Embed Size (px)
Citation preview

8/28/2015
1
Hot Topics: Provider Status, Workforce and Accreditation Update
Janet A. Silvester, Pharm.D., MBA, FASHP
Vice‐President, Accreditation Services
ASHP
Conflicts of Interest
I have no conflicts of interest to disclose
Overall Learning Objectives for Pharmacists
Explain provider status and steps required for grassroots activities to impact legislation.
Describe the results of the 2014 National Pharmacy Workforce Study and the priorities of the Pharmacy Workforce Center.
Address issues related to accreditation of both pharmacy residency programs and the new collaboration between ASHP and ACPE for accredited technician education and training programs.
Review new resources available for implementation of the new PGY1 residency standards.
Discuss the alignment of the PTCB 2020 policies with ASHP policies and the goals of the ASHP/ACPE collaboration on technician education and training.
Overall Learning Objectives for Pharmacy Technicians
Describe what provider status is.
Describe the results of the 2014 National Pharmacy Workforce Study and the priorities of the Pharmacy Workforce Center.
Address issues related to accreditation of both pharmacy residency programs and the new collaboration between ASHP and ACPE for accredited technician education and training programs.
Discuss the alignment of the PTCB 2020 policies with ASHP policies and the goals of the ASHP/ACPE collaboration on technician education and training.
Review key requirements in the technician program standards.
PROVIDER STATUS
Discussion PointsDescribe what provider status is.
Describe why amending the Social Security Act to recognize pharmacists as Medicare Part B providers is important for patients.
Explain current legislation, and the efforts of ASHP and the Patient Access to Pharmacists’ Care Coalition to facilitate amending the Social Security Act to recognize pharmacists as Medicare Part B providers.
Describe grassroots efforts that individual pharmacists and ASHP state affiliates need to take to achieve recognition as Medicare Part B providers in the Social Security Act.

8/28/2015
2
Provider Status is About Patients
Achieving provider status is about giving patients access to care that improves:
Patient safety
Healthcare quality
Outcomes
Decreases costs
Who Has Provider Status?
Physicians
Nurse practitioners
Physician assistants
Certified nurse midwives
Psychologists
Clinical social workers
Certified nurse anesthetists
Speech‐language pathologists
Audiologists
Registered dietitians
Physical therapists
What is Provider Status?
Being listed in section 1842 or 1861 of the Social Security Act as a supplier of medical and other health services.
Becoming a “provider” in the Social Security Act means:
Pharmacists can participate in Part B of the Medicare program and bill Medicare for services that are within their state scope of practice to perform.
Why is provider status important for pharmacists?
Pharmacists are not recognized under the Social Security Act as health care providers
New payment systems emphasize quality and outcomes Accountable Care Organizations
Medical Homes
Social Security Act determines eligibility
What is H.R. 592/S. 314?A bipartisan bill that would amend the Social Security Act to recognize pharmacist services to patients under Medicare Part B in medically underserved communities
Applies to licensed pharmacists working within their state’s scope of practice laws
Establishes a mechanism of pay for pharmacist provider services under Medicare Part B
Reintroduction of H.R. 4190, a bill which was introduced by Representatives Guthrie (R‐KY), Butterfield (D‐NC) and Young (R‐IN) in the House of Representatives on March 11, 2014
That bill had 123 bipartisan cosponsors include two physicians: Reps. Roe (R‐TN) and Bera (D‐CA).
H.R. 592/S. 314 SpecificsAmends Section 1861(s)(2) of the Social Security Act to include:
Pharmacists services furnished by a pharmacist licensed by State law
Which the pharmacist is legally authorized to perform in the State
In setting located in/for and defined in federal law:
Medically underserved area
Medically underserved population
Health professional shortage area

8/28/2015
3
Why does H.R. 592/S. 314 only cover medically underserved communities?
Help meet unmet health care needs Increase access
Improve quality
Decrease costs
Follow similar successful paths taken by other health care professionals to gain provider status
What are medically underserved communities?
Medically Underserved Areas
Medically Underserved Populations
Health Professional Shortage Areas
Medically Underserved Communities, a Closer Look
Medically Underserved Areas:
Medically Underserved Areas (MUAs) may be a whole county or a group of contiguous counties, a group of county or civil divisions or a group of urban census tracts in which residents have a shortage of personal health services.
Medically Underserved Areas, MUA
Medically Underserved Areas, how are they calculated?Uses Index of Medical Underservice (IMU), scale 0‐100; 62 or less is MUA
Uses 4 variables to calculate:Ratio of primary care physicians per 1,000 people
Infant mortality rate
Percent of population below poverty
Percent of population 65 or older
Medically Underserved Populations, MUP
Medically Underserved Populations
Uses same IMU but applies it to population groups
Medically Underserved Populations (MUPs) may include groups of persons who face economic, cultural or linguistic barriers to health care
Typically low income or Medicaid eligible
Exceptional Designations
May not fit the criteria of MUA/MUP
Governor can make the request for an exception
Based upon “unusual Local Conditions”

