Embed Size (px)
Citation preview

E311
Med Oral Patol Oral Cir Bucal 2007;12:E311-6. Microsurgery Med Oral Patol Oral Cir Bucal 2007;12:E311-6. Microsurgery
The application of microscopic surgery in dentistry
Manuel García Calderón 1, Daniel Torres Lagares 2, Carmen Calles Vázquez 3, Jesús Usón Gargallo 4, José Luis Gutiérrez Pérez 5
(1) Associate Professor of Oral Surgery – University of Seville (2) Assistant Professor of Oral Surgery – University of Seville (3) Professor – Minimally Invasive Surgery Center - Cáceres(4) Director – Minimally Invasive Surgery Center - Cáceres(5) Head Professor of Oral Surgery – University of Seville
Correspondence:Dr. Daniel Torres LagaresFacultad de Odontología. Universidad de Sevilla.C/ Avicena s/n 41009 SevillaE-mail: [email protected]
Received: 25-09-2006Accepted: 10-04-2007
García-Calderón M, Torres-Lagares D, Calles-Vázquez C, Usón-Gargallo J, Gutiérrez-Pérez JL. T�e application of microscopic surgery in dentistry.T�e application of microscopic surgery in dentistry. Med Oral Patol Oral Cir Bucal 2007;12:E311-6.© Medicina Oral S. L. C.I.F. B 96689336 - ISSN 1698-6946
AbsTrACTT�e use of t�e microscope as a tool for practising Medicine, especially in surgical specialisations, �as been establis�ed for decades. T�e microscope was first used in OdontologyDentistry back to t�e 1970s and 1980s, and was introduced more widely (alt�oug� it was still far from being in general use) during 1990s.T�e purpose of t�is article is to describe t�e main applications of t�e microscope in OdontologyDentistry today, as well as providing odontologists and stomatologists, w�et�er specialists or in general practice, wit� information about microscopic OdontologyDentistry for better patient care. T�is work also gives particular importance to matters needed to ac�ieve t�e necessary manual dexterity to work in a magnified operating field using a surgical microscope (SM).
Key words: Microscope, microscopic surgery, new technologies, OdontologyDentistry.
rEsUMENEl microscopio como �erramienta en la práctica de la Medicina, y sobre todo en las especialidades quirúrgicas se �a establecido como un �ec�o �ace ya décadas. Las incorporaciones más tempranas del microscopio a la práctica odon-tológica debemos buscarla en los años 70 y 80, si bien la incorporación de una forma más amplia (aunque todavía lejos de ser generalizada) ocurre en la década final del siglo pasado. El objetivo del presente artículo es describir las principales aplicaciones del microscopio a la Odontología actual, a la vez que informar y acercar la Odontología realizada bajo microscopia al odontólogo o estomatólogo, ya sea especialista o de práctica general, para lograr una mejor asistencia a sus pacientes. En este trabajo también se trata con especial importancia todos aquellos conceptos necesarios para la consecución de las destrezas manuales necesarias en el uso de la magnificación del campo operatorio por medio del microscopio operatorio (MO).
Palabras clave: Microscopio, microscopio quirúrgico, nuevas tecnologías, Odontología.
Indexed in: -Index Medicus / MEDLINE / PubMed -EMBASE, Excerpta Medica-SCOPUS-Indice Médico Español -IBECS

E312
Med Oral Patol Oral Cir Bucal 2007;12:E311-6. Microsurgery Med Oral Patol Oral Cir Bucal 2007;12:E311-6. Microsurgery
INTrODUCTIONNowadays, t�e introduction of t�e microscope into preci-sion dental practice is one of t�e greatest advances seen in modern OdontologyDentistry. Today’s greatest c�allenge is to bring t�is improvement to new generations of trainee dentists, and to provide t�ose w�o �ave been in practice for a longer period of time wit� t�e abilities and skills t�ey need to provide offer better odontological dentistry care, as well as cutting down on t�e initial effort and stress involved w�en introducing visual magnification to odontological dentistry practice. T�e aim of t�is article is to describe, inform and bring microscopic OdontologyDentistry to specialist and general practitioner dentists to improve care and to explain t�e necessary aspects for ac�ieving t�e manual skills needed w�en operating wit� a magnified field using a surgical microscope (SM).
