Embed Size (px)
Citation preview

CNS Infections
February 20, 2008
George P. Allen, Pharm.D.Assistant Professor, Pharmacy PracticeOSU College of Pharmacy at OHSU

Introduction
• Meningitis: inflammation of the meninges– protective membranes covering the CNS
• Encephalitis: inflammation of the brain– usually viral

Epidemiology
• Incidence: 4-6 / 100,000 / year in U.S.• Mortality ~ 3-33%
– overall mortality remains high (~25%) despite advances in therapy
• Neurologic sequelae are frequent (~61% in Gram -)– seizures– hearing loss– hydrocephalus

Epidemiologic Considerations
• Significant changes in the distribution of causative organisms have occurred
• Rates of infection by specific pathogens are most influenced by patient age
• Morbidity and mortality are influenced by organism, patient age
• Increases in nosocomial CNS infections• Increases in antimicrobial resistance

Predisposing Factors
• Recent respiratory tract infection• Otitis media• Sinusitis• Mastoiditis• Immunosuppression• Splenectomy• Sickle cell disease

Pathophysiology
• Nasopharyngeal colonization• Passage into bloodstream• Bacteria invade subarachnoid space• Subarachnoid defenses limited• Infection and inflammation result

Clinical Considerations
• Age• Time of year• Previous antibiotic therapy • Laboratory analysis

Clinical Presentation: Adults
• Early signs:– photophobia– headache– neck stiffness (nuchal rigidity)
• Late signs:– seizures– focal neurologic deficits– hydrocephalus

Clinical Presentation: Infants
• Non-specific signs and symptoms are common– irritability– altered sleep– vomiting– high-pitched crying– diminished oral intake– seizures

Clinical Presentation: Children
• Decreased activity• Somnolence• Confusion• Lethargy

Diagnosis

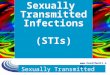
Kernig’s Sign
Saberi A et al. Hosp Phys 1999:23-4.

Brudzinski’s Sign
Saberi A et al. Hosp Phys 1999:23-4.

Accuracy of Clinical Signs
95%5%Kernig’s sign
95%5%Brudzinski’s sign
68%30%Nuchal rigidity
SpecificitySensitivityClinical Sign
Thomas KE et al. Clin Infect Dis 2000;35:46-52.

Lumbar Puncture
• 4 tubes collected• Appropriate technique important (contamination,
traumatic LP)

CSF Analysis
• 4 tubes: chemistry, hematology, microbiology, latex agglutination testing
• Normal CSF:– clear– sterile– protein < 50 mg/dL– glucose 50 - 66% serum value– WBC < 10 (all mononuclear)

Typical CSF Findings
< 30-70 mg/dL< 30-70 mg/dL< 1/2 serum1/2-2/3 serumGlucose
≥ 40-15030-15080-500< 50Protein (mg/dL)
> 80% L50% L> 90% PMN> 90% MWBC differential
100-10005-500400-100,000< 10WBC (#/mL)
TubercularViralBacterialNormalComponent

CSF Analysis: Microbiology
• Gram’s stain – 60-90% confirmatory before ABX– 40-60% confirmatory after ABX
• Cultures– CSF– blood

Other CSF Evaluations
• Opening pressure• Latex agglutination • Limulus lysate assay• Polymerase chain reaction (PCR)• Lactate• C-reactive protein• Procalcitonin

Treatment

Causative Bacteria: Children
Newborns (less than 1 month old):
• group B streptococcus (Streptococcus agalactiae)• Escherichia coli• Listeria monocytogenes• Klebsiella spp.