8/28/2015
4
Patient Access to Pharmacists’ Care Coalition (PAPCC)
Formed January 2014
Group of 30 organizations representing patients, pharmacists, pharmacies and other interested stakeholders
Drafted H.R. 4190 to expand medically‐underserved patients’ access to pharmacist services consistent with state scope of practice
Facilitated reintroduction
Patient Access to Pharmacists’ Care Coalition (PAPCC)
Current Members
ASHP
APhA
AACP
ASCP
HLC
IACP
HOPA
NCPA
NACDS
NASPA
Walgreens
Current Members
Albertson's
Amerisource Bergen
Bi‐Lo Pharmacy
Cardinal Health
CVS Caremark
Food Marketing Institute
Fred's Pharmacy
Fruth Pharmacy
Kroger
National Center for Farmworker Health
Omnicell
Rite Aid
Safeway Inc.
SuperValu Pharmacies
Target
Thrifty White Pharmacy
WalMart
Winn‐Dixie
Why Do Pharmacists Want Provider Status When Fee‐For‐Service is Going Away?
Over the next 5 or more years traditional fee‐for‐service will be phased out and replaced with new payment systems that emphasize quality, outcomes, and team‐based patient care.
Pharmacists recognize that traditional fee‐for‐service is not the model of the future, and we view ourselves as members of interprofessional teams collaborating with physicians, nurses, and others throughout the continuum of care.
However, the Social Security Act (SSA) remains the reference point for which practitioners are eligible to participate in current, new, and emerging delivery systems and payment models (see ACO example).
Therefore, for pharmacists to fully participate in current and emerging delivery and payment systems, pharmacists need to be listed in the SSA along with other providers.
State Scope of Practice
Provider status at the federal level will only allow a pharmacist to participate in the Medicare program and to bill for services that are within their state scope of practice to perform (the same is true for physicians and other providers)
State scope of practice will determine what pharmacists can actually do in terms of the provision of service
As provider status at the federal level is achieved continued efforts by states to ensure scope of practice for pharmacists is sufficiently robust will be vital
Status Update
As mentioned earlier, HR 4190 had 123 cosponsors at the end of the 113 Congress Reintroduced in 2015 as H.R. 592/S. 314.
The strategy for 2014, late in the Congressional session, was to build support for this legislation by getting as many cosponsors as possible, for quick re‐introduction in 2015
2015 will see Coalition pushing for cosponsors; House and Senate hearings and committee consideration
Status Update
H.R. 592 Co‐Sponsors ( as of August 11, 2015)
185
SB 31428

8/28/2015
5
ASHP Students Visit Capitol Hill Questions (both House and Senate)
How qualified are pharmacists to provide these services? Pharmacists are very well‐qualified to provide these services. The legislation would enable pharmacists to provide services
they already are authorized to provide under state law, and prepared to provide through their extensive professional education.
What will this cost Medicare?We believe that pharmacist provided patient care will lead
to better health outcomes and in many cases reduce costs – care transitions is a good example
However, we also know that the Congressional Budget Office often does not score (assign a price tag) bills with offsets
Questions (both House and Senate)
Who decides what services pharmacists could provide? The services pharmacist can provide would still be set by state
scope of practice laws and regulations, just as is done today. This bill does nothing to change such regulations; it simply permits Medicare to pay pharmacists for delivering care to patients that fits within the regulations of each state.
Is there precedence for this type of legislation? Yes. Longstanding law has enabled nurse practitioners and
physician assistants to be reimbursed by Medicare for providing Part B services. The law originally limited such reimbursement to cases when delivered to underserved rural populations, but such restrictions were removed in the late 1990s.
Questions (both House and Senate)
Does this proposal seek to have pharmacists fill the role of doctors? No. It simply seeks to have pharmacists help address acute shortages
and to be eligible for payment for services they are already allowed to provide under their respective state licenses.
The intention is not to displace doctors; rather it is to help doctors in medically underserved communities so physicians can focus their time and attention on those patients who need it most.
Just like NPs, PAs and others are part of the large healthcare ecosystem and seen as part of the interdisciplinary care team, so to should be pharmacists.
To date, no physician groups have come out opposed to the bill
Is this collaborative? Yes, full ACO, medical home or other integrated effort can only be
achieved with provider status—all roads lead back to being listed
Does H.R. 592/S. 314 require pharmacists to be residency trained, Board certified, or possess other
credentials?
A: No, just like other health care professionals who are recognized as providers, H.R. 592/S. 314 requires pharmacists to be licensed by a state, and the state legislature and board of pharmacy, health care organizations, and private health plans determine what credentials are required to perform certain services (e.g., CA: “Advanced Practice Pharmacist” NM: “Pharmacist Clinician”).
Most hospitals and health systems have a process to credential and privilege pharmacists based on the type and level of patient care services they provide.
Why isn’t ASHP calling for credentialing requirements given that ASHP started pharmacy residencies and supports Board certification?
A: ASHP supports these concepts, but they do not belong in federal law.
Instead, credentialing and privileging requirements are for states and organizations to decide through state pharmacy practice acts, private health plan requirements, and credentialing and privileging requirements by hospitals and health systems.