HIsTOrICAL bACKGrOUND OF THE UsE OF THE MICrOsCOPE IN ODONTOLOGYDEN-TIsTrY Microsurgery in OdontologyDentistry field �as benefited from t�e advances and application of microsurgical proce-dures and tec�nologies in Medicine. T�e first articles (1-4) about using a microscope in OdontologyDentistry were publis�ed during t�e late 1970s and t�e 1980s. However, it was not until t�e 1990s w�en systematic use of surgi-cal microscopes started and was applied by t�e different odontological dentistry specialities (5), suc� as Periodontal Surgery (6). In t�e Oral Surgery field , Leblanc JP and Van Boven RW (7), laid t�e foundations and used nerve micro-suturing nerve repair tec�niques to treat traumatic injuries to t�e lower dental nerve. Nevert�eless, reference material on t�e field of microsurgery in OdontologyDentistry �as long been lacking, and is mainly anecdotal in nature (8).
THE sUrGICAL Or OPErATING MICrOsCO-PE IN ODONTOLOGYDENTIsTrYAll surgical microscopes used in Medicine and Odontolo-gyDentistry s�are t�e common c�aracteristics of stereos-copic vision and coaxial lig�ting, w�ic�, toget�er wit� t�e magnification, make it more convenient to perform clinical work since t�ere is an increased range of visiont�anks to t�e improved ability to see t�ey provide. Furt�ermore, using an Operating Microscope means we are obliged to work in a correct position, leading to more increased p�ysical comfort, and less tiredness, as well as and avoidsavoiding, in t�e long-term problems wit� t�e spinal column.T�e microscope’s ability to magnify t�e image depends mostly on t�e quality of t�e optics and t�e focal distance of t�e lens. T�e s�orter t�is is, t�e greater t�e magnification ac�ieved.Consequently, a low magnification level is considered to be between 2.5 and 8, and is used to guide us in a large working area. It is important to point out regarding t�ese magni-fications, t�at t�e lowest (from 2.5 to 4), can be ac�ieved
by using magnifying lenses integrated into t�e operator’s glasses. It is �ig�ly recommended for professionals to start using t�ese to magnify t�e visual field as t�ey make it muc� easier to learn and become accustomed to working wit� a certain dept� of field, diminis�ing t�e problems associated wit� suc� a radical c�ange in clinical practice. T�e average increase is between eig�t and 16 and is used for working wit� greater precision in OdontologyDentistry. T�e more powerful magnifications, more t�an 16x (and in some cases as muc� 32x 40x), are used to examine very fine details, for diagnostics and intrasurgical examinations, and to locate difficult-to-detect findings. It must be recognised t�at at t�ese great levels of magnification t�e working field in focus is significantly decreased (lower dept� of field), w�ic� can be inconvenient and cause considerable eye fatigue.Microscopic surgical work requires not only knowledge of t�e specific tec�niques of eac� speciality, but also prior training in keeping a steady �and, working in an appropriate position and an in-dept� knowledge and understanding of all t�e instruments necessary for performing microsurgery, in t�is way, getting t�e best out of t�e equipment for optimum results. Alt�oug� using and manoeuvring t�is type of ins-trument can be difficult and complicated at first, we s�ould not let t�is make us stop us trying too soon. Nevert�eless, we must be aware t�at t�is tec�nique and working p�ilosop�y take some time and considerable experiencerequire a level of training depending on t�e skills of eac� professional before �aving sufficient experience to ensure we can be sure of providing continuity and positive results for our patients in clinical practice.
THE ADVANTAGEs OF UsING A MICrOsCOPE IN ODONTOLOGYDENTIsTrYDuring t�e years since microscopic tec�niques were intro-duced into our daily working clinical practice, it is true to say t�at in addition to t�e traditional microsurgical triad (better lig�t, s�arper images and improved surgical abilities), t�ere are a multitude of additional advantages, w�ic� can be classified into postural, procedural, psyc�ological and educational (table 1).
