Embed Size (px)
Citation preview
Conference Name: Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Scheduled Conference Date: Wednesday, March 12th , 2003
Scheduled Conference Time: 1:00 p.m.–2:30 p.m. (Eastern), 12:00 p.m.–1:30 p.m. (Central), 11:00 a.m.– 12:30 p.m. (Mountain),10:00 a.m.–11:30 a.m (Pacific); 9:00 am - 10:30 am ADT (Alaska); 8:00 am - 9:30 am H/AST (Hawaii-Aleutian)
Scheduled Conference Duration: 90 Minutes
PLEASE NOTE: If the audioconference occurs April through October, the time reflects daylight savings. If your area doesNOT observe Daylight Savings, times will be one hour earlier.
Your registration entitles you to: ONE telephone connection to the audioconference. Invite as many people as you wish to listen to the audioconference on your speakerphone.
Permission is given to make copies of the written materials for anyone else who is listening.
In order to avoid delays in connecting to the conference, we recommend that you dial into the audioconference 15 minutes prior to the start time
Dial-In Instructions:1. Dial 1-973-321-1030 and follow the voice prompts.2. You will be greeted by an operator3. Give the operator your pass code 031203 and the last name of the person who registered for the audioconference.4. The operator will then verify the name of your facility.5. You will then be placed into the conference.
Technical Difficulties1. If you experience any difficulties with the dial-in process, please call the Conference Center reservation line at
973-633-8500.2. If you should need technical assistance during the audio portion of the program, please press the * key followed by
the 0 key on your touch-tone phone and an operator will assist you. If you are disconnected during the conference, dial973-633-8500.
Q&A Session1. To enter the questioning queue during the Q&A session, callers need to push the 1 key followed by the 4 key on their
touch-tone phones. Note: This portion of the program generally falls after the first hour of presentation. Please do nottry to enter the queue before this portion of the program.
2. If you prefer not to ask your question on the air, you can fax your question to 1-877-865-4210 or 1-973-237-3904.(Please note: You can only fax your question during the program.)
Prior to the programIf you prefer not to ask your question on the air, you can send your questions via email to [email protected]. Cutoff dateand time for questions: 03/11/03 @ 5:30 PM EST. Please note that not all questions will be answered.
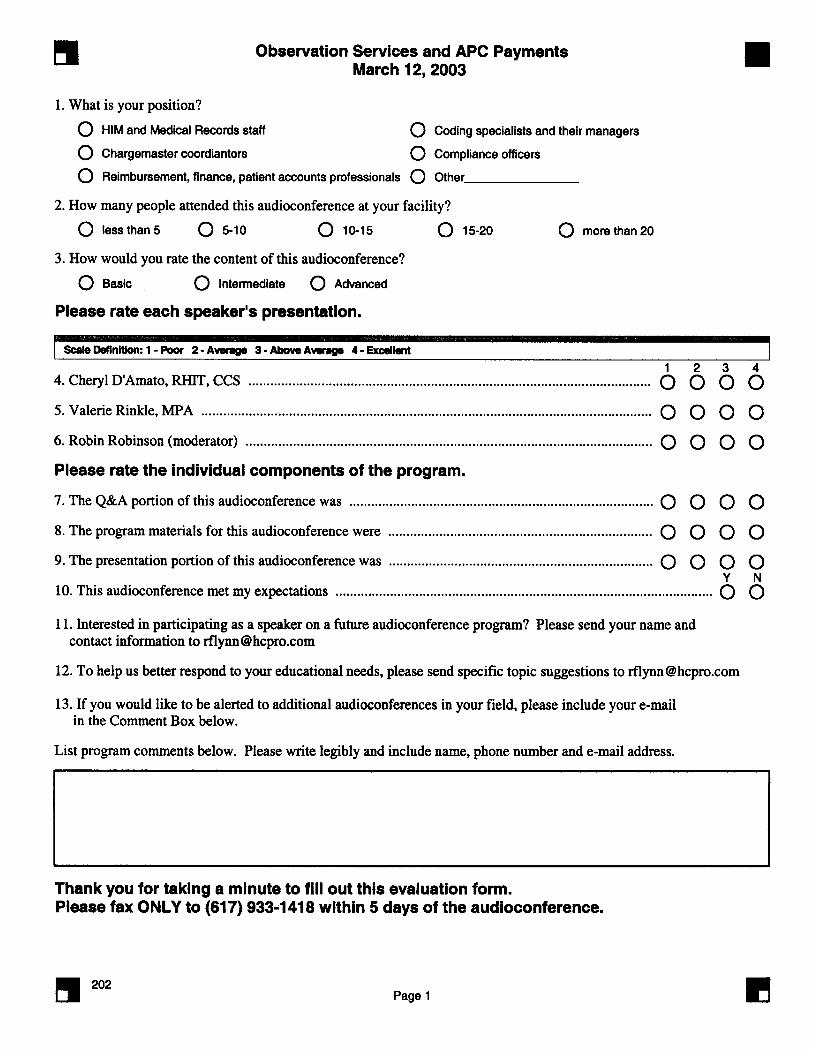
Evaluation FormAt the conclusion of the program, please return the evaluation form included with the materials package by fax to the num-ber at the bottom of the evaluation form. If you downloaded your materials from the Internet, please print the evaluationform and fax it to the number on the bottom of the evaluation form.