8/28/2015
6
Key Takeaways
Key Takeaway #1H.R. 592/S. 314 would grant provider status to pharmacists practicing in medically underserved areas, or populations
Key Takeaway #2 Virtually all of the pharmacy profession is on board
Key Takeaway #3Must continue pushing, addressing the cost questions and grow the coalition
The Path Forward
Reintroduction of the House bill in 2015
Introduction in Senate
Ramp up grassroots efforts
Secure additional cosponsors
Push for committee hearings
Grow the coalition
Educate the public on value of pharmacists’ care
Keys to Success
Pharmacy must maintain unified stance
Grassroots efforts must be robust 270,000 licensed pharmacists in the U.S. can have a huge impact
Focusing on the unmet need, new Medicare enrollees
Election results do not change our message
How can you support H.R. 592/S. 314?
Ask your legislators to cosponsor the bill
Encourage colleagues to get involved.http://www.ashp.org/menu/Advocacy/GrassrootsNetwork
Participate in the ASHP PAChttp://www.ashp.org/menu/Advocacy/ASHPPAC
Specific State Affiliate and Individual Actions
Recruit individual health system support of H.R. 592/S. 314
Solicit other state‐level health profession organization support of H.R. 592/S. 314: Medical specialties
Nurse practitioners
Physician assistants
Visit elected officials/staff in Washington DC or district office
State Provider Status
ASHP to work with state affiliates to move state legislation to recognize pharmacists as providers
Expanding state scope of practice so pharmacists can practice at the top of their license
State Medicaid, private payers

8/28/2015
7
Recent Report
The Expanding Role of Pharmacists in a Transformed Health Care System
National Governors Association
January 13, 2015
http://www.nga.org/files/live/sites/NGA/files/pdf/2015/1501TheExpandingRoleOfPharmacists.pdf
Conclusions
The patients we serve will benefit greatly when pharmacists are recognized by Medicare.
Pharmacy is better positioned and closer than ever to being federally recognized as providers.
Conclusions
It will take unprecedented levels of grassroots engagement by individual pharmacists and state affiliates to make it happen.
Students can and should play a major role
ASHP is here to help you every step of the way.
•Being listed in the Social Security Act as Medicare Part B providers will expand pharmacists’ scope of practice.
A. True
B. False
Medically underserved areas include both urban and rural parts of the United States.
A. True
B. False
The Pharmacy and Medically Underserved Areas Enhancement Act (H.R. 592 and S. 314) prohibits states, health insurers, and healthcare organizations from requiring pharmacists to have additional training or credentials such as residency training and/or Board certification.
A. True
B. False

8/28/2015
8
•A key goal of The Pharmacy and Medically Underserved Areas Enhancement Act (H.R. 592 and S. 314) is to help
fulfill and unmet need in the healthcare delivery system.
A. True
B. False
The healthcare payment system is moving to a value-based (pay for outcomes and performance) versus volume-based (fee-for-service) model.
A. True
B. False
National Pharmacist Workforce Study 2014
Discussion Points
Describe the priorities of the Pharmacy Workforce Center
Describe the results of the 2014 National Pharmacy Workforce Study
Recognize trends presented in patient care and pharmacists activities
Pharmacy Workforce Center, Inc.
American Association of Colleges of Pharmacy (AACP)
American College of Clinical Pharmacy (ACCP)
American Pharmacists Association (APhA)
American Society of Health‐System Pharmacists (ASHP)
Board of Pharmacy Specialties (BPS)
Bureau of Health Workforce (BHW)
National Alliance of State Pharmacy Associations (NASPA)
National Association of Boards of Pharmacy (NABP)
National Association of Chain Drug Stores (NACDS) Foundation
National Community Pharmacists Association (NCPA),
Pharmacy Technician Certification Board (PTCB)
Presentation Overview
Overview of the National Pharmacist Workforce Studies
Results of the 2014 National Pharmacist Workforce Study
Trends in Patient Care and Other Activity Pharmacists
Conclusions

8/28/2015
9
Response Distribution by Region
RespondentsNortheast (n=458)South (n=793)Midwest (n=649)West (n=546)
Non‐RespondentsNortheast (n=536)South (n=963)Midwest (n=553)West (n=578)
Overall Response Rate: 2446/5073 = 48.2%
Work Status of Licensed Pharmacists
73
68
67
62
15
18
21
13
3
4
2
3
9
10
10
22
0% 20% 40% 60% 80% 100%
2000
2004
2009
2014
Full‐Time Part‐time Not Working in Pharmacy Retired/Not Working
Age of Licensed Pharmacists
41
31
23
28
45
50
54
48
14
20
24
24
0% 20% 40% 60% 80% 100%
2000
2004
2009
2014
23‐40 41‐60 61 +
Race/Ethnicity of Licensed Pharmacists
88
88
87
85
7
7
8
9
2
2
2
2
2
2
2
2
1
1
1
2
75% 80% 85% 90% 95% 100%
2000
2004
2009
2014
White Asian Black Latino/a American Indian Other
Highest Degree Earned by Licensed Pharmacists
74
71
66
52
14
19
22
38
12
10
12
10
0% 20% 40% 60% 80% 100%
2000
2004
2009
2014
BS Pharmacy PharmD MS/MBA/PhD/Other
Percent of Actively Practicing Pharmacists that are Female: 1990‐2014
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
1990 2000 2004 2009 2014
31.3%
44.8% 45.9% 46.4%
57.1%

