Embed Size (px)
Citation preview
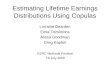
A mother presented to clinic concerned that herbaby developed “a red mark and bruising” onher cheek weeks after being born (Figure 1).The child is otherwise healthy. Diagnosisrevealed that this child has a strawberry heman-gioma, or hemangioma of infancy.
What is a strawberry hemangioma?Hemangiomas are the most common tumours ofinfancy, and usually are medically insignificant,although the cosmetic concern is often animportant issue with parents.
Thirty per cent of hemangiomas are presentat birth. The other 70% of them appear in thefirst several weeks of life. Fifty per cent ofhemangiomas complete involution by age 5,70% by age 7, and 90% by age 9. Hemangiomasthat take longer to involute have a higher inci-dence of permanent cutaneous changes thatinclude scar formation, telangiectasia, or redun-dant skin.
How do I know that it is a hemangioma?Hemangiomas are much more common inCaucasian infants (10% to 12%), and consider-ably less common in black (1.4%) and Asian(0.8%) infants. Females are more commonly
affected than males (3:1), and hemangiomas aremuch more common in preterm infants weigh-ing less than 1 kg (22% to 30%). Most cases areconsidered sporadic.
The earliest sign of a hemangioma is blanch-ing of the involved skin, often followed by finetelangiectases and then a red macule. Rapidgrowth during the neonatal period is the hall-mark of hemangiomas, occurring characteristi-cally beyond the growth rate of the infant.During involution, the hemangioma shrinkscentrifugally from the centre of the lesion. The
A Look at Dermatological Cases
Figure 1. Left cheek strawberry hemangioma in an infant.
The Canadian Journal of CME / November 2003 45
Photo Clinic
What is aStrawberry Hemangioma?Benjamin Barankin, MD

superficial lesions become less red, taking on aduskier purple color, and finally regaining nor-mal flesh tones (often referred to as “graying”).With involution, the hemangiomas become soft-er and more compressible with decreased ten-derness.
Radiographic investigation can include mag-netic resonance imaging to delineate the loca-tion and extent of both cutaneous and extracuta-neous hemangiomas, and to differentiate fromother high-flow vascular lesions. Ultrasound isoccasionally useful in differentiating heman-giomas from other deep dermal or subcutaneousstructures, such as cysts or lymph nodes. Plainradiography is of some use for evaluatinghemangiomas suspected of impinging on theairway. A carefully performed skin biopsy canbe helpful in distinguishing unusual or atypicalhemangiomas from other vascular lesions orneoplasms.
What treatments are available?The best approach in the non-complicatedpatient is the “wait and see,” and educateapproach. The best cosmetic result is most oftenfound when the hemangioma is allowed toresolve on its own without interference.Referral to a dermatologist or pediatric derma-tologist is often beneficial in terms of educa-tion, investigation, and treatment.
In patients in whom hemangiomas are ulcer-ated, painful, or in a location that has significantpsychological impact, lasers used by an experi-enced physician can hasten the resolution.Surgical excision of atrophic or hypertrophicskin, or of redundant skin is an option only inthe involuting phase to improve cosmesis.
To reduce morbidity and mortality in com-plicated hemangiomas, oral (preferred) andintralesional corticosteroids are effective atdecreasing the size of hemangiomas. Oral corti-costeroids should be administered during theproliferative phase, as they have only a negligi-ble effect on involuting hemangiomas. Becauseinterferon alfa-2a works by a different mecha-nism, it can be used in lesions that are unre-sponsive to steroids, and in fact should only beused after steroid failure. Unlike steroids, inter-feron alfa-2a does not have to be administeredduring the proliferation phase to be effective.The onset of action is slower, however, usuallyrequiring several weeks. This makes it lessattractive for use in acute life- or sight-threaten-ing situations.
Dr. Barankin is a dermatology resident atthe University of Alberta,Edmonton, Alberta.