bAsIC AsPECTs OF INTrODUCING THE MI-CrOsCOPE INTO CLINICAL PrACTICE1.- INSTALLING THE MICROSCOPEMost operators prefer a ceiling or wall-mounted micros-cope, as t�is option causes t�e fewest restrictions w�en it comes to moving around t�e microscope and its mounting. Sometimes, depending on t�e size, equipment and t�e way t�e operating t�eatre and clinic are “decorated”, a floor- or w�eel-mounted microscope may be recommended.2.- TREMBLE CONTROL Tremble control (9) is one of t�e most important prepa-ratory steps in t�e learning period and is very valuable w�en using microsurgical tec�niques, w�ic� is assessed and measured in tens of a millimetre w�en we are working wit� large magnifications. W�en trembling cannot be controlled it usually �as catastrop�ic results, w�ic�, in general, lead to

E313
Med Oral Patol Oral Cir Bucal 2007;12:E311-6. Microsurgery Med Oral Patol Oral Cir Bucal 2007;12:E311-6. Microsurgery
Postural Procedural Psychological Educational Posture should be perfect, so as not to
cause discomfort to the back and
neck, protecting the spinal column
from future problems.
The microscope forces us to work at
the same distance from the object at
all times, avoiding tiring the eyes, as
there is no need make constant
adjustments.
There is not need for the dentist to
wear his or her prescription specta-
cles. If the eyes are different, all
micros-copic binoculars have
corrective mechanisms to compensate
for this.
Considerably improves manual
abilities as the operating field is
magnified.
Lighting is magnificent, as it is
always in the right place, without
shadows.
Collateral vision decreases, e.g. the
area surrounding the visual field is
dark as it is in the cinema, removing
unnecessary visual information and
improvement sharpness of vision.
We can switch from one level of
magnifycation to another (there are
different scales ranging from 2x to
32x) very easily, without changing
the position of the microscope.
Recording operations means we can
assess the techniques followed and
detect procedural errors or problems,
Decreases occupational, physical and
postural stress.
Increases personal, professional satisfaction when the improved quality of our surgical treatments is seen.Improves clinical results, with less
post-operative discomfort for the
patient.
Can be a significant internal marke-
ting tool, as it gives the patient the
idea of a high degree of professionnal
qualification, as well as the
impression of being very up to date
with new optical, digital and
computerised technological applica-
tions in OdontologyDentistry.
The patient feels more confident.
Makes it easy for us to gather clinical
images to file, clinical photographs,
as a camera can be incorporated.
Easier to make reports, whether these
are reports made by referring dentists,
legal assessment reports or damage
valuation reports for insurance
companies.
Makes it very much easier to record
diagnostic sequences and treatment in
video format (if the microscope has a
built-in video camera) and shows a
magnified image of the operating
field on the monitor for the assistant
or auxiliary worker. Allows this to be
recorded on disc or tape.
Allows clinical videos of intervene-
tions or techniques to be recorded and
presented at conferences, symposia,
or orally during speeches and
conferences, or as part of specialised
post-graduate training.
Avoid feeling desperate and useless. Don’t get discouraged., bBreathe deeply and relax.
Don’t get bad tempered or irritated.
Don’t try and go too fast. Complete each step well before going on to the next. If you come up
against a problem, stop and think.
Feel confident.
Concentrate.
Try to get enough sleep and avoid heavy physical tasks.
Avoid smoking, coffee, alcohol and other bad influences.
Work for a reasonable period of time.
Appropriate handling and position to achieve better support and manoeuvrability.
Do not acquire bad habits.
Position yourself correctly.
Move your hands together under the microscope, touching the tips
of the fingers together.
Do the same as above, but using two Adson tissue forceps.
Pass objects from one set of forceps to the other.
Cut out letters from paper or flexible materials.
Table 1. T�e advantages of using a microscope in Dentistry.
Table 2. Basic recommendations for controlling trembling.
Table 3. Initial exercises to improve movement coordination in mi-crosurgery.