CEU attendance documentation form Please note: (1) If there is an attendance documentation form attached to the packet, that form must have the names ofthe participants in order to receive continuing education credit. (2) If the packet DOES NOT contain attendance documenta-tion form, please use the certificate as proof to receive credit. (3) If the packet only contains a certificate but there are nohours of credit on the certificate, HCPro, Inc didn’t apply for credit for this program. FAX OR MAIL THE ATTENDANCE DOCU-MENTATION FORM TO the address or fax number listed on the form.
Dial-In Instructions

hcProhcPro
Observation Services and APCPayments: Key Coding and
Billing Changes for 2003
Wednesday, March 12, 2003
1:00 p.m.–2:30 p.m. (Eastern)
12:00 p.m.–1:30 p.m. (Central)
11:00 a.m.–12:30 p.m. (Mountain)
10:00 a.m.–11:30 a.m. (Pacific)
presents . . .

ii Observation Services and APC Payments: Key Coding and Billing Changes for 2003
In our materials we strive to provide our audience with useful, timely information. The live audioconference willfollow the enclosed agenda. Occasionally our speakers will refer to the materials enclosed. We have noticed thatother non-HCPro audioconference materials follow the speaker’s presentation bullet-by-bullet, page-by-page.Because our presentations are less rigid and rely more on speaker interaction, we do not include each speaker’sentire presentation. The materials contain helpful forms, crosswalks, policies, charts, and graphs. We hope that youfind this information useful in the future.
iiiObservation Services and APC Payments: Key Coding and Billing Changes for 2003
The “Observation Services and APC Payments: Key Coding and Billing Changes for 2003” audioconferencematerials package is published by HCPro, Inc., 200 Hoods Lane, P.O. Box 1168, Marblehead, MA 01945.
Copyright 2003, HCPro.
Attendance at the audioconference is restricted to employees, consultants and members of the medical staff of theLicensee.
The audioconference materials are intended solely for use in conjunction with the associated HCPro audioconfer-ence. Licensee may make copies of these materials for your internal use by attendees of the audioconference only.All such copies must bear this legend. Dissemination of any information in these materials or the Audioconferenceto any party other than the Licensee or its employees is strictly prohibited.
Advice given is general, and attendees and readers of the materials should consult professional counsel for specificlegal, ethical, or clinical questions. HCPro is not affiliated in any way with the Joint Commission on Accreditationof Healthcare Organizations, which owns the JCAHO trademark.
For more information, contact:
HCPro200 Hoods LaneP.O. Box 1168Marblehead, MA 01945Telephone: 800/575-6787Fax: 781/639-0179E-mail: [email protected]: www.hcpro.com
hcPro
iv Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Dear colleague,
Thank you for participating in our “Observation Services and APCPayments: Key Coding and Billing Changes for 2003” audioconference withCheryl D’Amato, RHIT, CCS, and Valerie Rinkle, MPA. We are excitedabout the opportunity to interact with you directly and encourage you to takeadvantage of the opportunity to ask our experts your questions during theaudioconference. If you would like to submit a question before the audiocon-ference, please send it to [email protected] and provide the program date inthe subject line. We cannot guarantee your question will be answered duringthe program, but we will do our best to take a good cross section of questions.
