Embed Size (px)
DESCRIPTION
Meropenem
Citation preview

Intensive Care MedDOI 10.1007/s00134-008-1034-7 BRIEF REPORT
Julia LanggartnerAntje VasoldThomas GlückMichel RengFrieder Kees
Pharmacokinetics of meropenem duringintermittent and continuous intravenousapplication in patients treated by continuousrenal replacement therapy
Received: 20 September 2007Accepted: 24 December 2007
© Springer-Verlag 2008
The authors wrote this article in cooperationwith the TAHI section of the ESICM.
J. Langgartner (�) · A. VasoldUniversity of Regensburg, Departmentof Internal Medicine I,93042 Regensburg, Germanye-mail:[email protected]
T. GlückGeneral Hospital Traunstein, Departmentof Internal Medicine,Postfach 1820, 83276 Traunstein, Germany
M. RengGeneral Hospital Bogen, Departmentof Internal Medicine,Mussinanstr. 8, 94327 Bogen, Germany
F. KeesUniversity of Regensburg, Departmentof Pharmacology,93053 Regensburg, Germany
Abstract Objective: The clinicaleffect of beta-lactam antibioticsdepends on the time of drug concen-tration above the minimal inhibitoryconcentration (MIC) for a susceptiblebacterium. Continuous infusion (CI)of ß-lactams such as meropenemmay therefore be a more rationalapproach than intermittent bolusinjections (IB). The aim of thisstudy was to test whether CI ofmeropenem achieves effective drugconcentrations comparable to IBin patients treated by continuousrenal replacement therapy (CRRT).Design: Prospective, randomisedcross-over study. Setting: Twelve-bed medical intensive care unit(ICU). Patients and interventions:Six ICU patients were randomisedto receive either meropenem 1 g IBevery 12 h or a 0.5 g i.v. loading dosefollowed by 2 g i.v. CI over 24 h.After 2 days, regimens were crossedover. Meropenem pharmacokineticswere determined on days 2 and 4.Measurements and results: Peakserum concentration [median (25%
and 75% quartiles)] after shortinfusion of 1 g meropenem were 62.8(51.4; 85.0) mg/l, trough levels at12 h were 8.1 (4.5; 18.7) mg/l, andserum half-life was 5.3 (5.1; 7.0) h.Steady-state concentrations duringCI were 18.6 (13.3; 24.5) mg/l. TheAUCs during either treatment werecomparable and determined as 233(202; 254) mg/l*h (IB) and 227 (182;283) mg/l*h (CI), respectively. Fourhours after IB, drug concentrationsdropped below CI steady-stateconcentrations. Conclusion: Appro-priate antibacterial concentrations ofmeropenem in patients with CRRTare easily achievable with CI. CI maybe an effective alternative dosingregimen to IB. A prospective com-parison of the clinical efficacy of thetwo dosage regimens is warranted.
Keywords Meropenem · Beta-lactamantibiotics · Continuous infusion ·Pharmacokinetics · CVVHD · Renalreplacement therapy · Pharmacody-namics
Introduction
Antimicrobial agents such as aminoglycosides and fluoro-quinolones exhibit a concentration-dependent activity.Their antibacterial effect is related to their peak con-centrations. By contrast the clinical effect of ß-lactamantibiotics depends on the time of drug concentrationabove the minimal inhibitory concentration (MIC) fora susceptible bacterium. ß-Lactams achieve maximum
bacterial killing at concentrations 4–5 times the MIC forthe microorganism and exhibit no or only a minimumpost-antibiotic effect [1–4]. Further elevation of drugconcentration does not improve antibacterial activity [5].Intermittent administration of a drug leads to high peakand low trough serum concentrations; the latter may fallbelow the MIC for the microorganism during the dosinginterval. Continuous i.v. infusion (CI) produces a constantconcentration of the antibiotic, thereby optimising the

pharmacodynamic characteristics of the ß-lactam antibi-otics. This has led to reconsideration of CI of ß-lactamantibiotics as a potentially valuable approach [2, 6, 7],provided that doses sufficient to reach concentrationsseveral times above the MIC are chosen.
