Embed Size (px)
DESCRIPTION
Article
Citation preview

American Journal of Public Health | March 2006, Vol 96, No. 3452 | Opportunities and Demands in Public Health Systems | Peer Reviewed | Homer and Hirsch
OPPORTUNITIES AND DEMANDS IN PUBLIC HEALTH SYSTEMS
System Dynamics Modeling for Public Health: Background and Opportunities
| Jack B. Homer, PhD, and Gary B. Hirsch, SMThe systems modelingmethodology of system dy-namics is well suited to ad-dress the dynamic complex-ity that characterizes manypublic health issues. Thesystem dynamics approachinvolves the development ofcomputer simulation mod-els that portray processes ofaccumulation and feedbackand that may be tested sys-tematically to find effectivepolicies for overcoming pol-icy resistance.
System dynamics model-ing of chronic disease pre-vention should seek toincorporate all the basicelements of a modern eco-logical approach, includingdisease outcomes, healthand risk behaviors, environ-mental factors, and health-related resources and deliverysystems. System dynamicsshows promise as a meansof modeling multiple inter-acting diseases and risks, theinteraction of delivery sys-tems and diseased popu-lations, and matters of na-tional and state policy. (Am JPublic Health. 2006;96:452–458. doi:10.2105/AJPH.2005.062059)
By applying a remedy to one sore, you
will provoke another; and that which re-
moves the one ill symptom produces
others, whereas the strengthening one
part of the body weakens the rest.
—Sir Thomas More, Utopia,
Part I (1516)
DESPITE REMARKABLE successes in some areas, thehealth enterprise in Americastill faces difficult challenges inmeeting its primary objective ofreducing the burden of diseaseand injury. Examples includethe growth of the underinsuredpopulation, epidemics of obe-sity and asthma, the rise ofdrug-resistant infectious dis-eases, ineffective managementof chronic illness,1 long-standingracial and ethnic health dispari-ties,2 and an overall decline inthe health-related quality oflife.3 Many of these complexproblems have persisted fordecades, often proving resistantto attempts to solve them.4
It has been argued that manypublic health interventions fallshort of their goals because theyare made in piecemeal fashion,rather than comprehensively andfrom a whole-system perspective.5
This compartmentalized ap-proach is engrained in the finan-cial structures, intervention de-signs, and evaluation methodsof most health agencies. Con-ventional analytic methods aregenerally unable to satisfacto-rily address situations in whichpopulation needs change overtime (often in response to theinterventions themselves), andin which risk factors, diseases,
and health resources are in acontinuous state of interactionand flux.6
The term dynamic complexityhas been used to describe suchevolving situations.7 Dynamicallycomplex problems are oftencharacterized by long delays be-tween causes and effects, and bymultiple goals and interests thatmay in some ways conflict withone another. In such situations,it is difficult to know how,where, and when to intervene,because most interventions willhave unintended consequencesand will tend to be resisted orundermined by opposing inter-ests or as a result of limited re-sources or capacities.
THE SYSTEM DYNAMICSAPPROACH
We believe that in manycases the challenges of dy-namic complexity in publichealth may be effectively ad-dressed with the systems mod-eling methodology of systemdynamics. The methodology in-volves development of causaldiagrams and policy-orientedcomputer simulation modelsthat are unique to each prob-lem setting. The approach wasdeveloped by computer pio-neer Jay W. Forrester in themid-1950s and first describedat length in his book IndustrialDynamics,8 with some addi-tional principles presented inlater works.9–12 The Interna-tional System Dynamics Societywas established in 1983, andwithin the society a special
interest group on health issueswas organized in 2003.