48 The Canadian Journal of CME November 2003
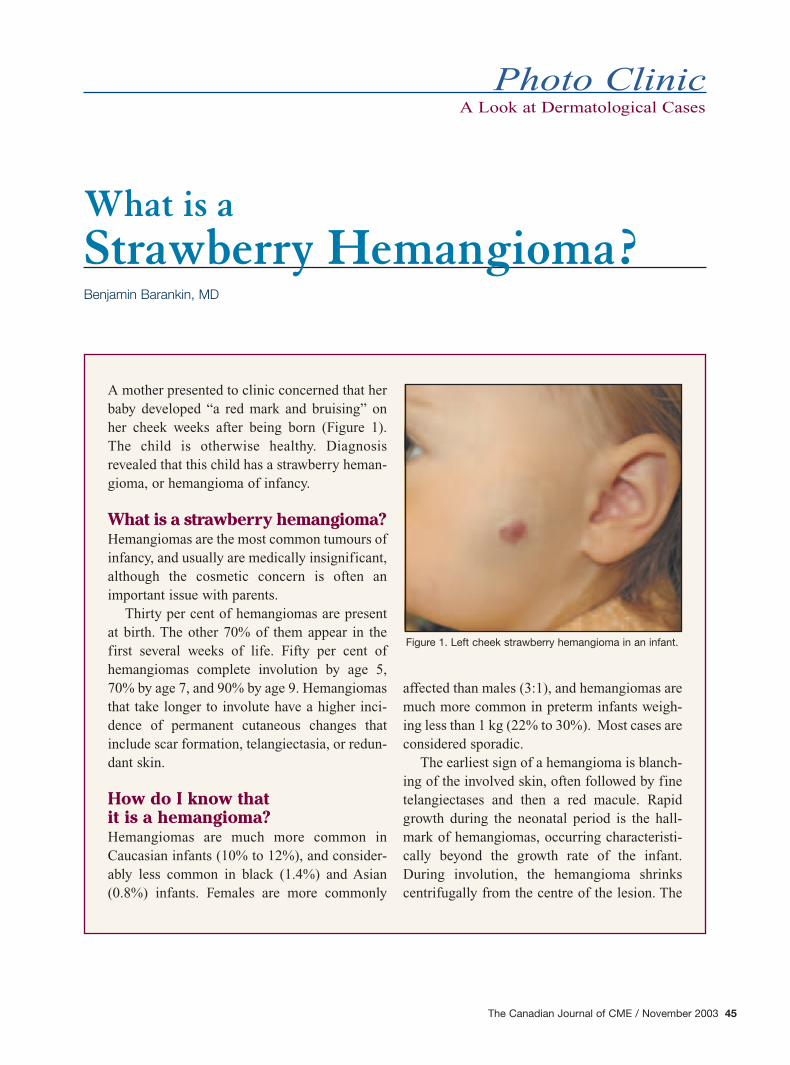
An eight-year-old boy and his mothercame into the clinic regarding papulesthat were developing on the boy’s chest,upper arms, and neck (Figure 1). Thesepapules were mildly pruritic, had beenpresent for two months, and newpapules were still appearing. Therewere no sick contacts, and the boy oth-erwise felt well.
What is your diagnosis?This patient has MolluscumContagiosum. This common conditionis caused by the molluscum contagio-sum virus (MCV), an unclassifiedmember of the poxviridae family,which is a benign and generally self-limited viral infection. Skin lesions usually con-sist of multiple dome-shaped, pink to skin-col-ored papules 2 mm to 6 mm in diameter, ofwhich some lesions show the classic feature ofumbilication. MC is usually asymptomatic,although individual lesions may be tender or pru-ritic.
What’s the cause?MC is encountered most commonly in childrenwho become infected through direct skin-to-skin contact, or indirect skin contact withfomites, as well as by auto-innoculation.
Papules on the Neck
Photo Clinic
Anti-inflammatory analgesic agent. Product Monograph available on request.General warnings for NSAIDs should be borne in mind.
CELEBREX® is a registered trademark of G.D. Searle & Co., used under permission by Pharmacia Canada Inc.
Family Tree
Figure 1. Multiple 2 mm to 4 mm slightly erythematous papules withcentral umbilication on the neck of a child.
50 The Canadian Journal of CME / November 2003
Lesions typically occur on the chest, arms,trunk, legs, and face. Mucous membraneinvolvement is quite rare, and palmoplantarskin is spared. Patients with atopic dermatitisare more prone to MC, and may develop largenumbers of lesions. Approximately 10% of allpatients will develop eczema around thelesions. In adults, MC is most commonly asexually transmitted disease (STD), and pre-sents as a few scattered lesions that are oftenlimited to the perineum, genitalia, innerthighs, lower abdomen, or buttocks. MC inhealthy children and adults is usually a self-limited disease, but may persist for severalmonths to a few years. Widespread, persistent,and atypical MC may occur in patients whoare significantly immunocompromised, orwho have acquired immunodeficiency syn-drome (AIDS) with low CD4 T-lymphocytecounts.