8/28/2015
10
Mean Age by Gender: 2000‐2014
0
10
20
30
40
50
60
2000 2004 2009 2014
Male
Female
46
3841
53
45
50
44
50
Mean Full‐Time Equivalent (FTE) Contributions by Age & Gender
1.03 1.03
0.98
1.1
1.041.01 1.00
0.88
0.62
0.61
0.99 1.000.96
0.9 0.9
0.98
0.85 0.87
0.69
0.44
0
0.2
0.4
0.6
0.8
1
1.2
<30 31-35 36-40 41-45 46-50 51-55 56-60 61-65 66-70 >70
Males
Females
2009Females: 0.82Males: 0.92
2014Females: 0.93Males: 0.95
Pharmacy Degrees Conferred as First Professional Degree (1965 – 2013)
0
2000
4000
6000
8000
10000
12000
14000
1965
1967
1969
1971
1973
1975
1977
1979
1981
1983
1985
1987
1989
1991
1993
1995
1997
1999
2001
2003
2005
2007
2009
2011
2013
BS Pharm
PharmD
Total
Linear (Total)
Post‐Capitation
All PharmD
Health Reform
Source: 2012‐13 Profile of Pharmacy Students ‐ AACP
Capitation
Practice Settings
Community: Independent, Chain, Mass Merchandiser, Supermarket
Hospital: In‐patient or out‐patient hospital settings
Other Patient Care Settings: nursing home, long term care, HMO, nuclear, clinic‐based, mail service, central fill, home health/infusion, and specialty pharmacies
Other Non‐Patient Care Settings: pharmacy benefit administration, academic, government administration, pharmaceutical industry, consulting, professional associations, and other organizations that were not licensed as a pharmacy
Actively Practicing Pharmacists’ Employment Setting: 2009
Independent
Chain
Mass Merchandiser
Supermarket
Hospital
Other Patient Care
Non Patient Care
14%
25%
5%
9%
10%
27%
10%54%Community
38%Hospital/other pt care
9% Other
Actively Practicing Pharmacists’ Employment Setting: 2014
Independent
Chain
Mass Merchandiser
Supermarket
Hospital
Other Patient Care
Non Patient Care
10%
19%
7%
10%
8%29%
17%
44%Community
46%Hospital/Other pt care
10% Other

8/28/2015
11
Practice Settings 2009 and 2014
54%
27%
10% 9%
44%
30%
16%10%
0%
10%
20%
30%
40%
50%
60%
Community Hospital Other, PharmacySetting
Other, Non‐PharmacySetting
2009
2014
Position Type 2000, 2004, 2009,2014
7% 7% 8% 5%
30% 29% 30% 30%
0%
10%
20%
30%
40%
50%
60%
70%
2000 2004 2009 2014
Owner Management Staff
63% 62%65%65%
Services Offered At Practice Site: 2014
0% 10% 20% 30% 40% 50% 60% 70%
Medication Therapy Management
Immunizations
Adjusting Medication Therapy
Medication Reconcillation
Ordering Lab Tests
Health Coaching/Screening
Proportion of Full‐time Pharmacists with High* Job Satisfaction by Practice Setting: 2000, 2004, & 2014
0%10%20%30%40%50%60%70%80%90%
100%
Indep Chain MM Super Hosp OPC ONPC Overall
2000 2004 2014* High is a summated score of five items (1 = strongly disagree to 5 = strongly agree) > midpoint (15)
Proportion of Full‐time Pharmacists with High* Professional Commitment by Practice Setting: 2000,
2004 & 2014
0%10%20%30%40%50%60%70%80%90%
100%
Indep Chain MM Super Hosp OPC Other Overall
2000 2004 2014 * High is a summated score of five items (1 = strongly disagree to 5 = strongly agree) > midpoint (15)
Proportion of Pharmacists Who Are Part of an Interprofessional Health Care Team Providing
Patient Care by Practice Site: 2014
0%
10%
20%
30%
40%
50%
60%
Indep Chain MM Super Hosp OPC ONPC Overall

8/28/2015
12
Proportion of With Regular Direct Contact with Other Health Care Providers Regarding Patient Care Activities
by Practice Site: 2014
0%
10%
20%
30%
40%
50%
60%
70%
80%
Indep Chain MM Super Hosp OPC ONPC Overall
Participation in Contemporary Healthcare Activities 2014 (all pharmacy settings)
0% 20% 40% 60% 80% 100%
Part of an Interprofessional Health CareTeam?
Regular Direct Contact with Health CareProviders Regarding Patient Care?
Patient‐Centered Medical Home?
Affiliated with Accountable CareOrganization?
Activities Monitored or Evaluated in Your Work Place 2014
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
Patient Satisfaction
Quality of Care
Patient Outcomes
Patient Safety
Percent Time Spent in Patient Care: 2014
0% 5% 10% 15% 20% 25%
2000
2004
2009
2014
Percentage of Time Spent in Patient Care by Community Pharmacists: 2000‐2014
0 2 4 6 8 10 12 14
Independent
Chain
Mass Merchandiser
Supermarket
2014
2009
2004
2000
Percentage of Time Spent in Patient Care Activities by Hospital, Other Patient Care and Non‐Patient Pharmacists: 2000‐2014
0 5 10 15 20 25 30 35
Hospital/Health System
Other Patient Care (OPC)
Other Non‐Patient Care (ONPC)
2014
2009
2004
2000