A central tenet of system dy-namics is that the complex behav-iors of organizational and socialsystems are the result of ongoingaccumulations—of people, mate-rial or financial assets, informa-tion, or even biological or psycho-logical states—and both balancingand reinforcing feedback mecha-nisms. The concepts of accumula-tion and feedback have beendiscussed in various forms forcenturies.13 System dynamicsuniquely offers the practical appli-cation of these concepts in theform of computerized models inwhich alternative policies and sce-narios can be tested in a system-atic way that answers both “whatif” and “why.”14–16
A system dynamics modelconsists of an interlocking set ofdifferential and algebraic equa-tions developed from a broadspectrum of relevant measuredand experiential data. A com-pleted model may contain scoresor hundreds of such equationsalong with the appropriate nu-merical inputs. Modeling is an it-erative process of scope selection,hypothesis generation, causaldiagramming, quantification, reli-ability testing, and policy analy-sis.7 The refinement process con-tinues until the model is able tosatisfy requirements concerningits realism, robustness, flexibility,clarity, ability to reproduce his-torical patterns, and ability togenerate useful insights. Thesenumerous requirements help toensure that a model is reliableand useful not only for studying

March 2006, Vol 96, No. 3 | American Journal of Public Health Homer and Hirsch | Peer Reviewed | Opportunities and Demands in Public Health Systems | 453
OPPORTUNITIES AND DEMANDS IN PUBLIC HEALTH SYSTEMS
the past, but also for exploringpossible futures.12,17
The calibration of a systemdynamics model’s numericalinputs—its initial values, con-stants, and functional relations—merits special mention. Insystem dynamics modeling,variables are not automaticallyexcluded from consideration ifrecorded measurements onthem are lacking. Most thingsin the world are not measured,including many that experiencetells us are important. Whensubject matter experts agreethat a factor may be important,it is included in the model, andthen the best effort is made toquantify it, whether through(in approximately this order ofpreference) the use of recordedmeasurements, inference fromrelated data, logic, educatedguesswork, or adjustmentsneeded to provide a bettersimulated fit to history.11,17,18
Uncertainties abound in modelcalibration, which is one of thereasons that sensitivity testing iscritical. Sensitivity testing of awell-built system dynamicsmodel typically reveals that itspolicy implications are unaf-fected by changes to most cali-bration uncertainties.9,10 Buteven when some uncertaintiesare found to affect policy find-ings, modeling contributes byidentifying the few key areas—out of the overwhelming num-ber of possibilities—in whichpolicymakers should focus theirlimited resources for metricscreation and measurement.
System dynamics modelinghas been applied to issues ofpopulation health since the1970s. Topic areas have includedthe following:
1. Disease epidemiology includ-ing work in heart disease,19–21
diabetes,21,22 HIV/AIDS,23–25
cervical cancer,26 chlamydiainfection,26 dengue fever,27
and drug-resistant pneumococ-cal infections28;
2. Substance abuse epidemiologycovering heroin addiction,29
cocaine prevalence,30 and to-bacco reduction policy31,32;
3. Patient flows in emergencyand extended care26,33–35;
4. Health care capacity anddelivery in such areas aspopulation-based healthmaintenance organizationplanning,36 dental care,37,38
and mental health,38 and asaffected by natural disastersor terrorist acts39;
5. Interactions between healthcare or public health capacityand disease epidemiology.40–43
Most of these modeling effortshave been done with the close in-volvement of clinicians and poli-cymakers who have a direct stakein the problem being modeled.A good example is a chronic ill-ness study conducted in What-com County, Washington, thatfocused on diabetes and heartfailure.21 Health care providers,payers, and community represen-tatives (supplemented by thehealth care literature) identifiedinfluential variables, articulatedpolicy-related concerns, provideddata, and provided experience-based estimates when measureddata were not available. Themodels projected the potentialimpacts of programs on morbid-ity, mortality, disability, costs,and the various stakeholders andidentified the programmatic in-vestments required. Establishedsystem dynamics techniques forgroup model building44 can helpto harness the insights and in-volvement of those who deal withpublic health problems on a day-to-day basis.
It is useful to consider howsystem dynamics methodologyand models compare with thoseof other simulation methods thathave been applied to publichealth issues, particularly in epi-demiological modeling. Othertypes of models include lumpedpopulation contagion models45,46;Markov models that distinguishamong demographic categories ofage, sex, race, and so forth47–49;and microsimulations or agent-based models at the level of indi-viduals.50–52 There is significantoverlap among the methods, andone cannot always look at amodel’s equations and instantlyknow by what method it was de-veloped. In general, though, onemay say that system dynamicsmodels tend to have broaderboundaries than other types ofmodels and accordingly tend toadmit more variables on the basisof logic or expert opinion and forwhich solid statistical estimatesmay not available. System dynam-ics modelers find that a broadboundary including a variety ofrealistic causal factors, policylevers, and feedback loops is oftenwhat is needed for finding effec-tive solutions to persistent, dy-namically complex problems.7,53
CHRONIC DISEASEPREVENTION
The value of system dynamicsmodeling is best explained byway of illustration. We start witha challenging question: Why isit that, despite repeated calls fora greater emphasis on primaryprevention of chronic disease(including a prominent recentexample54), the vast majority ofhealth activities and expendituresin the United States are madenot for such prevention butrather for disease managementand care?55 This dominance of
“downstream” over “upstream”health activities appears to havegrown ever greater during theera of modern medicine and isnow seen as a pressing problemby public health agencies such asthe Centers for Disease Controland Prevention (CDC).56
To illustrate how system dy-namics simulation might shedlight on this question, we havebuilt a relatively simple modelexploring how a hypotheticalchronic disease population maybe affected by 2 types of preven-tion: upstream prevention of dis-ease onset, and downstream pre-vention of disease complications.The model demonstrates howupstream prevention may be-come inadvertently “squeezedout” by downstream preventionand suggests that a focusing ofresources on life-extending clini-cal tools may ultimately hurtmore than it helps. The modelhas only a single aggregated pop-ulation stock, 27 differential andalgebraic equations and 12 nu-merical inputs, and is based ongeneral knowledge rather thanon any specific case study orother hard data. If the modelwere intended for actual policy-making and not only for illustra-tion or exploration, one wouldcertainly expect to see a moredetailed depiction of the popula-tion and causal factors and poli-cies, and a more data-reliant ap-proach to parameter estimation.
