Embed Size (px)
Citation preview

8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 110
RATIONALE AND BASIC SCIENCE PERTINENT TOTHE PROCEDURE
Injury to the triangular fibrocartilage complex (FCC) is a com-mon cause of ulnar-sided pain and disability in the wrist
In 1989 Palmer1 proposed a classification system for disor-ders of the FCC that considers two basic categories traumatic(class 1) and degenerative (class 2) (able 54-1) Tese classes are
further subdivided into types depending on the location of thetear and the presence or absence of associated chondromalacicchanges Class 1 traumatic lesions are subdivided into four typesaccording to the tearrsquos location ype 1B injuries are peripheraltears located on the ulnar side of the FCC Recent advances inhistology and functional anatomy show that the ulnar side of theFCC is arranged in a complex tri-dimensional structure
According to structure and function the FCC is separatedinto three components the proximal triangular ligament the dis-tal hammock structure and the ulnar collateral ligament (UCL)2 Some authors debate the existence of the UCL34 or consider it tobe a part of the floor of the extensor carpi ulnaris (ECU) sheath56 eventually including some surrounding loose ligamentous tissue2 However the functional UCL can be assimilated to the distalhammock structure since they both share the same function of
supporting and suspending the ulnar carpus2
Te distal ham-mock structure and the UCL should be considered as the distalcomponent of the FCC (dc-FCC) which is the opposite ofthe proximal component (pc-FCC) represented by the proxi-mal triangular ligament (Fig 54-1) Te proximal triangular liga-ment is a strong ligamentous structure that originates from thefovea ulnaris and spans to the ulnar corners of the distal radius with two limbsmdashvolar and dorsal It should be considered thetrue radioulnar ligament that stabilizes the distal radioulnar joint(DRUJ)
Because of the intensity and direction of the traumatic forceeither the dc-FCC or the pc-FCC or both may be torn Tere-fore ulnar-sided pain reduced grip strength decreased forearmrotation and clinical signs of DRUJ instability may be presentaccordingly
Appropriate management of peripheral tears should aim at re-
storing the original anatomy by direct suture or osseous reattach-ment of the FCC by open or arthroscopic repair7
Many arthroscopic techniques have been proposed that su-ture the torn FCC to the dorsal ulnocarpal joint capsule andthe ECU tendon subsheath Tese techniques restore FCCtautness and thus improve the patientrsquos symptoms However ar-throscopic suture is of limited benefit when FCC tears involvethe pc-FCC and when the DRUJ is clinically unstable In theseinstances an arthroscopic repair is unable to reconstitute the
preinjury anatomy and provide adequate joint stability Tereforeopen repair is generally recommended since it is the only tech-nique that allows for a direct reattachment of the proximal compo-nent of the FCC to its foveal insertion8 However a careful andrather extensive exposure of the distal radioulnocarpal joint910 isrequired to perform a FCC reattachment via either transosseoussutures passed through drill holes1011 or bone anchors12
Continuous advances in the understanding of the intra-
articular anatomy and the kinematics of the wrist8 as well asthe introduction of new volar portals13 have contributed to theemergence of an ldquoall-arthroscopicrdquo attitude toward ulnar-sideddisorders of the wrist for many surgeons14ndash16
Tis chapter describes a method of an arthroscopic-assistedfoveal reattachment using a newly devised DRUJ working por-talmdashthe direct foveal (DF) portalmdashwhich is indicated for repair-able proximal or complete peripheral FCC tears associated withDRUJ instability but without secondary degenerative changes
CLINICAL CONSIDERATIONS
Te typical candidate for an arthroscopic FCC foveal reattach-ment is a patient complaining of ulnar-sided wrist pain usuallyafter a fall on an outstretched hand or a violent traction and twist-
ing injury of the wrist or forearmPatients may complain that their wrist spontaneously ldquogives wayrdquo when they are trying to open a bottle rotate a steering wheel turn a door handle or hold an object in their hand duringforearm rotation Te suspected diagnosis is achieved by meansof special provocative maneuvers and diagnostic tests817 Pain isexacerbated by passive forearm rotation and may be associated with the presence of a click or crepitus or an intra-articular grind-ing sensation Resistance rotational movements are often weakand reproduce the patientrsquos complaints Te ulnar foveal sign18 ispositive that is the patient has point tenderness over the ulnarcapsule just volar to the ECU tendon Provided that the forearmmuscles are relaxed provocative maneuvers for DRUJ instabilityshow greater laxity in the painful wrist compared with the oppo-site side Hypertonicity of the muscular stabilizers of the DRUJmay lead to false-negative findings hence it is recommended that
DRUJ stability should be evaluated under regional anesthesia be-fore the operation
Although all patients presenting with acute or chronic wristpain should have radiographs taken of the wrist these are usu-ally of limited help in diagnosing isolated FCC tears but theymay reveal an associated ulnar styloid fracture or nonunion Stillthe usefulness of magnetic resonance imaging (MRI) even withintra-articular gadolinium is a controversial issue Whereas anMRI arthrogram may be both sensitive and specific in diagnosing
54C H A P T E R Repair of the Foveal Insertion of the
TFCC Through the DF Portal Andrea Atzei MD and Riccardo Luchetti MD
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 210
Part IX Ligament InstabilityTears560
a tear it has not shown similar accuracy in assessing tear sizeand location19 Studies comparing specificity and sensitivity ofarthrography MRI and arthroscopy confirm arthroscopic visu-alization of a FCC tear to be the gold standard for definitivediagnosis2021
Arthroscopy of the radiocarpal joint (RC-Arth) and theDRUJ (DRU-Arth) allows for a thorough evaluation of the tearrsquoscharacteristics RC-Arth is used to evaluate the dc-FCC22 Tetear is visualized in the dorsoulnar corner of the FCC TeFCC tension is evaluated by the trampoline test11 and the hooktest Te trampoline test evaluates the FCC resilience (tram-
poline effect) by applying a compressive load across it with theprobe Te test is positive when there is a peripheral FCC tearsince the FCC becomes soft and compliant Te hook test con-sists of applying traction to the ulnarmost border of the FCC with the probe inserted through the 4-5 or 6R portal Te test ispositive when the FCC can be pulled upward and radially to- ward the center of the radiocarpal joint (Fig 54-2) It is a usefulmaneuver for detecting a foveal disruption of the pc-FCC23
DRU-Arth is the only method for detecting any ligamentouslaceration of the pc-FCC or avulsion of the foveal attachmentsIt is mandatory when a hook test yields positive results or when theFCC tear is associated with clinical signs of DRUJ instability
Because the DRUJ is a very narrow and tight joint it may bediffi cult to perform DRU-Arth when the pc-FCC is still intactHowever when the pc-FCC is torn the articular disk is looseand more space is available for DRUJ exploration An 18-gauge
hypodermic needle may be placed percutaneously 1 cm proximalto the 6U portal It will enter the joint close to the fovea and maybe used to lift the articular diskmdashthus enlarging the visual fieldmdashand to palpate the pc-FCC Furthermore DRU-Arth allowsDRUJ cartilage to be examined for chondromalacic changes
RC-Arth and DRU-Arth provide a combination of findingsthat should be considered when deciding on the appropriatetreatment of a FCC tear Tey are summarized in the followingfour parameters22
Lacerated Components of the Triangular Fibrocartilage
Complex
Establishing the extent of FCC disruption is of utmost impor-tance Each component of the FCC that is distal (dc-FCC)and proximal (pc-FCC) may be involved either separately or
in associationTree types of ligamentous damage are possible
1 Distal tear (isolated tear of the distal component of the TFCC) When only the dc-FCC is lacerated the trampoline test re-sult is positive for loss of FCC resilience but the hook testresult is negative Integrity of the foveal attachments of thepc-FCC is confirmed by DRU-Arth
2 Complete tear (tear of both distal and proximal components of theTFCC) Complete peripheral FCC tear involves both com-ponents of the FCC A tear of the dc-FCC is visible duringRC-Arth and a pc-FCC avulsion is demonstrated by DRU- Arth Both trampoline and hook test results are positive
3 Proximal tear (isolated tear of the proximal component of theTFCC) An isolated avulsion of the pc-FCC from the foveaulnaris can be demonstrated by DRU-Arth which is manda-
tory to achieve the correct diagnosis Standard RC-Arth failsto show any abnormalities of the contour and capsular reflec-tion of the FCC even though both trampoline and hooktests show positive results
Surgical treatment varies according to which FCC componentis lacerated22 In case of a proximal or complete tear a FCC rein-sertion onto the fovea ulnaris is recommended However in case ofa distal tear arthroscopic suturing of the FCC to the dorsal ulno-carpal joint capsule and the ECU tendon subsheath is appropriate
TABLE 549830851
Palmer Classi1047297cation of TFCC Injuries
Class1 Traumatic Injuries
A Central per foration of the disk proper
B Peripheral avulsion from the ulna
Without styloid fractureWith styloid fracture
C Distal avulsion from the carpus
D Radial avulsionWithout sigmoid notch fractureWith sigmoid notch fracture
Class 2 Degenerative Injuries
A TFCC wear
B TFCC wear + lunate andor head chondromalacia
C TFCC perforation + lunate andor head chondromalacia
D TFCC perforation + lunate andor head chondromalacia +lunotriquetral ligament perforation
E TFCC per foration + ulnocarpal ar thritis
TFCC triangular 1047297brocartilage complex
Classi1047297cation from Palmer AK Triangular 1047297brocartilage complex lesions a classi1047297ca-tion J Hand Surg [Am] 198914594ndash606
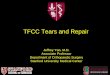
FIGURE 54-1 Coronal slice of the ulnar wrist at the level ofthe fovea The triangular 1047297brocartilage complex
(TFCC) is outlined It is separated into the distal component of the TFCC (D) formed by the ulnar collateral ligament and the distal ham-mock structure and the proximal component (P) represented by theproximal triangular ligament which originates from the ulnar foveaand the styloid (From Atzei A New trends in arthroscopic manage-ment of type 1-B TFCC injuries with DRUJ instability J Hand Surg [Eur]2009 Epub ahead of print)
dc-TFCC
pc-TFCC
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 310
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
Reducibility of the Triangular Fibrocartilage Complex Tear With a small FCC tear as well as an avulsion type of rupturethe tearrsquos edges can be reapproximated or reduced easily and aFCC repair can be successfully performed By contrast in thepresence of a massive rupture of the FCC andor retraction ofthe ligamentous remnants reapproximation of the avulsed liga-ment or repair of the FCC tear to its anatomic position is notfeasible Terefore reconstruction with tendon graft should betaken into consideration
Healing Potential of the Triangular Fibrocartilage
Complex Tear
Chronic midsubstance ligamentous tears showing degeneratedor necrotic edges cannot be debrided back to a well-vascularizedarea therefore direct repair is unlikely to provide adequate heal-
ing Te same applies to the elongated and frayed ligament aftera failed suture direct repair is unlikely to be successful and aFCC reconstruction with tendon graft is recommended In ourexperience pc-FCC tears have a good healing potential for upto 3 months after injury (acute tears) whereas tears treated from 3to 6 months after injury (subacute tears) have unpredictable char-acteristics More chronic tears usually have a poor healing poten-tial Moreover congenital dysmorphisms of the styloid and fovealarea of the ulna (eg styloid hypoplasia and flattened ulnar head)represent other conditions that are associated with poor healingpotential after a repair and hence require reconstruction
Cartilage Status of the Distal Radioulnar Joint
Healthy cartilage status is of the utmost importance when plan-ning any reconstructive surgery for FCC disruption After high-energy trauma a cartilage defect over the ulnar head and sigmoid
notch may have been produced at the time of the initial injury Alternatively degenerative chondromalacia may be the conse-quence of the altered joint kinematics resulting in chronic DRUJinstability Well-preserved cartilage is a sine qua non for every typeof ligament repair or reconstruction of the DRUJ When DRU- Arth shows a chondral lesion some type of salvage arthroplasty isrecommended as an alternative
Based on the above-mentioned criteria a novel classification22 is defined that considers the variety of FCC peripheral tears and
provides guidelines for specific treatment modalities repair (sutureor foveal insertion) reconstruction with tendon graft or salvageprocedures (arthroplasty or joint replacement) (able 54-2)
INDICATIONS FOR FOVEAL REPAIR
When pain and impaired function show no improvement aftera trial of conservative treatment a foveal repair23 is indicated with type 1B FCC injuries of the Palmer classification Tis isrepresented as both class 2 and 3 tears (complete and isolatedproximal repairable FCC tears) in the authorsrsquo proposed clas-sification
CONTRAINDICATIONS
A foveal reattachment is not indicated for classes 1 4 and 5tears in the authorsrsquo classificationClass 1 (an isolated distal repairable tear) should be treated by
arthroscopic suturing of the FCC to the dorsal ulnocarpal jointcapsule and the ECU tendon subsheath Class 4 (nonrepairabletears owing to either a large tear size or poor quality of the tornligaments) should undergo ligament reconstruction by tendongraft as either an open24 or arthroscopic procedure2225
Chronic Essex-Lopresti injuries in which longitudinal stabil-ity of the forearm is altered as a result of the laceration of theinterosseous membrane are not amenable to simple FCCreattachment
Other absolute contraindications include previous soft tis-sue infection osteomyelitis and severe osteoporosis of the ulnarhead
Relative contraindications include a positive ulnar variance
with secondary ulnar impaction and carpal chondromalacia
SURGICAL TECHNIQUE
Operative Setup and Diagnostic Arthroscopy
Te patient is positioned supine with the affected arm on a handtable and a padded tourniquet on the proximal arm After a bra-chial plexus block has been administered the DRUJ laxity is
FIGURE 54-2 The hook test A In a left wrist the probe is inserted via the 6R portal through the triangular 1047297brocartilage complex (TFCC) tear Traction is applied to the ulnarmost border of the TFCC B The test result is considered positive when the TFCC (outlined by the dotted
line) can be pulled upward and radially as the pc-TFCC is interrupted or avulsed from the fovea (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopicfoveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 410
Part IX Ligament InstabilityTears562
TABLE 549830852
Arthroscopic Classi1047297cation of TFCC Peripheral Tears
ClinicalDRUJ In-stability
DistalCompo-nent
ProximalCompo-nent
TearReduc-ibility
HealingPoten-tial
DRUJCartilage Treatment
Class1
Repairabledistal tear D
P
None ndashslight
Torn Intact Easy Good Good RepairSuture(ligament-to-capsule)
Class2
Repairablecompletetear
DP
Mild ndashsevere
Torn Torn Easy Good Good RepairFoveal
re1047297xation
Class3
Repairableproximaltear
DP
Mild ndash severe
Intact Torn Easy Good Good RepairFoveal
re1047297xation
Class4-A
Non-repairablemassivetear
Non-reducible
D
P
Severe Torn Torn Impossible Good Good Reconstruction Tendon graft
Class4-B
Non-repairable
Failedsuture
Frayedligament
DP
Mild ndash severe
Torn Torn Impossible Poor Good Reconstruction Tendon graft
Class5
ArthriticDRUJ D
P
Mild ndashsevere
dagger dagger dagger dagger Poor SalvageArthroplasty
or jointreplacement
After debridement to bleeding edgesdagger Variable 1047297ndings that would not change treatment
Novel classi1047297cation22 based on arthroscopic 1047297ndings provides guidelines for treatment of diff erent triangular 1047297brocartilage complex (TFCC) peripheral tears The 1047297rst columnreports 1047297ndings of clinical instability of the distal radioulnar joint (DRUJ ) Classes 1ndash3 are repairable lesions that should be treated by either suture or foveal re1047297xation Classes4-A and 4-B are nonrepairable lesions that should undergo reconstruction by tendon graf t Class 5 includes diff erent conditions whose main characteristic consists of cartilagedegeneration of the DRUJ Such cases should be treated by salvage procedures that is arthroplasties or prosthetic joint replacement From Atzei A New trends in ar throscopicmanagement of type 1-B TFCC injuries with DRUJ instability J Hand Surg [Eur] 2009 Epub ahead of publishing
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 510
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
examined again before starting the arthroscopic procedure Com-plete forearm muscle relaxation following anesthesia may revealpreviously undetected DRUJ instability Te upper limb is exsan-guinated and the tourniquet is inflated to 250 mm Hg
A standard wrist arthroscopy setup is used26 Te wrist is sus-pended by finger traps using a wrist traction tower with approxi-
mately 10 to 15 pounds of traction depending on the size ofthe extremity Joint distention by saline infusion is usually notrequired to completely visualize the joint26 Te authorsrsquo pref-erence is to use a dry technique which facilitates arthroscopicrepair methods2728
A 27-mm arthroscope is used routinely but the 19-mm ar-throscope is used for smaller wrists Te wrist is systematicallyevaluated by RC-Arth with the scope in the 3-4 portal Care istaken to detect any associated disorders of the ulnar carpus
ears of the dc-FCC are visualized on the dorsoulnar portionof the articular disk and are frequently covered by hypertrophicsynovitis or fibrovascular granulation tissue which is removed with a small motorized shaver
A probe is inserted into the 6R portal to palpate the articulardisk and to assess the tension to the FCCmdashby the trampolinetest and the hook test
If the FCC is redundant and tests are positive for loss ofnormal resilience pc-FCC integrity and tautness are evaluatedthrough DRU-Arth
Te forearm is supinated the traction reduced and the DRUJexplored through the distal DRUJ portal In smaller wrists use ofa volar ulnar (VU) portal is recommended29 Scope insertion iseasier when the pc-FCC is torn since the articular disk is looseand more joint space is available DRU-Arth shows the ligamen-tous laceration or avulsion of the pc-FCC from the fovea Fora preliminary assessment of pc-FCC tautness an 18-gaugeneedle is inserted percutaneously about 1 cm proximal to the 6Uportal with the forearm held in full supination
When a FCC Palmer type 1B tear is associated with DRUJinstability the most common finding is the combination of a dc-FCC tear and a pc-FCC avulsion (complete FCC tear class 2)
Less frequently a pc-FCC tear is present as an isolated finding(proximal FCC tear class 3) In the latter case a standard RC- Arth reveals a normal FCC appearance which may lead to themisdiagnosis of a normal FCC since the pc-FCC tear can bedemonstrated only by DRU-Arth For this reason DRU-Arth isconsidered mandatory in cases of a suspected FCC tear that isassociated with DRUJ instability
Repair Technique
Repair of the foveal insertion of the FCC is performed by reat-tachment of the pc-FCC through a suture screw or anchor23
Te procedure begins with debridement of the foveal region as well as the torn edges of the FCC back to healthy tissue using asmall motorized shaver inserted through the 6R portal Althoughthe fovea can be debrided from the radiocarpal joint through theFCC tear it is recommended to establish a separate DRUJ por-
tal not only to remove the ligamentous remnants and refresh thebone at the fovea but also to drill and insert the suture screwanchor A dedicated working portal named the direct foveal (DF)portal has been devised to provide access to the fovea ulnaris2223
Te DF portal is located about 1 cm proximal to the 6U portaland is created with the forearm held in full supination Full fore-arm supination produces dorsal displacement of the ulnar styloidand the ECU tendon and uncovers the volar aspect of the distalulna on wristrsquos ulnar side (Fig 54-3) Tus the fovea and the
ulnarmost area of the distal ulna become subcutaneous and maybe reached through a very limited exposure Te DF portal is lesstechnically demanding compared with the formal VU portal29 but its use is limited to the introduction of working instrumentsin the area of the ulnar styloid and fovea (Fig 54-4)
After portal placement is checked under arthroscopic control
with an 18-gauge needle the longitudinal skin incision of the 6Uportal is extended proximally between the ECU and the flexorcarpi ulnaris (FCU) for a total length of 2 to 25 cm Troughthis mini-open approach the dorsal sensory branch of the ulnarnerve (DSBUN) and its transverse branches are identified andprotected by careful subcutaneous dissection Te risk of damag-ing the DSBUN is further reduced as the forearm is supinatedgiven that the DSBUN is displaced more volarly and along aslacker path than when the forearm is held in neutral position