Meropenem is a ß-lactam antibiotic. Because of theshort half-life of meropenem, necessitating frequent dos-ing in intermittent bolus (IB) regimens, it is considered anexcellent candidate for application by CI.
On pharmacokinetic considerations, especially critic-ally ill patients with continuous renal replacement therapy(CRRT) would benefit from a continuous administration ofß-lactam antibiotics.
Therefore, the aim of this study was to test whetherCI of meropenem achieves effective drug concentrationscomparable to IB in patients with renal failure treated byCRRT.
Some of the data were presented at the World Con-ference of Magic Bullets, held in Nuremberg, Germanyin September 2004 in celebration of the 150th anniver-sary of Paul Ehrlich’s birth (abstract book Nr. 241, A-61;http://www.ehrlich2004.org).
Material and methods
Patients
Patients who were admitted to the medical intensive careunit of the University Hospital of Regensburg, Germany,were eligible for enrolment into the study if they metthe following criteria: (1) suspected infection warrantingantibiotic therapy; (2) suspected pathogen presumablysusceptible to meropenem, according to standard criteriafor empirical antimicrobial therapy for critically ill pa-tients; (3) age at least 18 years; (4) i.v. antibiotic treatmentof the infection expected to be necessary for more than 4days; (5) renal failure with indication for CRRT.
Patients were excluded if they had documentedor presumed hypersensitivity to meropenem or peni-cillins. Switch to an alternative regimen at any timewas left to the discretion of the attending physician incharge, if microbiological results or other informationindicated that therapy with meropenem was no longeradequate.
The patients’ demographic data of the patients wererecorded. Daily data collection included peak body tem-perature, leucocyte count, serum urea nitrogen, and creati-nine.
Renal replacement therapy
Vascular access was obtained by insertion of a double-lumen dialysis catheter. Each patient was dialysed,using a Fresenius Multifiltrate dialysis monitor (Frese-
nius Medical Care, Bad Homburg, Germany). Continuoushaemodiafiltration (CVVHD) was performed using a high-flux polysulfone capillary haemofilter with a membranesurface area of 1.4 m2 (Ultraflux® AV600S; FreseniusMedical Care). NaBic substitution fluid was reinfused. Thestandard blood flow rate in the dialyser was 150 ml/min.The ultrafiltrate pump rate was adjusted to 25 ml/kgBW/h.
Study design
This prospective study was conducted in a randomised,cross-over design. The patients received meropenemeither as 0.5 g i.v. loading dose followed by 2 g CI per 24 hdivided in two 1 g fractions or as a 1 g IB over 15–20 minadministered every 12 h. IB or CI was continued for 2days, then patients were crossed over to the other treat-ment for another 2 days. At days 2 and 4 of the studypharmacokinetic analyses were performed. Thereafter,therapy was continued by standard intermittent dosing.
The study protocol was approved by the ethics commit-tee of the University of Regensburg.
Drug administration and sampling
All patients received meropenem (Meronem®; AstraZeneca, Germany), which was reconstituted according tothe manufacturer’s instructions. The solutions were givenvia an infusion pump.
Blood samples (3–4 ml) were obtained immediatelyprior to the start of dosing on days 2 and 4 (time 0), and at20 min (the end of short infusion) and 1, 2, 3, 4, 6, 8, 10and 12 h thereafter. All blood samples were drawn fromindwelling arterial catheters. The blood was centrifuged(2.500 g for 10 min), and serum separated immediately.Similarly, aliquots of dialysate collected from timedfractionated collection bags were taken. All samples werekept at –80 °C until assayed.
Analytical methods
Meropenem was determined by means of an adaptedhigh-performance liquid chromatographic (HPLC)method [8]. Meropenem eluted after 5.4–5.8 min (flowrate of 1.0 ml/min). The lower limit of detection was300 pg meropenem injected.
To prove the stability of meropenem in the infusionsolution, 1 g meropenem was dissolved in 100 ml saline,and an aliquot of 3 ml was incubated at 25.0 °C up to 24 hin the autosampler of the HPLC apparatus. Aliquots wereinjected automatically onto the column at intervals of0.5–1 h and assayed for meropenem.