Figure 1 presents the model’sessential causal structure and pol-icy inputs. The single stock ofpeople with disease representsthe gradually changing net accu-mulation of 2 flows: an inflow ofdisease onset and an outflow ofdeaths. Skilled resources for pre-vention, consisting perhaps of allprimary care providers in the re-gion where the disease popula-tion is located, are assumed to be

American Journal of Public Health | March 2006, Vol 96, No. 3454 | Opportunities and Demands in Public Health Systems | Peer Reviewed | Homer and Hirsch
OPPORTUNITIES AND DEMANDS IN PUBLIC HEALTH SYSTEMS
Note. The rectangle represents a stock of people; thick arrows with valves and cloud symbols represent flows of people; thinner arrows indicatecausal influence; arrows with minus signs indicate inverse causal influence.
FIGURE 1—A simple model of chronic disease prevention.
FIGURE 2—Chronic disease prevention model output for 3 scenarios over 50 simulated years, showingonset prevention fraction (a), complications prevention fraction (b), people with disease (c), and deathsfrom complications (d).
fixed in number. Certain clinicaltools (diagnostic and therapeutic)are available to these providersfor complications prevention, andother tools are available for onsetprevention. The greater the num-ber of people with disease, andthe greater the number of toolsavailable for complications pre-vention, the more the time of pro-viders will be devoted to compli-cations prevention. Theremainder of provider time isthen available for onset preven-tion efforts among nondiseasedpatients (to the extent that avail-able onset prevention tools allow)or is absorbed by other, nonpre-vention activities.
For both types of prevention,assumptions are made about thepreventable fractions of casesgiven existing clinical tools, andalso about the resource require-ments per case prevented, andthe time delay between the avail-ability of new tools and theiradoption by providers and impact
on patients. Our starting assump-tions are that 25% of complica-tions are preventable, 25% ofonset is preventable, and re-sources are sufficient to achieveboth these prevention fractions,with some capacity to spare.Under these assumptions, up-stream prevention activities aresignificant and nearly on a parwith downstream prevention activ-ities. This balanced situation maybe similar to the state of affairsthat prevailed in general medicineseveral decades ago when thetools of disease diagnosis andmanagement were limited—andvery unlike the situation today.
Figure 2 presents simulationoutput, over a period of 50years, for 4 key variables (onsetprevention fraction, complica-tions prevention fraction, peoplewith disease, and deaths from

March 2006, Vol 96, No. 3 | American Journal of Public Health Homer and Hirsch | Peer Reviewed | Opportunities and Demands in Public Health Systems | 455
OPPORTUNITIES AND DEMANDS IN PUBLIC HEALTH SYSTEMS
complications) under 3 differentpolicy scenarios we have tested(Status Quo, More ComplicationsPrevention, and More Onset Pre-vention). In all 3 scenarios, themodel has been initialized in adynamic equilibrium or steadystate in which there are about1 million people with disease,with 75000 new cases per yearand an equal number of deaths,and with 56000 of the annualdeaths from complications. Inthe Status Quo scenario, no newprevention tools are introducedduring the simulation; conse-quently, the graph lines remainflat, making this scenario a con-venient baseline for comparison.
In the More ComplicationsPrevention scenario, new toolsfor complications prevention be-come available during years 5 to10, increasing the preventablefraction of complications from25% to 50%. The results lookgood early on, as a rising compli-cations prevention fraction (Fig-ure 2b) leads to a significant re-duction in complications deaths(Figure 2d). But the reduction indeaths means a longer averagestay in the diseased populationstock and thus, an increase in thenumber of people with disease(Figure 2c). Greater disease prev-alence, in turn, increases theneed for resources for complica-tions prevention.
This increased demand forlimited resources has 2 negativeeffects. The first is that resourcesbecome inadequate to preventcomplications in some patientswho could have been helped oth-erwise. Consequently, the com-plications prevention fractionstarts to fall from its peak, andthe number of deaths starts to re-bound. This effect, reflecting thebalancing (B) loop seen in theright-hand portion of Figure 1, isunfortunate but by itself would
cause only a limited rebound indeaths. More problematic isthe second effect of resourcesqueezing, which is a decline inthe onset prevention fraction(Figure 2a). The drop in onsetprevention allows a further in-crease in disease prevalence,which causes more resources tobe absorbed in complicationsprevention, leaving even less foronset prevention. This reinforc-ing (R) loop, seen in the left-handportion of Figure 1, ultimatelydrives out onset prevention en-tirely, leading to large permanentincreases in both disease preva-lence and complications deathsrelative to their starting points.