If at any time you have comments, suggestions, or ideas about how we mightimprove our audioconference, or if you have any questions about the audio-conference itself, please do not hesitate to contact me. And if you would likeany additional information about other products and services, please contactour Customer Service Department at 800/575-6787.
Along with these audioconference materials, we have enclosed a fax evalua-tion. We value your opinion. After the audioconference, please take a minuteto complete the evaluation to let us know what you think.
Thanks again for working with us.
Best regards,
Siva CoffeyAudio / Web Conference CoordinatorFax: 781/639-0179E-mail: [email protected]
hcPro200 Hoods LaneP.O. Box 1168
Marblehead, MA 01945Tel: 800/650-6787Fax: 800/639-8511
vObservation Services and APC Payments: Key Coding and Billing Changes for 2003
Table of contents
Agenda . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .vi
About your sponsors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .vii
Speaker profiles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .viii
Exhibit A . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1Presentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2
Exhibit B . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21 Articles from HCPro, Inc:• Documentation key in establishing medical necessity for observation . 22• Physician documentation drive observation payment . . . . . . . . . . . . . 23
Resources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Certificate of attendance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
vi Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Agenda
Observation ServicesRequired ICD-9-CM Codes Criteria for Separate APC Observation Payment Coding and Billing Requirements for Observation APCDocumentation Requirements for Observation APCRequired Diagnostic Tests for Observation APCDocumentation Requirements for APC Observation - Risk StratificationDocumentationBilling Other Observation ServicesOther Issues to considerLive Q&A
viiObservation Services and APC Payments: Key Coding and Billing Changes for 2003
About HCProHCPro is the premier health care information and resource provider on compliance and regulatory issues faced byhospitals, home health organizations, nursing homes, physicians’ offices and other health care facilities. HCPro haslaunched a number of Web “supersites” that include tips, how-to information, Ask the Expert columns, free e-mailnewsletters, and so much more.
Briefings on APCsCreated exclusively for HIM directors, coding supervisors, Medicare reimbursement directors, directors of ambula-tory care and outpatient services, and other HIM professionals, Briefings on APCs helps facilities understand thecomplexities of the changing rules under OPPS and APCs and the impact they will have on hospital HIM systemsand processes, including coding, documentation, and billing. Subscribers receive the latest information on
• understanding the basics of OPPS and APCs • techniques for correct coding • continued education for staff • APCs and OPPS in your emergency department • financial impact of APCs • compliance under OPPS and APCs • analysis of the impact of HCFA program memos • and much more
For more information, please call HCPro, Inc., customer service at 800/650-6787
About your sponsors

viii Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Speaker profiles
Robin Robinson (Moderator)
Robin Robinson is the managing editor of two monthly publications covering APC coding and compliance stories.She also writes a weekly electronic news update on APC issues.
Cheryl D’Amato, RHIT, CCS
Cheryl D’Amato, RHIT, CCS, is the director of Health Information Management at HSS, Inc., a company providingproducts and services that help the health care industry manage complex reimbursement, casemix management, clin-ical encoding, severity-of-illness and quality measurement. She is responsible for the development, enhancement andmaintenance of all products with a coding focus. D’Amato has over 20 years’ experience in the health care industrywith expertise in implementing and managing utilization, quality assurance and health information coding systems.She has served on the board of the AHIMA’s Society for Clinical Coding (SCC) and is currently involved in AHIMAcoding leadership activities and is a member of AHIMA’s Coding Policy and Strategy Committee.
D’Amato has spoken at nation and state HIM and SCC meetings and a number of other educational sessions andteleconferences on OPPS, compliance and coding. In addition to her speaking engagements, D’Amato is a fre-quent contributor to a number of publications including Opus Communications, a division of HCPro, APC AnswerLetter and is a one of the co-authors of their on-line APC Weekly Monitor.
Valerie A. Rinkle, MPA
Valerie A. Rinkle, MPA, is the revenue cycle director for Asante Health System. Rinkle has 17 years’ health carereimbursement experience including eleven years in nationwide consulting to hospitals and physicians regardingMedicare and Medicaid payment systems and compliance. Rinkle is the author of numerous articles on OPPS andhospital-based clinics in Dennis Barry’s Reimbursement Advisor. Currently serves on editorial board of APCMonitor, an ezine on APCs. Former Reimbursement Manager for UCSF Medical Center and previous governmentexperience with HHS and CMS.