Pharmacokinetic analysis
Pharmacokinetic parameters were determined by non-compartmental analysis. The area under the curve duringone dosing interval (AUCt) was estimated by the linear-trapezoidal rule. The total clearance (CL) was then derivedas CL = D/AUCt (l/h) where D is the administered doseof 1.0 g. The apparent terminal elimination rate constant(λz) was determined by log-linear least squares regressionanalysis of the serum concentrations from 2 h post doseuntil the end of the dosing interval. The elimination half-life (t1/2) and the terminal volume of distribution (Vz) werecalculated as t1/2 = ln(2)/λz (h) and Vz = CL/λz (l). Thesieving coefficient Sc was calculated as Sc = CUF/CS, withCUF being the concentration of meropenem in ultrafiltrate(CUF) and Cs the concomitant serum concentration. Thepercentage of time with a meropenem concentration abovea MIC (%(T)>MIC) of 4 mg/l and 8 mg/l, respectively,was extrapolated from serological measurements.
Statistical analysis
Values are reported as median and interquartile range.
Results
Patient demographics
11 patients were enrolled into the study. Five of these werewithdrawn for different reasons: one patient died duringthe study, in one patient antibiotic therapy was changed,and in three patients CVVHD was interrupted due torapidly improving renal function. Two of the six evaluatedpatients (five males, one female) died in the further courseof ICU treatment (Table 1). No adverse event related to the
Table 2 Pharmacokinetic parameters of meropenem in six patients during CVVHD following bolus infusion or continuous infusion of 1.0 gmeropenem q12 h
Patient Bolus infusion Continuous infusionCmax Cmin %(T) %(T) t1/2 CL Vz Sc Cmax Cmin Cmedian %(T) %(T) CL Scmg/l mg/l >8 mg/l >4 mg/l h l/h L mg/l mg/l mg/l >8 mg/l >4 mg/l l/h
1 90.6 18.7 54.7 75.6 7.5 2.60 28.1 0.41 18.8 12.0 13.3 1.0 1.0 5.93 0.772 92.3 8.1 49.2 72.1 5.5 3.91 31.0 1.02 26.5 22.8 25.4 1.0 1.0 3.34 1.013 49.4 4.5 32.1 53.8 5.2 6.68 50.1 0.92 10.2 6.5 9.8 0.83 1.0 9.20 0.724 41.9 10.8 64.6 95.8 7.5 3.99 43.0 0.86 56.8 17.0 22.7 1.0 1.0 2.99 0.915 57.4 8.2 42.5 63.8 5.0 4.66 33.7 1.08 20.0 14.4 18.7 1.0 1.0 4.53 0.936 68.3 4.0 25.0 47.5 3.4 5.05 25.0 1.06 20.0 19.0 19.6 1.0 1.0 4.27 0.87Median 62.8 8.2 45.9 67.9 5.3 4.32 32.3 0.97 20.0 15.7 19.1 1.0 1.0 4.40 0.8925% 51.4 5.4 34.7 56.3 5.1 3.93 28.9 0.87 19.1 12.6 14.6 1.0 1.0 3.58 0.7975% 85.0 10.1 53.3 74.7 7.0 4.96 40.7 1.05 24.8 18.5 23.6 1.0 1.0 5.58 0.93
Cmax , peak concentration; Cmin , trough concentration; individual Cmedian , median concentration during continuous infusion; %(T), percent-age of time with meropenem concentration above MIC; t1/2, terminal half-life; CL, total clearance from serum; Vz, volume of distribution;Sc, sieving coefficient
Table 1 Demographic data of patients
Patient Age Sex Size Weight Main diagnosis Outcome(years) (cm) (kg)
1 50 M 175 70 Pneumonia and Survivedsepsis
2 51 F 160 55 Acute pancreatitis Survived3 65 M 180 95 Pneumonia and Survived
sepsis4 56 M 170 90 Sepsis Died5 42 M 175 60 Sepsis Died6 58 M 180 86 Pneumonia Survived
study drug was observed in any patient during the studyperiod.