To summarize this second sce-nario, although the complicationsprevention fraction is in fact per-manently increased, the prolon-gation of life and the squeezingout of onset prevention ulti-mately cause the prevalence ofdisease to increase proportion-ately even more; the net result isan increase in deaths from com-plications. The squeezing out ofonset prevention is a viciouscycle and a trap that the healthcare system may be prone to fallinto, given its commitment to thebest possible management of ex-isting disease. In a system withlimited prevention resources, thiswell-intentioned commitment mayend up doing more harm thangood. (The over-dependence ondownstream work and squeezingout of upstream work has beenobserved in many domains out-side of health care. This arche-typical “fire fighting” dynamichas been the subject of SD mod-els in the area of product devel-opment57 and business processimprovement.58)
A much brighter outcome isseen in the third scenario in Fig-ure 2, More Onset Prevention. Inthis scenario, new tools for onset
prevention become availableduring years 5 to 10, increasingthe preventable fraction of onsetfrom 25% to 50%. Using thespare resources initially avail-able, some additional onset isprevented (Figure 2a), and thenumber of people with disease(Figure 2c) declines. As diseaseprevalence declines, even moreprevention resources are freedup to do onset prevention. Withdisease prevalence decreasing inthis scenario, the reinforcingloop in Figure 1 becomes a “vir-tuous cycle” rather than a vi-cious cycle, making possible along-term decline in both diseaseprevalence and deaths fromcomplications (Figure 2d). A sim-ilar beneficial result might be ob-tained by other means; for ex-ample, by changes in fundingmechanisms that shift more re-sources toward onset prevention.
TOWARD MORECOMPLETE MODELS OFPOPULATION HEALTH
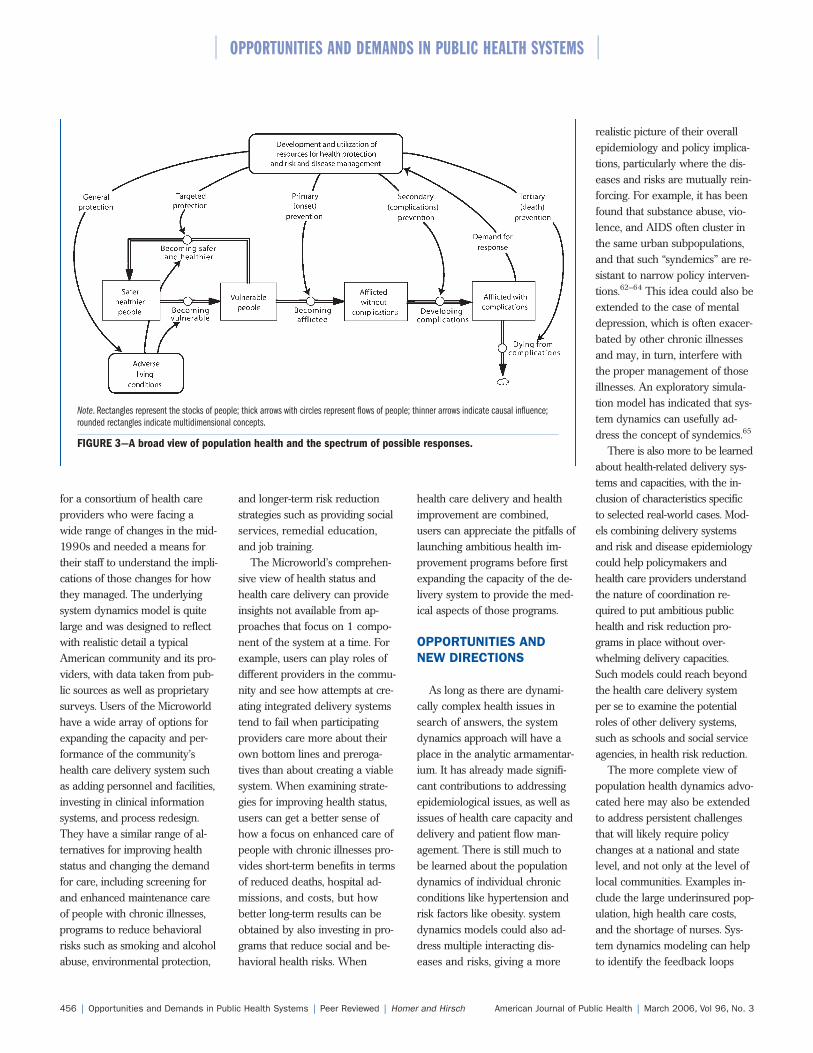
The preceding example, ex-ploring the interplay of a diseasedpopulation and the utilization ofhealth resources, gives some indi-cation of how a broader view ofhealth dynamics can yield insightsthat would be out of the grasp ofa less integrated approach. Butsystem dynamics modeling canand should go further still to in-corporate all the basic elementsof a modern ecological approachthat can help public health agen-cies achieve their goals of diseaseprevention, health promotion, andassurance of healthy conditions.Such a broad approach would en-compass disease, health and riskbehaviors, environmental factors,and resources that provide healthand social services or are in-volved in health-related socialtransformation.59,60 Figure 3
presents a system dynamics–typediagram for thinking about thedynamics of population healthin these broader terms. Thisframework has been used at theCDC in discussions about howthe agency should move forwardin an era of expanded publichealth goals and greater healthchallenges.56
Only a few system dynamicsstudies to date have gone be-yond diagramming to explore bymeans of simulation a more com-plete view of health like that seenin Figure 3. One such study is de-scribed by Homer and Milstein.43
Their community health modelexamines the typical feedback in-teractions among broadly definedstates of affliction prevalence, ad-verse living conditions, and thecommunity’s capacity to act. Likethe chronic disease preventionmodel presented earlier, the com-munity health model is relativelycompact and was not developedon the basis of any specific case.Nonetheless, sensitivity testing ofthe model across many possiblecommunity and affliction charac-teristics has led to some conclu-sions about how different typesof outside assistance are likelyto affect a community in theshort and long term. For example,the model suggests that outsideassistance focused on building acommunity’s capacity to act maybe the most effective place tostart in a community strugglingagainst disease and poverty, en-suring longer-term success in away that more direct interven-tions fail to do.