8/28/2015
13
Ratings of Workload as High or Excessively High* by Work Setting: 2004, 2009 & 2014
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Indep Chain MM Super Hosp OPC Other Overall
2004 2009 2014 * High is a summated score of five items (1 = strongly disagree to 5 = strongly agree) > midpoint (15)
Pharmacists’ Ratings of Highly Stressful Events: 2004 & 2014
0% 10% 20% 30% 40% 50%
Having so Much Work to doEverything Cannot be Done Well
Not Being Staffed with an AdequateNumber of Pharmacy Technicians
Having to Meet Quotas
Being Interupted by Phone Calls orPeople While Performing Job Duties
Disagreement Concerning theTreatment of Patients
2014
2004
Workplace Labor Reductions: 2009 & 2014
0% 5% 10%15%20%25%30%35%40%
Pharmacist Lay Offs
Mandatory Reduction in PharmacistHours
Early Retirement Incentives
Restructuring of Pharmacist WorkSchedules
2014
2009
Work Activities
Patient Care Services Not Associated with Medication Provision: assessing and evaluating patient medication‐related needs, monitoring and adjusting patients’ treatments to attain desired outcome, and other services designed for patient care management
Patient Care Services Associated with Medication Provision: preparing, distributing, and administering medication products, including associated consultation, interacting with patients about selection and use of over‐the‐counter products, and interactions with other professionals during the medication dispensing process
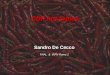
Proportion of U.S. Pharmacists by Segment in Descending Size
(2009 data in lighter tone and 2014 data in darker tone) ASHP Surveys show peak pharmacist shortage in 2000, with decline in vacancy rates since
0
1
2
3
4
5
6
7
8
9
2000 2002 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
8.9
7.2
5.76.3
5.76.3
5.9
3.7
2.82.4 2.7
2.1 2.2
Per
cen
t V
acan
cies
Hospital Pharmacist Vacancy Rates

8/28/2015
14
Pharmacy Director perceptions of availabilityType of Staff 2014 2008
Management
Shortage 68% 90%
Balanced 29% 9%
Excess 3% 1%
Clinical Coordinator
Shortage 44% 72%
Balanced 46% 23%
Excess 10% 5%
Clinical Specialist
Shortage 37% 70%
Balanced 45% 23%
Excess 18% 7%
Entry‐level Frontline R.Ph.
Shortage 10% 75%
Balanced 35% 23%
Excess 55% 2%
Experienced Frontline R.Ph.
Shortage 41% 89%
Balanced 40% 10%
Excess 19% 1%
2008‐2014 ASHP National Survey
A lot of press on possible surplus of pharmacists
National Center for Health Workforce Analysis
Health Workforce Projection: Pharmacists
Released December 2014
Uses HRSA Health Workforce Simulation Model
Accounts for changes in supply (new entrants, retirement, hours worked patterns)
Accounts for changes in demand (ACA Rx coverage, population demographics, demand for prescription medications)
Does not account for future growth in patient care services/roles of pharmacists, provider status, changes in part D coverage
Projected Supply for Pharmacists: 2012‐2025
FACTOR SUPPLY
Estimated supply in 2012 264,100
Total supply growth 2012‐2025: 91,200 (35%)
New entrants 160,500
Changing work patterns (61,340)
Attrition 7,960
Projected supply, 2025 355,300
Health Workforce Projections: Pharmacists; National Center for Health Work Force Analysis: May 2015
Projected Demand for Pharmacists: 2012‐2025
FACTOR DEMAND
Estimated demand, 2012 264,100
Total demand growth 2012‐2025 42,300 (16%)
Changing demographics impact 35,800 (14%)
ACA insurance coverage impact 6,500 (2%)
Projected demand, 2025 306,400
Adequacy of supply, 2025 355,300 ‐ 306,400 = +48,900
Health Workforce Projections: Pharmacists; National Center for Health Work ForceAnalysis: May 2015
Factors influencing the “supply”
The number of pharmacy graduates (big, long term)
State of the economy (big, short term) Impact on the number of pharmacists retiring
Impact on part time to full time shift
The gender mix (slowly growing)
The number of international pharmacy graduates (minimal)

8/28/2015
15
Factors influencing the “demand”
The demand by employers
State of the economy
Prescription volume
NEW roles of pharmacists
Changing role of pharmacists
Changing role of pharmacy technicians
Impact of automation and technology
Conclusions
We are living in dynamic times as a health care profession
Pharmacists have taken a larger role in health care delivery by increasing access for patients through provision of expanded service offerings
But, how do we determine the appropriate supply of and demand for pharmacists?
Continued monitoring of the pharmacist workforce is crucial so the pharmacy profession is able respond to the rapidly changing landscape
The percentage of female practicing pharmacists is ______ compared to the previous study.
A. Growing
B. Decreasing
C. Remaining constant
There are more workforce labor reductions in 2014 than in 2009
A. True
B. False
The HRSA workforce projection report from 2014 says that we will have a _____ of pharmacists by 2025.
A. Deficit
B. Surplus
ASHP Accreditation Update

8/28/2015
16
Discussion Points
Identify key changes in the revised PGY1 residency standard
Review new resources available for implementation of the new PGY1 residency standards
Describe the 2014 residency match statistics and results
New PGY1 Standards: Background
New PGY1 Standards approved 2014
Major goals of revision:
Update and streamline while maintaining quality
Highlights
Same purpose statement for all PGY1 residency programs
From the Standard
PGY1 Program Purpose:
PGY1 pharmacy residency programs build on Doctor of Pharmacy (Pharm.D.) education and outcomes to contribute to the development of clinical pharmacists responsible for medication‐related care of patients with a wide range of conditions, eligible for board certification, and eligible for postgraduate year two (PGY2) pharmacy residency training.
Goals and objectives streamlined and reduced in number
2005 2014
Competency areas / Outcomes 6 4
Goals 23 9
Objectives 66 33
RPD may delegate some authority 1.1: The RPD or designee must evaluate qualification of applicants…
3.4.a.(2): The results of residents’ initial assessments must be document by the program director or designee in each resident’s development plan…
3.4.d.(1) Each resident must have a resident development plan documented by the RPD or designee.
3.4.d.(2) On a quarterly basis, the RPD or designee must assess residents’ progress and determine if the…plan needs to be adjusted.
3.5.b: The RPD or designee must develop and implement program improvement activities…
4.1.c: The RPD may delegate, with oversight, to one or more individuals…administrative duties/activities for the conduct of the residency program.