Te extensor retinaculum is exposed and split along the courseof its fibers Te DRUJ capsule is incised longitudinally to reachthe distal articular surface of the ulnar head under the FCCTe fovea is located volarly at the base of the ulnar styloid justlateral to the capsule
With the scope in the distal DRUJ portal a small shaver orcuret can be inserted through the DF portal to refresh the torn
avulsed ligament to remove the inflammatory fibrovascular tissuefrom the fovea and to prepare it for suture screwanchor inser-tion Curettage of the fovea can also be performed as a mini-openprocedure
Screwanchor drilling and insertion are performed as a mini-open procedure as well (Fig 54-5) Te fovea is palpable as anarea of soft bone at the base of the ulnar styloid just lateral tothe capsule A power drill and intraoperative fluoroscopy are notrequired although the latter may be advisable for the less experi-enced surgeon
It is recommended to use a screwanchor that supports a pairof sutures so that a distinct suture can be passed through eachlimb of the radioulnar ligament Tis also improves the strengthof the repair by recreating a broader footprint of the pc-FCCanalogous to a rotator cuff repair in the shoulder30 Te authors
prefer to use a 28 or 32 titanium screw with two preloaded non-absorbable 2-0 Ultrabraid sutures (winfix Smith amp Nephew Andover MA) or a 35-mm absorbable screw preloaded withtwo 2-0 FiberWire sutures (Bio-Corkscrew Arthrex Naples FL)
Once the screw is in place sutures should exit the DF por-tal from underneath the FCC (Fig 54-6) Ten the wrist isplaced back in neutral pronosupination so that the screwrsquos head isbrought under the ulnarmost part of the FCC
Te suture ends are inserted into the tip of a 25-gauge needleor preferably a uohy needle to facilitate passage through theFCC
With the scope in the 3-4 portal the first suture is inserted inan outside-in fashion from the DF portal close to the FCCrsquospalmar contour to hold the palmar limb of the radioulnar liga-ment (Fig 54-7) A grasper is used to retrieve the suture from the6U portal (Fig 54-8) Te same procedure is repeated for sutur-
ing the dorsal limb of the radioulnar ligamentTe wrist traction is then released and the forearm is held in
neutral rotation Te surgical assistant maintains the ulnar head inreduced position Te sutures are tied under arthroscopic controlusing a small knot-pusher ensuring adequate pc-FCC compres-sion against the distal ulna (Fig 54-9) Knots should be located atthe prestyloid recess or just outside the DRUJ capsule (Fig 54-10)
RC-Arth is used as a control to ensure complete tear closureEven in the larger type 2 FCC peripheral tears it is seldom
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 610
Part IX Ligament InstabilityTears564
necessary to apply any further ligament-to-capsule sutures toclose off the dc-FCC
Te DRUJ is evaluated for complete range of pronosupinationand residual instability
Te DRUJ capsule and the opening between retinaculum fi-bers are approximated with two PDS 4-0 stitches Skin is closedby a subcuticular running suture
Postoperative Treatment
Te patient is placed in a long-arm splint in neutral forearm rota-tion for the first week which is substituted by a short Muumlnster
splint for another 2 weeksFull wrist flexionextension can be started as early as 3 weeks post-
operatively During the first week of rehabilitation progressive fore-arm rotation is allowed but the splint is still worn between exercises
During the following 6 weeks the patient is not permitted toperform any resistance movements Progressive resistance wrist-and hand-strengthening exercises are begun after the sixth weekuntil the patient is able to bear weight on the operated wrist Sportand heavy work activities are started 3 months postoperatively
COMPLICATIONS
Few complications should be encountered during arthroscopic-assisted palmar repair of the foveal insertion of the FCC providedthat there is careful application of standard arthroscopic principlesand of the described surgical technique Te most serious complica-tion is potential injury to the DSBUN which is related to surgicalexperience It can be prevented by careful dissection techniques anda sound understanding of the underlying anatomy and its variationfollowing forearm rotation ransitory neuropraxia of the DSBUNmay be observed which recovers spontaneously in 3 to 4 months
Te surgical scar of the ulnar side of the wrist may adhere to deeperstructures and become painful during the first stages of physicaltherapy especially after a prolonged period of wrist immobilization
As in other arthroscopic procedures infection remains a risk which is usually prevented by a prophylactic dose of parenteralantibiotics before initiating the procedure
Te dry technique of joint exploration27 is recommended toreduce soft tissue infiltration and swelling by the continuous leak-ing of saline through the portals
FIGURE 54-3 Full forearm supination is required to create the direct foveal (DF) portal After supination the ulnar styloid and the extensorcarpi ulnaris tendon displace dorsally and the fovea and the ulnarmost area of the distal ulna become subcutaneous (From
Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
Fovea
Neutral PS Supination
DF
portal
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 710
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-5 Screwanchor drilling and insertion are performed as a mini-open procedure through the direct foveal portal (From Atzei ARizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar
joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
FIGURE 54-4 The direct foveal (DF) portal is located about 1 cm proximal to the 6U portal It has been devised as a working portal toprovide access to the area of the ulnar styloid and fovea With the scope in the distal radioulnar joint portal a curet
or small shaver is inserted through the DF portal to refresh the tornavulsed ligament and the fovea (From Atzei A Rizzo A Luchetti R Fairplay TArthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up ExtremSurg 200812226ndash235)
6-U
DF
A B
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 810
Part IX Ligament InstabilityTears566
FIGURE 54-6 Once the screw is in place sutures should exit the direct foveal portal from underneath the triangular 1047297brocartilage complex(TFCC) When the wrist is placed back in neutral pronosupination the screwrsquos head is brought under the TFCC (From Atzei A
Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability TechHand Up Extrem Surg 200812226ndash235)
Te technique of arthroscopic-assisted palmar repair of the fo-veal insertion of the FCC has a learning curve However once
the technique is mastered the rate of complications for this pro-cedure is comparable to that of larger series of common wristarthroscopic procedures31
RESULTS
Te authorsrsquo clinical experience started in 2001 and up until now we have operated on 37 FCC tears (29 type 2 FCC peripheraltears and 8 type 3 tears)
In a control series study 18 patients (13 males and5 females with a mean age of 342) were investigated prospec-
tively for a minimum follow-up of 1 year (average 18 monthsmaximum 37 months) All patients had a history of traumacomplained of pain in the ulnar fovea and had clinical signsof DRUJ instability ranging from mild (10 patients) to mod-erate (8 patients) Although radiographs showed a positive ul-nar variance in three patients there were no detectable signsof ulnocarpal impaction or carpal degenerative chondropa-thy Arthroscopy revealed a Palmer type 1B ulnar avulsionof the FCC in all patients Fourteen cases were classified as
FIGURE 54-7 With the scope in the 3-4 portal the 1047297rst suture end is inserted into the tip of a 25-gauge needle (preferably a Tuohy needle) The needle is passed through the triangular 1047297brocartilage complex (TFCC) in an outside-in fashion via the direct foveal portal
toward the palmar contour of the TFCC (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complexperipheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 910
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-8 A grasper is inserted through the 6U portal and used to retrieve the suture (From Atzei A Rizzo A Luchetti R Fairplay T Arthro-scopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up
Extrem Surg 200812226ndash235)
FIGURE 54-9 The suture is tied under arthroscopic control using a small knot-pusher The pc-TFCC (proximal component of the triangular1047297brocartilage complex) is pushed forcefully against the distal ulna provided that the wrist traction is released the forearm is
held in neutral rotation and the ulnar head is reduced by the assistant (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
complete FCC peripheral tears (type 2) and four as proximaltears (type 3)
At fol low-up evaluation the patients showed an increasedrange of motion (from 907 to 96 of the contralateralside) and grip strength (from 73 to 90) Pain decreasedfrom 83 to 12 on a 10-point visual analogue scale Gripstrength and pain changes reached statistical significance
(P lt 005) he Modified Mayo Wrist Score was excellentin 14 patients good in 3 and fair in 1 A total of 944 ofthe results scored excellent and good DASH (disabilities ofthe arm shoulder and hand) score averaged 105 Fifteenpatients (833) resumed previous work and recreation-al activities and 3 patients (167) returned to restrictedemployment
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 1010
Part IX Ligament InstabilityTears568
REFERENCES
1 Palmer AK riangular fibrocartilage complex lesions a classification J HandSurg [Am] 198914594ndash606
2 Nakamura Yabe Y Horiuchi Y Functional anatomy of the triangularfibrocartilage complex J Hand Surg [Br] 199621581ndash586
3 Palmer AK Werner F W Te triangular fibrocartilage complex of the wristmdashanatomy and function J Hand Surg [Am] 19816153ndash162
4 Adams BD Holly K A Strains in the articular disk of the triangular fibro-cartilage complex a biomechanical study J Hand Surg [Am] 199318919ndash925
5 Benjamin M Evans E J Pemberton D J Histological studies on the triangularfibrocartilage complex of the wrist J Anat 199017259ndash67
6 Kauer JMG Te distal radioulnar joint anatomic and functional consider-ations Clin Orthop 199227537ndash45
7 Atzei A Luchetti R Garcia-Elias M Lesioni capsulo-legamentose dellaradio-ulnare distale e fibrocartilagine triangolare In Landi A Catalano FLuchetti R (eds) rattato di Chirurgia della Mano Verduci Editore Roma2006 pp 159ndash187
8 Kleinman WB Stability of the distal radioulnar joint biomechanics patho-physiology physical diagnosis and restoration of function What we havelearned in 25 years J Hand Surg [Am] 2007321087ndash1106
9 Garcia-Elias M Smith DE Llusa M Surgical approach to the triangularfibrocartilage complex ech Hand Up Extrem Surg 20037(4)134ndash140
10 Nakamura Nakao Y Ikegami H et al Open repair of the ulnar disruptionof the triangular fibrocartilage complex with double three-dimensional mat-tress suturing technique ech Hand Up Extrem Surg 20048(2)116ndash123
11 Hermansdorfer JD Kleinman WB Management of chronic peripheraltears of the triangular fibrocartilage complex J Hand Surg [Am] 199116340ndash346
12 Chou KH Sarris IK Sotereanos DG Suture anchor repair of ulnar-sidedtriangular fibrocartilage complex tears J Hand Surg [Br] 200328546ndash550
13 Slutsky D J Clinical applications of volar portals in wrist arthroscopy echHand Up Extrem Surg 20048(4)229ndash238
14 omaino M Weiser R Combined arthroscopic FCC debridement and wa-fer resection of the distal ulna in wrists with triangular fibrocartilage complextears and positive ulnar variance J Hand Surg [Am] 2001261047ndash1052
15 Hanker G J Management of ulnar impaction syndrome In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 63ndash71
16 Moskal M J Savoie FH III Management of lunotriquetral instability InGeissler WB (ed) Wrist Arthroscopy New York Springer-Verlag 2005pp 94ndash101
17 Atzei A Luchetti R Clinical approach to the painful wrist In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 185ndash195
18 ay SC omita K Berger R A Te ldquoulnar fovea signrdquo for defining ulnar wrist pain an analysis of sensitivity and specificity J Hand Surg [Am]200732(4)438ndash444
19 Zanetti M Bram J Hodler J riangular fibrocartilage and intercarpal liga-ments of the wrist does MR arthrography improve standard MRI J Magn
Reson Imaging 19977 (3)590ndash59420 Pederzini L Luchetti R Soragni O et al Evaluation of the triangular
fibrocartilage complex tears by arthroscopy arthrography and magnetic reso-nance imaging Arthroscopy 19928191ndash197
21 Fulcher S Poehling G Te role of operative arthroscopy for the diag-nosis and treatment of lesions about the distal ulna Hand Clin 199814285ndash296
22 Atzei A New trends in arthroscopic management of type 1-B FCC injuries with DRUJ instability J Hand Surg [Eur] 2009Epub ahead of print
23 Atzei A Rizzo A Luchetti R Fairplay Arthroscopic foveal repair of tri-angular fibrocartilage complex peripheral lesion with distal radioulnar jointinstability ech Hand Up Extrem Surg 200812226ndash235
24 Adams BD Anatomic reconstruction of the distal radioulnar ligaments forDRUJ instability ech Hand Up Extrem Surg 20004154ndash160
25 Atzei A Luchetti R Borelli PP et al Arthroscopic FCC reconstruction bytendon graft Riv Chir Mano 200643(3)370ndash376
26 Atzei A Luchetti R Sgarbossa A et al Set-up portals and normal explora-tion in wrist arthroscopy Chir Main 200625S131ndashS144
27 del Pintildeal F Garciacutea-Bernal F J Pisani D et al Dry arthroscopy of the wrist
surgical technique J Hand Surg [Am] 200732119ndash12328 del Pintildeal F Garciacutea-Bernal F J Delgado J et al Correction of malunited
intra-articular distal radius fractures with an inside-out osteotomy technique J Hand Surg [Am] 200531(6)1029ndash1034
29 Slutsky D J Distal radioulnar joint arthroscopy and the volar ulnar portalech Hand Up Extrem Surg 200711(1)38ndash44
30 Lo IK Y Burkhart SS Double-row arthroscopic rotator cuff repair re-establishing the footprint of the rotator cuff Arthroscopy 200319(9)1035ndash1042
31 Luchetti R Atzei A Rocchi L Incidence and causes of failures in wristarthroscopic techniques Chir Main 200625(1)48ndash53
FIGURE 54-10 At the end of the procedure the knots of bothsutures are located at the level of the 6U portal just
outside the distal radioulnar joint capsule or in the prestyloid recess(From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)

8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 210
Part IX Ligament InstabilityTears560
a tear it has not shown similar accuracy in assessing tear sizeand location19 Studies comparing specificity and sensitivity ofarthrography MRI and arthroscopy confirm arthroscopic visu-alization of a FCC tear to be the gold standard for definitivediagnosis2021
Arthroscopy of the radiocarpal joint (RC-Arth) and theDRUJ (DRU-Arth) allows for a thorough evaluation of the tearrsquoscharacteristics RC-Arth is used to evaluate the dc-FCC22 Tetear is visualized in the dorsoulnar corner of the FCC TeFCC tension is evaluated by the trampoline test11 and the hooktest Te trampoline test evaluates the FCC resilience (tram-
poline effect) by applying a compressive load across it with theprobe Te test is positive when there is a peripheral FCC tearsince the FCC becomes soft and compliant Te hook test con-sists of applying traction to the ulnarmost border of the FCC with the probe inserted through the 4-5 or 6R portal Te test ispositive when the FCC can be pulled upward and radially to- ward the center of the radiocarpal joint (Fig 54-2) It is a usefulmaneuver for detecting a foveal disruption of the pc-FCC23
DRU-Arth is the only method for detecting any ligamentouslaceration of the pc-FCC or avulsion of the foveal attachmentsIt is mandatory when a hook test yields positive results or when theFCC tear is associated with clinical signs of DRUJ instability
Because the DRUJ is a very narrow and tight joint it may bediffi cult to perform DRU-Arth when the pc-FCC is still intactHowever when the pc-FCC is torn the articular disk is looseand more space is available for DRUJ exploration An 18-gauge
hypodermic needle may be placed percutaneously 1 cm proximalto the 6U portal It will enter the joint close to the fovea and maybe used to lift the articular diskmdashthus enlarging the visual fieldmdashand to palpate the pc-FCC Furthermore DRU-Arth allowsDRUJ cartilage to be examined for chondromalacic changes
RC-Arth and DRU-Arth provide a combination of findingsthat should be considered when deciding on the appropriatetreatment of a FCC tear Tey are summarized in the followingfour parameters22
Lacerated Components of the Triangular Fibrocartilage
Complex
Establishing the extent of FCC disruption is of utmost impor-tance Each component of the FCC that is distal (dc-FCC)and proximal (pc-FCC) may be involved either separately or
in associationTree types of ligamentous damage are possible
1 Distal tear (isolated tear of the distal component of the TFCC) When only the dc-FCC is lacerated the trampoline test re-sult is positive for loss of FCC resilience but the hook testresult is negative Integrity of the foveal attachments of thepc-FCC is confirmed by DRU-Arth
2 Complete tear (tear of both distal and proximal components of theTFCC) Complete peripheral FCC tear involves both com-ponents of the FCC A tear of the dc-FCC is visible duringRC-Arth and a pc-FCC avulsion is demonstrated by DRU- Arth Both trampoline and hook test results are positive
3 Proximal tear (isolated tear of the proximal component of theTFCC) An isolated avulsion of the pc-FCC from the foveaulnaris can be demonstrated by DRU-Arth which is manda-
tory to achieve the correct diagnosis Standard RC-Arth failsto show any abnormalities of the contour and capsular reflec-tion of the FCC even though both trampoline and hooktests show positive results
Surgical treatment varies according to which FCC componentis lacerated22 In case of a proximal or complete tear a FCC rein-sertion onto the fovea ulnaris is recommended However in case ofa distal tear arthroscopic suturing of the FCC to the dorsal ulno-carpal joint capsule and the ECU tendon subsheath is appropriate
TABLE 549830851
Palmer Classi1047297cation of TFCC Injuries
Class1 Traumatic Injuries
A Central per foration of the disk proper
B Peripheral avulsion from the ulna
Without styloid fractureWith styloid fracture
C Distal avulsion from the carpus
D Radial avulsionWithout sigmoid notch fractureWith sigmoid notch fracture
Class 2 Degenerative Injuries
A TFCC wear
B TFCC wear + lunate andor head chondromalacia
C TFCC perforation + lunate andor head chondromalacia
D TFCC perforation + lunate andor head chondromalacia +lunotriquetral ligament perforation
E TFCC per foration + ulnocarpal ar thritis
TFCC triangular 1047297brocartilage complex
Classi1047297cation from Palmer AK Triangular 1047297brocartilage complex lesions a classi1047297ca-tion J Hand Surg [Am] 198914594ndash606
FIGURE 54-1 Coronal slice of the ulnar wrist at the level ofthe fovea The triangular 1047297brocartilage complex
(TFCC) is outlined It is separated into the distal component of the TFCC (D) formed by the ulnar collateral ligament and the distal ham-mock structure and the proximal component (P) represented by theproximal triangular ligament which originates from the ulnar foveaand the styloid (From Atzei A New trends in arthroscopic manage-ment of type 1-B TFCC injuries with DRUJ instability J Hand Surg [Eur]2009 Epub ahead of print)
dc-TFCC
pc-TFCC
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 310
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
Reducibility of the Triangular Fibrocartilage Complex Tear With a small FCC tear as well as an avulsion type of rupturethe tearrsquos edges can be reapproximated or reduced easily and aFCC repair can be successfully performed By contrast in thepresence of a massive rupture of the FCC andor retraction ofthe ligamentous remnants reapproximation of the avulsed liga-ment or repair of the FCC tear to its anatomic position is notfeasible Terefore reconstruction with tendon graft should betaken into consideration
Healing Potential of the Triangular Fibrocartilage
Complex Tear
Chronic midsubstance ligamentous tears showing degeneratedor necrotic edges cannot be debrided back to a well-vascularizedarea therefore direct repair is unlikely to provide adequate heal-
ing Te same applies to the elongated and frayed ligament aftera failed suture direct repair is unlikely to be successful and aFCC reconstruction with tendon graft is recommended In ourexperience pc-FCC tears have a good healing potential for upto 3 months after injury (acute tears) whereas tears treated from 3to 6 months after injury (subacute tears) have unpredictable char-acteristics More chronic tears usually have a poor healing poten-tial Moreover congenital dysmorphisms of the styloid and fovealarea of the ulna (eg styloid hypoplasia and flattened ulnar head)represent other conditions that are associated with poor healingpotential after a repair and hence require reconstruction
Cartilage Status of the Distal Radioulnar Joint
Healthy cartilage status is of the utmost importance when plan-ning any reconstructive surgery for FCC disruption After high-energy trauma a cartilage defect over the ulnar head and sigmoid
notch may have been produced at the time of the initial injury Alternatively degenerative chondromalacia may be the conse-quence of the altered joint kinematics resulting in chronic DRUJinstability Well-preserved cartilage is a sine qua non for every typeof ligament repair or reconstruction of the DRUJ When DRU- Arth shows a chondral lesion some type of salvage arthroplasty isrecommended as an alternative