Causative Bacteria: Children, Adults
1 month - ~ 50 years old:
• Streptococcus pneumoniae• Neisseria meningitidis• Haemophilus influenzae• L. monocytogenes• Group B streptococci

Causative Bacteria: Elderly
>50 yrs old:
• Streptococcus pneumoniae• Listeria monocytogenes• Gram - enteric bacilli • P. aeruginosa (less common)• Neisseria meningitidis (rare)

CNS Anatomy
• Cerebrospinal fluid (CSF)– 0.5 mL/min produced – unidirectional flow

Blood-Brain Barrier (BBB)

Blood-Brain Barrier
• Excluded:– proteins, polar molecules
• Move freely:– water, most ions, lipids
• Transported:– amino acids, glucose

Management Principles
• Prompt empiric coverage• Do not delay therapy for lumbar puncture• Base antibacterial coverage on:
– age– risk factors– allergies

Therapy Considerations
• Bactericidal activity in CSF– impaired host defenses– bacteriostatic therapy = poor outcome
• CSF concentration 10-20 x MBC desirable– decreased activity in infected CSF– lower pH– higher protein concentrations

• Consider penetration in both presence and absence of inflammation
• Antimicrobial characteristics favoring penetration:– small molecular weight– high lipophilicity– low ionization – low protein binding
CSF Penetration

Penetration of Selected ABX
fluoroquinolonesrifampin
aztreonamisoniazid
clindamycincarbapenemsmetronidazole
1st gen. cephalosporinsvancomycinchloramphenicol
2nd gen. cephalosporins3rd gen. cephalosporinstrimethoprim
aminoglycosidesmost penicillinssulfonamides
Inadequate concentrationsTherapeutic [ ] with Inflamed Meninges Only
Therapeutic [ ] Regardless of Inflammation

Intrathecal / Intraventricular Therapy
• Avoids issues of CNS penetration• Intrathecal
– may not achieve adequate concentrations– may produce local tissue irritation
• Intraventricular– surgical procedure needed for reservoir placement
• May not offer increased efficacy

Antibiotic Dosing in Meningitis
Cmin = 15-20 mg/LCmin = 5-15 mg/Lvancomycin
24 million U/day6-24 million U/daypenicillin G
2 gm q3-4h0.5-2 gm q4-6hampicillin
2 gm q12h1 gm q24hceftriaxone
2 gm q4h1-2 gm q8hcefotaxime
Dosing in MeningitisStandard DosingAntibiotic

Treatment of Specific Bacteria

Neisseria meningitidis
• Children & young adults• Cases common in winter & spring• Close contacts are at 200-1000x higher risk for
development of meningitis• Unique clinical findings
– petechiae/purpuric rash – 50%– hearing loss – 10%

Wellcome Trust Photographic Library, Synchrotron Radiation Dept., CLRC Daresbury Laboratory.

Neisseria meningitidis
• DOC: ceftriaxone or cefotaxime• Alternatives:
– chloramphenicol– meropenem– fluoroquinolone

Streptococcus pneumoniae
• #1 in adults; 12% incidence in children • Clinical findings:
– predisposing: ear/sinus (50%), pneumonia, endocarditis, head trauma, splenectomy, BMT
– seizures, coma, hearing loss common• Close contacts not at higher risk for development of
meningitis• Penicillin resistance becoming more prevalent

Streptococcus pneumoniae
gatifloxacin or moxifloxacinvancomycin +
ceftriaxone or cefotaxime+ rifampin
ceftriaxone-resistant2
gatifloxacin or moxifloxacinvancomycin +
ceftriaxone or cefotaximeceftriaxone-resistant1
gatifloxacin or moxifloxacinvancomycin +
ceftriaxone or cefotaximePRSP/DRSP
cefepime or meropenemceftriaxone or cefotaximePIRSP
ceftriaxone or chloramphenicolampicillin or penicillin GPSSP
Alternative(s)Drug(s) of ChoiceSusceptibility

Haemophilus influenzae
• Majority of cases begin as primary infection of a parameningeal focus or lung infection
• Decreasing incidence (vaccine)• Close contacts are at high risk for development of
secondary infection• β-lactamase production is common

Haemophilus influenzae
• 30-40% ampicillin-resistant (β-lactamase)• DOC: ceftriaxone or cefotaxime• Alternatives:
– chloramphenicol– meropenem– fluoroquinolone

