledgements
The analysis was led by Dr Dan Chisholm, Dr Dele Abegunde and Dr Shanthi Mendis of World Health Organization, with contributions from many WHO experts.
The support and contribution of the American Cancer Society to this work is gratefully acknowledged.
For tobacco costing, the contributions of Dr Ioana Popovici of Nova Southeastern University and Professor Michael French of the University of Miami were funded by Bloomberg Philanthropies and the World Lung Foundation, while the time and contributions of Judith Watt was funded by the Framework Convention Alliance.

3 |
Economic evidence for NCD prevention & control – a story with 3 parts –
Economic evidence for NCD prevention & control – a story with 3 parts –
1. Economic burden (the size of the problem): Micro-economic impact (at level of households and firms) Macro-economic impact (at aggregate level of society)
2. Priorities for investment (potential solutions): Synthesis of available cost-effectiveness evidence Identification of 'best buys' for low- and middle-income countries
3. Costs of scaled up action (financial 'price tag'): Resource needs associated with enhanced coverage / implementation Budgetary gaps and implications

4 |
Cost of scaling-up for NCDs: immediate and future stepsCost of scaling-up for NCDs: immediate and future steps
1. Global 'price tag' for all Low and Middle Income Countries (LAMIC) (for input into NCD summit;
Sept 2011)– a financial planning tool for scaled-up delivery of a defined set of population-wide and individual health care
interventions.
2. Country-level use / contextualization (for national planning; 2011-2012)
3. Incorporation into OneHealth (for integrated health system planning; 2012)
4. Modelling of health gains / return on investment (impact analysis; 2012 ?)

5 |
What to scale up?What to scale up?
1. Scope (WHO NCD action plan): Risk factors: tobacco & (harmful) alcohol use; unhealthy diet & physical inactivity Diseases: CVD and diabetes; cancers; respiratory disorders (asthma, COPD)
2. 'Best buys': Interventions that are very cost-effective but also feasible, low-cost and
appropriate to implement within the constraints of the local health system 'Very cost-effective' = one year of healthy life is obtained for less than average
annual income per person [GDP per capita] Interventions that do not meet all of these criteria - but which still offer good
value for money and have other attributes that recommend their use – can be considered as 'good buys' (we also cost this expanded intervention set)

6 |
Summary of 'best buys'Summary of 'best buys'
ConditionInterventions
Tobacco use (4)Tax increases; smoke-free indoor workplaces & public places; health information / warnings; advertising/promotion bans
Alcohol use (3)Tax increases; restrict retail access; advertising bans
Unhealthy diet & physical inactivity
(3)
Reduced salt intake; replacement of trans fat with polyunsaturated fat; public awareness about diet & physical
activity
CVD & diabetes (2)Counselling & multi-drug therapy (including glycaemic control for diabetes) for people with >30% CVD risk (including those with
CVD); treatment of heart attacks with aspirin
Cancer (2)Hepatitis B immunization to prevent liver cancer; screening & treatment of pre-cancerous lesions to prevent cervical cancer
2008-2013 Action Plan for the WHO Global Strategy for the Prevention and Control of Noncommunicable Diseases
Addressing population risk factors
Primary care

7 |
Estimating the cost of scale up: information neededEstimating the cost of scale up: information needed
ParameterDefinitionData source(s)PopulationTotal population of countryUN population division statistics
Prevalence% of population with disease / risk factor exposure (by age & sex)
Global burden of disease estimates: Comparative Risk Assessment study NCD surveillance (e.g. Infobase)
Coverage% of population in need in receipt of intervention
Current coverage: Survey data Target coverage: expert consensus
Resource useResources needed to implement intervention
Treatment protocols, costing studies
Unit cost / price
Cost per unit/item of resource use
Drug prices from MSH; WHO costing data base (CHOICE) – e.g., salaries, media costs, per diems, etc.

8 |
Estimating the global cost of scale up: 2011 study produces a more extensive estimate
Estimating the global cost of scale up: 2011 study produces a more extensive estimate
Parameter2007
(Lancet chronic disease series)
2011
(forthcoming WHO report)
Countries23 (80% of LAMIC burden)42 (90% of LAMIC burden)
Scale-up period (price year)
2006-2015 (in 2005 prices)2011-2025 (in 2008 prices)
NCDs / risk factorsTobacco use; high BP; CVDAll elements of NCD action plan (4 risk factors, 4 diseases)
InterventionsTobacco control measures (4); salt reduction (1); multi-drug
therapy for those at high risk (1)
Core set: all 'best buys' (14) Expanded set: range of 'good buys'