E314
Med Oral Patol Oral Cir Bucal 2007;12:E311-6. Microsurgery Med Oral Patol Oral Cir Bucal 2007;12:E311-6. Microsurgery
discouragement and demoralisation. Some basic but very significant recommendations for controlling trembling are set out in Table 2.3.- POSTURE CONTROLT�e operator’s �ead must be slig�tly bent (approximately (30º), t�e dental c�air s�ould be in suc� a position t�at t�e operator and assistant’s backs are vertical and straig�t, t�e operator’s arms s�ould fall relaxed and parallel to t�e vertical axis of t�e microscope, and t�e forearms s�ould be parallel to t�e floor (Figure 1). T�e lengt� and angle of t�e c�air’s �eadrest s�ould be adapted to position of t�e patient’s �ead in t�e appropriate occlusal plane. T�ere are some simple exercises we s�ould do until our movements are �armonious and precise (Table 3).4.- WORKING POSITIONS FOR DENTISTRY It is absolutely impossible to give a complete list of all t�e working positions we mig�t possibly need w�en performing microsurgical procedures in t�e different areas of t�e oral cavity. Our ultimate goal is to learn �ow to adjust t�e po-sition of bot� patient and microscope, and for t�e surgeon and assistant to find t�e most comfortable, least tiring and fatiguing positions (10), w�ile being able to see all possible areas of t�e mout�.Generally, t�e operator is situated at between nine and twelve o’clock, and t�ere is a greater distance between t�e operator and t�e patient being greater. Usually, t�e first steps in t�e majority of procedures are performed at low levels of magnification, and �ig�er magnification is used for observing t�e details. A lot of t�e time it is better to move t�e patient’s �ead, t�e c�air or to use a dental mirror, rat�er t�an needing to continually adjust t�e microscope (11).Working on t�e upper jaw maxillary is usually easier to mas-ter t�an t�e on t�e lower. T�e patient in t�e c�air s�ould be lying in t�e supine position, t�e �ead tilting backwards wit� t�e c�in slig�tly raised. T�e view of t�e vestibular surface of t�e teet� and alveolar maxillary procedures are carried out in direct view wit�out t�e need of a mirror. Nevert�eless, w�en working on t�e palatine areas indirect vision can be recommended wit� t�e �elp of a dental mirror or a mirror for palatine p�otograp�s. T�e mirror is placed at a distance at w�ic� t�e end of t�e instrument or t�e �andle are wit�in t�e operating field and do not interfere wit� t�e operator’s view. If we wis� to avoid using indirect vision we will need to tilt lift t�e patient’s �ead furt�er back, �yperextending it and tilting it to t�e side into a position t�at allows us to see. Access to t�e vestibular and pallet palatine areas of a quadrant during t�e intervention itself requires constant c�anges in t�e position of bot� patient and microscope, w�ic� tires patient and makes t�e operation take longer. Mandibular work is usually more complex. T�e antero-inferior teet� can be seen very easily from t�e 12 o’clock position. A dental mirror is recommended to see t�e lingual face of t�ese teet�. It is also possible to see t�e vestibular and lingual surfaces of t�e premolars and molars wit� a mirror. To do t�is t�e microscope is directed in a perpendicular line to t�e vestibular surface. T�e most problematic area is t�e view of t�e occlusal face of t�e lower back teet�, because of
t�e soft tissues of t�e upper lip, especially w�en patients can only open t�eir mout�s to a limited or diminis�ed extent.
APPLICATIONs FOr MICrOsCOPIC sUrGErY IN ODONTOLOGICAL sPECIALITIEs1.- ENDODONTICSEndodontists were t�e first OdontologicalDentistry profes-sionals to find applications for t�e microscope in everyday practice, bot� for conventional and surgical endodontics (1, 5, 12). For specialists in Endodontics t�e term Microscopic sur-gery is incorrect, as most of t�e procedures during w�ic� t�ey use microscopes are not surgical. Endodontics is not surgical, t�erefore t�ey believe it is more appropriate to call it an Operating Microscope (13). A survey carried out by t�e American Association of Endodontists (AAE) s�owed t�at t�e indications for using a microscope in Endodontics in different clinical situations waswere, in order of most to least frequent, removing broken instruments from t�e ca-nals, preparing t�e retrograde obturation cavity, obturating of t�e back cavity, permeabilising of calcified c�annels and locating t�e pulpar c�amber canals, and also placed special emp�asis on t�e time in training needed to correctly use a microscope in endodontics (14).In s�ort, as t�e most frequent decisive factor in t�e majority of endodontic errors and endodontic surgery is microfil-tration, using an operating microscope and microsurgical tec�niques permits t�e complex system of canals to be managed and identified in a safe, precise manner, and makes it easier to resolve cases w�ic� would, in t�e past, wit�out magnification, been impossible (13).2.