Listeria monocytogenes
• GI tract is usual route of invasion• Incidence peaks in summer and fall• May present atypically
– often subtle signs/symptoms• Associated with high mortality (22-29%)• DOC: ampicillin ± aminoglycoside• Alternatives:
– TMP/SMX– meropenem

Empiric Therapy by Age
ampicillin + 3rd gen. cephalosporin + vancomycin
S. pneumoniaeN. meningitidis
L. monocytogenes> 50 years
3rd gen. cephalosporin ± vancomycin
H. influenzaeN. meningitidisS. pneumoniae
1-23 months
3rd gen. cephalosporin ± vancomycin
S. pneumoniaeN. meningitidis
2-50 years
3rd gen. cephalosporin +vancomycin ± ampicillin
S. agalactiaeGram - enterics
L. monocytogenes< 1 month
AntibioticsOrganismsAge

Empiric Therapy based on Gram’s Stain
H. influenzae, enterics,
? P. aeruginosa
N. meningitidis
L. monocytogenes
S. pneumoniae
Organism (s)
ceftazidime or cefepime + aminoglycosidebacilli
3rd gen. cephalosporincocci/coccobacilli
Gram negative:
ampicillin ± aminoglycosidebacilli/coccobacilli
3rd gen. cephalosporin ± vancomycincocci
Gram positive:
Suggested Empiric RegimenGram’s Stain Result

Monitoring CNS Infections
• Signs and symptoms:– frequent monitoring (q4h x 3 days)– fever, HA, VS, meningeal signs (nuchal rigidity, etc.)
• CSF: – no repeat LP unless no improvement occurs– improvement generally in 12-24h

Use of Corticosteroids

Rationale for Use
• Used since the 1950’s• Rationale: attenuation of inflammatory response
inflicted by bacterial death• Effects:
– ↓ cerebral edema, ICP– ↓ inflammation– ↓ CSF outflow resistance– ↓ neurologic/audiologic sequelae

Controversies
• Conflicting results in terms of efficacy• Potential adverse effects on antibiotic penetration• Does the organism matter?
– children: H. influenzae– adults: S. pneumoniae, N. meningitidis
• Use in adults versus children

Corticosteroid Usage
• Use in patients > 1 mo. old– insufficient data in neonates
• Administer prior to or with the first dose of ABX• Dexamethasone 0.15 mg/kg q6h x 2-4 days

Prevention

Prophylaxis
“Close contacts” – who are they?
1. within 5-7 days of onset, for ≥ 4 hours2. household members3. shared sleeping quarters4. day care attendees5. nursing homes 6. crowded/confined populations (prisons, etc.)

Prophylaxis Regimens
• N. meningitidis:– rifampin (5-10 mg/kg q12h x 4 doses)– alternatives: ceftriaxone, azithromycin, ciprofloxacin
• H. influenzae:– rifampin (20 mg/kg q24h x 4 doses)

Vaccines: H. influenzae
• Hib capsular polysaccharide• Part of usual childhood vaccine schedule• Start at 2 months of age:
– 1 dose q 2 mo. x 3 doses– 1 dose at 12 mo.

Vaccines: N. meningitidis
• Quadrivalent vaccines: serogroups A,C,Y,W-135– MenomuneR
– MenactraR
• Vaccinate high-risk patients:– splenectomy– sickle cell disease– complement deficiency– outbreaks

Vaccines: S. pneumoniae
• Antigens of 23 serotypes• 80-85% effective, 40,000 deaths/year preventable• Vaccinate:
– all > 65 y.o.– lung/heart disease, diabetes– chronic renal failure– s/p organ transplant– chemotherapy recipients– HIV


![Adult Allergy Questionnaire [Word] - webmedia · Web viewEar Infections Sinusitis Pneumonia Bronchitis Meningitis Dental Infections Bladder/Kidney Infections Skin Infections Joint](https://img.pdfslide.us/doc/110x75/5bca0ccb09d3f2f7708ba511/adult-allergy-questionnaire-word-webmedia-web-viewear-infections-sinusitis.jpg)