Hirsch and Immediato40,61
describe another more completeview of health. Their Health CareMicroworld, depicted in highlysimplified form in Figure 4, simu-lates the health status of andhealth care delivered to a popula-tion. The Microworld was created
American Journal of Public Health | March 2006, Vol 96, No. 3456 | Opportunities and Demands in Public Health Systems | Peer Reviewed | Homer and Hirsch
OPPORTUNITIES AND DEMANDS IN PUBLIC HEALTH SYSTEMS
Note. Rectangles represent the stocks of people; thick arrows with circles represent flows of people; thinner arrows indicate causal influence;rounded rectangles indicate multidimensional concepts.
FIGURE 3—A broad view of population health and the spectrum of possible responses.
for a consortium of health careproviders who were facing awide range of changes in the mid-1990s and needed a means fortheir staff to understand the impli-cations of those changes for howthey managed. The underlyingsystem dynamics model is quitelarge and was designed to reflectwith realistic detail a typicalAmerican community and its pro-viders, with data taken from pub-lic sources as well as proprietarysurveys. Users of the Microworldhave a wide array of options forexpanding the capacity and per-formance of the community’shealth care delivery system suchas adding personnel and facilities,investing in clinical informationsystems, and process redesign.They have a similar range of al-ternatives for improving healthstatus and changing the demandfor care, including screening forand enhanced maintenance careof people with chronic illnesses,programs to reduce behavioralrisks such as smoking and alcoholabuse, environmental protection,
and longer-term risk reductionstrategies such as providing socialservices, remedial education,and job training.
The Microworld’s comprehen-sive view of health status andhealth care delivery can provideinsights not available from ap-proaches that focus on 1 compo-nent of the system at a time. Forexample, users can play roles ofdifferent providers in the commu-nity and see how attempts at cre-ating integrated delivery systemstend to fail when participatingproviders care more about theirown bottom lines and preroga-tives than about creating a viablesystem. When examining strate-gies for improving health status,users can get a better sense ofhow a focus on enhanced care ofpeople with chronic illnesses pro-vides short-term benefits in termsof reduced deaths, hospital ad-missions, and costs, but howbetter long-term results can beobtained by also investing in pro-grams that reduce social and be-havioral health risks. When
health care delivery and healthimprovement are combined,users can appreciate the pitfalls oflaunching ambitious health im-provement programs before firstexpanding the capacity of the de-livery system to provide the med-ical aspects of those programs.
OPPORTUNITIES ANDNEW DIRECTIONS
As long as there are dynami-cally complex health issues insearch of answers, the systemdynamics approach will have aplace in the analytic armamentar-ium. It has already made signifi-cant contributions to addressingepidemiological issues, as well asissues of health care capacity anddelivery and patient flow man-agement. There is still much tobe learned about the populationdynamics of individual chronicconditions like hypertension andrisk factors like obesity. systemdynamics models could also ad-dress multiple interacting dis-eases and risks, giving a more
realistic picture of their overallepidemiology and policy implica-tions, particularly where the dis-eases and risks are mutually rein-forcing. For example, it has beenfound that substance abuse, vio-lence, and AIDS often cluster inthe same urban subpopulations,and that such “syndemics” are re-sistant to narrow policy interven-tions.62–64 This idea could also beextended to the case of mentaldepression, which is often exacer-bated by other chronic illnessesand may, in turn, interfere withthe proper management of thoseillnesses. An exploratory simula-tion model has indicated that sys-tem dynamics can usefully ad-dress the concept of syndemics.65
There is also more to be learnedabout health-related delivery sys-tems and capacities, with the in-clusion of characteristics specificto selected real-world cases. Mod-els combining delivery systemsand risk and disease epidemiologycould help policymakers andhealth care providers understandthe nature of coordination re-quired to put ambitious publichealth and risk reduction pro-grams in place without over-whelming delivery capacities.Such models could reach beyondthe health care delivery systemper se to examine the potentialroles of other delivery systems,such as schools and social serviceagencies, in health risk reduction.