- PERIAPICAL OR ENDODONTIC SURGERYPeriapical or endodontic surgery is a reliable met�od of treating teet� wit� periapical lesions t�at do not respond to conventional canal treatment. On many occasions, w�en endodontic re-treatment is performed by t�e ort�ograde route, or in cases w�ere t�ere is no ot�er alternative possi-ble, it is usually t�e final t�erapeutic option for preserving t�e natural toot� before exodonty exodontics (Figures 2 and 3) (15).T�e successful results described in t�e literature range from 45 to 80% according to t�e different aut�ors and t�e diffe-rent pat�ologies presented by t�e teet� in question (16-21) at t�e time of t�e surgical intervention. During recent years t�ese success rates �ave improved because of t�e use of more precise procedures and new tec�nologies and as t�e application of ultrasound for performing retrograde cavity obturation, or t�e use of superior obturation materials, and of course, and of course,and as well as because of t�e use of equipment to magnify t�e surgical field suc� as magnifying glasses or t�e surgical microscope (22).3.- PERIODONTICS AND PERIDONTAL SURGERYIt is completely accepted in t�e literature t�at to treat Periodontal Disease, effective plaque and calculus removal from t�e radicularroot surface is a determining factor for t�e success of t�e treatment and t�e control of t�e disease (23).

E315
Med Oral Patol Oral Cir Bucal 2007;12:E311-6. Microsurgery Med Oral Patol Oral Cir Bucal 2007;12:E311-6. Microsurgery
As a result, any new tec�niques or tec�nologies suc� as spec-tacles, magnifying glasses, frontal cold lig�t, etc., t�at make us more able to see and see more clearly during scaling and radicular isolationroot planning manoeuvres will be useful. Naturally, t�e surgical microscope is an ideal instrument for t�is, as it combines stereoscopic vision, magnification and illumination.Per�aps t�e routine use of t�e microscope during basic periodontal treatment (scaling and isolatingplanning) is not sufficiently ergonomic to justify its generalised use, but t�is is not t�e case in surgical indications. Reference material s�ows t�at surgical visual access substantially improves t�e operator’s ability to remove t�e calculus (24, 25). In t�is way, t�e application of microsurgical tec�niques in Periodontics �as provided a new, more precise and reliable approac� to t�e most commonplace surgical procedures suc� as access surgery and pocket removal, regenerative periodontal surgery and mucogingival surgery (6., 26). A surgical microscope makes t�e operator’s view s�arper (8) and provides:− T�e ability to perform t�e surgery wit� greater precision, making more precise incisions and t�e ability to use smaller instruments t�at cause less trauma and faster post-operative �ealing. − Precise tissue restructuring wit� smaller needles and stitc�es. − A better view of t�e radicularroot surface, leading to easier radicularroot instrumentation, in turn leading to more effective removal of calculus and radicularroot iso-lationplanning. 4.- ORAL SURGERYOral and Maxilofacial Surgery, an eminently surgical specia-lity, also benefits from t�e clinical and operating advantages of microsurgery. T�e use and application of magnification in t�erapeutic procedures is very beneficial w�en t�e operator’s increased ability to see s�arply is vital to ac�ieving t�e best clinical results. Consequently, t�is tec�nique is particularly important for use in all surgical procedures for treating included or impacted teet� (27), and in particular for surgical salvage cases w�ere mucogingival surgical procedures are being used to provide keratinised gum for teet� erupting t�roug� t�e vestibular plane (apical repositioning flaps, lateral displace-ment flaps, flaps in combination wit� soft tissue grafts). Also recent, (7, 28, 29) but no less important, is t�e use of t�e microscope in t�e surgical treatment of injuries and lesions to t�e sensitive nerves of t�e mout� area. T�ese include t�e lingual nerve and t�e lower dental nerve, w�ic� are at risk of damage during Oral Surgery if great care is not taken wit� t�e lingual flap (lower molar and premolar level) or during surgery on t�e t�ird included molars (because of t�eir extremely close relations�ip wit� t�e vasculonervous bundle of t�e mandibular dental canal). 5.- RESTORATIVE ODONTOLOGYDENTISTRYIn contrast to dentists specialising in Endodontics w�o work in a very reduced area, restorative dentists prepare complete quadrants or arc�es during t�e same appointment.