Exhibit A
Presentation by Cheryl D’Amato and Valerie Rinkle
hcProhcPro

Exhibit A
2 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Observation Services and APCPayments: An Update for 2003
March 12, 2003
Objectives
� Review criteria for observation status
� Review coding and billing for hourly observation charges andthe Observation APC
� Understand the 2003 changes for Observation APC
� Understand APC payment opportunities for observationservices beyond the observation APC
� Understanding the importance of inter disciplinary, or multidepartmental approach dealing with observations services
3Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Exhibit A
Observation Services
�Outpatient services must be provided in the hospital setting (ie,licensed hospital space)
�Observation status is not determined by location, but isdetermined by physician order & medical necessity
� Physician is monitoring patient to determine if inpatientadmission is necessary/appropriate
Observation Services –not covered
� Services not covered by Medicare as outpatient observationservices include:
� Services exceeding 48 hours without an FI exception
� Services provides for the convenience of the patient, family orphysician (ie, time that is not medically necessary or time whenmedical monitoring is not occurring)
� Standing orders for observation following outpatient surgery
� Pre- or post- diagnostic or surgical procedure time that isroutine/expected for the procedure
� An inpatient admission that is subsequently converted to outpatientobservation (CMS does not allow this practice)
Exhibit A
4 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Observation APC 0339
� APC 0339 is still limited to 3 conditions:� Chest pain
� Asthma
� Congestive Heart Failure
� Payment status indicator “S”
� 2003 payment rate is $376.47 ($75.29 of which is patientco-payment)
� All criteria for separate APC payment must be met
� Medicare will continue to package observation servicesinto the APC payment for the visit or procedure for allother diagnoses
Required ICD-9-CM Codes forChest Pain
� 411.0 Post MI syndrome� 411.1 Intermed. Coronary syndrome� 411.81 Coronary occlusion w/out MI� 411.89 Other acute ischemic heart disease� 413.0 Angina decubitus� 413.1 Prinzmetal angina� 413.9 Other & unspecified angina pectoris� 786.05 Shortness of breath� 786.50 Chest pain, unspecified� 786.51 Precordial pain� 786.52 Painful respiration� 786.59 Other chest pain
5Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Exhibit A
Required ICD-9-CM Codes for Asthma
� 493.01 Extrinsic asthma w/status asthmaticus
� 493.02 Extrinsic asthma w/acute exacerbation
� 493.11 Intrinsic asthma w/status asthmaticus
� 493.12 Intrinsic asthma w/acute exacerbation
� 493.21 Chronic obstructive asthma w/status asthmaticus
� 493.22 Chronic obstructive asthma w/acute exacerbation
� 493.91 Asthma, unspecified w/status asthmaticus
� 493.92 Asthma, unspecified w/acute exacerbation
