Embed Size (px)
Citation preview

**What is your specialty?
• 1-Gynecologist (general)
• 2-Gynecologic oncologist
• 3-Surgical Oncologist
• 4-Radiation Oncologist
• 5-Medical Oncologist

Post-operative Cervical Ca35 yo
– Pap smear + ASCUS, HPV DNA+– Colposcopy/biopsy: invasive squamous
cell ca– Exam: no visible lesion– Radical hysterectomy with bilateral
complete lymphadenectomy– Final path: 2cm inv sq cell ca, extensive
LVI+, 1.5 cm deep stromal invasion– Staging: Chest X-ray, PET/CT, MRI
(optional < Stage IB1)

Post-operative Cervical caIntermediate Risk Factors
• Pelvic RT: EB 45 Gy– Prone, belly board– IMRT, supine– No VB necessary after a rad hyst (only
after a simple hyst)
• Concurrent chemotherapy: – weekly cis 40 mg/m2
RTOG trial: concurrent cisplatin, post-RT carbo/taxol x 4

Viswanathan ASTRO 11/3/09
Management of IB1: Radical Hysterectomy

Viswanathan ASTRO 11/3/09
Radiation or hysterectomy Landoni et al. Lancet 350: 535, 1997
• Randomized trial of 469 patients
• IB or IIA cervical cancer
• Median f/u: 87 months
• 54% of IB1 & 84% of IB2 surgical pts had adjuvant radiation for high risk features

Viswanathan ASTRO 11/3/09
Radiation or Hysterectomy
5 year OS DFS Rec tox
RT 83% 74% 25% 12%
Surgery 83% 74% 26% 28%
(p=0.0004)
SBO risk increased with LND

Viswanathan ASTRO 11/3/09
Post-operative RT : GOG 92Intermediate risk factors
• Indications (Sedlis et al. GOG92 Gynecol Oncol 73:177-183)
– LN+, LVI+– any 2 other factors including >1/3
stromal invasion, large tumor size

Viswanathan ASTRO 9/25/08
GOG 92 update IJROBP 65(1):169-176, 2006
• Median f/u 10 years• 46% reduction in risk
of recurrence (HR 0.54) – 42% reduction in risk of
progression/death– Reduction in adenoca
8.8% vs. 44%– 30% improvement in
overall survival (p=0.07)– Increases Grade 3/4
toxicity by 4.5% Upcoming RTOG trial

Viswanathan ASTRO 11/3/09
Post-op Chemo-RT: SWOG 8797High-risk patients
• + LN• + Margins• + Parametria• 4 yr PFS
– 63% vs. 80% (p=0.003)
• 4yr OS – 71% vs. 81%
(p=0.007)
Peters et al. JCO 2000Upcoming GOG trial

Other considerations for post op RT
– Close margins, 2x local recurrence rate
– Simple hysterectomy

Para-aortic node positive
• 45 yo, 4 cm exophytic, friable mass
• EUA: R sidewall extension, L parametrium +
• Biopsy: invasive squamous cell ca
• PET/CT: positive 2 cm LN level renal hilum
• Hematocrit 25, normal WBC, platelets, BUN/Cr, AST, ALT

PAN + Treatment
• Extended field RT
– 4F vs. IMRT– 45 Gy/1.8 Gy/fraction– IMRT Nodal boost 18-25 Gy w small bowel limit
5cc < 55 Gy; – 4F nodal boost limit 54Gy
• Concurrent weekly cisplatin 40 mg/m2 x 6 cycles (last inbetween brachy fractions)
• HDR: 5.5Gy x 5 fractions 3D planning; LDR: 40 Gy to point A

Common iliac node positive
• 28 yo known high risk HPV+
• Routine annual exam 4cm protuberant cvx
• Exam: L>R parametrial extension
• MRI: Bilateral parametrial extension, 1.5cm common iliac LN+
• PET: +uptake common iliac LN, no other LN involved
• FIGO Stage IIB

Common iliac LN+ Treatment
• Consider prophylactic coverage with an extended field
• IMRT para-aortics and full pelvic field (at least 3 cm margin on cervix and uterus)
• 45 Gy entire field• Nodal boost IMRT + 18 Gy = 63 Gy • Concurrent weekly cisplatin 40 mg/m2 x 6 • HDR Brachytherapy 5.5Gy x 5 3D

Stage IB1
• 72 yo w vaginal spotting
• Exam: 5mm red polyp at os, firm cervix, no PM extension
• MRI: 10 cm fibroid uterus, tumor extending along endocervical canal, tumor 3 cm height, 2cm width
• Biopsy: endocervical adenocarcinoma

Stage IB1
• Options: Radical Hysterectomy (robotic) with complete lymphadenectomy, but….
• Post-op EBRT: toxicity increases
• External beam radiation with concurrent chemotherapy (no hyst) best option
• Followed by brachytherapy

Vulvar Carcinoma Case
• 50 yo with long hx of lichen sclerosus
• 6 month hx of scant bleeding
• Seen for year exam• Bx mod differentiated
squamous cell ca
• Physical exam reveals right inguinal node 2.5 cm

**You would recommend:
1- Obtain PET/CT to assess disease extent and distant metastatic disease
2- Send immediately for radiation +/- chemo treatment
3- Aspirate enlarged node
4- Proceed directly to radical surgery
5- Initiate Aldara cream

Preop Workup
• CT/PET: High FDG uptake in right vulva, right inguinal node and lesser FDG uptake in nodes bilaterally in groin

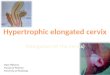
PET

Vulvar cancer.
McMahon C J et al. Radiology 2010;254:31-46
©2009 by Radiological Society of North America
MRI

Surgical Approach and final pathology
• Bilateral inguinal dissection with removal of enlarged lymph nodes
• Partial radical vulvectomy with removal of clitoris and upper vulva (bilateral)
• Pathology: 2.5 cm moderately differentiated squamous cell ca invasive, closest margin 4mm to urethra, + LVI, Right inguinal node (1)/3 positive, 0/5 Left inguinal

**For the next step, you would recommend:
1- Re-excise close margin
2- Send for radiation therapy alone
3- Give chemotherapy with radiation therapy
4- Follow patient for recurrence
5- Refer to urologist

Vaginal cancer
• 65 yo hysterectomy for benign fibroids 20ya
• No pap smears for 20 years
• Vaginal spotting
• Exam: friable mass upper L fornix extending to L introius @6cm
• Biopsy: invasive squamous cell carcinoma