8/28/2015
17
Preceptor qualifications include more options and include teaching and precepting
skills
4.8 Preceptor Qualifications
4.8.a. Ability to precept residents… by use of clinical teaching roles…
4.8.b. Ability to assess residents’ performance
Preceptor‐in‐training role added
4.9.a. Pharmacists new to precepting who do not meet the qualifications for residency preceptors…must:
(1) be assigned an advisor or coach who is
a qualified preceptor; and,
(2) have a documented preceptor
development plan to meet the
qualifications for becoming a residency
preceptor within two years.
New Training Update:Residency Program Design and
Conduct
New online recorded webinars
New workshops
NEW! Recorded Webinars Available OnlineRecorded webinars:Design of PGY1 residency programs
PGY1 residency program purpose
PGY1 competency areas, goals, and objectives
Residency program structure
Learning experience descriptions
The four preceptor roles
Evaluation
Residents’ development plans
Continuous residency program improvement
New workshops: National Pharmacy Preceptors Conference and the Midyear
Residency Program Design and Conduct (RPDC) Workshops
Instructors answer your questions
Apply information to your program
Bring your program’s materials for individualized feedback
Peer sharing
More‐see Accreditation webpage “Additional Accreditation Resources,” “Accreditation‐
Related Online Education”:
Resident's Learning Activities: Understanding Learning Taxonomies and Levels ‐ New (2014) Standards
Customizing the Resident Training Plan (2005 Standard)
All About Purpose Statements (2005 Standard)
Anatomy of the Outcomes, Goals and Objectives (2005 Standard)
Level With Your Resident: Learning Taxonomies and Levels (2005 Standard)
Starring Roles: The Four Preceptor Roles and When to Use Them (2005 Standard)
Responding to an ASHP Accreditation Survey Report
Coming soon:
Additional programs on the new standards

8/28/2015
18
AJHP: Residents Edition
Expands publication opportunities for residents
Further engages residents, preceptors and residency program directors in AJHP and ASHP
AJHP: Residents Edition
Quarterly, online supplement to AJHP
Founders Bryan McCarthy and David Reardon to become AJHP contributing editors, pharmacy resident publications
Coming … June 2015
Member benefit
ASHP Match 2015
Pharmacy Residencies
0
200
400
600
800
1000
1200
1400
1600
1800
2000
ASHP Accredited Pharmacy Residency Program Growth (1980-2015) as of 1/5/15
Hospital Pharmacy Practice PGY1 Clinical Specialized PGY2
1,861

8/28/2015
19
Program Count by Category as of 7/2015Category Sub Category Programs
PGY1
Pharmacy 926
Community Pharmacy 122
Managed Care Pharmacy 45
PGY1 & PGY2 Combined
PGY1 Pharmacy & PGY2 Health‐System Pharmacy Administration/MS
37
PGY1 Pharmacy & PGY2 Pharmacotherapy 12
PGY1 Pharmacy & PGY2 Health System Pharmacy Administration
7
PGY1 Pharmacy & PGY2 Pharmacy Informatics 1
PGY1 Community Pharmacy & PGY2 Community Pharmacy Administration/MS
1
Pharmacotherapy 1
PGY1 Pharmacy & PGY2 Specialty Pharmacy 1
PGY1 Pharmacy & PGY2 Specialized Area: Medication Systems & Operations
1
PGY2 Critical Care Pharmacy 116
Ambulatory Care Pharmacy 102
Oncology Pharmacy 88
Infectious Diseases Pharmacy 72
Psychiatric Pharmacy 51
Pediatric Pharmacy 47
Solid Organ Transplant Pharmacy 35
Internal Medicine Pharmacy 34
Health‐System Pharmacy Administration 33
Emergency Medicine Pharmacy 29
Cardiology Pharmacy 28
Pharmacy Informatics 20
Geriatric Pharmacy 18
Drug Information 13
Palliative Care/Pain Management Pharmacy 11
Medication‐Use Safety 9
Pharmacotherapy 5
Pharmacy Outcomes/Healthcare Analytics 4
Transitions of Care 4
Pharmacogenetics 3
HIV Pharmacy 3
Nutrition Support Pharmacy 2
Neurology 1
Nephrology Pharmacy 1
Nuclear Pharmacy 1
Family Medicine 1
Health System Corporate Pharmacy Administration
1
Corporate Pharmacy Leadership 1
390
157
104
78
222240
281
168
219
2007 2008 2009 2010 2011 2012 2013 2014 2015
# PGY1 positions added to Match each year
Residency Capacity Conference 2/11
58
29
59
7571
107
100
114
2008 2009 2010 2011 2012 2013 2014 2015
# PGY2 positions added to Match each year
Residency Capacity Conference 2/11
2015 versus 2014 match
5% increase in PGY1 applicants
6.5% increase in # of filled PGY1 positions
(total = 2,640 PGY1 positions filled)
7% increase in PGY2 applicants
12.5% increase in filled PGY2 positions(total = 794 PGY2 positions filled ‐ includes 297 early
commits)
Applicants view on March 20, 2015
3,308 applicants match day
2811 PGY1 matched
497 PGY2 match & 297 Early Commit = 794 PGY2
1,755 applicants unmatched
1,547 PGY1 & 208 PGY2