Stability of meropenem solution
Seven per cent loss of concentration of meropenem infu-sion solution (10 mg/ml) at room temperature (25 °C) wasobserved after 12 h and 10% loss after 17 h.
Pharmacokinetic parameters
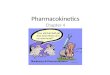
After 4–5 h median drug concentrations were higher in theCI than in the IB regimen (Fig. 1). The median peak con-centration of meropenem was 62.8 mg/l at the end of IBand decreased to 8.2 mg/l at the end of the 12-h dosing in-terval with a median serum half-life of 5.3 h (Table 2). Themedian volume of distribution was 32 l (range 25–50 l).During CI the lowest serum concentration measured at anytime in any patient was 6.5 mg/l and the highest concentra-tion 56.8 mg/l. The %(T)>MIC at 4 mg/l and 8 mg/l washigher for CI than for IB. The median serum concentrationin the patients over the dosing interval was 19.1 mg/l. Me-dian total clearance was 4.3 l/h (IB) vs 4.4 l/h (CI), and thesieving coefficient was 0.97 (IB) vs 0.89 (CI).

Fig. 1 Steady-state serumconcentrations of meropenem insix patients during CVVHDfollowing 1 g meropenem b.i.d.as bolus infusion (a) or ascontinuous infusion (b)
Discussion
Meropenem is a carbapenem with a broad spectrum of ac-tivity against Gram-positive and Gram-negative bacteria.It is often used for the treatment of nosocomial infectionsand sepsis in critical care units. As ß-lactam antibiotics ex-hibit time-dependent bacterial killing, time above MIC isthe parameter that correlates best with clinical efficacy [6].Therefore, CI appears to be a particularly attractive optionfor parenterally administered ß-lactam antibiotics such asmeropenem.
Meropenem is primarily eliminated renally, so dosageadjustment is necessary in patients with impaired renalfunction. In patients with renal failure and CRRT, correctdosing of antibiotics is very difficult. Several factors thatare dependent on the particular modality of CRRT have tobe considered. In these patients, underdosing causing in-effective antimicrobial therapy is a more frequent problemthan the risk of toxicity due to overdosed antibiotics. Frompharmacokinetic considerations, patients with CRRT inparticular would benefit from CI of ß-lactam antibiotics.
A prerequisite for CI is sufficient stability of the drugsin solution at room temperature. In good agreement withprevious studies [9–12] we demonstrated that meropenemis sufficiently stable in the infusion solution at 25 °Cfor 12 h with a loss of concentration of 7%. Therefore,the 2 g i.v. CI in 24 h was divided into two 1-g fractions.The only study reporting different findings on the stabilityof antipseudomonal ß-lactams was published by Viaeneet al. [13]. We could not confirm that meropenem istoo unstable to be recommended for CI dosing in anair-conditioned ICU setting. For tropical countries withoutair conditioning Jaruratanasirikul et al. showed a lossof concentration of meropenem at room temperature(32–37 °C) of 12% after 8 h [9].
In general, few data are available on meropenem andCRRT. Most of the published studies evaluated pharma-cokinetic parameters of meropenem in patients with acuterenal failure on continuous veno-venous haemofiltration(CVVHF) or continuous veno-venous haemodiafiltra-tion (CVVHD) [14–24]. The peak concentrations of
meropenem differ significantly among these studies. Also,the half-life during CVVHF ranges from 2.46 h in thestudy by Thalhammer et al. [19] to 7.5 h in the study byValtonen et al. [15]. The reason may be the different ultra-filtration flow rates used in these two studies. Accordingly,recommendations for dosage adjustments for meropenemfor patients with CRRT range between 0.5 g twice dailyand 1 g every 8 h. No studies have been published on thepharmacokinetic parameters of meropenem in patients onCVVHD.