Based on the above-mentioned criteria a novel classification22 is defined that considers the variety of FCC peripheral tears and
provides guidelines for specific treatment modalities repair (sutureor foveal insertion) reconstruction with tendon graft or salvageprocedures (arthroplasty or joint replacement) (able 54-2)
INDICATIONS FOR FOVEAL REPAIR
When pain and impaired function show no improvement aftera trial of conservative treatment a foveal repair23 is indicated with type 1B FCC injuries of the Palmer classification Tis isrepresented as both class 2 and 3 tears (complete and isolatedproximal repairable FCC tears) in the authorsrsquo proposed clas-sification
CONTRAINDICATIONS
A foveal reattachment is not indicated for classes 1 4 and 5tears in the authorsrsquo classificationClass 1 (an isolated distal repairable tear) should be treated by
arthroscopic suturing of the FCC to the dorsal ulnocarpal jointcapsule and the ECU tendon subsheath Class 4 (nonrepairabletears owing to either a large tear size or poor quality of the tornligaments) should undergo ligament reconstruction by tendongraft as either an open24 or arthroscopic procedure2225
Chronic Essex-Lopresti injuries in which longitudinal stabil-ity of the forearm is altered as a result of the laceration of theinterosseous membrane are not amenable to simple FCCreattachment
Other absolute contraindications include previous soft tis-sue infection osteomyelitis and severe osteoporosis of the ulnarhead
Relative contraindications include a positive ulnar variance
with secondary ulnar impaction and carpal chondromalacia
SURGICAL TECHNIQUE
Operative Setup and Diagnostic Arthroscopy
Te patient is positioned supine with the affected arm on a handtable and a padded tourniquet on the proximal arm After a bra-chial plexus block has been administered the DRUJ laxity is
FIGURE 54-2 The hook test A In a left wrist the probe is inserted via the 6R portal through the triangular 1047297brocartilage complex (TFCC) tear Traction is applied to the ulnarmost border of the TFCC B The test result is considered positive when the TFCC (outlined by the dotted
line) can be pulled upward and radially as the pc-TFCC is interrupted or avulsed from the fovea (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopicfoveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 410
Part IX Ligament InstabilityTears562
TABLE 549830852
Arthroscopic Classi1047297cation of TFCC Peripheral Tears
ClinicalDRUJ In-stability
DistalCompo-nent
ProximalCompo-nent
TearReduc-ibility
HealingPoten-tial
DRUJCartilage Treatment
Class1
Repairabledistal tear D
P
None ndashslight
Torn Intact Easy Good Good RepairSuture(ligament-to-capsule)
Class2
Repairablecompletetear
DP
Mild ndashsevere
Torn Torn Easy Good Good RepairFoveal
re1047297xation
Class3
Repairableproximaltear
DP
Mild ndash severe
Intact Torn Easy Good Good RepairFoveal
re1047297xation
Class4-A
Non-repairablemassivetear
Non-reducible
D
P
Severe Torn Torn Impossible Good Good Reconstruction Tendon graft
Class4-B
Non-repairable
Failedsuture
Frayedligament
DP
Mild ndash severe
Torn Torn Impossible Poor Good Reconstruction Tendon graft
Class5
ArthriticDRUJ D
P
Mild ndashsevere
dagger dagger dagger dagger Poor SalvageArthroplasty
or jointreplacement
After debridement to bleeding edgesdagger Variable 1047297ndings that would not change treatment
Novel classi1047297cation22 based on arthroscopic 1047297ndings provides guidelines for treatment of diff erent triangular 1047297brocartilage complex (TFCC) peripheral tears The 1047297rst columnreports 1047297ndings of clinical instability of the distal radioulnar joint (DRUJ ) Classes 1ndash3 are repairable lesions that should be treated by either suture or foveal re1047297xation Classes4-A and 4-B are nonrepairable lesions that should undergo reconstruction by tendon graf t Class 5 includes diff erent conditions whose main characteristic consists of cartilagedegeneration of the DRUJ Such cases should be treated by salvage procedures that is arthroplasties or prosthetic joint replacement From Atzei A New trends in ar throscopicmanagement of type 1-B TFCC injuries with DRUJ instability J Hand Surg [Eur] 2009 Epub ahead of publishing
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 510
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
examined again before starting the arthroscopic procedure Com-plete forearm muscle relaxation following anesthesia may revealpreviously undetected DRUJ instability Te upper limb is exsan-guinated and the tourniquet is inflated to 250 mm Hg
A standard wrist arthroscopy setup is used26 Te wrist is sus-pended by finger traps using a wrist traction tower with approxi-
mately 10 to 15 pounds of traction depending on the size ofthe extremity Joint distention by saline infusion is usually notrequired to completely visualize the joint26 Te authorsrsquo pref-erence is to use a dry technique which facilitates arthroscopicrepair methods2728
A 27-mm arthroscope is used routinely but the 19-mm ar-throscope is used for smaller wrists Te wrist is systematicallyevaluated by RC-Arth with the scope in the 3-4 portal Care istaken to detect any associated disorders of the ulnar carpus
ears of the dc-FCC are visualized on the dorsoulnar portionof the articular disk and are frequently covered by hypertrophicsynovitis or fibrovascular granulation tissue which is removed with a small motorized shaver
A probe is inserted into the 6R portal to palpate the articulardisk and to assess the tension to the FCCmdashby the trampolinetest and the hook test
If the FCC is redundant and tests are positive for loss ofnormal resilience pc-FCC integrity and tautness are evaluatedthrough DRU-Arth
Te forearm is supinated the traction reduced and the DRUJexplored through the distal DRUJ portal In smaller wrists use ofa volar ulnar (VU) portal is recommended29 Scope insertion iseasier when the pc-FCC is torn since the articular disk is looseand more joint space is available DRU-Arth shows the ligamen-tous laceration or avulsion of the pc-FCC from the fovea Fora preliminary assessment of pc-FCC tautness an 18-gaugeneedle is inserted percutaneously about 1 cm proximal to the 6Uportal with the forearm held in full supination
When a FCC Palmer type 1B tear is associated with DRUJinstability the most common finding is the combination of a dc-FCC tear and a pc-FCC avulsion (complete FCC tear class 2)
Less frequently a pc-FCC tear is present as an isolated finding(proximal FCC tear class 3) In the latter case a standard RC- Arth reveals a normal FCC appearance which may lead to themisdiagnosis of a normal FCC since the pc-FCC tear can bedemonstrated only by DRU-Arth For this reason DRU-Arth isconsidered mandatory in cases of a suspected FCC tear that isassociated with DRUJ instability
Repair Technique
Repair of the foveal insertion of the FCC is performed by reat-tachment of the pc-FCC through a suture screw or anchor23
Te procedure begins with debridement of the foveal region as well as the torn edges of the FCC back to healthy tissue using asmall motorized shaver inserted through the 6R portal Althoughthe fovea can be debrided from the radiocarpal joint through theFCC tear it is recommended to establish a separate DRUJ por-
tal not only to remove the ligamentous remnants and refresh thebone at the fovea but also to drill and insert the suture screwanchor A dedicated working portal named the direct foveal (DF)portal has been devised to provide access to the fovea ulnaris2223
Te DF portal is located about 1 cm proximal to the 6U portaland is created with the forearm held in full supination Full fore-arm supination produces dorsal displacement of the ulnar styloidand the ECU tendon and uncovers the volar aspect of the distalulna on wristrsquos ulnar side (Fig 54-3) Tus the fovea and the
ulnarmost area of the distal ulna become subcutaneous and maybe reached through a very limited exposure Te DF portal is lesstechnically demanding compared with the formal VU portal29 but its use is limited to the introduction of working instrumentsin the area of the ulnar styloid and fovea (Fig 54-4)
After portal placement is checked under arthroscopic control
with an 18-gauge needle the longitudinal skin incision of the 6Uportal is extended proximally between the ECU and the flexorcarpi ulnaris (FCU) for a total length of 2 to 25 cm Troughthis mini-open approach the dorsal sensory branch of the ulnarnerve (DSBUN) and its transverse branches are identified andprotected by careful subcutaneous dissection Te risk of damag-ing the DSBUN is further reduced as the forearm is supinatedgiven that the DSBUN is displaced more volarly and along aslacker path than when the forearm is held in neutral position
Te extensor retinaculum is exposed and split along the courseof its fibers Te DRUJ capsule is incised longitudinally to reachthe distal articular surface of the ulnar head under the FCCTe fovea is located volarly at the base of the ulnar styloid justlateral to the capsule
With the scope in the distal DRUJ portal a small shaver orcuret can be inserted through the DF portal to refresh the torn
avulsed ligament to remove the inflammatory fibrovascular tissuefrom the fovea and to prepare it for suture screwanchor inser-tion Curettage of the fovea can also be performed as a mini-openprocedure
Screwanchor drilling and insertion are performed as a mini-open procedure as well (Fig 54-5) Te fovea is palpable as anarea of soft bone at the base of the ulnar styloid just lateral tothe capsule A power drill and intraoperative fluoroscopy are notrequired although the latter may be advisable for the less experi-enced surgeon
It is recommended to use a screwanchor that supports a pairof sutures so that a distinct suture can be passed through eachlimb of the radioulnar ligament Tis also improves the strengthof the repair by recreating a broader footprint of the pc-FCCanalogous to a rotator cuff repair in the shoulder30 Te authors
prefer to use a 28 or 32 titanium screw with two preloaded non-absorbable 2-0 Ultrabraid sutures (winfix Smith amp Nephew Andover MA) or a 35-mm absorbable screw preloaded withtwo 2-0 FiberWire sutures (Bio-Corkscrew Arthrex Naples FL)
Once the screw is in place sutures should exit the DF por-tal from underneath the FCC (Fig 54-6) Ten the wrist isplaced back in neutral pronosupination so that the screwrsquos head isbrought under the ulnarmost part of the FCC
Te suture ends are inserted into the tip of a 25-gauge needleor preferably a uohy needle to facilitate passage through theFCC
With the scope in the 3-4 portal the first suture is inserted inan outside-in fashion from the DF portal close to the FCCrsquospalmar contour to hold the palmar limb of the radioulnar liga-ment (Fig 54-7) A grasper is used to retrieve the suture from the6U portal (Fig 54-8) Te same procedure is repeated for sutur-
ing the dorsal limb of the radioulnar ligamentTe wrist traction is then released and the forearm is held in
neutral rotation Te surgical assistant maintains the ulnar head inreduced position Te sutures are tied under arthroscopic controlusing a small knot-pusher ensuring adequate pc-FCC compres-sion against the distal ulna (Fig 54-9) Knots should be located atthe prestyloid recess or just outside the DRUJ capsule (Fig 54-10)
RC-Arth is used as a control to ensure complete tear closureEven in the larger type 2 FCC peripheral tears it is seldom
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 610
Part IX Ligament InstabilityTears564
necessary to apply any further ligament-to-capsule sutures toclose off the dc-FCC
Te DRUJ is evaluated for complete range of pronosupinationand residual instability
Te DRUJ capsule and the opening between retinaculum fi-bers are approximated with two PDS 4-0 stitches Skin is closedby a subcuticular running suture
Postoperative Treatment
Te patient is placed in a long-arm splint in neutral forearm rota-tion for the first week which is substituted by a short Muumlnster
splint for another 2 weeksFull wrist flexionextension can be started as early as 3 weeks post-
operatively During the first week of rehabilitation progressive fore-arm rotation is allowed but the splint is still worn between exercises
During the following 6 weeks the patient is not permitted toperform any resistance movements Progressive resistance wrist-and hand-strengthening exercises are begun after the sixth weekuntil the patient is able to bear weight on the operated wrist Sportand heavy work activities are started 3 months postoperatively
COMPLICATIONS
Few complications should be encountered during arthroscopic-assisted palmar repair of the foveal insertion of the FCC providedthat there is careful application of standard arthroscopic principlesand of the described surgical technique Te most serious complica-tion is potential injury to the DSBUN which is related to surgicalexperience It can be prevented by careful dissection techniques anda sound understanding of the underlying anatomy and its variationfollowing forearm rotation ransitory neuropraxia of the DSBUNmay be observed which recovers spontaneously in 3 to 4 months
Te surgical scar of the ulnar side of the wrist may adhere to deeperstructures and become painful during the first stages of physicaltherapy especially after a prolonged period of wrist immobilization
As in other arthroscopic procedures infection remains a risk which is usually prevented by a prophylactic dose of parenteralantibiotics before initiating the procedure
Te dry technique of joint exploration27 is recommended toreduce soft tissue infiltration and swelling by the continuous leak-ing of saline through the portals
FIGURE 54-3 Full forearm supination is required to create the direct foveal (DF) portal After supination the ulnar styloid and the extensorcarpi ulnaris tendon displace dorsally and the fovea and the ulnarmost area of the distal ulna become subcutaneous (From
Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
Fovea
Neutral PS Supination
DF
portal
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 710
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-5 Screwanchor drilling and insertion are performed as a mini-open procedure through the direct foveal portal (From Atzei ARizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar
joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
FIGURE 54-4 The direct foveal (DF) portal is located about 1 cm proximal to the 6U portal It has been devised as a working portal toprovide access to the area of the ulnar styloid and fovea With the scope in the distal radioulnar joint portal a curet
or small shaver is inserted through the DF portal to refresh the tornavulsed ligament and the fovea (From Atzei A Rizzo A Luchetti R Fairplay TArthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up ExtremSurg 200812226ndash235)
6-U
DF
A B
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 810
Part IX Ligament InstabilityTears566
FIGURE 54-6 Once the screw is in place sutures should exit the direct foveal portal from underneath the triangular 1047297brocartilage complex(TFCC) When the wrist is placed back in neutral pronosupination the screwrsquos head is brought under the TFCC (From Atzei A
Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability TechHand Up Extrem Surg 200812226ndash235)
Te technique of arthroscopic-assisted palmar repair of the fo-veal insertion of the FCC has a learning curve However once
the technique is mastered the rate of complications for this pro-cedure is comparable to that of larger series of common wristarthroscopic procedures31
RESULTS
Te authorsrsquo clinical experience started in 2001 and up until now we have operated on 37 FCC tears (29 type 2 FCC peripheraltears and 8 type 3 tears)
In a control series study 18 patients (13 males and5 females with a mean age of 342) were investigated prospec-
tively for a minimum follow-up of 1 year (average 18 monthsmaximum 37 months) All patients had a history of traumacomplained of pain in the ulnar fovea and had clinical signsof DRUJ instability ranging from mild (10 patients) to mod-erate (8 patients) Although radiographs showed a positive ul-nar variance in three patients there were no detectable signsof ulnocarpal impaction or carpal degenerative chondropa-thy Arthroscopy revealed a Palmer type 1B ulnar avulsionof the FCC in all patients Fourteen cases were classified as
FIGURE 54-7 With the scope in the 3-4 portal the 1047297rst suture end is inserted into the tip of a 25-gauge needle (preferably a Tuohy needle) The needle is passed through the triangular 1047297brocartilage complex (TFCC) in an outside-in fashion via the direct foveal portal
toward the palmar contour of the TFCC (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complexperipheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 910
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-8 A grasper is inserted through the 6U portal and used to retrieve the suture (From Atzei A Rizzo A Luchetti R Fairplay T Arthro-scopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up
Extrem Surg 200812226ndash235)
FIGURE 54-9 The suture is tied under arthroscopic control using a small knot-pusher The pc-TFCC (proximal component of the triangular1047297brocartilage complex) is pushed forcefully against the distal ulna provided that the wrist traction is released the forearm is
held in neutral rotation and the ulnar head is reduced by the assistant (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
complete FCC peripheral tears (type 2) and four as proximaltears (type 3)
At fol low-up evaluation the patients showed an increasedrange of motion (from 907 to 96 of the contralateralside) and grip strength (from 73 to 90) Pain decreasedfrom 83 to 12 on a 10-point visual analogue scale Gripstrength and pain changes reached statistical significance
(P lt 005) he Modified Mayo Wrist Score was excellentin 14 patients good in 3 and fair in 1 A total of 944 ofthe results scored excellent and good DASH (disabilities ofthe arm shoulder and hand) score averaged 105 Fifteenpatients (833) resumed previous work and recreation-al activities and 3 patients (167) returned to restrictedemployment
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 1010
Part IX Ligament InstabilityTears568
REFERENCES
1 Palmer AK riangular fibrocartilage complex lesions a classification J HandSurg [Am] 198914594ndash606
2 Nakamura Yabe Y Horiuchi Y Functional anatomy of the triangularfibrocartilage complex J Hand Surg [Br] 199621581ndash586
3 Palmer AK Werner F W Te triangular fibrocartilage complex of the wristmdashanatomy and function J Hand Surg [Am] 19816153ndash162
4 Adams BD Holly K A Strains in the articular disk of the triangular fibro-cartilage complex a biomechanical study J Hand Surg [Am] 199318919ndash925
5 Benjamin M Evans E J Pemberton D J Histological studies on the triangularfibrocartilage complex of the wrist J Anat 199017259ndash67
6 Kauer JMG Te distal radioulnar joint anatomic and functional consider-ations Clin Orthop 199227537ndash45
7 Atzei A Luchetti R Garcia-Elias M Lesioni capsulo-legamentose dellaradio-ulnare distale e fibrocartilagine triangolare In Landi A Catalano FLuchetti R (eds) rattato di Chirurgia della Mano Verduci Editore Roma2006 pp 159ndash187
8 Kleinman WB Stability of the distal radioulnar joint biomechanics patho-physiology physical diagnosis and restoration of function What we havelearned in 25 years J Hand Surg [Am] 2007321087ndash1106
9 Garcia-Elias M Smith DE Llusa M Surgical approach to the triangularfibrocartilage complex ech Hand Up Extrem Surg 20037(4)134ndash140
10 Nakamura Nakao Y Ikegami H et al Open repair of the ulnar disruptionof the triangular fibrocartilage complex with double three-dimensional mat-tress suturing technique ech Hand Up Extrem Surg 20048(2)116ndash123
11 Hermansdorfer JD Kleinman WB Management of chronic peripheraltears of the triangular fibrocartilage complex J Hand Surg [Am] 199116340ndash346
12 Chou KH Sarris IK Sotereanos DG Suture anchor repair of ulnar-sidedtriangular fibrocartilage complex tears J Hand Surg [Br] 200328546ndash550
13 Slutsky D J Clinical applications of volar portals in wrist arthroscopy echHand Up Extrem Surg 20048(4)229ndash238
14 omaino M Weiser R Combined arthroscopic FCC debridement and wa-fer resection of the distal ulna in wrists with triangular fibrocartilage complextears and positive ulnar variance J Hand Surg [Am] 2001261047ndash1052
15 Hanker G J Management of ulnar impaction syndrome In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 63ndash71
16 Moskal M J Savoie FH III Management of lunotriquetral instability InGeissler WB (ed) Wrist Arthroscopy New York Springer-Verlag 2005pp 94ndash101
17 Atzei A Luchetti R Clinical approach to the painful wrist In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 185ndash195
18 ay SC omita K Berger R A Te ldquoulnar fovea signrdquo for defining ulnar wrist pain an analysis of sensitivity and specificity J Hand Surg [Am]200732(4)438ndash444
19 Zanetti M Bram J Hodler J riangular fibrocartilage and intercarpal liga-ments of the wrist does MR arthrography improve standard MRI J Magn
Reson Imaging 19977 (3)590ndash59420 Pederzini L Luchetti R Soragni O et al Evaluation of the triangular
fibrocartilage complex tears by arthroscopy arthrography and magnetic reso-nance imaging Arthroscopy 19928191ndash197
21 Fulcher S Poehling G Te role of operative arthroscopy for the diag-nosis and treatment of lesions about the distal ulna Hand Clin 199814285ndash296