The more complete view ofpopulation health dynamics advo-cated here may also be extendedto address persistent challengesthat will likely require policychanges at a national and statelevel, and not only at the level oflocal communities. Examples in-clude the large underinsured pop-ulation, high health care costs,and the shortage of nurses. Sys-tem dynamics modeling can helpto identify the feedback loops

March 2006, Vol 96, No. 3 | American Journal of Public Health Homer and Hirsch | Peer Reviewed | Opportunities and Demands in Public Health Systems | 457
OPPORTUNITIES AND DEMANDS IN PUBLIC HEALTH SYSTEMS
Source. Adapted from Hirsch and Immediato.61
Note. Episodes of illness in the bottom half of the diagram determine demand for care in the top half of the diagram. Rectangles in the bottomhalf represent stocks of ill patients. Rectangles in the top half represent stocks of provider capacity and workload. Arrows represent causalinfluences.
FIGURE 4—Overview of the health care microworld.
responsible for these problemsand point the way to policies thatcan make a lasting difference.
About the AuthorsJack Homer and Gary Hirsch are inde-pendent consultants specializing in the ap-plication of system dynamics methodologyin both the public and the private spheres.
Requests for reprints should be sent toJack Homer, 3618 Avalon Court,Voorhees, NJ 08043 (e-mail: [email protected]).
This article was accepted March 14,2005.
ContributorsThe authors worked together equally toconceptualize, write, and edit the article.
References1. Institute of Medicine (Committeeon Quality of Health Care in America).Crossing the Quality Chasm: A New
Health System for the 21st Century.Washington, DC: National AcademiesPress; 2001.
2. Institute of Medicine (Board onHealth Sciences Policy). Unequal Treat-ment: Confronting Racial and Ethnic Dis-parities in Health Care. Washington, DC:National Academies Press; 2003.
3. Zack MM, Moriarty DG, Stroup DF,Ford ES, Mokdad AH. Worseningtrends in adult health-related quality oflife and self-rated health—United States,1993–2001. Public Health Rep. 2004;119:493–505.
4. Lee P, Paxman D. Reinventingpublic health. Annu Rev Public Health.1997;18:1–35.
5. Heirich M. Rethinking Health Care:Innovation and Change in America. Boul-der, Colo: Westview Press; 1999.
6. Schorr LB. Common Purpose:Strengthening Families and Neighbor-hoods to Rebuild America. New York,NY: Doubleday/Anchor Books; 1997.
7. Sterman JD. Business Dynamics:
Systems Thinking and Modeling for aComplex World. Boston, Mass: Irwin/McGraw-Hill; 2000.
8. Forrester JW. Industrial Dynamics.Cambridge, Mass: MIT Press; 1961.
9. Forrester JW. Urban Dynamics.Cambridge, Mass: MIT Press; 1969.
10. Forrester JW. Counterintuitive be-havior of social systems. Technol Rev.1971;73:53–68.
11. Forrester JW. Information sourcesfor modeling the national economy. J AmStat Assoc. 1980;75:555–574.
12. Forrester JW, Senge PM. Tests forbuilding confidence in system dynamicsmodels. In: System Dynamics, TIMS Stud-ies in the Management Sciences. New York,NY: North-Holland; 1980:209–228.
13. Richardson GP. Feedback Thoughtin Social Science and Systems Theory.Philadelphia, Pa: University of Pennsyl-vania Press; 1991.
14. Tank-Nielsen C. Sensitivity analysisin system dynamics. In: Randers J, ed.Elements of the System Dynamics Method.
Cambridge, Mass: MIT Press; 1980:185–202.
15. Morecroft JDW. Rationality in theanalysis of behavioral simulation mod-els. Manage Sci. 1985;31:900–916.
16. Sterman J. System dynamics model-ing: tools for learning in a complex world.Calif Manage Rev. 2001; 43:8–25.
17. Homer JB. Why we iterate: scien-tific modeling in theory and practice.System Dynamics Rev. 1996;12:1–19.
18. Graham AK. Parameter estimationin system dynamics modeling. In: Ran-ders J, ed. Elements of the System Dy-namics Method. Cambridge, Mass: MITPress; 1980:143–161.
19. Luginbuhl W, Forsyth B, Hirsch G,Goodman M. Prevention and rehabilita-tion as a means of cost-containment: theexample of myocardial infarction. J Pub-lic Health Policy. 1981;2:1103–1115.