The main objectives of this study were to investigatethe pharmacokinetics of CI compared to IB administra-tion of meropenem in ICU patients on CVVHD, and todetermine the applicability of CI in this special condition.In order to shorten the time necessary to reach effectiveantibacterial serum concentrations and to improve treat-ment success, we chose a loading dose of 0.5 g meropenembefore initiation of CI. During the whole period of CI,antibiotic serum concentrations were high enough to pro-vide sufficient antibacterial activity at a MIC of 4 mg/l andeven 8 mg/l of meropenem. In IB, there was a drop be-low the MIC in most patients. The %(T)>MIC is higher atCI than at IB. Hence, theoretically, CI should be a moresuitable application mode for meropenem than IB. Me-dian half-life, volume of distribution and total clearance ofmeropenem at CI in our patients were in good agreementwith published data [15, 18–24].
Pseudomonas aeruginosa is a common, difficult totreat bacterium that often causes infections in critically illpatients. To cover intermediately resistant P. aeruginosastains with a MIC of 8 mg/l, a mean meropenem concen-tration of at least 12 mg/l is desired. Our pharmacokineticparameters during IB dosing show a median Cmax of63 mg/l and a Cmin of 8.2 mg/l at the end of the dosinginterval. Accordingly, 1.0 g meropenem every 12 h forpatients during CVVHD can be recommended if thesame CVVHD parameters are used. However, our datacannot easily be transferred to other CVVHD settingsor even other modes of renal replacement therapy. Inaddition, more data on the influence of patient-dependentparameters (e.g. weight, ethnic background) are desir-

able. Therefore, further investigations are necessary toevaluate the clinical efficacy of both dosing regimens.Until then therapeutic drug monitoring may be usefulin this subset of patients to obtain optimal meropenemconcentrations.
ConclusionsCI of meropenem can achieve serum concentrationssufficient for the treatment of various bacterial infections.Our data suggest that CI allows a safe and effective anti-
bacterial therapy in ICU patients similar to IB, with serumconcentrations well above the MIC for most pathogens. InCI, a loading dose of 0.5 g of meropenem is recommendedto obtain bactericidal drug concentrations as quickly aspossible. Prospective studies are warranted to comparethe clinical efficacy of CI and IB regimens in patients onCVVHD.
Acknowledgements. Thanks to Carl Waldman for his stimulatingcomments on our work.
This work was supported by a grant from AstraZeneca for phar-macokinetic analysis.
References
1. Craig WA, Ebert SC (1990) Killing andregrowth of bacteria in vitro: a review.Scand J Infect Dis Suppl 74:63–70
2. Craig WA, Ebert SC (1992) Continu-ous infusion of beta-lactam antibi-otics. Antimicrob Agents Chemother36:2577–2583
3. Turnidge JD (1998) The pharmacody-namics of beta-lactams. Clin Infect Dis27:10–22
4. Vogelman B, Craig WA (1986) Kineticsof antimicrobial activity. J Pediatr108:835–840
5. Craig WA (1998) Pharmacokinet-ic/pharmacodynamic parameters:rationale for antibacterial dosing ofmice and men. Clin Infect Dis 26:1–10;quiz 11–12
6. Nicolau DP (2001) Predicting antibac-terial response from pharmacodynamicand pharmacokinetic profiles. Infection29 Suppl 2:11–15
7. Nicolau DP, Nightingale CH, Banevi-cius MA, Fu Q, Quintiliani R (1996)Serum bactericidal activity of cef-tazidime: continuous infusion versusintermittent injections. AntimicrobAgents Chemother 40:61–64
8. Elkhaili H, Niedergang S, Pompei D,Linger L, Leveque D, Jehl F (1996)High-performance liquid chromato-graphic assay for meropenem in serum.J Chromatogr B 686:19–26