22 Atzei A New trends in arthroscopic management of type 1-B FCC injuries with DRUJ instability J Hand Surg [Eur] 2009Epub ahead of print
23 Atzei A Rizzo A Luchetti R Fairplay Arthroscopic foveal repair of tri-angular fibrocartilage complex peripheral lesion with distal radioulnar jointinstability ech Hand Up Extrem Surg 200812226ndash235
24 Adams BD Anatomic reconstruction of the distal radioulnar ligaments forDRUJ instability ech Hand Up Extrem Surg 20004154ndash160
25 Atzei A Luchetti R Borelli PP et al Arthroscopic FCC reconstruction bytendon graft Riv Chir Mano 200643(3)370ndash376
26 Atzei A Luchetti R Sgarbossa A et al Set-up portals and normal explora-tion in wrist arthroscopy Chir Main 200625S131ndashS144
27 del Pintildeal F Garciacutea-Bernal F J Pisani D et al Dry arthroscopy of the wrist
surgical technique J Hand Surg [Am] 200732119ndash12328 del Pintildeal F Garciacutea-Bernal F J Delgado J et al Correction of malunited
intra-articular distal radius fractures with an inside-out osteotomy technique J Hand Surg [Am] 200531(6)1029ndash1034
29 Slutsky D J Distal radioulnar joint arthroscopy and the volar ulnar portalech Hand Up Extrem Surg 200711(1)38ndash44
30 Lo IK Y Burkhart SS Double-row arthroscopic rotator cuff repair re-establishing the footprint of the rotator cuff Arthroscopy 200319(9)1035ndash1042
31 Luchetti R Atzei A Rocchi L Incidence and causes of failures in wristarthroscopic techniques Chir Main 200625(1)48ndash53
FIGURE 54-10 At the end of the procedure the knots of bothsutures are located at the level of the 6U portal just
outside the distal radioulnar joint capsule or in the prestyloid recess(From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)

8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 310
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
Reducibility of the Triangular Fibrocartilage Complex Tear With a small FCC tear as well as an avulsion type of rupturethe tearrsquos edges can be reapproximated or reduced easily and aFCC repair can be successfully performed By contrast in thepresence of a massive rupture of the FCC andor retraction ofthe ligamentous remnants reapproximation of the avulsed liga-ment or repair of the FCC tear to its anatomic position is notfeasible Terefore reconstruction with tendon graft should betaken into consideration
Healing Potential of the Triangular Fibrocartilage
Complex Tear
Chronic midsubstance ligamentous tears showing degeneratedor necrotic edges cannot be debrided back to a well-vascularizedarea therefore direct repair is unlikely to provide adequate heal-
ing Te same applies to the elongated and frayed ligament aftera failed suture direct repair is unlikely to be successful and aFCC reconstruction with tendon graft is recommended In ourexperience pc-FCC tears have a good healing potential for upto 3 months after injury (acute tears) whereas tears treated from 3to 6 months after injury (subacute tears) have unpredictable char-acteristics More chronic tears usually have a poor healing poten-tial Moreover congenital dysmorphisms of the styloid and fovealarea of the ulna (eg styloid hypoplasia and flattened ulnar head)represent other conditions that are associated with poor healingpotential after a repair and hence require reconstruction
Cartilage Status of the Distal Radioulnar Joint
Healthy cartilage status is of the utmost importance when plan-ning any reconstructive surgery for FCC disruption After high-energy trauma a cartilage defect over the ulnar head and sigmoid
notch may have been produced at the time of the initial injury Alternatively degenerative chondromalacia may be the conse-quence of the altered joint kinematics resulting in chronic DRUJinstability Well-preserved cartilage is a sine qua non for every typeof ligament repair or reconstruction of the DRUJ When DRU- Arth shows a chondral lesion some type of salvage arthroplasty isrecommended as an alternative
Based on the above-mentioned criteria a novel classification22 is defined that considers the variety of FCC peripheral tears and
provides guidelines for specific treatment modalities repair (sutureor foveal insertion) reconstruction with tendon graft or salvageprocedures (arthroplasty or joint replacement) (able 54-2)
INDICATIONS FOR FOVEAL REPAIR
When pain and impaired function show no improvement aftera trial of conservative treatment a foveal repair23 is indicated with type 1B FCC injuries of the Palmer classification Tis isrepresented as both class 2 and 3 tears (complete and isolatedproximal repairable FCC tears) in the authorsrsquo proposed clas-sification
CONTRAINDICATIONS
A foveal reattachment is not indicated for classes 1 4 and 5tears in the authorsrsquo classificationClass 1 (an isolated distal repairable tear) should be treated by
arthroscopic suturing of the FCC to the dorsal ulnocarpal jointcapsule and the ECU tendon subsheath Class 4 (nonrepairabletears owing to either a large tear size or poor quality of the tornligaments) should undergo ligament reconstruction by tendongraft as either an open24 or arthroscopic procedure2225
Chronic Essex-Lopresti injuries in which longitudinal stabil-ity of the forearm is altered as a result of the laceration of theinterosseous membrane are not amenable to simple FCCreattachment
Other absolute contraindications include previous soft tis-sue infection osteomyelitis and severe osteoporosis of the ulnarhead
Relative contraindications include a positive ulnar variance
with secondary ulnar impaction and carpal chondromalacia
SURGICAL TECHNIQUE
Operative Setup and Diagnostic Arthroscopy
Te patient is positioned supine with the affected arm on a handtable and a padded tourniquet on the proximal arm After a bra-chial plexus block has been administered the DRUJ laxity is
FIGURE 54-2 The hook test A In a left wrist the probe is inserted via the 6R portal through the triangular 1047297brocartilage complex (TFCC) tear Traction is applied to the ulnarmost border of the TFCC B The test result is considered positive when the TFCC (outlined by the dotted
line) can be pulled upward and radially as the pc-TFCC is interrupted or avulsed from the fovea (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopicfoveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 410
Part IX Ligament InstabilityTears562
TABLE 549830852
Arthroscopic Classi1047297cation of TFCC Peripheral Tears
ClinicalDRUJ In-stability
DistalCompo-nent
ProximalCompo-nent
TearReduc-ibility
HealingPoten-tial
DRUJCartilage Treatment
Class1
Repairabledistal tear D
P
None ndashslight
Torn Intact Easy Good Good RepairSuture(ligament-to-capsule)
Class2
Repairablecompletetear
DP
Mild ndashsevere
Torn Torn Easy Good Good RepairFoveal
re1047297xation
Class3
Repairableproximaltear
DP
Mild ndash severe
Intact Torn Easy Good Good RepairFoveal
re1047297xation
Class4-A
Non-repairablemassivetear
Non-reducible
D
P
Severe Torn Torn Impossible Good Good Reconstruction Tendon graft
Class4-B
Non-repairable
Failedsuture
Frayedligament
DP
Mild ndash severe
Torn Torn Impossible Poor Good Reconstruction Tendon graft
Class5
ArthriticDRUJ D
P
Mild ndashsevere
dagger dagger dagger dagger Poor SalvageArthroplasty
or jointreplacement
After debridement to bleeding edgesdagger Variable 1047297ndings that would not change treatment
Novel classi1047297cation22 based on arthroscopic 1047297ndings provides guidelines for treatment of diff erent triangular 1047297brocartilage complex (TFCC) peripheral tears The 1047297rst columnreports 1047297ndings of clinical instability of the distal radioulnar joint (DRUJ ) Classes 1ndash3 are repairable lesions that should be treated by either suture or foveal re1047297xation Classes4-A and 4-B are nonrepairable lesions that should undergo reconstruction by tendon graf t Class 5 includes diff erent conditions whose main characteristic consists of cartilagedegeneration of the DRUJ Such cases should be treated by salvage procedures that is arthroplasties or prosthetic joint replacement From Atzei A New trends in ar throscopicmanagement of type 1-B TFCC injuries with DRUJ instability J Hand Surg [Eur] 2009 Epub ahead of publishing
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 510
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
examined again before starting the arthroscopic procedure Com-plete forearm muscle relaxation following anesthesia may revealpreviously undetected DRUJ instability Te upper limb is exsan-guinated and the tourniquet is inflated to 250 mm Hg
A standard wrist arthroscopy setup is used26 Te wrist is sus-pended by finger traps using a wrist traction tower with approxi-
mately 10 to 15 pounds of traction depending on the size ofthe extremity Joint distention by saline infusion is usually notrequired to completely visualize the joint26 Te authorsrsquo pref-erence is to use a dry technique which facilitates arthroscopicrepair methods2728
A 27-mm arthroscope is used routinely but the 19-mm ar-throscope is used for smaller wrists Te wrist is systematicallyevaluated by RC-Arth with the scope in the 3-4 portal Care istaken to detect any associated disorders of the ulnar carpus
ears of the dc-FCC are visualized on the dorsoulnar portionof the articular disk and are frequently covered by hypertrophicsynovitis or fibrovascular granulation tissue which is removed with a small motorized shaver
A probe is inserted into the 6R portal to palpate the articulardisk and to assess the tension to the FCCmdashby the trampolinetest and the hook test
If the FCC is redundant and tests are positive for loss ofnormal resilience pc-FCC integrity and tautness are evaluatedthrough DRU-Arth
Te forearm is supinated the traction reduced and the DRUJexplored through the distal DRUJ portal In smaller wrists use ofa volar ulnar (VU) portal is recommended29 Scope insertion iseasier when the pc-FCC is torn since the articular disk is looseand more joint space is available DRU-Arth shows the ligamen-tous laceration or avulsion of the pc-FCC from the fovea Fora preliminary assessment of pc-FCC tautness an 18-gaugeneedle is inserted percutaneously about 1 cm proximal to the 6Uportal with the forearm held in full supination
When a FCC Palmer type 1B tear is associated with DRUJinstability the most common finding is the combination of a dc-FCC tear and a pc-FCC avulsion (complete FCC tear class 2)
Less frequently a pc-FCC tear is present as an isolated finding(proximal FCC tear class 3) In the latter case a standard RC- Arth reveals a normal FCC appearance which may lead to themisdiagnosis of a normal FCC since the pc-FCC tear can bedemonstrated only by DRU-Arth For this reason DRU-Arth isconsidered mandatory in cases of a suspected FCC tear that isassociated with DRUJ instability
Repair Technique
Repair of the foveal insertion of the FCC is performed by reat-tachment of the pc-FCC through a suture screw or anchor23
Te procedure begins with debridement of the foveal region as well as the torn edges of the FCC back to healthy tissue using asmall motorized shaver inserted through the 6R portal Althoughthe fovea can be debrided from the radiocarpal joint through theFCC tear it is recommended to establish a separate DRUJ por-
tal not only to remove the ligamentous remnants and refresh thebone at the fovea but also to drill and insert the suture screwanchor A dedicated working portal named the direct foveal (DF)portal has been devised to provide access to the fovea ulnaris2223
Te DF portal is located about 1 cm proximal to the 6U portaland is created with the forearm held in full supination Full fore-arm supination produces dorsal displacement of the ulnar styloidand the ECU tendon and uncovers the volar aspect of the distalulna on wristrsquos ulnar side (Fig 54-3) Tus the fovea and the
ulnarmost area of the distal ulna become subcutaneous and maybe reached through a very limited exposure Te DF portal is lesstechnically demanding compared with the formal VU portal29 but its use is limited to the introduction of working instrumentsin the area of the ulnar styloid and fovea (Fig 54-4)
After portal placement is checked under arthroscopic control
with an 18-gauge needle the longitudinal skin incision of the 6Uportal is extended proximally between the ECU and the flexorcarpi ulnaris (FCU) for a total length of 2 to 25 cm Troughthis mini-open approach the dorsal sensory branch of the ulnarnerve (DSBUN) and its transverse branches are identified andprotected by careful subcutaneous dissection Te risk of damag-ing the DSBUN is further reduced as the forearm is supinatedgiven that the DSBUN is displaced more volarly and along aslacker path than when the forearm is held in neutral position
Te extensor retinaculum is exposed and split along the courseof its fibers Te DRUJ capsule is incised longitudinally to reachthe distal articular surface of the ulnar head under the FCCTe fovea is located volarly at the base of the ulnar styloid justlateral to the capsule
With the scope in the distal DRUJ portal a small shaver orcuret can be inserted through the DF portal to refresh the torn
avulsed ligament to remove the inflammatory fibrovascular tissuefrom the fovea and to prepare it for suture screwanchor inser-tion Curettage of the fovea can also be performed as a mini-openprocedure
Screwanchor drilling and insertion are performed as a mini-open procedure as well (Fig 54-5) Te fovea is palpable as anarea of soft bone at the base of the ulnar styloid just lateral tothe capsule A power drill and intraoperative fluoroscopy are notrequired although the latter may be advisable for the less experi-enced surgeon
It is recommended to use a screwanchor that supports a pairof sutures so that a distinct suture can be passed through eachlimb of the radioulnar ligament Tis also improves the strengthof the repair by recreating a broader footprint of the pc-FCCanalogous to a rotator cuff repair in the shoulder30 Te authors
prefer to use a 28 or 32 titanium screw with two preloaded non-absorbable 2-0 Ultrabraid sutures (winfix Smith amp Nephew Andover MA) or a 35-mm absorbable screw preloaded withtwo 2-0 FiberWire sutures (Bio-Corkscrew Arthrex Naples FL)
Once the screw is in place sutures should exit the DF por-tal from underneath the FCC (Fig 54-6) Ten the wrist isplaced back in neutral pronosupination so that the screwrsquos head isbrought under the ulnarmost part of the FCC
Te suture ends are inserted into the tip of a 25-gauge needleor preferably a uohy needle to facilitate passage through theFCC
With the scope in the 3-4 portal the first suture is inserted inan outside-in fashion from the DF portal close to the FCCrsquospalmar contour to hold the palmar limb of the radioulnar liga-ment (Fig 54-7) A grasper is used to retrieve the suture from the6U portal (Fig 54-8) Te same procedure is repeated for sutur-
ing the dorsal limb of the radioulnar ligamentTe wrist traction is then released and the forearm is held in
neutral rotation Te surgical assistant maintains the ulnar head inreduced position Te sutures are tied under arthroscopic controlusing a small knot-pusher ensuring adequate pc-FCC compres-sion against the distal ulna (Fig 54-9) Knots should be located atthe prestyloid recess or just outside the DRUJ capsule (Fig 54-10)
RC-Arth is used as a control to ensure complete tear closureEven in the larger type 2 FCC peripheral tears it is seldom
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 610
Part IX Ligament InstabilityTears564
necessary to apply any further ligament-to-capsule sutures toclose off the dc-FCC
Te DRUJ is evaluated for complete range of pronosupinationand residual instability
Te DRUJ capsule and the opening between retinaculum fi-bers are approximated with two PDS 4-0 stitches Skin is closedby a subcuticular running suture
Postoperative Treatment
Te patient is placed in a long-arm splint in neutral forearm rota-tion for the first week which is substituted by a short Muumlnster
splint for another 2 weeksFull wrist flexionextension can be started as early as 3 weeks post-
operatively During the first week of rehabilitation progressive fore-arm rotation is allowed but the splint is still worn between exercises
During the following 6 weeks the patient is not permitted toperform any resistance movements Progressive resistance wrist-and hand-strengthening exercises are begun after the sixth weekuntil the patient is able to bear weight on the operated wrist Sportand heavy work activities are started 3 months postoperatively
COMPLICATIONS
Few complications should be encountered during arthroscopic-assisted palmar repair of the foveal insertion of the FCC providedthat there is careful application of standard arthroscopic principlesand of the described surgical technique Te most serious complica-tion is potential injury to the DSBUN which is related to surgicalexperience It can be prevented by careful dissection techniques anda sound understanding of the underlying anatomy and its variationfollowing forearm rotation ransitory neuropraxia of the DSBUNmay be observed which recovers spontaneously in 3 to 4 months
Te surgical scar of the ulnar side of the wrist may adhere to deeperstructures and become painful during the first stages of physicaltherapy especially after a prolonged period of wrist immobilization
As in other arthroscopic procedures infection remains a risk which is usually prevented by a prophylactic dose of parenteralantibiotics before initiating the procedure
Te dry technique of joint exploration27 is recommended toreduce soft tissue infiltration and swelling by the continuous leak-ing of saline through the portals
FIGURE 54-3 Full forearm supination is required to create the direct foveal (DF) portal After supination the ulnar styloid and the extensorcarpi ulnaris tendon displace dorsally and the fovea and the ulnarmost area of the distal ulna become subcutaneous (From
Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
Fovea
Neutral PS Supination
DF
portal
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 710
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-5 Screwanchor drilling and insertion are performed as a mini-open procedure through the direct foveal portal (From Atzei ARizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar
joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
FIGURE 54-4 The direct foveal (DF) portal is located about 1 cm proximal to the 6U portal It has been devised as a working portal toprovide access to the area of the ulnar styloid and fovea With the scope in the distal radioulnar joint portal a curet
or small shaver is inserted through the DF portal to refresh the tornavulsed ligament and the fovea (From Atzei A Rizzo A Luchetti R Fairplay TArthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up ExtremSurg 200812226ndash235)
6-U
DF
A B
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 810
Part IX Ligament InstabilityTears566
FIGURE 54-6 Once the screw is in place sutures should exit the direct foveal portal from underneath the triangular 1047297brocartilage complex(TFCC) When the wrist is placed back in neutral pronosupination the screwrsquos head is brought under the TFCC (From Atzei A
Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability TechHand Up Extrem Surg 200812226ndash235)
Te technique of arthroscopic-assisted palmar repair of the fo-veal insertion of the FCC has a learning curve However once
the technique is mastered the rate of complications for this pro-cedure is comparable to that of larger series of common wristarthroscopic procedures31
RESULTS
Te authorsrsquo clinical experience started in 2001 and up until now we have operated on 37 FCC tears (29 type 2 FCC peripheraltears and 8 type 3 tears)
In a control series study 18 patients (13 males and5 females with a mean age of 342) were investigated prospec-
tively for a minimum follow-up of 1 year (average 18 monthsmaximum 37 months) All patients had a history of traumacomplained of pain in the ulnar fovea and had clinical signsof DRUJ instability ranging from mild (10 patients) to mod-erate (8 patients) Although radiographs showed a positive ul-nar variance in three patients there were no detectable signsof ulnocarpal impaction or carpal degenerative chondropa-thy Arthroscopy revealed a Palmer type 1B ulnar avulsionof the FCC in all patients Fourteen cases were classified as
FIGURE 54-7 With the scope in the 3-4 portal the 1047297rst suture end is inserted into the tip of a 25-gauge needle (preferably a Tuohy needle) The needle is passed through the triangular 1047297brocartilage complex (TFCC) in an outside-in fashion via the direct foveal portal
toward the palmar contour of the TFCC (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complexperipheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 910
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-8 A grasper is inserted through the 6U portal and used to retrieve the suture (From Atzei A Rizzo A Luchetti R Fairplay T Arthro-scopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up
Extrem Surg 200812226ndash235)
FIGURE 54-9 The suture is tied under arthroscopic control using a small knot-pusher The pc-TFCC (proximal component of the triangular1047297brocartilage complex) is pushed forcefully against the distal ulna provided that the wrist traction is released the forearm is
held in neutral rotation and the ulnar head is reduced by the assistant (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
complete FCC peripheral tears (type 2) and four as proximaltears (type 3)
At fol low-up evaluation the patients showed an increasedrange of motion (from 907 to 96 of the contralateralside) and grip strength (from 73 to 90) Pain decreasedfrom 83 to 12 on a 10-point visual analogue scale Gripstrength and pain changes reached statistical significance