20. Hirsch GB, Wils W. Cardiovasculardisease in the Dutch population: amodel-based approach to scenarios. In:Ministry of Health: Conference on HealthCare Scenarios. The Hague, Nether-lands; 1984.
21. Homer J, Hirsch G, Minniti M,Pierson M. Models for collaboration:how system dynamics helped a commu-nity organize cost-effective care forchronic illness. System Dynamics Rev.2004;20:199–222.
22. Homer J, Jones A, Milstein B,Seville D, Essien J, Murphy D. The CDC’sdiabetes systems modeling project: devel-oping a new tool for chronic diseaseprevention and control. In: Kennedy M,Winch GW, Langer RS, Rowe JI, Yanni JM,eds. 22nd International System DynamicsConference. Oxford, England: SystemDynamics Society; 2004.
23. Roberts C, Dangerfield B. Model-ling the epidemiological consequencesof HIV infection and AIDS: a contribu-tion from operational research. J Opera-tional Res Soc. 1990; 41:273–289.
24. Homer JB, St. Clair CL. A modelof HIV transmission through needlesharing. Interfaces. 1991;21:26–49.
25. Dangerfield B, Fang Y, Roberts C.Model based scenarios for the epidemiol-ogy of HIV/AIDS: the consequences ofhighly active antiretroviral therapy. Sys-tem Dynamics Rev. 2001;17:119–150.
26. Royston G, Dost A, Townshend J,Turner H. Using system dynamics tohelp develop and implement policiesand programmes in health care in En-gland. System Dynamics Rev. 1999;15:293–313.
27. Ritchie-Dunham JL, Mendéz GalvanJF. Evaluating epidemic interventionpolicies with systems thinking: a casestudy of dengue fever in Mexico. SystemDynamics Rev. 1999;15:119–138.

American Journal of Public Health | March 2006, Vol 96, No. 3458 | Opportunities and Demands in Public Health Systems | Peer Reviewed | Homer and Hirsch
OPPORTUNITIES AND DEMANDS IN PUBLIC HEALTH SYSTEMS
28. Homer J, Ritchie-Dunham J, Rabbino H, Puente LM, Jorgensen J,Hendricks K. Toward a dynamic theoryof antibiotic resistance. System DynamicsRev. 2000;16:287–319.
29. Levin G, Roberts EB, Hirsch GB.The Persistent Poppy. Cambridge, Mass:Ballinger; 1975.
30. Homer JB. A system dynamicsmodel of national cocaine prevalence.System Dynamics Rev. 1993;9:49–78.
31. Roberts EB, Homer J, Kasabian A,Varrell M. A systems view of the smok-ing problem: perspective and limitationsof the role of science in decision-making.Int J Biomed Comput. 1982;13:69–86.
32. Tengs TO, Osgood ND, Chen LL.The cost-effectiveness of intensive na-tional school-based antitobacco educa-tion: results from the tobacco policymodel. Prev Med. 2001;33:558–570.
33. Lane DC, Monefeldt C, RosenheadJV. Looking in the wrong place forhealthcare improvements: a system dy-namics study of an accident and emer-gency department. J Operational ResSoc. 2000;51:518–531.
34. Wolstenholme EF. A managementflight simulator for community care. In:Cropper S, ed. Enhancing DecisionMaking in the NHS. Milton Keynes,UK: Open University Press; 1996.
35. Wolstenholme EF. A patient flowperspective of UK Health Services: ex-ploring the case for new “intermediatecare” initiatives. System Dynamics Rev.1999;15:253–271.
36. Hirsch G, Miller S. EvaluatingHMO policies with a computer simula-tion model. Med Care. 1974;12:668–681.
37. Hirsch GB, Killingsworth WR. Anew framework for projecting dentalmanpower requirements. Inquiry. 1975;12:126–142.
38. Levin G, Roberts EB, Hirsch GB,Kligler DS, Wilder JF, Roberts N. TheDynamics of Human Service Delivery.Cambridge, Mass: Ballinger; 1976.
39. Hirsch GB. Modeling the conse-quences of major incidents for healthcare systems. In: Kennedy M, Winch GW,Langer RS, Rowe JI, Yanni JM, eds.22nd International System DynamicsConference. Oxford, England: SystemDynamics Society; 2004.
40. Hirsch GB, Immediato CS. Mi-croworlds and generic structures as re-sources for integrating care and improv-ing health. System Dynamics Rev. 1999;15:315–330.
41. Hirsch G, Homer J. Modeling thedynamics of health care services for im-proved chronic illness management. In:Kennedy M, Winch GW, Langer RS,
Rowe JI, Yanni JM, eds. 22nd Interna-tional System Dynamics Conference.Oxford, England: System DynamicsSociety; 2004.