9 |
Different implementation time in different contexts, depending on existing health system and policy environment
Different implementation time in different contexts, depending on existing health system and policy environment
Scale up of activities for population interventions
(policy implementation) :Scale up of patient interventions
Based on available assessment of current enforcement or 'performance' of countries with respect to e.g.,
tobacco control policy ,alcohol control policy.4 stages of policyimplementation:
•Planning stage (year 1) •Policy development (year 2)
•Partial implementation (year 3-5) •Full implementation (year 6 onwards)

10 |
Resource needs matrix for NCD policy instrumentsResource needs matrix for NCD policy instruments
Stage of policy development
Human resources
TrainingMeetingsMass mediaSupplies & equipment
Other
Planning (year 1)
Program management; administration
Strategy / policy analysis
StakeholdersOffice equipment
Baseline survey
Development (year 2)
Advocacy; lawLegislationIntersectoral collaboration
Awareness campaigns
Opinion poll
Partial implementation (years 3-5)
InspectionRegulationMonitoringCounter-advertising
Vehicles, fuel
Full implementation (year 6 onwards)
EnforcementEvaluationFollow-up survey

11 |
Cost of scaling up : Illustrative exampleCost of scaling up : Illustrative example
A 20% rate of prevalence of smoking in a total population of 1 million persons would give a population in need of 200,000 individuals. All these individuals could benefit each year from
a brief intervention in primary care that, say, costs $1 per case to deliver .
• Cost of current coverage: If coverage of the brief intervention was currently only 10%, the total annual cost would be $20,000 (200,000 * 10% * $1).
• Cost of target coverage: If scaled up to a higher desired level of coverage (such as 50%), the total cost in that future year will jump five-fold to $100,000.
• Incremental cost: Difference between the current and target level of coverage ($80,000).
• Cost per capita: Division of total or incremental costs by total number of people in the population (annual cost per person would rise from $0.02 to $0.10, an increment of $0.08).

12 |
Costing population interventions (example)Costing population interventions (example)

13 |
Costing primary care services Ingredient-based costing, specific by level
Costing primary care services Ingredient-based costing, specific by level

14 |
Costing primary care services (contd.)Costing primary care services (contd.)

15 |
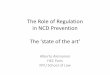
Modeled costs indicate variability of resource needs for scaling up NCD interventions
Modeled costs indicate variability of resource needs for scaling up NCD interventions
Median annual cost per capita of tobacco control, 2011-2025
$-
$0.05
$0.10
$0.15
$0.20
$0.25
$0.30
$0.35
$0.40
$0.45
$0.50
Low-income countries(N=14)
Lower middle-incomecountries (N=13)
Upper middle-incomecountries (N=15)
Cost
per
cap
ita (I
$)
Lower IQRMinMedianMaxUpper IQR

16 |
Cost of scaling up NCD prevention: population-based tobacco and salt reduction strategies
(Source: Asaria et al, Lancet 2007)
Cost of scaling up NCD prevention: population-based tobacco and salt reduction strategies
(Source: Asaria et al, Lancet 2007)
Over 10 years (2006–2015), 13·8 million deaths could be averted

17 |
Strengths and limitationsStrengths and limitations
STRENGTHS
Comprehensive assessment of 'best buys' and 'good buys'
Standard methodology used by WHO to derive global 'price tags' and country costing spreadsheets (similar to TB, malaria, child health, etc).
Ingredients based (Quantity x Price ) – easy for countries to review and validate
Assessment of current policies and health system as starting point
LIMITATIONS
Lacks assessment of health gains; does not model changes in epidemiology over time as preventive interventions are scaled up.
May need to be expanded to cover a broader intervention set for country planning.
Does not model health system investment needs.
Financial sustainability assessment needs to be done separately.

18 |
Next stepsNext steps
Report on global price tag launched before UNGASS Sept summit
NCD cost templates available for countries to validate and use
Integration of NCD module into OneHealth tool
will need to consider broader package, including other renal and liver diseases, gastrointestinal diseases, and mental disorders
Develop model for analysis of health impact

19 |
Additional slides

20 |

21 |
Estimating the cost of NCD scale up (2011) - 42 countries(each > 20m popn; together, account for 90% NCD LAMIC burden)
Estimating the cost of NCD scale up (2011) - 42 countries(each > 20m popn; together, account for 90% NCD LAMIC burden)
Low-income countries (14)
Afghanistan; Bangladesh; Côte d'Ivoire; DPR Korea; DR Congo; Ethiopia; Ghana; Kenya; Myanmar; Nepal; Nigeria; Sudan; Uganda; Tanzania
Lower-middle income countries (13)
China; Egypt; India; Indonesia; Iraq; Morocco; Pakistan; Philippines; Sri Lanka; Ukraine; Uzbekistan; Viet Nam; Yemen
Upper-middle income countries (15)
Algeria; Argentina; Brazil; Colombia; Iran; Kazakhstan; Malaysia; Mexico; Peru; Romania; Russian Federation; South Africa; Thailand; Turkey; Venezuela