(P lt 005) he Modified Mayo Wrist Score was excellentin 14 patients good in 3 and fair in 1 A total of 944 ofthe results scored excellent and good DASH (disabilities ofthe arm shoulder and hand) score averaged 105 Fifteenpatients (833) resumed previous work and recreation-al activities and 3 patients (167) returned to restrictedemployment
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 1010
Part IX Ligament InstabilityTears568
REFERENCES
1 Palmer AK riangular fibrocartilage complex lesions a classification J HandSurg [Am] 198914594ndash606
2 Nakamura Yabe Y Horiuchi Y Functional anatomy of the triangularfibrocartilage complex J Hand Surg [Br] 199621581ndash586
3 Palmer AK Werner F W Te triangular fibrocartilage complex of the wristmdashanatomy and function J Hand Surg [Am] 19816153ndash162
4 Adams BD Holly K A Strains in the articular disk of the triangular fibro-cartilage complex a biomechanical study J Hand Surg [Am] 199318919ndash925
5 Benjamin M Evans E J Pemberton D J Histological studies on the triangularfibrocartilage complex of the wrist J Anat 199017259ndash67
6 Kauer JMG Te distal radioulnar joint anatomic and functional consider-ations Clin Orthop 199227537ndash45
7 Atzei A Luchetti R Garcia-Elias M Lesioni capsulo-legamentose dellaradio-ulnare distale e fibrocartilagine triangolare In Landi A Catalano FLuchetti R (eds) rattato di Chirurgia della Mano Verduci Editore Roma2006 pp 159ndash187
8 Kleinman WB Stability of the distal radioulnar joint biomechanics patho-physiology physical diagnosis and restoration of function What we havelearned in 25 years J Hand Surg [Am] 2007321087ndash1106
9 Garcia-Elias M Smith DE Llusa M Surgical approach to the triangularfibrocartilage complex ech Hand Up Extrem Surg 20037(4)134ndash140
10 Nakamura Nakao Y Ikegami H et al Open repair of the ulnar disruptionof the triangular fibrocartilage complex with double three-dimensional mat-tress suturing technique ech Hand Up Extrem Surg 20048(2)116ndash123
11 Hermansdorfer JD Kleinman WB Management of chronic peripheraltears of the triangular fibrocartilage complex J Hand Surg [Am] 199116340ndash346
12 Chou KH Sarris IK Sotereanos DG Suture anchor repair of ulnar-sidedtriangular fibrocartilage complex tears J Hand Surg [Br] 200328546ndash550
13 Slutsky D J Clinical applications of volar portals in wrist arthroscopy echHand Up Extrem Surg 20048(4)229ndash238
14 omaino M Weiser R Combined arthroscopic FCC debridement and wa-fer resection of the distal ulna in wrists with triangular fibrocartilage complextears and positive ulnar variance J Hand Surg [Am] 2001261047ndash1052
15 Hanker G J Management of ulnar impaction syndrome In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 63ndash71
16 Moskal M J Savoie FH III Management of lunotriquetral instability InGeissler WB (ed) Wrist Arthroscopy New York Springer-Verlag 2005pp 94ndash101
17 Atzei A Luchetti R Clinical approach to the painful wrist In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 185ndash195
18 ay SC omita K Berger R A Te ldquoulnar fovea signrdquo for defining ulnar wrist pain an analysis of sensitivity and specificity J Hand Surg [Am]200732(4)438ndash444
19 Zanetti M Bram J Hodler J riangular fibrocartilage and intercarpal liga-ments of the wrist does MR arthrography improve standard MRI J Magn
Reson Imaging 19977 (3)590ndash59420 Pederzini L Luchetti R Soragni O et al Evaluation of the triangular
fibrocartilage complex tears by arthroscopy arthrography and magnetic reso-nance imaging Arthroscopy 19928191ndash197
21 Fulcher S Poehling G Te role of operative arthroscopy for the diag-nosis and treatment of lesions about the distal ulna Hand Clin 199814285ndash296
22 Atzei A New trends in arthroscopic management of type 1-B FCC injuries with DRUJ instability J Hand Surg [Eur] 2009Epub ahead of print
23 Atzei A Rizzo A Luchetti R Fairplay Arthroscopic foveal repair of tri-angular fibrocartilage complex peripheral lesion with distal radioulnar jointinstability ech Hand Up Extrem Surg 200812226ndash235
24 Adams BD Anatomic reconstruction of the distal radioulnar ligaments forDRUJ instability ech Hand Up Extrem Surg 20004154ndash160
25 Atzei A Luchetti R Borelli PP et al Arthroscopic FCC reconstruction bytendon graft Riv Chir Mano 200643(3)370ndash376
26 Atzei A Luchetti R Sgarbossa A et al Set-up portals and normal explora-tion in wrist arthroscopy Chir Main 200625S131ndashS144
27 del Pintildeal F Garciacutea-Bernal F J Pisani D et al Dry arthroscopy of the wrist
surgical technique J Hand Surg [Am] 200732119ndash12328 del Pintildeal F Garciacutea-Bernal F J Delgado J et al Correction of malunited
intra-articular distal radius fractures with an inside-out osteotomy technique J Hand Surg [Am] 200531(6)1029ndash1034
29 Slutsky D J Distal radioulnar joint arthroscopy and the volar ulnar portalech Hand Up Extrem Surg 200711(1)38ndash44
30 Lo IK Y Burkhart SS Double-row arthroscopic rotator cuff repair re-establishing the footprint of the rotator cuff Arthroscopy 200319(9)1035ndash1042
31 Luchetti R Atzei A Rocchi L Incidence and causes of failures in wristarthroscopic techniques Chir Main 200625(1)48ndash53
FIGURE 54-10 At the end of the procedure the knots of bothsutures are located at the level of the 6U portal just
outside the distal radioulnar joint capsule or in the prestyloid recess(From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)

8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 410
Part IX Ligament InstabilityTears562
TABLE 549830852
Arthroscopic Classi1047297cation of TFCC Peripheral Tears
ClinicalDRUJ In-stability
DistalCompo-nent
ProximalCompo-nent
TearReduc-ibility
HealingPoten-tial
DRUJCartilage Treatment
Class1
Repairabledistal tear D
P
None ndashslight
Torn Intact Easy Good Good RepairSuture(ligament-to-capsule)
Class2
Repairablecompletetear
DP
Mild ndashsevere
Torn Torn Easy Good Good RepairFoveal
re1047297xation
Class3
Repairableproximaltear
DP
Mild ndash severe
Intact Torn Easy Good Good RepairFoveal
re1047297xation
Class4-A
Non-repairablemassivetear
Non-reducible
D
P
Severe Torn Torn Impossible Good Good Reconstruction Tendon graft
Class4-B
Non-repairable
Failedsuture
Frayedligament
DP
Mild ndash severe
Torn Torn Impossible Poor Good Reconstruction Tendon graft
Class5
ArthriticDRUJ D
P
Mild ndashsevere
dagger dagger dagger dagger Poor SalvageArthroplasty
or jointreplacement
After debridement to bleeding edgesdagger Variable 1047297ndings that would not change treatment
Novel classi1047297cation22 based on arthroscopic 1047297ndings provides guidelines for treatment of diff erent triangular 1047297brocartilage complex (TFCC) peripheral tears The 1047297rst columnreports 1047297ndings of clinical instability of the distal radioulnar joint (DRUJ ) Classes 1ndash3 are repairable lesions that should be treated by either suture or foveal re1047297xation Classes4-A and 4-B are nonrepairable lesions that should undergo reconstruction by tendon graf t Class 5 includes diff erent conditions whose main characteristic consists of cartilagedegeneration of the DRUJ Such cases should be treated by salvage procedures that is arthroplasties or prosthetic joint replacement From Atzei A New trends in ar throscopicmanagement of type 1-B TFCC injuries with DRUJ instability J Hand Surg [Eur] 2009 Epub ahead of publishing
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 510
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
examined again before starting the arthroscopic procedure Com-plete forearm muscle relaxation following anesthesia may revealpreviously undetected DRUJ instability Te upper limb is exsan-guinated and the tourniquet is inflated to 250 mm Hg
A standard wrist arthroscopy setup is used26 Te wrist is sus-pended by finger traps using a wrist traction tower with approxi-
mately 10 to 15 pounds of traction depending on the size ofthe extremity Joint distention by saline infusion is usually notrequired to completely visualize the joint26 Te authorsrsquo pref-erence is to use a dry technique which facilitates arthroscopicrepair methods2728
A 27-mm arthroscope is used routinely but the 19-mm ar-throscope is used for smaller wrists Te wrist is systematicallyevaluated by RC-Arth with the scope in the 3-4 portal Care istaken to detect any associated disorders of the ulnar carpus
ears of the dc-FCC are visualized on the dorsoulnar portionof the articular disk and are frequently covered by hypertrophicsynovitis or fibrovascular granulation tissue which is removed with a small motorized shaver
A probe is inserted into the 6R portal to palpate the articulardisk and to assess the tension to the FCCmdashby the trampolinetest and the hook test
If the FCC is redundant and tests are positive for loss ofnormal resilience pc-FCC integrity and tautness are evaluatedthrough DRU-Arth
Te forearm is supinated the traction reduced and the DRUJexplored through the distal DRUJ portal In smaller wrists use ofa volar ulnar (VU) portal is recommended29 Scope insertion iseasier when the pc-FCC is torn since the articular disk is looseand more joint space is available DRU-Arth shows the ligamen-tous laceration or avulsion of the pc-FCC from the fovea Fora preliminary assessment of pc-FCC tautness an 18-gaugeneedle is inserted percutaneously about 1 cm proximal to the 6Uportal with the forearm held in full supination
When a FCC Palmer type 1B tear is associated with DRUJinstability the most common finding is the combination of a dc-FCC tear and a pc-FCC avulsion (complete FCC tear class 2)
Less frequently a pc-FCC tear is present as an isolated finding(proximal FCC tear class 3) In the latter case a standard RC- Arth reveals a normal FCC appearance which may lead to themisdiagnosis of a normal FCC since the pc-FCC tear can bedemonstrated only by DRU-Arth For this reason DRU-Arth isconsidered mandatory in cases of a suspected FCC tear that isassociated with DRUJ instability
Repair Technique
Repair of the foveal insertion of the FCC is performed by reat-tachment of the pc-FCC through a suture screw or anchor23
Te procedure begins with debridement of the foveal region as well as the torn edges of the FCC back to healthy tissue using asmall motorized shaver inserted through the 6R portal Althoughthe fovea can be debrided from the radiocarpal joint through theFCC tear it is recommended to establish a separate DRUJ por-
tal not only to remove the ligamentous remnants and refresh thebone at the fovea but also to drill and insert the suture screwanchor A dedicated working portal named the direct foveal (DF)portal has been devised to provide access to the fovea ulnaris2223
Te DF portal is located about 1 cm proximal to the 6U portaland is created with the forearm held in full supination Full fore-arm supination produces dorsal displacement of the ulnar styloidand the ECU tendon and uncovers the volar aspect of the distalulna on wristrsquos ulnar side (Fig 54-3) Tus the fovea and the
ulnarmost area of the distal ulna become subcutaneous and maybe reached through a very limited exposure Te DF portal is lesstechnically demanding compared with the formal VU portal29 but its use is limited to the introduction of working instrumentsin the area of the ulnar styloid and fovea (Fig 54-4)
After portal placement is checked under arthroscopic control
with an 18-gauge needle the longitudinal skin incision of the 6Uportal is extended proximally between the ECU and the flexorcarpi ulnaris (FCU) for a total length of 2 to 25 cm Troughthis mini-open approach the dorsal sensory branch of the ulnarnerve (DSBUN) and its transverse branches are identified andprotected by careful subcutaneous dissection Te risk of damag-ing the DSBUN is further reduced as the forearm is supinatedgiven that the DSBUN is displaced more volarly and along aslacker path than when the forearm is held in neutral position
Te extensor retinaculum is exposed and split along the courseof its fibers Te DRUJ capsule is incised longitudinally to reachthe distal articular surface of the ulnar head under the FCCTe fovea is located volarly at the base of the ulnar styloid justlateral to the capsule
With the scope in the distal DRUJ portal a small shaver orcuret can be inserted through the DF portal to refresh the torn
avulsed ligament to remove the inflammatory fibrovascular tissuefrom the fovea and to prepare it for suture screwanchor inser-tion Curettage of the fovea can also be performed as a mini-openprocedure
Screwanchor drilling and insertion are performed as a mini-open procedure as well (Fig 54-5) Te fovea is palpable as anarea of soft bone at the base of the ulnar styloid just lateral tothe capsule A power drill and intraoperative fluoroscopy are notrequired although the latter may be advisable for the less experi-enced surgeon
It is recommended to use a screwanchor that supports a pairof sutures so that a distinct suture can be passed through eachlimb of the radioulnar ligament Tis also improves the strengthof the repair by recreating a broader footprint of the pc-FCCanalogous to a rotator cuff repair in the shoulder30 Te authors
prefer to use a 28 or 32 titanium screw with two preloaded non-absorbable 2-0 Ultrabraid sutures (winfix Smith amp Nephew Andover MA) or a 35-mm absorbable screw preloaded withtwo 2-0 FiberWire sutures (Bio-Corkscrew Arthrex Naples FL)
Once the screw is in place sutures should exit the DF por-tal from underneath the FCC (Fig 54-6) Ten the wrist isplaced back in neutral pronosupination so that the screwrsquos head isbrought under the ulnarmost part of the FCC
Te suture ends are inserted into the tip of a 25-gauge needleor preferably a uohy needle to facilitate passage through theFCC
With the scope in the 3-4 portal the first suture is inserted inan outside-in fashion from the DF portal close to the FCCrsquospalmar contour to hold the palmar limb of the radioulnar liga-ment (Fig 54-7) A grasper is used to retrieve the suture from the6U portal (Fig 54-8) Te same procedure is repeated for sutur-
ing the dorsal limb of the radioulnar ligamentTe wrist traction is then released and the forearm is held in
neutral rotation Te surgical assistant maintains the ulnar head inreduced position Te sutures are tied under arthroscopic controlusing a small knot-pusher ensuring adequate pc-FCC compres-sion against the distal ulna (Fig 54-9) Knots should be located atthe prestyloid recess or just outside the DRUJ capsule (Fig 54-10)
RC-Arth is used as a control to ensure complete tear closureEven in the larger type 2 FCC peripheral tears it is seldom
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 610
Part IX Ligament InstabilityTears564
necessary to apply any further ligament-to-capsule sutures toclose off the dc-FCC
Te DRUJ is evaluated for complete range of pronosupinationand residual instability
Te DRUJ capsule and the opening between retinaculum fi-bers are approximated with two PDS 4-0 stitches Skin is closedby a subcuticular running suture
Postoperative Treatment
Te patient is placed in a long-arm splint in neutral forearm rota-tion for the first week which is substituted by a short Muumlnster
splint for another 2 weeksFull wrist flexionextension can be started as early as 3 weeks post-
operatively During the first week of rehabilitation progressive fore-arm rotation is allowed but the splint is still worn between exercises
During the following 6 weeks the patient is not permitted toperform any resistance movements Progressive resistance wrist-and hand-strengthening exercises are begun after the sixth weekuntil the patient is able to bear weight on the operated wrist Sportand heavy work activities are started 3 months postoperatively
COMPLICATIONS
Few complications should be encountered during arthroscopic-assisted palmar repair of the foveal insertion of the FCC providedthat there is careful application of standard arthroscopic principlesand of the described surgical technique Te most serious complica-tion is potential injury to the DSBUN which is related to surgicalexperience It can be prevented by careful dissection techniques anda sound understanding of the underlying anatomy and its variationfollowing forearm rotation ransitory neuropraxia of the DSBUNmay be observed which recovers spontaneously in 3 to 4 months
Te surgical scar of the ulnar side of the wrist may adhere to deeperstructures and become painful during the first stages of physicaltherapy especially after a prolonged period of wrist immobilization
As in other arthroscopic procedures infection remains a risk which is usually prevented by a prophylactic dose of parenteralantibiotics before initiating the procedure
Te dry technique of joint exploration27 is recommended toreduce soft tissue infiltration and swelling by the continuous leak-ing of saline through the portals
FIGURE 54-3 Full forearm supination is required to create the direct foveal (DF) portal After supination the ulnar styloid and the extensorcarpi ulnaris tendon displace dorsally and the fovea and the ulnarmost area of the distal ulna become subcutaneous (From
Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
Fovea
Neutral PS Supination
DF
portal
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 710
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-5 Screwanchor drilling and insertion are performed as a mini-open procedure through the direct foveal portal (From Atzei ARizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar
joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
FIGURE 54-4 The direct foveal (DF) portal is located about 1 cm proximal to the 6U portal It has been devised as a working portal toprovide access to the area of the ulnar styloid and fovea With the scope in the distal radioulnar joint portal a curet
or small shaver is inserted through the DF portal to refresh the tornavulsed ligament and the fovea (From Atzei A Rizzo A Luchetti R Fairplay TArthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up ExtremSurg 200812226ndash235)
6-U
DF
A B
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 810
Part IX Ligament InstabilityTears566
FIGURE 54-6 Once the screw is in place sutures should exit the direct foveal portal from underneath the triangular 1047297brocartilage complex(TFCC) When the wrist is placed back in neutral pronosupination the screwrsquos head is brought under the TFCC (From Atzei A
Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability TechHand Up Extrem Surg 200812226ndash235)
Te technique of arthroscopic-assisted palmar repair of the fo-veal insertion of the FCC has a learning curve However once
the technique is mastered the rate of complications for this pro-cedure is comparable to that of larger series of common wristarthroscopic procedures31
RESULTS
Te authorsrsquo clinical experience started in 2001 and up until now we have operated on 37 FCC tears (29 type 2 FCC peripheraltears and 8 type 3 tears)
In a control series study 18 patients (13 males and5 females with a mean age of 342) were investigated prospec-
tively for a minimum follow-up of 1 year (average 18 monthsmaximum 37 months) All patients had a history of traumacomplained of pain in the ulnar fovea and had clinical signsof DRUJ instability ranging from mild (10 patients) to mod-erate (8 patients) Although radiographs showed a positive ul-nar variance in three patients there were no detectable signsof ulnocarpal impaction or carpal degenerative chondropa-thy Arthroscopy revealed a Palmer type 1B ulnar avulsionof the FCC in all patients Fourteen cases were classified as
FIGURE 54-7 With the scope in the 3-4 portal the 1047297rst suture end is inserted into the tip of a 25-gauge needle (preferably a Tuohy needle) The needle is passed through the triangular 1047297brocartilage complex (TFCC) in an outside-in fashion via the direct foveal portal
toward the palmar contour of the TFCC (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complexperipheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 910
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-8 A grasper is inserted through the 6U portal and used to retrieve the suture (From Atzei A Rizzo A Luchetti R Fairplay T Arthro-scopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up
Extrem Surg 200812226ndash235)
FIGURE 54-9 The suture is tied under arthroscopic control using a small knot-pusher The pc-TFCC (proximal component of the triangular1047297brocartilage complex) is pushed forcefully against the distal ulna provided that the wrist traction is released the forearm is
held in neutral rotation and the ulnar head is reduced by the assistant (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
complete FCC peripheral tears (type 2) and four as proximaltears (type 3)
At fol low-up evaluation the patients showed an increasedrange of motion (from 907 to 96 of the contralateralside) and grip strength (from 73 to 90) Pain decreasedfrom 83 to 12 on a 10-point visual analogue scale Gripstrength and pain changes reached statistical significance
(P lt 005) he Modified Mayo Wrist Score was excellentin 14 patients good in 3 and fair in 1 A total of 944 ofthe results scored excellent and good DASH (disabilities ofthe arm shoulder and hand) score averaged 105 Fifteenpatients (833) resumed previous work and recreation-al activities and 3 patients (167) returned to restrictedemployment
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 1010
Part IX Ligament InstabilityTears568
REFERENCES
1 Palmer AK riangular fibrocartilage complex lesions a classification J HandSurg [Am] 198914594ndash606
2 Nakamura Yabe Y Horiuchi Y Functional anatomy of the triangularfibrocartilage complex J Hand Surg [Br] 199621581ndash586