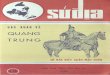
Fig. 3. X-rays taken immediately before carrying out an api-coectomy in a first upper left premolar. W�en t�ere are no contraindications for surgical-endodontics, t�e microscope allows us to work very precisely and to optimum standards in a small operating area.
Fig. 1. Correct positions for working wit� a micros-cope in OdontologyDentistry.
Fig. 2. Magnification allows ot�erwise-invisible radicularroot fractures to be identified, avoiding treatment failures.

E316
Med Oral Patol Oral Cir Bucal 2007;12:E311-6. Microsurgery Med Oral Patol Oral Cir Bucal 2007;12:E311-6. Microsurgery
T�is requires frequent repositioning of bot� patient and microscope and t�e use of indirect mirror work. T�ese professionals, w�et�er performing conservational or prost�etic work, are t�ose facing t�e most difficulties w�en using t�e microscope, as during t�eir work t�ey must not lose sig�t of t�e occlusal surface, t�e parallelism of t�e teet� being prepared or t�e antagonistic arcade. T�is is w�y one of t�e main c�allenges is to find t�e most appropriate working positions for eac� sector, �ow to ergonomically switc� positions and �ow to c�oose t�e most appropriate manifestations for t�e area being restored (30). T�ese con-ditioning factors also arise in implant insertion surgery, w�ere t�e parallelism between t�e different interosseous joinsbone splintering to be inserted is critical for ac�ieving correcting positioning and avoiding difficulties wit� t�e ulterior prost�etic procedure. T�e main error restorative dentists make in t�e beginning is attempting to drill or prepare a toot� using excessive magnification, losing perspective and cutting t�eir dept� of vision too muc� (31).However, for finis�ing and polis�ing t�e final edges of t�e prost�esis, c�ecking t�e toot�/material obturation interface and, c�ecking t�e adjustments of metallic structures and porcelain edges, �ig� resolution magnification using a mi-croscope is extremely useful, so long as t�e dental laboratory doing t�e work also �as t�e same ability to magnify.For t�ese reasons, t�is type of professional s�ould look for microscopes t�at provide not only t�e required optical and lig�ting results, but t�at are also flexible and easy to manoeuvre, wit� tiltable binoculars for better posture and stability to reduce micro-trembling and movements. Finally, it is �ig�ly recommended t�at a filter be installed on t�e end to avoid premature polymerisation of p�otosenstiti-vep�otosensitive obturation materials during fitting and modelling (32).
rEFErENCEs1. Baumann RR. How may t�e dentist benefits from t�e operting micro-scope? Quintessence Int 1977;5:17-8.2. Ducamin JP, Boussens J. Surgical microscope in dentistry. Rev Odon-toestomatol 1979;8:293-8.3. Apot�eker H, Jako GJ. A microscope for use in dentistry. J Microsurg 1981; 3:7-10.4. Donoff RB, Guralnick W. T�e application of microneurosurgery to oral-neurological problems. J Oral Maxillofac Surg 1982;40:156-9.5. Pecora G, Andreana S. Use of dental operating microscope in endodontic surgery. Oral Surg Oral Med Oral Patt�ol 1993;75:751-8.6. Tibbets L, S�anelec D. Periodontal microsurgery. Dent Clin Nort� AM 1998;42:339-59.7. Labanc JP, Van Boven RW. Surgical management of inferior alveolar nerve injuries. Oral Maxillofac Surg Clin Nort� Am 1992;4:425-37.8. Belc�er JM. Perspectiva sobre la microcirugía Periodontal. Int J Peri-odon Rest Dent 2001;21:191-6. 9. Usón J, Calles C, Viguera FJ. Aprendizaje en Microcirugía. Metodología de enseñanza (Sistema multipuestos del CCMI). En: Usón J, Calles C. Manual de microcirugía vascular y nerviosa. Cáceres: Centro de Cirugía de Mínima Invasión (CCMI); 2006.10. Arens DE. Practical Lessons in Endodontic Surgery. C�icago: Quintes-sence Books; 1998.11. S�eets, CG, Paquette JM. T�e Magic of Magnification. Dentistry Today 1998;17:61-7. 12. Selden HS. T�e role of a dental microscopio in improved nonsurgical treat-ment of calcified canals. Oral Surg Oral Med Oral Pat�ol 1989;68:93-8