8/28/2015
20
1900
2092
2508
2915
3277
3706
3933
4142
4358
16121769
18731951
2173
2413
26942862
3081
1343
14871651
1801
20272268
24952640
2811
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
2007 2008 2009 2010 2011 2012 2013 2014 2015
ASHP Residency Matching Program2007‐2015
PGY1
# applicants
# positions
# matched
91% fill for all PGY1
239
330384
483
541
677
777
917
1002
286334
380
439
514
585
692
792
906
195
267297
369438
505
601
706
794
4181 88
114144 179
230260
297
0
200
400
600
800
1000
1200
2007 2008 2009 2010 2011 2012 2013 2014 2015
ASHP Residency Matching Program2007‐2015
PGY2
# applicants (includesearly commits)
# positions (includesearly commits)
# total match (earlycommit+match)
# early comit
88% fill for PGY2
288 323
635
964
1104
12931239
1491
1373
0
200
400
600
800
1000
1200
1400
1600
1800
2007 2008 2009 2010 2011 2012 2013 2014 2015
Shortage of PGY1 positions ‐ based on match participants and available PGY1 positions
0
2000
4000
6000
8000
10000
12000
14000
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Pharmacy Graduates vs Resident PGY1 Positions
Graduates Positions Linear (Graduates) Linear (Positions)
4.84:1
4.9:1
5.27:1
13,838
2,862
Percentage of Graduates seeking Residency
Year Graduates Participants in PGY1 Match
Percentage of Grads in Match
2006 10,199 1,356 13.3%
2007 10,282 1,898 18.5%
2008 11,127 2,092 18.8%
2009 11,516 2,501 21.7%
2010 11,487 2,898 25.2%
2011 12,346 3,257 26.4%
2012 13,163 3,706 28.2%
2013 13,207 3,933 30%
2014 13,838 4,142 30%
2015 (Knapp, et al) 13,856
2016 14,923 3,925 (26%), 4,477 (30%)
We will need to grow positions by 56% or by 1,615 positions by 2016
What is ASHP doing to address shortage?
2/11 Capacity Conference
Highlighting programs with expansion at Meetings
New training programs – including web based
How To Start a Residency
How To Expand Existing Residencies
National Pharmacy Preceptors Conference (NPPC)Yearly
Preceptor Skills Resource Page
On line education about accreditation standard
PR – Video
New streamlined Accreditation Standards
Guidance documents for PGY1 standard
New AJHP residents edition for journal

8/28/2015
21
Pharmacy Technician Program Accreditation
Discussion Points
Describe the new collaboration between ASHP and ACPE for accredited technician education and training programs
Review key requirements in the technician program standards
Discuss the alignment of the PTCB 2020 policies with ASHP policies and the goals of the ASHP/ACPE collaboration on technician education and training
Pharmacy Technician Accreditation Commission (PTAC)
Formed through ASHP/ACPE collaboration
PTAC recommendations require approval of both ASHP and ACPE Boards
Transition occurred in 2014 and joint accreditation decision recommendations to ASHP and ACPE Boards began in June 2015
PTAC adopted newly approved ASHP standards, guidelines, procedures
Programs now transitioning from ASHP‐accredited to ASHP/ACPE accredited status
Pharmacy Technician Accreditation Commission
Angela Cassano, PharmD, BCPS, FASHP – President Pharmfusion Consulting, LLC, Midlothian, VA
Michael Diamond, MSc – President World Resources Chicago Evanston, IL
Jacqueline Hall, RPh, MBA –Pharmacy Manager Walgreens, New Orleans, LA
Jan Keresztes, PharmD – South Suburban College, South Holland, IL
Barbara Lacher, BS, RPhTech, CPhT –North Dakota State College of Science Wahpeton, ND
Douglas Scribner, CPhT, Med –Central New Mexico Community College, Albuquerque, NM
John Smith, EdD – Corinthian Colleges, Inc., Santa Ana, CA
Donna Wall, PharmD – Indiana University Hospital, Indianapolis, IN
LiAnne (Webster) Brown, CPhT –Richland College, Dallas, TX
Lisa Lifshin, B.S.Pharm, ASHP, Secretary
Board Liaisons
Anthony Provenzano, PharmD – ACPE Board Liaison, New Albertson’s, Inc. Chicago, IL
Kelly Smith, PharmD – ASHP Board Liaison, University of Kentucky College of Pharmacy, Lexington, KY
Functions of PTAC Reviewing applications for accreditation and evaluations of pharmacy technician education and training programs,
Recommending accreditation actions to the ASHPBoard of Directors and the ACPE Board of Directors
Making recommendations to the Boards regarding standards, policies and procedures, and other matters related to PTAC’s activities and services
Assisting in strategic planning in matters related to pharmacy technician education and training accreditation.
Functions of PTAC cont.
Identifying potential activities and collaborative opportunities
Soliciting and receiving input and advice from other stakeholders to obtain broad perspectives to help assure the quality, validity and improvement of PTAC’s accreditation standards, activities and services.