3 Palmer AK Werner F W Te triangular fibrocartilage complex of the wristmdashanatomy and function J Hand Surg [Am] 19816153ndash162
4 Adams BD Holly K A Strains in the articular disk of the triangular fibro-cartilage complex a biomechanical study J Hand Surg [Am] 199318919ndash925
5 Benjamin M Evans E J Pemberton D J Histological studies on the triangularfibrocartilage complex of the wrist J Anat 199017259ndash67
6 Kauer JMG Te distal radioulnar joint anatomic and functional consider-ations Clin Orthop 199227537ndash45
7 Atzei A Luchetti R Garcia-Elias M Lesioni capsulo-legamentose dellaradio-ulnare distale e fibrocartilagine triangolare In Landi A Catalano FLuchetti R (eds) rattato di Chirurgia della Mano Verduci Editore Roma2006 pp 159ndash187
8 Kleinman WB Stability of the distal radioulnar joint biomechanics patho-physiology physical diagnosis and restoration of function What we havelearned in 25 years J Hand Surg [Am] 2007321087ndash1106
9 Garcia-Elias M Smith DE Llusa M Surgical approach to the triangularfibrocartilage complex ech Hand Up Extrem Surg 20037(4)134ndash140
10 Nakamura Nakao Y Ikegami H et al Open repair of the ulnar disruptionof the triangular fibrocartilage complex with double three-dimensional mat-tress suturing technique ech Hand Up Extrem Surg 20048(2)116ndash123
11 Hermansdorfer JD Kleinman WB Management of chronic peripheraltears of the triangular fibrocartilage complex J Hand Surg [Am] 199116340ndash346
12 Chou KH Sarris IK Sotereanos DG Suture anchor repair of ulnar-sidedtriangular fibrocartilage complex tears J Hand Surg [Br] 200328546ndash550
13 Slutsky D J Clinical applications of volar portals in wrist arthroscopy echHand Up Extrem Surg 20048(4)229ndash238
14 omaino M Weiser R Combined arthroscopic FCC debridement and wa-fer resection of the distal ulna in wrists with triangular fibrocartilage complextears and positive ulnar variance J Hand Surg [Am] 2001261047ndash1052
15 Hanker G J Management of ulnar impaction syndrome In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 63ndash71
16 Moskal M J Savoie FH III Management of lunotriquetral instability InGeissler WB (ed) Wrist Arthroscopy New York Springer-Verlag 2005pp 94ndash101
17 Atzei A Luchetti R Clinical approach to the painful wrist In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 185ndash195
18 ay SC omita K Berger R A Te ldquoulnar fovea signrdquo for defining ulnar wrist pain an analysis of sensitivity and specificity J Hand Surg [Am]200732(4)438ndash444
19 Zanetti M Bram J Hodler J riangular fibrocartilage and intercarpal liga-ments of the wrist does MR arthrography improve standard MRI J Magn
Reson Imaging 19977 (3)590ndash59420 Pederzini L Luchetti R Soragni O et al Evaluation of the triangular
fibrocartilage complex tears by arthroscopy arthrography and magnetic reso-nance imaging Arthroscopy 19928191ndash197
21 Fulcher S Poehling G Te role of operative arthroscopy for the diag-nosis and treatment of lesions about the distal ulna Hand Clin 199814285ndash296
22 Atzei A New trends in arthroscopic management of type 1-B FCC injuries with DRUJ instability J Hand Surg [Eur] 2009Epub ahead of print
23 Atzei A Rizzo A Luchetti R Fairplay Arthroscopic foveal repair of tri-angular fibrocartilage complex peripheral lesion with distal radioulnar jointinstability ech Hand Up Extrem Surg 200812226ndash235
24 Adams BD Anatomic reconstruction of the distal radioulnar ligaments forDRUJ instability ech Hand Up Extrem Surg 20004154ndash160
25 Atzei A Luchetti R Borelli PP et al Arthroscopic FCC reconstruction bytendon graft Riv Chir Mano 200643(3)370ndash376
26 Atzei A Luchetti R Sgarbossa A et al Set-up portals and normal explora-tion in wrist arthroscopy Chir Main 200625S131ndashS144
27 del Pintildeal F Garciacutea-Bernal F J Pisani D et al Dry arthroscopy of the wrist
surgical technique J Hand Surg [Am] 200732119ndash12328 del Pintildeal F Garciacutea-Bernal F J Delgado J et al Correction of malunited
intra-articular distal radius fractures with an inside-out osteotomy technique J Hand Surg [Am] 200531(6)1029ndash1034
29 Slutsky D J Distal radioulnar joint arthroscopy and the volar ulnar portalech Hand Up Extrem Surg 200711(1)38ndash44
30 Lo IK Y Burkhart SS Double-row arthroscopic rotator cuff repair re-establishing the footprint of the rotator cuff Arthroscopy 200319(9)1035ndash1042
31 Luchetti R Atzei A Rocchi L Incidence and causes of failures in wristarthroscopic techniques Chir Main 200625(1)48ndash53
FIGURE 54-10 At the end of the procedure the knots of bothsutures are located at the level of the 6U portal just
outside the distal radioulnar joint capsule or in the prestyloid recess(From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)

8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 510
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
examined again before starting the arthroscopic procedure Com-plete forearm muscle relaxation following anesthesia may revealpreviously undetected DRUJ instability Te upper limb is exsan-guinated and the tourniquet is inflated to 250 mm Hg
A standard wrist arthroscopy setup is used26 Te wrist is sus-pended by finger traps using a wrist traction tower with approxi-
mately 10 to 15 pounds of traction depending on the size ofthe extremity Joint distention by saline infusion is usually notrequired to completely visualize the joint26 Te authorsrsquo pref-erence is to use a dry technique which facilitates arthroscopicrepair methods2728
A 27-mm arthroscope is used routinely but the 19-mm ar-throscope is used for smaller wrists Te wrist is systematicallyevaluated by RC-Arth with the scope in the 3-4 portal Care istaken to detect any associated disorders of the ulnar carpus
ears of the dc-FCC are visualized on the dorsoulnar portionof the articular disk and are frequently covered by hypertrophicsynovitis or fibrovascular granulation tissue which is removed with a small motorized shaver
A probe is inserted into the 6R portal to palpate the articulardisk and to assess the tension to the FCCmdashby the trampolinetest and the hook test
If the FCC is redundant and tests are positive for loss ofnormal resilience pc-FCC integrity and tautness are evaluatedthrough DRU-Arth
Te forearm is supinated the traction reduced and the DRUJexplored through the distal DRUJ portal In smaller wrists use ofa volar ulnar (VU) portal is recommended29 Scope insertion iseasier when the pc-FCC is torn since the articular disk is looseand more joint space is available DRU-Arth shows the ligamen-tous laceration or avulsion of the pc-FCC from the fovea Fora preliminary assessment of pc-FCC tautness an 18-gaugeneedle is inserted percutaneously about 1 cm proximal to the 6Uportal with the forearm held in full supination
When a FCC Palmer type 1B tear is associated with DRUJinstability the most common finding is the combination of a dc-FCC tear and a pc-FCC avulsion (complete FCC tear class 2)
Less frequently a pc-FCC tear is present as an isolated finding(proximal FCC tear class 3) In the latter case a standard RC- Arth reveals a normal FCC appearance which may lead to themisdiagnosis of a normal FCC since the pc-FCC tear can bedemonstrated only by DRU-Arth For this reason DRU-Arth isconsidered mandatory in cases of a suspected FCC tear that isassociated with DRUJ instability
Repair Technique
Repair of the foveal insertion of the FCC is performed by reat-tachment of the pc-FCC through a suture screw or anchor23
Te procedure begins with debridement of the foveal region as well as the torn edges of the FCC back to healthy tissue using asmall motorized shaver inserted through the 6R portal Althoughthe fovea can be debrided from the radiocarpal joint through theFCC tear it is recommended to establish a separate DRUJ por-
tal not only to remove the ligamentous remnants and refresh thebone at the fovea but also to drill and insert the suture screwanchor A dedicated working portal named the direct foveal (DF)portal has been devised to provide access to the fovea ulnaris2223
Te DF portal is located about 1 cm proximal to the 6U portaland is created with the forearm held in full supination Full fore-arm supination produces dorsal displacement of the ulnar styloidand the ECU tendon and uncovers the volar aspect of the distalulna on wristrsquos ulnar side (Fig 54-3) Tus the fovea and the
ulnarmost area of the distal ulna become subcutaneous and maybe reached through a very limited exposure Te DF portal is lesstechnically demanding compared with the formal VU portal29 but its use is limited to the introduction of working instrumentsin the area of the ulnar styloid and fovea (Fig 54-4)
After portal placement is checked under arthroscopic control
with an 18-gauge needle the longitudinal skin incision of the 6Uportal is extended proximally between the ECU and the flexorcarpi ulnaris (FCU) for a total length of 2 to 25 cm Troughthis mini-open approach the dorsal sensory branch of the ulnarnerve (DSBUN) and its transverse branches are identified andprotected by careful subcutaneous dissection Te risk of damag-ing the DSBUN is further reduced as the forearm is supinatedgiven that the DSBUN is displaced more volarly and along aslacker path than when the forearm is held in neutral position
Te extensor retinaculum is exposed and split along the courseof its fibers Te DRUJ capsule is incised longitudinally to reachthe distal articular surface of the ulnar head under the FCCTe fovea is located volarly at the base of the ulnar styloid justlateral to the capsule
With the scope in the distal DRUJ portal a small shaver orcuret can be inserted through the DF portal to refresh the torn
avulsed ligament to remove the inflammatory fibrovascular tissuefrom the fovea and to prepare it for suture screwanchor inser-tion Curettage of the fovea can also be performed as a mini-openprocedure
Screwanchor drilling and insertion are performed as a mini-open procedure as well (Fig 54-5) Te fovea is palpable as anarea of soft bone at the base of the ulnar styloid just lateral tothe capsule A power drill and intraoperative fluoroscopy are notrequired although the latter may be advisable for the less experi-enced surgeon
It is recommended to use a screwanchor that supports a pairof sutures so that a distinct suture can be passed through eachlimb of the radioulnar ligament Tis also improves the strengthof the repair by recreating a broader footprint of the pc-FCCanalogous to a rotator cuff repair in the shoulder30 Te authors
prefer to use a 28 or 32 titanium screw with two preloaded non-absorbable 2-0 Ultrabraid sutures (winfix Smith amp Nephew Andover MA) or a 35-mm absorbable screw preloaded withtwo 2-0 FiberWire sutures (Bio-Corkscrew Arthrex Naples FL)
Once the screw is in place sutures should exit the DF por-tal from underneath the FCC (Fig 54-6) Ten the wrist isplaced back in neutral pronosupination so that the screwrsquos head isbrought under the ulnarmost part of the FCC
Te suture ends are inserted into the tip of a 25-gauge needleor preferably a uohy needle to facilitate passage through theFCC
With the scope in the 3-4 portal the first suture is inserted inan outside-in fashion from the DF portal close to the FCCrsquospalmar contour to hold the palmar limb of the radioulnar liga-ment (Fig 54-7) A grasper is used to retrieve the suture from the6U portal (Fig 54-8) Te same procedure is repeated for sutur-
ing the dorsal limb of the radioulnar ligamentTe wrist traction is then released and the forearm is held in
neutral rotation Te surgical assistant maintains the ulnar head inreduced position Te sutures are tied under arthroscopic controlusing a small knot-pusher ensuring adequate pc-FCC compres-sion against the distal ulna (Fig 54-9) Knots should be located atthe prestyloid recess or just outside the DRUJ capsule (Fig 54-10)
RC-Arth is used as a control to ensure complete tear closureEven in the larger type 2 FCC peripheral tears it is seldom
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 610
Part IX Ligament InstabilityTears564
necessary to apply any further ligament-to-capsule sutures toclose off the dc-FCC
Te DRUJ is evaluated for complete range of pronosupinationand residual instability
Te DRUJ capsule and the opening between retinaculum fi-bers are approximated with two PDS 4-0 stitches Skin is closedby a subcuticular running suture
Postoperative Treatment
Te patient is placed in a long-arm splint in neutral forearm rota-tion for the first week which is substituted by a short Muumlnster
splint for another 2 weeksFull wrist flexionextension can be started as early as 3 weeks post-
operatively During the first week of rehabilitation progressive fore-arm rotation is allowed but the splint is still worn between exercises
During the following 6 weeks the patient is not permitted toperform any resistance movements Progressive resistance wrist-and hand-strengthening exercises are begun after the sixth weekuntil the patient is able to bear weight on the operated wrist Sportand heavy work activities are started 3 months postoperatively
COMPLICATIONS
Few complications should be encountered during arthroscopic-assisted palmar repair of the foveal insertion of the FCC providedthat there is careful application of standard arthroscopic principlesand of the described surgical technique Te most serious complica-tion is potential injury to the DSBUN which is related to surgicalexperience It can be prevented by careful dissection techniques anda sound understanding of the underlying anatomy and its variationfollowing forearm rotation ransitory neuropraxia of the DSBUNmay be observed which recovers spontaneously in 3 to 4 months
Te surgical scar of the ulnar side of the wrist may adhere to deeperstructures and become painful during the first stages of physicaltherapy especially after a prolonged period of wrist immobilization
As in other arthroscopic procedures infection remains a risk which is usually prevented by a prophylactic dose of parenteralantibiotics before initiating the procedure
Te dry technique of joint exploration27 is recommended toreduce soft tissue infiltration and swelling by the continuous leak-ing of saline through the portals
FIGURE 54-3 Full forearm supination is required to create the direct foveal (DF) portal After supination the ulnar styloid and the extensorcarpi ulnaris tendon displace dorsally and the fovea and the ulnarmost area of the distal ulna become subcutaneous (From
Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
Fovea
Neutral PS Supination
DF
portal
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 710
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-5 Screwanchor drilling and insertion are performed as a mini-open procedure through the direct foveal portal (From Atzei ARizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar
joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
FIGURE 54-4 The direct foveal (DF) portal is located about 1 cm proximal to the 6U portal It has been devised as a working portal toprovide access to the area of the ulnar styloid and fovea With the scope in the distal radioulnar joint portal a curet
or small shaver is inserted through the DF portal to refresh the tornavulsed ligament and the fovea (From Atzei A Rizzo A Luchetti R Fairplay TArthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up ExtremSurg 200812226ndash235)
6-U
DF
A B
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 810
Part IX Ligament InstabilityTears566
FIGURE 54-6 Once the screw is in place sutures should exit the direct foveal portal from underneath the triangular 1047297brocartilage complex(TFCC) When the wrist is placed back in neutral pronosupination the screwrsquos head is brought under the TFCC (From Atzei A
Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability TechHand Up Extrem Surg 200812226ndash235)
Te technique of arthroscopic-assisted palmar repair of the fo-veal insertion of the FCC has a learning curve However once
the technique is mastered the rate of complications for this pro-cedure is comparable to that of larger series of common wristarthroscopic procedures31
RESULTS
Te authorsrsquo clinical experience started in 2001 and up until now we have operated on 37 FCC tears (29 type 2 FCC peripheraltears and 8 type 3 tears)
In a control series study 18 patients (13 males and5 females with a mean age of 342) were investigated prospec-
tively for a minimum follow-up of 1 year (average 18 monthsmaximum 37 months) All patients had a history of traumacomplained of pain in the ulnar fovea and had clinical signsof DRUJ instability ranging from mild (10 patients) to mod-erate (8 patients) Although radiographs showed a positive ul-nar variance in three patients there were no detectable signsof ulnocarpal impaction or carpal degenerative chondropa-thy Arthroscopy revealed a Palmer type 1B ulnar avulsionof the FCC in all patients Fourteen cases were classified as
FIGURE 54-7 With the scope in the 3-4 portal the 1047297rst suture end is inserted into the tip of a 25-gauge needle (preferably a Tuohy needle) The needle is passed through the triangular 1047297brocartilage complex (TFCC) in an outside-in fashion via the direct foveal portal
toward the palmar contour of the TFCC (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complexperipheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 910
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-8 A grasper is inserted through the 6U portal and used to retrieve the suture (From Atzei A Rizzo A Luchetti R Fairplay T Arthro-scopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up
Extrem Surg 200812226ndash235)
FIGURE 54-9 The suture is tied under arthroscopic control using a small knot-pusher The pc-TFCC (proximal component of the triangular1047297brocartilage complex) is pushed forcefully against the distal ulna provided that the wrist traction is released the forearm is
held in neutral rotation and the ulnar head is reduced by the assistant (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
complete FCC peripheral tears (type 2) and four as proximaltears (type 3)
At fol low-up evaluation the patients showed an increasedrange of motion (from 907 to 96 of the contralateralside) and grip strength (from 73 to 90) Pain decreasedfrom 83 to 12 on a 10-point visual analogue scale Gripstrength and pain changes reached statistical significance
(P lt 005) he Modified Mayo Wrist Score was excellentin 14 patients good in 3 and fair in 1 A total of 944 ofthe results scored excellent and good DASH (disabilities ofthe arm shoulder and hand) score averaged 105 Fifteenpatients (833) resumed previous work and recreation-al activities and 3 patients (167) returned to restrictedemployment
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 1010
Part IX Ligament InstabilityTears568
REFERENCES
1 Palmer AK riangular fibrocartilage complex lesions a classification J HandSurg [Am] 198914594ndash606
2 Nakamura Yabe Y Horiuchi Y Functional anatomy of the triangularfibrocartilage complex J Hand Surg [Br] 199621581ndash586
3 Palmer AK Werner F W Te triangular fibrocartilage complex of the wristmdashanatomy and function J Hand Surg [Am] 19816153ndash162
4 Adams BD Holly K A Strains in the articular disk of the triangular fibro-cartilage complex a biomechanical study J Hand Surg [Am] 199318919ndash925
5 Benjamin M Evans E J Pemberton D J Histological studies on the triangularfibrocartilage complex of the wrist J Anat 199017259ndash67
6 Kauer JMG Te distal radioulnar joint anatomic and functional consider-ations Clin Orthop 199227537ndash45
7 Atzei A Luchetti R Garcia-Elias M Lesioni capsulo-legamentose dellaradio-ulnare distale e fibrocartilagine triangolare In Landi A Catalano FLuchetti R (eds) rattato di Chirurgia della Mano Verduci Editore Roma2006 pp 159ndash187
8 Kleinman WB Stability of the distal radioulnar joint biomechanics patho-physiology physical diagnosis and restoration of function What we havelearned in 25 years J Hand Surg [Am] 2007321087ndash1106
9 Garcia-Elias M Smith DE Llusa M Surgical approach to the triangularfibrocartilage complex ech Hand Up Extrem Surg 20037(4)134ndash140
10 Nakamura Nakao Y Ikegami H et al Open repair of the ulnar disruptionof the triangular fibrocartilage complex with double three-dimensional mat-tress suturing technique ech Hand Up Extrem Surg 20048(2)116ndash123
11 Hermansdorfer JD Kleinman WB Management of chronic peripheraltears of the triangular fibrocartilage complex J Hand Surg [Am] 199116340ndash346
12 Chou KH Sarris IK Sotereanos DG Suture anchor repair of ulnar-sidedtriangular fibrocartilage complex tears J Hand Surg [Br] 200328546ndash550
13 Slutsky D J Clinical applications of volar portals in wrist arthroscopy echHand Up Extrem Surg 20048(4)229ndash238
14 omaino M Weiser R Combined arthroscopic FCC debridement and wa-fer resection of the distal ulna in wrists with triangular fibrocartilage complextears and positive ulnar variance J Hand Surg [Am] 2001261047ndash1052
15 Hanker G J Management of ulnar impaction syndrome In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 63ndash71
16 Moskal M J Savoie FH III Management of lunotriquetral instability InGeissler WB (ed) Wrist Arthroscopy New York Springer-Verlag 2005pp 94ndash101
17 Atzei A Luchetti R Clinical approach to the painful wrist In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 185ndash195
18 ay SC omita K Berger R A Te ldquoulnar fovea signrdquo for defining ulnar wrist pain an analysis of sensitivity and specificity J Hand Surg [Am]200732(4)438ndash444
19 Zanetti M Bram J Hodler J riangular fibrocartilage and intercarpal liga-ments of the wrist does MR arthrography improve standard MRI J Magn