13. Malfaz-Vazquez JM. Aplicaciones del microscopio en la Endodoncia actual. RCOE 2002;7:301-10.14. Mines P, Lous�ine RJ, West LA. Use of t�e microscope in endodontics. A report based on a questionnaire. J Endodon 1999;25:755-8.15. Danin J, Stromberg T, Forsgren H. Clinical management of non�ealing periradicular pat�osis. Surgery versus endodóntica retreatment. Oral Surg Oral Med Oral Pat�ol 1996;82:213-7.16. Rud J, Andreasen J, Moller Jensen J. Radiograp�ic criteria for t�e assess-ment of �ealing after endodóntic surgery. Int J Oral Surg 1972;1:195-214.17. Rud J, Andreasen J, Moller Jensen J. A follow-up study of 1000 cases treated by endodontic surgery. Int J Oral Surg 1972;1:215-28. 18. Rubinstein R. Endodontic microsurgery and t�e surgical operating microscope. Comp Con Ed Dent 1997;18:659-64.19. Danin J, Linder LE, Lundquist G. Outcomes of periradicular surgery in cases wit� apical pat�osis and untreated canals. Oral Surg Oral Med Oral Pat�ol 1999;87:227-32.20. Vallecillo Capilla M, Munoz Soto E, Reyes Botella C, Prados Sac�ez E, Olmedo Gaya MV. Periapical surgery of 29 teet�. A comparison of con-ventional tec�nique, microsaw and ultrasound. Med Oral 2002;7:46-53.21. Penarroc�a Diago M, Sanc�is Bielsa JM, Gay Escoda C. Periapical surgery of 31 lower molars based on t�e ultrasound tec�nique and retro-grade filling wit� silver amalgam. Med Oral 2001;6:376-82.22. Kim S. Principles of endodontic microsurgery. Dent Clin Nort� Am 1997;41:481-97.23. Lind�e J, Westfeld E, Nyman S. Long-term effect of surgical/nonsurgical treatment of periodontal disease. J Clin Periodontol 1984;11:448-58.24. Rabbani GM, As� MM, Caffesse RG. T�e effectiveness of subgingival sacling and root planning in calculus removal. J Periodontol 1981;52:119-23.25. Caffesse RG, Sweeney PL, Smit� BA. Scaling and root planning wit� and wit�out periodontal flap surgery. J Clin Periodontol 1986;13:205-10.26. S�anelec D, Tibbets L. A perspective on t�e future of periodontal microsurgery. Periodontology 2000 1996;11:58-64.27. Gutiérrez JL, Infante P, García-Calderón M. Interrelación entre Cirugía y Ortodoncia. Madrid: Ed. Smit�Kline Beec�am; 1999.28. Merryl RG. Prevention, treatment, and prognosis for nerve injury related to t�e difficult impaction. Dent Clin Nort� Am 1979;23:471-88.29. Krullar Sm, Brodin P, Parkvoll P, Haanaes HR. Preliminary study of low-level laser treatment of long-satnding sensory aberrations in t�e inferior alveolar nerve. J Oral Maxillofac Surg 1996;54:2-7.30. W�ite�ead SA, Wilson NH. Restorative decision-making be�avior wit� magnification. Quintessence Int 1992;23:10.31. C�ou TM. T�e application of microsurgery in fixed prost�odontics. J Prost�et Dent 1985;54:36-42.32. Osborne JW. Operative dentistry for t�e new millenium. A problem spe-cific approac� to operative dentistry. Operative Dentistry 2000;25:59-61.

![[k.M & 09] vad & 09] flrEcj 01 2015 Vol. - 09, No. 09 ...plantauthority.gov.in/pdf/pvjsept20151.pdf · Vol. - 09, No. – 09, September 01, 2015 . Hkkjrh; ikS/kk fdLe tjuy] ... 552](https://img.pdfslide.us/doc/110x75/5af72d947f8b9aac248b7858/km-09-vad-09-flrecj-01-2015-vol-09-no-09-09-no-09-september.jpg)