8/28/2015
22
ASHP‐Accredited Pharmacy Technician Training Programs
‐50
0
50
100
150
200
250
300 275258
234
169
Ultimate Goal of ASHP‐ACPE Collaboration
→ A better qualified and trained workforce
→ Improved patient safety
→ Greater consistency in technician workforce
→ Accreditation standards updated as needed to stay consistent with expanding roles and responsibilities of technicians
→ Greater ability to delegate technical tasks from pharmacists to technicians
→ Less turnover in pharmacy technician positions
Accreditation Standards for Pharmacy Technician Training Programs
New accreditation standards approved by ASHP and ACPESix components to new standard:
Administration, Program Faculty, Education & Training, Students, Evaluation & Assessment, Graduation & Certificate
Knowledge areas mapped to PTCB task analysis
Changes to program director/experiential site requirements
Hours requirement revised
Faculty (Standard 2)
Program Director
Must be Pharmacist or Pharmacy Technician
Pharmacy Technician Minimum – working on Associates Degree or State Teaching Certificate
Experiential Site coordinator
Individual working at the experiential training site, coordinating activities
Liaison to Program Director
Std. 3.6: Education and Training Goals (n= 45)
Personal/Interpersonal Knowledge and Skills (n=7)
Foundational Professional Knowledge and Skills (n=9)
Processing and Handling of Medications and Medication Orders (n=11)
Sterile and Non‐Sterile Compounding (n=3)
Procurement, Billing, Reimbursement and Inventory Management (n=4)
Patient‐ and Medication‐Safety (n=6)
Technology and Informatics (n=1)
Regulatory Issues (n=2)
Quality assurance (n=2)
Students ‐ Qualifications of Candidates (Standard 4)
In High School, or HS graduate or equivalent
English Proficiency
Math Proficiency
Age Requirements (state dependent)
Illicit drug use and criminal background Assessed prior to acceptance

8/28/2015
23
Related MaterialsGuidance document
http://www.ashp.org/DocLibrary/Accreditation/Guidance‐Document.pdf
Model curriculumhttp://www.ashp.org/DocLibrary/Accreditation/Model‐Curriculum.pdf
Regulationshttp://www.ashp.org/DocLibrary/Accreditation/Regulations‐on‐Accreditation‐of‐Pharmacy‐Technician‐Education.pdf
Program Composition Standard:Knowledge Areas
Technician Accreditation Standard
Personal/Interpersonal Knowledge & skills
Foundation Professional Knowledge & skills
Processing & Handling of Medication Orders
Sterile & Non‐Sterile Compounding
Procurement, Billing, Reimbursement &
Inventory Management
Patient and Medication Safety
Technology & Informatics
Regulatory Issues
Quality Assurance
45 total goals
PTCB Blueprint
‐‐‐‐‐‐‐‐
↔ Pharmacology
↔ Medication Order Entry and Fill Process
↔ Sterile and Non‐Sterile Compounding
↔ Pharmacy Billing & Reimbursement
↔ Pharmacy Inventory Management
↔ Medication Safety
↔ Rx Information System Usage/Application
↔ Pharmacy Law & Regulations
↔ Pharmacy Quality Assurance
About PTCBMission Statement
PTCB develops, maintains, promotes and administers a nationally
accredited certification program for pharmacy
technicians to enable the most effective support of
pharmacists to advance patient safety.
Certification Program Changes
New PTCB requirements:2015: PTCB only accepting technician‐specific CE
2020: Complete an ACPE/ASHP‐accredited education program ‐Pharmacy Technician Accreditation Commission (PTAC)
Advanced Certification Programs in DevelopmentTask force met in May for sterile compounding
Why 2020?
Changing pharmacy roles
Pharmacist
Technician
Clerk
National pharmacy organization input
ASHP PPMI
NABP Task Force on Technician Education
CREST Summit
2011 job analysis
Evolution of technician responsibilities
Knowledge domains
Revising the PTCE
Blueprint and item mapping
Gap analysis and new item development
Standard setting
PTCE Updated Blueprint

8/28/2015
24
Going in the Same Direction
Pharmacist provider status
Increased pharmacist access = increased care Telepharmacy, clinical team, immunizations
Increased clinical tasks Flu test, strep test, MTM
All non‐clinical tasks Tech‐check‐tech
National standard for pharmacy techniciansDefines minimally competent technician
ConclusionsPTCB requirements and ASHP Technician Training Program Standards are closely aligned
Still have 4 ½ years to grow technician training programs
Currently ASHP, ACPE and PTCB working with Chains to support training program development to meet the standards
We all support standardized education, training and certification of technicians and we will all have to work together to get there
In the new PGY1 residency standard, the number of goals and objectives has been
A. Reduced
B. Increased
C. Left the same
The number of graduates from pharmacy school is growing as fast as the number of residency programs
A. True
B. False
There are currently about _____ Accredited Technician Training Programs
A. 350
B. 275
C. 425
D. 500
The new PTAC commission is a collaboration between ASHP and ________
A. ACCP
B. APhA
C. ACPE
D. PTCB

8/28/2015
25
To sit for the PTCB exam in 2020, a technician will have to have what?
A. Worked in a pharmacy for 2 years
B. Completed and ASHP/ACPE accredited training program
C. Pay a fee of $200
D. Must be 18 years old
Questions?