Reson Imaging 19977 (3)590ndash59420 Pederzini L Luchetti R Soragni O et al Evaluation of the triangular
fibrocartilage complex tears by arthroscopy arthrography and magnetic reso-nance imaging Arthroscopy 19928191ndash197
21 Fulcher S Poehling G Te role of operative arthroscopy for the diag-nosis and treatment of lesions about the distal ulna Hand Clin 199814285ndash296
22 Atzei A New trends in arthroscopic management of type 1-B FCC injuries with DRUJ instability J Hand Surg [Eur] 2009Epub ahead of print
23 Atzei A Rizzo A Luchetti R Fairplay Arthroscopic foveal repair of tri-angular fibrocartilage complex peripheral lesion with distal radioulnar jointinstability ech Hand Up Extrem Surg 200812226ndash235
24 Adams BD Anatomic reconstruction of the distal radioulnar ligaments forDRUJ instability ech Hand Up Extrem Surg 20004154ndash160
25 Atzei A Luchetti R Borelli PP et al Arthroscopic FCC reconstruction bytendon graft Riv Chir Mano 200643(3)370ndash376
26 Atzei A Luchetti R Sgarbossa A et al Set-up portals and normal explora-tion in wrist arthroscopy Chir Main 200625S131ndashS144
27 del Pintildeal F Garciacutea-Bernal F J Pisani D et al Dry arthroscopy of the wrist
surgical technique J Hand Surg [Am] 200732119ndash12328 del Pintildeal F Garciacutea-Bernal F J Delgado J et al Correction of malunited
intra-articular distal radius fractures with an inside-out osteotomy technique J Hand Surg [Am] 200531(6)1029ndash1034
29 Slutsky D J Distal radioulnar joint arthroscopy and the volar ulnar portalech Hand Up Extrem Surg 200711(1)38ndash44
30 Lo IK Y Burkhart SS Double-row arthroscopic rotator cuff repair re-establishing the footprint of the rotator cuff Arthroscopy 200319(9)1035ndash1042
31 Luchetti R Atzei A Rocchi L Incidence and causes of failures in wristarthroscopic techniques Chir Main 200625(1)48ndash53
FIGURE 54-10 At the end of the procedure the knots of bothsutures are located at the level of the 6U portal just
outside the distal radioulnar joint capsule or in the prestyloid recess(From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)

8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 610
Part IX Ligament InstabilityTears564
necessary to apply any further ligament-to-capsule sutures toclose off the dc-FCC
Te DRUJ is evaluated for complete range of pronosupinationand residual instability
Te DRUJ capsule and the opening between retinaculum fi-bers are approximated with two PDS 4-0 stitches Skin is closedby a subcuticular running suture
Postoperative Treatment
Te patient is placed in a long-arm splint in neutral forearm rota-tion for the first week which is substituted by a short Muumlnster
splint for another 2 weeksFull wrist flexionextension can be started as early as 3 weeks post-
operatively During the first week of rehabilitation progressive fore-arm rotation is allowed but the splint is still worn between exercises
During the following 6 weeks the patient is not permitted toperform any resistance movements Progressive resistance wrist-and hand-strengthening exercises are begun after the sixth weekuntil the patient is able to bear weight on the operated wrist Sportand heavy work activities are started 3 months postoperatively
COMPLICATIONS
Few complications should be encountered during arthroscopic-assisted palmar repair of the foveal insertion of the FCC providedthat there is careful application of standard arthroscopic principlesand of the described surgical technique Te most serious complica-tion is potential injury to the DSBUN which is related to surgicalexperience It can be prevented by careful dissection techniques anda sound understanding of the underlying anatomy and its variationfollowing forearm rotation ransitory neuropraxia of the DSBUNmay be observed which recovers spontaneously in 3 to 4 months
Te surgical scar of the ulnar side of the wrist may adhere to deeperstructures and become painful during the first stages of physicaltherapy especially after a prolonged period of wrist immobilization
As in other arthroscopic procedures infection remains a risk which is usually prevented by a prophylactic dose of parenteralantibiotics before initiating the procedure
Te dry technique of joint exploration27 is recommended toreduce soft tissue infiltration and swelling by the continuous leak-ing of saline through the portals
FIGURE 54-3 Full forearm supination is required to create the direct foveal (DF) portal After supination the ulnar styloid and the extensorcarpi ulnaris tendon displace dorsally and the fovea and the ulnarmost area of the distal ulna become subcutaneous (From
Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
Fovea
Neutral PS Supination
DF
portal
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 710
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-5 Screwanchor drilling and insertion are performed as a mini-open procedure through the direct foveal portal (From Atzei ARizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar
joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
FIGURE 54-4 The direct foveal (DF) portal is located about 1 cm proximal to the 6U portal It has been devised as a working portal toprovide access to the area of the ulnar styloid and fovea With the scope in the distal radioulnar joint portal a curet
or small shaver is inserted through the DF portal to refresh the tornavulsed ligament and the fovea (From Atzei A Rizzo A Luchetti R Fairplay TArthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up ExtremSurg 200812226ndash235)
6-U
DF
A B
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 810
Part IX Ligament InstabilityTears566
FIGURE 54-6 Once the screw is in place sutures should exit the direct foveal portal from underneath the triangular 1047297brocartilage complex(TFCC) When the wrist is placed back in neutral pronosupination the screwrsquos head is brought under the TFCC (From Atzei A
Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability TechHand Up Extrem Surg 200812226ndash235)
Te technique of arthroscopic-assisted palmar repair of the fo-veal insertion of the FCC has a learning curve However once
the technique is mastered the rate of complications for this pro-cedure is comparable to that of larger series of common wristarthroscopic procedures31
RESULTS
Te authorsrsquo clinical experience started in 2001 and up until now we have operated on 37 FCC tears (29 type 2 FCC peripheraltears and 8 type 3 tears)
In a control series study 18 patients (13 males and5 females with a mean age of 342) were investigated prospec-
tively for a minimum follow-up of 1 year (average 18 monthsmaximum 37 months) All patients had a history of traumacomplained of pain in the ulnar fovea and had clinical signsof DRUJ instability ranging from mild (10 patients) to mod-erate (8 patients) Although radiographs showed a positive ul-nar variance in three patients there were no detectable signsof ulnocarpal impaction or carpal degenerative chondropa-thy Arthroscopy revealed a Palmer type 1B ulnar avulsionof the FCC in all patients Fourteen cases were classified as
FIGURE 54-7 With the scope in the 3-4 portal the 1047297rst suture end is inserted into the tip of a 25-gauge needle (preferably a Tuohy needle) The needle is passed through the triangular 1047297brocartilage complex (TFCC) in an outside-in fashion via the direct foveal portal
toward the palmar contour of the TFCC (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complexperipheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 910
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-8 A grasper is inserted through the 6U portal and used to retrieve the suture (From Atzei A Rizzo A Luchetti R Fairplay T Arthro-scopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up
Extrem Surg 200812226ndash235)
FIGURE 54-9 The suture is tied under arthroscopic control using a small knot-pusher The pc-TFCC (proximal component of the triangular1047297brocartilage complex) is pushed forcefully against the distal ulna provided that the wrist traction is released the forearm is
held in neutral rotation and the ulnar head is reduced by the assistant (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
complete FCC peripheral tears (type 2) and four as proximaltears (type 3)
At fol low-up evaluation the patients showed an increasedrange of motion (from 907 to 96 of the contralateralside) and grip strength (from 73 to 90) Pain decreasedfrom 83 to 12 on a 10-point visual analogue scale Gripstrength and pain changes reached statistical significance
(P lt 005) he Modified Mayo Wrist Score was excellentin 14 patients good in 3 and fair in 1 A total of 944 ofthe results scored excellent and good DASH (disabilities ofthe arm shoulder and hand) score averaged 105 Fifteenpatients (833) resumed previous work and recreation-al activities and 3 patients (167) returned to restrictedemployment
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 1010
Part IX Ligament InstabilityTears568
REFERENCES
1 Palmer AK riangular fibrocartilage complex lesions a classification J HandSurg [Am] 198914594ndash606
2 Nakamura Yabe Y Horiuchi Y Functional anatomy of the triangularfibrocartilage complex J Hand Surg [Br] 199621581ndash586
3 Palmer AK Werner F W Te triangular fibrocartilage complex of the wristmdashanatomy and function J Hand Surg [Am] 19816153ndash162
4 Adams BD Holly K A Strains in the articular disk of the triangular fibro-cartilage complex a biomechanical study J Hand Surg [Am] 199318919ndash925
5 Benjamin M Evans E J Pemberton D J Histological studies on the triangularfibrocartilage complex of the wrist J Anat 199017259ndash67
6 Kauer JMG Te distal radioulnar joint anatomic and functional consider-ations Clin Orthop 199227537ndash45
7 Atzei A Luchetti R Garcia-Elias M Lesioni capsulo-legamentose dellaradio-ulnare distale e fibrocartilagine triangolare In Landi A Catalano FLuchetti R (eds) rattato di Chirurgia della Mano Verduci Editore Roma2006 pp 159ndash187
8 Kleinman WB Stability of the distal radioulnar joint biomechanics patho-physiology physical diagnosis and restoration of function What we havelearned in 25 years J Hand Surg [Am] 2007321087ndash1106
9 Garcia-Elias M Smith DE Llusa M Surgical approach to the triangularfibrocartilage complex ech Hand Up Extrem Surg 20037(4)134ndash140
10 Nakamura Nakao Y Ikegami H et al Open repair of the ulnar disruptionof the triangular fibrocartilage complex with double three-dimensional mat-tress suturing technique ech Hand Up Extrem Surg 20048(2)116ndash123
11 Hermansdorfer JD Kleinman WB Management of chronic peripheraltears of the triangular fibrocartilage complex J Hand Surg [Am] 199116340ndash346
12 Chou KH Sarris IK Sotereanos DG Suture anchor repair of ulnar-sidedtriangular fibrocartilage complex tears J Hand Surg [Br] 200328546ndash550
13 Slutsky D J Clinical applications of volar portals in wrist arthroscopy echHand Up Extrem Surg 20048(4)229ndash238
14 omaino M Weiser R Combined arthroscopic FCC debridement and wa-fer resection of the distal ulna in wrists with triangular fibrocartilage complextears and positive ulnar variance J Hand Surg [Am] 2001261047ndash1052
15 Hanker G J Management of ulnar impaction syndrome In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 63ndash71
16 Moskal M J Savoie FH III Management of lunotriquetral instability InGeissler WB (ed) Wrist Arthroscopy New York Springer-Verlag 2005pp 94ndash101
17 Atzei A Luchetti R Clinical approach to the painful wrist In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 185ndash195
18 ay SC omita K Berger R A Te ldquoulnar fovea signrdquo for defining ulnar wrist pain an analysis of sensitivity and specificity J Hand Surg [Am]200732(4)438ndash444
19 Zanetti M Bram J Hodler J riangular fibrocartilage and intercarpal liga-ments of the wrist does MR arthrography improve standard MRI J Magn
Reson Imaging 19977 (3)590ndash59420 Pederzini L Luchetti R Soragni O et al Evaluation of the triangular
fibrocartilage complex tears by arthroscopy arthrography and magnetic reso-nance imaging Arthroscopy 19928191ndash197
21 Fulcher S Poehling G Te role of operative arthroscopy for the diag-nosis and treatment of lesions about the distal ulna Hand Clin 199814285ndash296
22 Atzei A New trends in arthroscopic management of type 1-B FCC injuries with DRUJ instability J Hand Surg [Eur] 2009Epub ahead of print
23 Atzei A Rizzo A Luchetti R Fairplay Arthroscopic foveal repair of tri-angular fibrocartilage complex peripheral lesion with distal radioulnar jointinstability ech Hand Up Extrem Surg 200812226ndash235
24 Adams BD Anatomic reconstruction of the distal radioulnar ligaments forDRUJ instability ech Hand Up Extrem Surg 20004154ndash160
25 Atzei A Luchetti R Borelli PP et al Arthroscopic FCC reconstruction bytendon graft Riv Chir Mano 200643(3)370ndash376
26 Atzei A Luchetti R Sgarbossa A et al Set-up portals and normal explora-tion in wrist arthroscopy Chir Main 200625S131ndashS144
27 del Pintildeal F Garciacutea-Bernal F J Pisani D et al Dry arthroscopy of the wrist
surgical technique J Hand Surg [Am] 200732119ndash12328 del Pintildeal F Garciacutea-Bernal F J Delgado J et al Correction of malunited
intra-articular distal radius fractures with an inside-out osteotomy technique J Hand Surg [Am] 200531(6)1029ndash1034
29 Slutsky D J Distal radioulnar joint arthroscopy and the volar ulnar portalech Hand Up Extrem Surg 200711(1)38ndash44
30 Lo IK Y Burkhart SS Double-row arthroscopic rotator cuff repair re-establishing the footprint of the rotator cuff Arthroscopy 200319(9)1035ndash1042
31 Luchetti R Atzei A Rocchi L Incidence and causes of failures in wristarthroscopic techniques Chir Main 200625(1)48ndash53
FIGURE 54-10 At the end of the procedure the knots of bothsutures are located at the level of the 6U portal just
outside the distal radioulnar joint capsule or in the prestyloid recess(From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)

8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 710
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-5 Screwanchor drilling and insertion are performed as a mini-open procedure through the direct foveal portal (From Atzei ARizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar
joint instability Tech Hand Up Extrem Surg 200812226ndash235)
A B
FIGURE 54-4 The direct foveal (DF) portal is located about 1 cm proximal to the 6U portal It has been devised as a working portal toprovide access to the area of the ulnar styloid and fovea With the scope in the distal radioulnar joint portal a curet
or small shaver is inserted through the DF portal to refresh the tornavulsed ligament and the fovea (From Atzei A Rizzo A Luchetti R Fairplay TArthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up ExtremSurg 200812226ndash235)
6-U
DF
A B
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 810
Part IX Ligament InstabilityTears566
FIGURE 54-6 Once the screw is in place sutures should exit the direct foveal portal from underneath the triangular 1047297brocartilage complex(TFCC) When the wrist is placed back in neutral pronosupination the screwrsquos head is brought under the TFCC (From Atzei A
Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability TechHand Up Extrem Surg 200812226ndash235)
Te technique of arthroscopic-assisted palmar repair of the fo-veal insertion of the FCC has a learning curve However once
the technique is mastered the rate of complications for this pro-cedure is comparable to that of larger series of common wristarthroscopic procedures31
RESULTS
Te authorsrsquo clinical experience started in 2001 and up until now we have operated on 37 FCC tears (29 type 2 FCC peripheraltears and 8 type 3 tears)
In a control series study 18 patients (13 males and5 females with a mean age of 342) were investigated prospec-
tively for a minimum follow-up of 1 year (average 18 monthsmaximum 37 months) All patients had a history of traumacomplained of pain in the ulnar fovea and had clinical signsof DRUJ instability ranging from mild (10 patients) to mod-erate (8 patients) Although radiographs showed a positive ul-nar variance in three patients there were no detectable signsof ulnocarpal impaction or carpal degenerative chondropa-thy Arthroscopy revealed a Palmer type 1B ulnar avulsionof the FCC in all patients Fourteen cases were classified as
FIGURE 54-7 With the scope in the 3-4 portal the 1047297rst suture end is inserted into the tip of a 25-gauge needle (preferably a Tuohy needle) The needle is passed through the triangular 1047297brocartilage complex (TFCC) in an outside-in fashion via the direct foveal portal
toward the palmar contour of the TFCC (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complexperipheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 910
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-8 A grasper is inserted through the 6U portal and used to retrieve the suture (From Atzei A Rizzo A Luchetti R Fairplay T Arthro-scopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up
Extrem Surg 200812226ndash235)
FIGURE 54-9 The suture is tied under arthroscopic control using a small knot-pusher The pc-TFCC (proximal component of the triangular1047297brocartilage complex) is pushed forcefully against the distal ulna provided that the wrist traction is released the forearm is
held in neutral rotation and the ulnar head is reduced by the assistant (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
complete FCC peripheral tears (type 2) and four as proximaltears (type 3)
At fol low-up evaluation the patients showed an increasedrange of motion (from 907 to 96 of the contralateralside) and grip strength (from 73 to 90) Pain decreasedfrom 83 to 12 on a 10-point visual analogue scale Gripstrength and pain changes reached statistical significance
(P lt 005) he Modified Mayo Wrist Score was excellentin 14 patients good in 3 and fair in 1 A total of 944 ofthe results scored excellent and good DASH (disabilities ofthe arm shoulder and hand) score averaged 105 Fifteenpatients (833) resumed previous work and recreation-al activities and 3 patients (167) returned to restrictedemployment
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 1010
Part IX Ligament InstabilityTears568
REFERENCES
1 Palmer AK riangular fibrocartilage complex lesions a classification J HandSurg [Am] 198914594ndash606
2 Nakamura Yabe Y Horiuchi Y Functional anatomy of the triangularfibrocartilage complex J Hand Surg [Br] 199621581ndash586
3 Palmer AK Werner F W Te triangular fibrocartilage complex of the wristmdashanatomy and function J Hand Surg [Am] 19816153ndash162
4 Adams BD Holly K A Strains in the articular disk of the triangular fibro-cartilage complex a biomechanical study J Hand Surg [Am] 199318919ndash925
5 Benjamin M Evans E J Pemberton D J Histological studies on the triangularfibrocartilage complex of the wrist J Anat 199017259ndash67
6 Kauer JMG Te distal radioulnar joint anatomic and functional consider-ations Clin Orthop 199227537ndash45
7 Atzei A Luchetti R Garcia-Elias M Lesioni capsulo-legamentose dellaradio-ulnare distale e fibrocartilagine triangolare In Landi A Catalano FLuchetti R (eds) rattato di Chirurgia della Mano Verduci Editore Roma2006 pp 159ndash187
8 Kleinman WB Stability of the distal radioulnar joint biomechanics patho-physiology physical diagnosis and restoration of function What we havelearned in 25 years J Hand Surg [Am] 2007321087ndash1106
9 Garcia-Elias M Smith DE Llusa M Surgical approach to the triangularfibrocartilage complex ech Hand Up Extrem Surg 20037(4)134ndash140
10 Nakamura Nakao Y Ikegami H et al Open repair of the ulnar disruptionof the triangular fibrocartilage complex with double three-dimensional mat-tress suturing technique ech Hand Up Extrem Surg 20048(2)116ndash123
11 Hermansdorfer JD Kleinman WB Management of chronic peripheraltears of the triangular fibrocartilage complex J Hand Surg [Am] 199116340ndash346
12 Chou KH Sarris IK Sotereanos DG Suture anchor repair of ulnar-sidedtriangular fibrocartilage complex tears J Hand Surg [Br] 200328546ndash550
13 Slutsky D J Clinical applications of volar portals in wrist arthroscopy echHand Up Extrem Surg 20048(4)229ndash238
14 omaino M Weiser R Combined arthroscopic FCC debridement and wa-fer resection of the distal ulna in wrists with triangular fibrocartilage complextears and positive ulnar variance J Hand Surg [Am] 2001261047ndash1052
15 Hanker G J Management of ulnar impaction syndrome In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 63ndash71
16 Moskal M J Savoie FH III Management of lunotriquetral instability InGeissler WB (ed) Wrist Arthroscopy New York Springer-Verlag 2005pp 94ndash101
17 Atzei A Luchetti R Clinical approach to the painful wrist In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 185ndash195
18 ay SC omita K Berger R A Te ldquoulnar fovea signrdquo for defining ulnar wrist pain an analysis of sensitivity and specificity J Hand Surg [Am]200732(4)438ndash444
19 Zanetti M Bram J Hodler J riangular fibrocartilage and intercarpal liga-ments of the wrist does MR arthrography improve standard MRI J Magn
Reson Imaging 19977 (3)590ndash59420 Pederzini L Luchetti R Soragni O et al Evaluation of the triangular
fibrocartilage complex tears by arthroscopy arthrography and magnetic reso-nance imaging Arthroscopy 19928191ndash197
21 Fulcher S Poehling G Te role of operative arthroscopy for the diag-nosis and treatment of lesions about the distal ulna Hand Clin 199814285ndash296
22 Atzei A New trends in arthroscopic management of type 1-B FCC injuries with DRUJ instability J Hand Surg [Eur] 2009Epub ahead of print
23 Atzei A Rizzo A Luchetti R Fairplay Arthroscopic foveal repair of tri-angular fibrocartilage complex peripheral lesion with distal radioulnar jointinstability ech Hand Up Extrem Surg 200812226ndash235