What is the main concern? For the most part, the main concern is tempo-rary adverse cosmetic results, and embarrass-ment. Most lesions resolve with no permanentresidual skin defect, however, occasionallesions may produce a slightly depressed scar,especially if excoriated.
How is it diagnosed?Diagnosis is usually clinical and based on thedistinctive central umbilication of the dome-shaped papule. If diagnosis is uncertain,papules can be biopsied, which gives a clas-sic histopathologic picture. Adult patientsshould be questioned about sexual historyand, where appropriate, evaluated for otherconcomitant STDs. Always consider testingfor HIV infection in patients with large orfacial lesions.
Patients and their families should be educat-ed as to the benign and self-limited nature ofthis condition, and that treatment is not anecessity.
Although treatment is not required, it canhelp reduce autoinoculation or transmission toclose contacts, and improve clinical appear-ance. More than one treatment session is fre-quently required.
In healthy children, a major goal is to limitdiscomfort, and benign-neglect or minordirect trauma is appropriate. Older childrencan better tolerate cryotherapy or curettage(can pre-apply EMLA), which is very effec-tive. For younger children, cantharidinapplied carefully by a physician to thelesions, can be effective. The lesions shouldbe taped over after the medication has been
CME
Photo ClinicLes défis sont différents,de même que les avantages.
Exercer la médecine familiale au sein desForces canadiennesvous offre unecarrière différente —en plus d’une primepouvant atteindre225 000 $*!
Cette indemnité de recrutementn’est qu’une façon de vousremercier de soigner lescitoyens d’élite de notre pays.Nous offrons également unerémunération, des avantages et des perspectives impression-nantes de perfectionnement.Vous développerez voscapacités de leader, et vousgagnerez de l’expérience dansde nombreuses sous-disciplines,y compris en soins intensifs, en médecine d’urgence, entrauma, en médecine d’aviationet de plongée, en médecinesportive, en hygiène profession-nelle, en médecine tropicale etbien plus encore.
Pour mieux connaître les défiset les avantages qui vousattendent à titre de médecinmilitaire, communiquez avec nous dès aujourd’hui.
*L’indemnité de recrutement estbasée sur l’engagement de quatreans d’un médecin de familleautorisé (minimum de 80 000 $pour un engagement de deux ans).
The challenges are different.So are the rewards.
Practising familymedicine with theCanadian Forcesoffers you a careerwith a difference—along with up to$225,000* inincentives!
A signing bonus is just oneway we’ll thank you for takingcare of our country’s finest.We also provide impressivecompensation, benefits andopportunities for professionaldevelopment. You’ll developyour leadership skills, as wellas gain expertise in a varietyof sub-disciplines includingacute care, emergencymedicine, trauma, aviationand diving medicine, sportsmedicine, occupationalhealth, tropical medicine and more.
To find out more about thechallenges and rewards thatawait you as a CanadianForces Medical Officer,contact us today.
*Signing bonus based on four-year undertaking for a licensedfamily physician (minimum$80,000 for a two-yearundertaking).
Strong. Proud. Today’s Canadian Forces.Découvrez vos forces dans les Forces canadiennes.
1 800 856-8488www.forces.gc.ca
applied. After 30 minutes to an hour, thetape should be removed and the lesionsshould be washed off. Similarly, tretinoincream applied daily, only to the lesions(with a toothpick), can be used. Moreexpensive, but very effective isImiquimod, a new topical immuneresponse modifier, which is a potentinducer of interferons.
In adults who are more motivated tohave their lesions treated, cryotherapy orcurettage of individual lesions is effectiveand well tolerated. In immunocompro-mised individuals, MC can be extensiveand difficult to treat. The goal may be totreat the most troublesome lesions only,such as on the face. In severe cases, thesepatients may warrant more aggressive ther-apy with lasers, imiquimod, optimized HIVantiviral therapy, or a combination ofapproaches.
What’s the prognosis?Prognosis is generally excellent becausethe disease usually is benign and self-limit-ed. In healthy patients, one to three treat-ments are usually effective.