42. Hirsch G, Homer J. Integratingchronic illness management, improvedaccess to care, and idealized clinicalpractice design in health care organiza-tions: a systems thinking approach. In:3rd International Conference on SystemsThinking in Management. Philadelphia,Pa: AFEI/University of Pennsylvania;2004. Abstract available at: http://www.acasa.upenn.edu/icstm04/abstracts/019.rtf. Accessed November 11, 2005.
43. Homer J, Milstein B. Optimal deci-sion making in a dynamic model ofcommunity health. In: Proceedings ofthe 37th Annual Hawaii InternationalConference on System Sciences. Waikoloa,Hawaii: IEEE; 2004. Available at: http://csdl.computer.org/comp/proceedings/hicss/2004/2056/03/2056toc.htm.Accessed November 4, 2005.
44. Vennix JAM. Group Model-building:Facilitating Team Learning Using SystemDynamics. Chichester, UK: Wiley; 1996.
45. Anderson R. Populations, infectiousdisease and immunity: a very nonlinearworld. Philos Trans R Soc London B BiolSci. 1994;B346:457–505.
46. Kaplan EH, Craft DL, Wein LM.Emergency response to a smallpox at-tack: the case for mass vaccination. ProcNatl Acad Sci. 2002;99:10935–10940.
47. Gunning-Schepers LJ. The healthbenefits of prevention: a simulation ap-proach. Health Policy Special Issue.1989;12:1–255.
48. Naidoo B, Thorogood M, McPhersonK, Gunning-Schepers LJ. Modelling theeffects of increased physical activity oncoronary heart disease in England andWales. J Epidemiol Commun Health.1997;51:144–150.
49. Honeycutt AA, Boyle JP, BroglioKR, et al. A dynamic Markov model forforecasting diabetes prevalence in theUnited States through 2050. HealthCare Manage Sci. 2003;6:155–164.
50. Wolfson MC. POHEM: a frame-work for understanding and modellingthe health of human populations. WorldHealth Stat Q. 1994;47:157–176.
51. Halloran EM, Longini IM, Nizam A,Yang Y. Containing bioterrorist small-pox. Science. 2002;298:1428–1432.
52. Schlessinger L, Eddy DM.Archimedes: a new model for simulat-ing health care systems—the mathemati-cal formulation. J Biomed Inf. 2002;35:37–50.
53. Sterman JD. A skeptic’s guide tocomputer models. In: Grant L, ed. Fore-sight and National Decisions. Lanham,
Md: University Press of America; 1988:133–169.
54. Eyre H, Kahn R, Robertson RM,et al. Preventing cancer, cardiovasculardisease, and diabetes: a common agendafor the American Cancer Society, theAmerican Diabetes Association, and theAmerican Heart Association. DiabetesCare. 2004;27:1812–1824.
55. Brown R, Elixhauser A, Corea J,Luce B, Sheingod S. National Expendi-tures for Health Promotion and DiseasePrevention Activities in the United States.Washington, DC: Battelle MedicalTechnology Assessment and PolicyResearch Center; 1991. ReportBHARC-013/91-019.
56. Centers for Disease Control andPrevention. CDC’s futures initiative.Webcast presentation slides and script.Available at: http://www.phppo.cdc.gov/phtn/webcast/futures. AccessedNovember 11, 2005.
57. Repenning N. Understanding firefighting in new product development.J Prod Innovation Manage. 2001;18:285–300.
58. Repenning N, Sterman J. Nobodyever gets credit for fixing problems thatnever happened: creating and sustainingprocess improvement. Calif Manage Rev.2001;43:64–88.
59. Kari NN, Boyte HC, Jennings B.Health as a civic question. AmericanCivic Forum; November 28, 1994.Available at: http://www.cpn.org/topics/health/healthquestion.html. AccessedJanuary 5, 2005.
60. Green LW, Kreuter MW. HealthPromotion Planning: An Educational andEcological Approach. 3rd ed. MountainView, Calif: Mayfield; 1999.
61. Hirsch GB, Immediato CS. Designof simulators to enhance learning: ex-amples from a health care microworld.In: 16th International System DynamicsConference. Quebec City, Que: SystemDynamics Society; 1998.
62. Wallace R. A synergism of plagues.Environ Res. 1988;47:1–33.
63. Singer M. A dose of drugs, a touchof violence, a case of AIDS: conceptual-izing the SAVA syndemic. Free Inquiry.1996;24:99–110.
64. Singer M, Clair S. Syndemics andpublic health: Reconceptualizing diseasein bio-social context. Med Anthropol Q.2003;17:423–441.
65. Homer J, Milstein B. Communitieswith multiple afflictions: a system dy-namics approach to the study and pre-vention of syndemics. In: Davidsen PI,Mollona E, Diker VG, Langer RS, Rowe JI. 20th International System Dynamics Conference. Palermo, Italy:System Dynamics Society; 2002.





