24 Adams BD Anatomic reconstruction of the distal radioulnar ligaments forDRUJ instability ech Hand Up Extrem Surg 20004154ndash160
25 Atzei A Luchetti R Borelli PP et al Arthroscopic FCC reconstruction bytendon graft Riv Chir Mano 200643(3)370ndash376
26 Atzei A Luchetti R Sgarbossa A et al Set-up portals and normal explora-tion in wrist arthroscopy Chir Main 200625S131ndashS144
27 del Pintildeal F Garciacutea-Bernal F J Pisani D et al Dry arthroscopy of the wrist
surgical technique J Hand Surg [Am] 200732119ndash12328 del Pintildeal F Garciacutea-Bernal F J Delgado J et al Correction of malunited
intra-articular distal radius fractures with an inside-out osteotomy technique J Hand Surg [Am] 200531(6)1029ndash1034
29 Slutsky D J Distal radioulnar joint arthroscopy and the volar ulnar portalech Hand Up Extrem Surg 200711(1)38ndash44
30 Lo IK Y Burkhart SS Double-row arthroscopic rotator cuff repair re-establishing the footprint of the rotator cuff Arthroscopy 200319(9)1035ndash1042
31 Luchetti R Atzei A Rocchi L Incidence and causes of failures in wristarthroscopic techniques Chir Main 200625(1)48ndash53
FIGURE 54-10 At the end of the procedure the knots of bothsutures are located at the level of the 6U portal just
outside the distal radioulnar joint capsule or in the prestyloid recess(From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)

8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 810
Part IX Ligament InstabilityTears566
FIGURE 54-6 Once the screw is in place sutures should exit the direct foveal portal from underneath the triangular 1047297brocartilage complex(TFCC) When the wrist is placed back in neutral pronosupination the screwrsquos head is brought under the TFCC (From Atzei A
Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability TechHand Up Extrem Surg 200812226ndash235)
Te technique of arthroscopic-assisted palmar repair of the fo-veal insertion of the FCC has a learning curve However once
the technique is mastered the rate of complications for this pro-cedure is comparable to that of larger series of common wristarthroscopic procedures31
RESULTS
Te authorsrsquo clinical experience started in 2001 and up until now we have operated on 37 FCC tears (29 type 2 FCC peripheraltears and 8 type 3 tears)
In a control series study 18 patients (13 males and5 females with a mean age of 342) were investigated prospec-
tively for a minimum follow-up of 1 year (average 18 monthsmaximum 37 months) All patients had a history of traumacomplained of pain in the ulnar fovea and had clinical signsof DRUJ instability ranging from mild (10 patients) to mod-erate (8 patients) Although radiographs showed a positive ul-nar variance in three patients there were no detectable signsof ulnocarpal impaction or carpal degenerative chondropa-thy Arthroscopy revealed a Palmer type 1B ulnar avulsionof the FCC in all patients Fourteen cases were classified as
FIGURE 54-7 With the scope in the 3-4 portal the 1047297rst suture end is inserted into the tip of a 25-gauge needle (preferably a Tuohy needle) The needle is passed through the triangular 1047297brocartilage complex (TFCC) in an outside-in fashion via the direct foveal portal
toward the palmar contour of the TFCC (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair of triangular 1047297brocartilage complexperipheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 910
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-8 A grasper is inserted through the 6U portal and used to retrieve the suture (From Atzei A Rizzo A Luchetti R Fairplay T Arthro-scopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up
Extrem Surg 200812226ndash235)
FIGURE 54-9 The suture is tied under arthroscopic control using a small knot-pusher The pc-TFCC (proximal component of the triangular1047297brocartilage complex) is pushed forcefully against the distal ulna provided that the wrist traction is released the forearm is
held in neutral rotation and the ulnar head is reduced by the assistant (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
complete FCC peripheral tears (type 2) and four as proximaltears (type 3)
At fol low-up evaluation the patients showed an increasedrange of motion (from 907 to 96 of the contralateralside) and grip strength (from 73 to 90) Pain decreasedfrom 83 to 12 on a 10-point visual analogue scale Gripstrength and pain changes reached statistical significance
(P lt 005) he Modified Mayo Wrist Score was excellentin 14 patients good in 3 and fair in 1 A total of 944 ofthe results scored excellent and good DASH (disabilities ofthe arm shoulder and hand) score averaged 105 Fifteenpatients (833) resumed previous work and recreation-al activities and 3 patients (167) returned to restrictedemployment
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 1010
Part IX Ligament InstabilityTears568
REFERENCES
1 Palmer AK riangular fibrocartilage complex lesions a classification J HandSurg [Am] 198914594ndash606
2 Nakamura Yabe Y Horiuchi Y Functional anatomy of the triangularfibrocartilage complex J Hand Surg [Br] 199621581ndash586
3 Palmer AK Werner F W Te triangular fibrocartilage complex of the wristmdashanatomy and function J Hand Surg [Am] 19816153ndash162
4 Adams BD Holly K A Strains in the articular disk of the triangular fibro-cartilage complex a biomechanical study J Hand Surg [Am] 199318919ndash925
5 Benjamin M Evans E J Pemberton D J Histological studies on the triangularfibrocartilage complex of the wrist J Anat 199017259ndash67
6 Kauer JMG Te distal radioulnar joint anatomic and functional consider-ations Clin Orthop 199227537ndash45
7 Atzei A Luchetti R Garcia-Elias M Lesioni capsulo-legamentose dellaradio-ulnare distale e fibrocartilagine triangolare In Landi A Catalano FLuchetti R (eds) rattato di Chirurgia della Mano Verduci Editore Roma2006 pp 159ndash187
8 Kleinman WB Stability of the distal radioulnar joint biomechanics patho-physiology physical diagnosis and restoration of function What we havelearned in 25 years J Hand Surg [Am] 2007321087ndash1106
9 Garcia-Elias M Smith DE Llusa M Surgical approach to the triangularfibrocartilage complex ech Hand Up Extrem Surg 20037(4)134ndash140
10 Nakamura Nakao Y Ikegami H et al Open repair of the ulnar disruptionof the triangular fibrocartilage complex with double three-dimensional mat-tress suturing technique ech Hand Up Extrem Surg 20048(2)116ndash123
11 Hermansdorfer JD Kleinman WB Management of chronic peripheraltears of the triangular fibrocartilage complex J Hand Surg [Am] 199116340ndash346
12 Chou KH Sarris IK Sotereanos DG Suture anchor repair of ulnar-sidedtriangular fibrocartilage complex tears J Hand Surg [Br] 200328546ndash550
13 Slutsky D J Clinical applications of volar portals in wrist arthroscopy echHand Up Extrem Surg 20048(4)229ndash238
14 omaino M Weiser R Combined arthroscopic FCC debridement and wa-fer resection of the distal ulna in wrists with triangular fibrocartilage complextears and positive ulnar variance J Hand Surg [Am] 2001261047ndash1052
15 Hanker G J Management of ulnar impaction syndrome In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 63ndash71
16 Moskal M J Savoie FH III Management of lunotriquetral instability InGeissler WB (ed) Wrist Arthroscopy New York Springer-Verlag 2005pp 94ndash101
17 Atzei A Luchetti R Clinical approach to the painful wrist In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 185ndash195
18 ay SC omita K Berger R A Te ldquoulnar fovea signrdquo for defining ulnar wrist pain an analysis of sensitivity and specificity J Hand Surg [Am]200732(4)438ndash444
19 Zanetti M Bram J Hodler J riangular fibrocartilage and intercarpal liga-ments of the wrist does MR arthrography improve standard MRI J Magn
Reson Imaging 19977 (3)590ndash59420 Pederzini L Luchetti R Soragni O et al Evaluation of the triangular
fibrocartilage complex tears by arthroscopy arthrography and magnetic reso-nance imaging Arthroscopy 19928191ndash197
21 Fulcher S Poehling G Te role of operative arthroscopy for the diag-nosis and treatment of lesions about the distal ulna Hand Clin 199814285ndash296
22 Atzei A New trends in arthroscopic management of type 1-B FCC injuries with DRUJ instability J Hand Surg [Eur] 2009Epub ahead of print
23 Atzei A Rizzo A Luchetti R Fairplay Arthroscopic foveal repair of tri-angular fibrocartilage complex peripheral lesion with distal radioulnar jointinstability ech Hand Up Extrem Surg 200812226ndash235
24 Adams BD Anatomic reconstruction of the distal radioulnar ligaments forDRUJ instability ech Hand Up Extrem Surg 20004154ndash160
25 Atzei A Luchetti R Borelli PP et al Arthroscopic FCC reconstruction bytendon graft Riv Chir Mano 200643(3)370ndash376
26 Atzei A Luchetti R Sgarbossa A et al Set-up portals and normal explora-tion in wrist arthroscopy Chir Main 200625S131ndashS144
27 del Pintildeal F Garciacutea-Bernal F J Pisani D et al Dry arthroscopy of the wrist
surgical technique J Hand Surg [Am] 200732119ndash12328 del Pintildeal F Garciacutea-Bernal F J Delgado J et al Correction of malunited
intra-articular distal radius fractures with an inside-out osteotomy technique J Hand Surg [Am] 200531(6)1029ndash1034
29 Slutsky D J Distal radioulnar joint arthroscopy and the volar ulnar portalech Hand Up Extrem Surg 200711(1)38ndash44
30 Lo IK Y Burkhart SS Double-row arthroscopic rotator cuff repair re-establishing the footprint of the rotator cuff Arthroscopy 200319(9)1035ndash1042
31 Luchetti R Atzei A Rocchi L Incidence and causes of failures in wristarthroscopic techniques Chir Main 200625(1)48ndash53
FIGURE 54-10 At the end of the procedure the knots of bothsutures are located at the level of the 6U portal just
outside the distal radioulnar joint capsule or in the prestyloid recess(From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)

8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 910
CHAPTER 54 Repair of the Foveal Insertion of the TFCC Through the DF Portal 5
FIGURE 54-8 A grasper is inserted through the 6U portal and used to retrieve the suture (From Atzei A Rizzo A Luchetti R Fairplay T Arthro-scopic foveal repair of triangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up
Extrem Surg 200812226ndash235)
FIGURE 54-9 The suture is tied under arthroscopic control using a small knot-pusher The pc-TFCC (proximal component of the triangular1047297brocartilage complex) is pushed forcefully against the distal ulna provided that the wrist traction is released the forearm is
held in neutral rotation and the ulnar head is reduced by the assistant (From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)
complete FCC peripheral tears (type 2) and four as proximaltears (type 3)
At fol low-up evaluation the patients showed an increasedrange of motion (from 907 to 96 of the contralateralside) and grip strength (from 73 to 90) Pain decreasedfrom 83 to 12 on a 10-point visual analogue scale Gripstrength and pain changes reached statistical significance
(P lt 005) he Modified Mayo Wrist Score was excellentin 14 patients good in 3 and fair in 1 A total of 944 ofthe results scored excellent and good DASH (disabilities ofthe arm shoulder and hand) score averaged 105 Fifteenpatients (833) resumed previous work and recreation-al activities and 3 patients (167) returned to restrictedemployment
8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 1010
Part IX Ligament InstabilityTears568
REFERENCES
1 Palmer AK riangular fibrocartilage complex lesions a classification J HandSurg [Am] 198914594ndash606
2 Nakamura Yabe Y Horiuchi Y Functional anatomy of the triangularfibrocartilage complex J Hand Surg [Br] 199621581ndash586
3 Palmer AK Werner F W Te triangular fibrocartilage complex of the wristmdashanatomy and function J Hand Surg [Am] 19816153ndash162
4 Adams BD Holly K A Strains in the articular disk of the triangular fibro-cartilage complex a biomechanical study J Hand Surg [Am] 199318919ndash925
5 Benjamin M Evans E J Pemberton D J Histological studies on the triangularfibrocartilage complex of the wrist J Anat 199017259ndash67
6 Kauer JMG Te distal radioulnar joint anatomic and functional consider-ations Clin Orthop 199227537ndash45
7 Atzei A Luchetti R Garcia-Elias M Lesioni capsulo-legamentose dellaradio-ulnare distale e fibrocartilagine triangolare In Landi A Catalano FLuchetti R (eds) rattato di Chirurgia della Mano Verduci Editore Roma2006 pp 159ndash187
8 Kleinman WB Stability of the distal radioulnar joint biomechanics patho-physiology physical diagnosis and restoration of function What we havelearned in 25 years J Hand Surg [Am] 2007321087ndash1106
9 Garcia-Elias M Smith DE Llusa M Surgical approach to the triangularfibrocartilage complex ech Hand Up Extrem Surg 20037(4)134ndash140
10 Nakamura Nakao Y Ikegami H et al Open repair of the ulnar disruptionof the triangular fibrocartilage complex with double three-dimensional mat-tress suturing technique ech Hand Up Extrem Surg 20048(2)116ndash123
11 Hermansdorfer JD Kleinman WB Management of chronic peripheraltears of the triangular fibrocartilage complex J Hand Surg [Am] 199116340ndash346
12 Chou KH Sarris IK Sotereanos DG Suture anchor repair of ulnar-sidedtriangular fibrocartilage complex tears J Hand Surg [Br] 200328546ndash550
13 Slutsky D J Clinical applications of volar portals in wrist arthroscopy echHand Up Extrem Surg 20048(4)229ndash238
14 omaino M Weiser R Combined arthroscopic FCC debridement and wa-fer resection of the distal ulna in wrists with triangular fibrocartilage complextears and positive ulnar variance J Hand Surg [Am] 2001261047ndash1052
15 Hanker G J Management of ulnar impaction syndrome In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 63ndash71
16 Moskal M J Savoie FH III Management of lunotriquetral instability InGeissler WB (ed) Wrist Arthroscopy New York Springer-Verlag 2005pp 94ndash101
17 Atzei A Luchetti R Clinical approach to the painful wrist In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 185ndash195
18 ay SC omita K Berger R A Te ldquoulnar fovea signrdquo for defining ulnar wrist pain an analysis of sensitivity and specificity J Hand Surg [Am]200732(4)438ndash444
19 Zanetti M Bram J Hodler J riangular fibrocartilage and intercarpal liga-ments of the wrist does MR arthrography improve standard MRI J Magn
Reson Imaging 19977 (3)590ndash59420 Pederzini L Luchetti R Soragni O et al Evaluation of the triangular
fibrocartilage complex tears by arthroscopy arthrography and magnetic reso-nance imaging Arthroscopy 19928191ndash197
21 Fulcher S Poehling G Te role of operative arthroscopy for the diag-nosis and treatment of lesions about the distal ulna Hand Clin 199814285ndash296
22 Atzei A New trends in arthroscopic management of type 1-B FCC injuries with DRUJ instability J Hand Surg [Eur] 2009Epub ahead of print
23 Atzei A Rizzo A Luchetti R Fairplay Arthroscopic foveal repair of tri-angular fibrocartilage complex peripheral lesion with distal radioulnar jointinstability ech Hand Up Extrem Surg 200812226ndash235
24 Adams BD Anatomic reconstruction of the distal radioulnar ligaments forDRUJ instability ech Hand Up Extrem Surg 20004154ndash160
25 Atzei A Luchetti R Borelli PP et al Arthroscopic FCC reconstruction bytendon graft Riv Chir Mano 200643(3)370ndash376
26 Atzei A Luchetti R Sgarbossa A et al Set-up portals and normal explora-tion in wrist arthroscopy Chir Main 200625S131ndashS144
27 del Pintildeal F Garciacutea-Bernal F J Pisani D et al Dry arthroscopy of the wrist
surgical technique J Hand Surg [Am] 200732119ndash12328 del Pintildeal F Garciacutea-Bernal F J Delgado J et al Correction of malunited
intra-articular distal radius fractures with an inside-out osteotomy technique J Hand Surg [Am] 200531(6)1029ndash1034
29 Slutsky D J Distal radioulnar joint arthroscopy and the volar ulnar portalech Hand Up Extrem Surg 200711(1)38ndash44
30 Lo IK Y Burkhart SS Double-row arthroscopic rotator cuff repair re-establishing the footprint of the rotator cuff Arthroscopy 200319(9)1035ndash1042
31 Luchetti R Atzei A Rocchi L Incidence and causes of failures in wristarthroscopic techniques Chir Main 200625(1)48ndash53
FIGURE 54-10 At the end of the procedure the knots of bothsutures are located at the level of the 6U portal just
outside the distal radioulnar joint capsule or in the prestyloid recess(From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)

8122019 09 Tfcc Repair Direct Foveal Portal
httpslidepdfcomreaderfull09-tfcc-repair-direct-foveal-portal 1010
Part IX Ligament InstabilityTears568
REFERENCES
1 Palmer AK riangular fibrocartilage complex lesions a classification J HandSurg [Am] 198914594ndash606
2 Nakamura Yabe Y Horiuchi Y Functional anatomy of the triangularfibrocartilage complex J Hand Surg [Br] 199621581ndash586
3 Palmer AK Werner F W Te triangular fibrocartilage complex of the wristmdashanatomy and function J Hand Surg [Am] 19816153ndash162
4 Adams BD Holly K A Strains in the articular disk of the triangular fibro-cartilage complex a biomechanical study J Hand Surg [Am] 199318919ndash925
5 Benjamin M Evans E J Pemberton D J Histological studies on the triangularfibrocartilage complex of the wrist J Anat 199017259ndash67
6 Kauer JMG Te distal radioulnar joint anatomic and functional consider-ations Clin Orthop 199227537ndash45
7 Atzei A Luchetti R Garcia-Elias M Lesioni capsulo-legamentose dellaradio-ulnare distale e fibrocartilagine triangolare In Landi A Catalano FLuchetti R (eds) rattato di Chirurgia della Mano Verduci Editore Roma2006 pp 159ndash187
8 Kleinman WB Stability of the distal radioulnar joint biomechanics patho-physiology physical diagnosis and restoration of function What we havelearned in 25 years J Hand Surg [Am] 2007321087ndash1106
9 Garcia-Elias M Smith DE Llusa M Surgical approach to the triangularfibrocartilage complex ech Hand Up Extrem Surg 20037(4)134ndash140
10 Nakamura Nakao Y Ikegami H et al Open repair of the ulnar disruptionof the triangular fibrocartilage complex with double three-dimensional mat-tress suturing technique ech Hand Up Extrem Surg 20048(2)116ndash123
11 Hermansdorfer JD Kleinman WB Management of chronic peripheraltears of the triangular fibrocartilage complex J Hand Surg [Am] 199116340ndash346
12 Chou KH Sarris IK Sotereanos DG Suture anchor repair of ulnar-sidedtriangular fibrocartilage complex tears J Hand Surg [Br] 200328546ndash550
13 Slutsky D J Clinical applications of volar portals in wrist arthroscopy echHand Up Extrem Surg 20048(4)229ndash238
14 omaino M Weiser R Combined arthroscopic FCC debridement and wa-fer resection of the distal ulna in wrists with triangular fibrocartilage complextears and positive ulnar variance J Hand Surg [Am] 2001261047ndash1052
15 Hanker G J Management of ulnar impaction syndrome In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 63ndash71
16 Moskal M J Savoie FH III Management of lunotriquetral instability InGeissler WB (ed) Wrist Arthroscopy New York Springer-Verlag 2005pp 94ndash101
17 Atzei A Luchetti R Clinical approach to the painful wrist In Geissler WB(ed) Wrist Arthroscopy New York Springer-Verlag 2005 pp 185ndash195
18 ay SC omita K Berger R A Te ldquoulnar fovea signrdquo for defining ulnar wrist pain an analysis of sensitivity and specificity J Hand Surg [Am]200732(4)438ndash444
19 Zanetti M Bram J Hodler J riangular fibrocartilage and intercarpal liga-ments of the wrist does MR arthrography improve standard MRI J Magn
Reson Imaging 19977 (3)590ndash59420 Pederzini L Luchetti R Soragni O et al Evaluation of the triangular
fibrocartilage complex tears by arthroscopy arthrography and magnetic reso-nance imaging Arthroscopy 19928191ndash197
21 Fulcher S Poehling G Te role of operative arthroscopy for the diag-nosis and treatment of lesions about the distal ulna Hand Clin 199814285ndash296
22 Atzei A New trends in arthroscopic management of type 1-B FCC injuries with DRUJ instability J Hand Surg [Eur] 2009Epub ahead of print
23 Atzei A Rizzo A Luchetti R Fairplay Arthroscopic foveal repair of tri-angular fibrocartilage complex peripheral lesion with distal radioulnar jointinstability ech Hand Up Extrem Surg 200812226ndash235
24 Adams BD Anatomic reconstruction of the distal radioulnar ligaments forDRUJ instability ech Hand Up Extrem Surg 20004154ndash160
25 Atzei A Luchetti R Borelli PP et al Arthroscopic FCC reconstruction bytendon graft Riv Chir Mano 200643(3)370ndash376
26 Atzei A Luchetti R Sgarbossa A et al Set-up portals and normal explora-tion in wrist arthroscopy Chir Main 200625S131ndashS144
27 del Pintildeal F Garciacutea-Bernal F J Pisani D et al Dry arthroscopy of the wrist
surgical technique J Hand Surg [Am] 200732119ndash12328 del Pintildeal F Garciacutea-Bernal F J Delgado J et al Correction of malunited
intra-articular distal radius fractures with an inside-out osteotomy technique J Hand Surg [Am] 200531(6)1029ndash1034
29 Slutsky D J Distal radioulnar joint arthroscopy and the volar ulnar portalech Hand Up Extrem Surg 200711(1)38ndash44
30 Lo IK Y Burkhart SS Double-row arthroscopic rotator cuff repair re-establishing the footprint of the rotator cuff Arthroscopy 200319(9)1035ndash1042
31 Luchetti R Atzei A Rocchi L Incidence and causes of failures in wristarthroscopic techniques Chir Main 200625(1)48ndash53
FIGURE 54-10 At the end of the procedure the knots of bothsutures are located at the level of the 6U portal just
outside the distal radioulnar joint capsule or in the prestyloid recess(From Atzei A Rizzo A Luchetti R Fairplay T Arthroscopic foveal repair oftriangular 1047297brocartilage complex peripheral lesion with distal radioulnar joint instability Tech Hand Up Extrem Surg 200812226ndash235)