9. Jaruratanasirikul S, Sriwiriyajan S(2003) Stability of meropenem innormal saline solution after storageat room temperature. Southeast AsianJ Trop Med Public Health 34:627–629
10. Takeuchi Y, Takebayashi Y, Suna-gawa M, Isobe Y, Hamazume Y,Uemura A, Noguchi T (1993) The sta-bility of a novel carbapenem antibiotic,meropenem (SM-7338), in a solid stateformulation for injection. Chem PharmBull (Tokyo) 41:1998–2002
11. Patel PR, Cook SE (1997) Stability ofmeropenem in intravenous solutions.Am J Health Syst Pharm 54:412–421
12. Kuti JL, Nightingale CH, Knauft RFNicolau DP (2004) Pharmacokineticproperties and stability of continuous-infusion meropenem in adults withcystic fibrosis. Clin Ther 26:493–501
13. Viaene E, Chanteux H, Servais H,Mingeot-Leclercq MP, Tulkens PM(2002) Comparative stability studiesof antipseudomonal beta-lactamsfor potential administration throughportable elastomeric pumps (hometherapy for cystic fibrosis patients) andmotor-operated syringes (intensive careunits). Antimicrob Agents Chemother46:2327–2332
14. Ververs TF, van Dijk A, Vinks SA,Blankestijn PJ, Savelkoul JF, Meu-lenbelt J, Boereboom FT (2000)Pharmacokinetics and dosing regi-men of meropenem in critically illpatients receiving continuous veno-venous hemofiltration. Crit Care Med28:3412–3416
15. Valtonen M, Tiula E, Backman JT,Neuvonen PJ (2000) Eliminationof meropenem during continuousveno-venous haemofiltration andhaemodiafiltration in patients withacute renal failure. J AntimicrobChemother 45:701–704
16. Krueger WA, Neeser G, Schus-ter H, Schroeder TH, Hoffmann E,Heininger A, Dieterich HJ, Forst H,Unertl KE (2003) Correlation ofmeropenem plasma levels with pharma-codynamic requirements in criticallyill patients receiving continuous veno-venous hemofiltration. Chemotherapy49:280–286
17. Thalhammer F, Traunmuller F, ElMenyawi I, Frass M, Hollenstein UM,Locker GJ, Stoiser B, Staudinger T,Thalhammer-Scherrer R, Burgmann H(1999) Continuous infusion versus in-termittent administration of meropenemin critically ill patients. J AntimicrobChemother 43:523–527
18. Tegeder I, Neumann F, Bremer F,Brune K, Lötsch J, Geisslinger G (1999)Pharmacokinetics of meropenem incritically ill patients with acute renalfailure undergoing continuous veno-venous hemofiltration. Clin PharmacolTher 65:50–57
19. Thalhammer F, Schenk P, Burgmann H,El Menyawi I, Hollenstein UM,Rosenkranz AR, Sunder-Plassmann G,Breyer S, Ratheiser K (1998) Single-dose pharmacokinetics of meropenemduring continuous venovenous hemofil-tration. Antimicrob Agents Chemother42:2417–2420
20. Krueger WA, Schroeder TH, Hutchi-son M, Hoffmann E, Dieterich HJ,Heininger A, Erley C, Wehrle A,Unertl K (1998) Pharmacokinetics ofmeropenem in critically ill patients withacute renal failure treated by continuoushemodiafiltration. Antimicrob AgentsChemother 42:2421–2424

21. Giles LJ, Jennings AC, Thomson AH,Creed G, Beale RJ, McLuckie A (2000)Pharmacokinetics of meropenem inintensive care unit patients receivingcontinuous veno-venous hemofiltrationor hemodiafiltration. Crit Care Med28:632–637
22. Meyer MM, Munar MY, Kohlhepp SJ,Bryant RE (1999) Meropenem phar-macokinetics in a patient with multi-organ failure from meningococcemiaundergoing continuous venovenoushemodiafiltration. Am J Kidney Dis33:790–795
23. Kuti JL, Nicolau DP (2005) Derivationof meropenem dosage in patientsreceiving continuous veno-venoushemofiltration based on pharmacody-namic target attainment. Chemotherapy51:211–216
24. Robatel C, Decosterd L A, Biollaz J,Eckert P, Schaller MD, Buclin T (2003)Pharmacokinetics and dosage adapta-tion of meropenem during continuousvenovenous hemodiafiltration in crit-ically ill patients. J Clin Pharmacol43:1329–1340