Required ICD-9-CM Codes for CHF
� 391.8 Other acute rheumatic heart disease� 398.91 Rheumatic heart failure (congestive)� 402.01 Malignant hypertensive heart disease with
congestive heart failure� 402.11 Benign hypertensive heart disease with congestive
heart failure� 402.91 Unspecified hypertensive heart disease with
congestive heart failure� 404.01 Malignant hypertensive heart and renal disease
with congestive heart failure� 404.03 Malignant hypertensive heart and renal disease
with congestive heart and renal failure
Exhibit A
6 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Required ICD-9-CM Codes for CHF(continued)
� 404.11 Benign hypertensive heart and renal disease with congestive heart failure
� 404.13 Benign hypertensive heart and renal disease with congestive heart and renal failure
� 404.91 Unspecified hypertensive heart and renal disease with congestive heart failure
� 404.93 Unspecified hypertensive heart and renal disease with congestive heart and renal failure 428.0 Congestive heart failure
� 428.0 Congestive Heart Failure� 428.1 Left heart failure� 428.9 Heart failure, unspecified
Required ICD-9-CM Codes for CHF(continued)
� 428.20 Unspecified systolic heart failure� 428.21 Acute systolic heart failure� 428.22 Chronic systolic heart failure� 428.23 Acute on chronic systolic heart failure� 428.30 Unspecified diastolic heart failure� 428.31 Acute diastolic heart failure� 428.32 Chronic diastolic heart failure� 428.33 Acute on chronic diastolic heart failure� 428.40 Unspecified combined systolic and diastolic heart
failure� 428.41 Acute combined systolic and diastolic heart failure� 428.42 Chronic combined systolic and diastolic hear failure� 428.43 Acute on chronic combined systolic and diastolic
heart failure
7Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Exhibit A
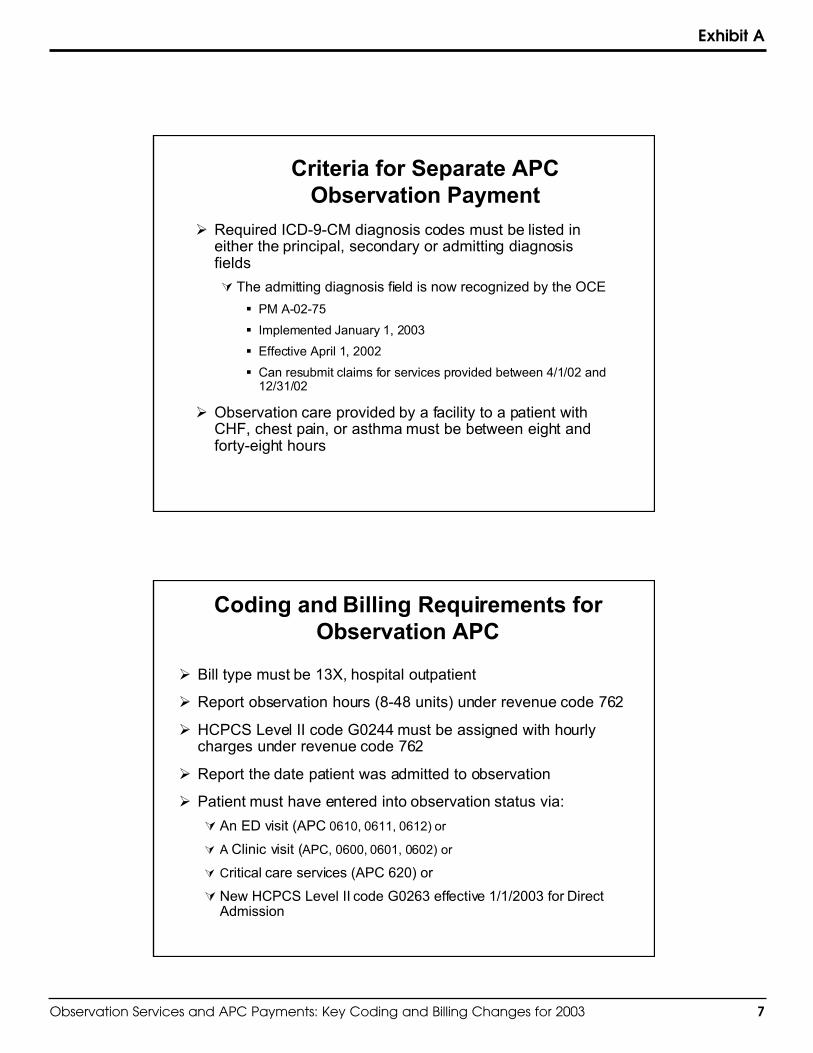
Criteria for Separate APCObservation Payment
� Required ICD-9-CM diagnosis codes must be listed ineither the principal, secondary or admitting diagnosisfields
� The admitting diagnosis field is now recognized by the OCE
� PM A-02-75
� Implemented January 1, 2003
� Effective April 1, 2002
� Can resubmit claims for services provided between 4/1/02 and12/31/02
� Observation care provided by a facility to a patient withCHF, chest pain, or asthma must be between eight andforty-eight hours
Coding and Billing Requirements forObservation APC
� Bill type must be 13X, hospital outpatient
� Report observation hours (8-48 units) under revenue code 762
� HCPCS Level II code G0244 must be assigned with hourlycharges under revenue code 762
� Report the date patient was admitted to observation
� Patient must have entered into observation status via:
� An ED visit (APC 0610, 0611, 0612) or
� A Clinic visit (APC, 0600, 0601, 0602) or
� Critical care services (APC 620) or
� New HCPCS Level II code G0263 effective 1/1/2003 for DirectAdmission
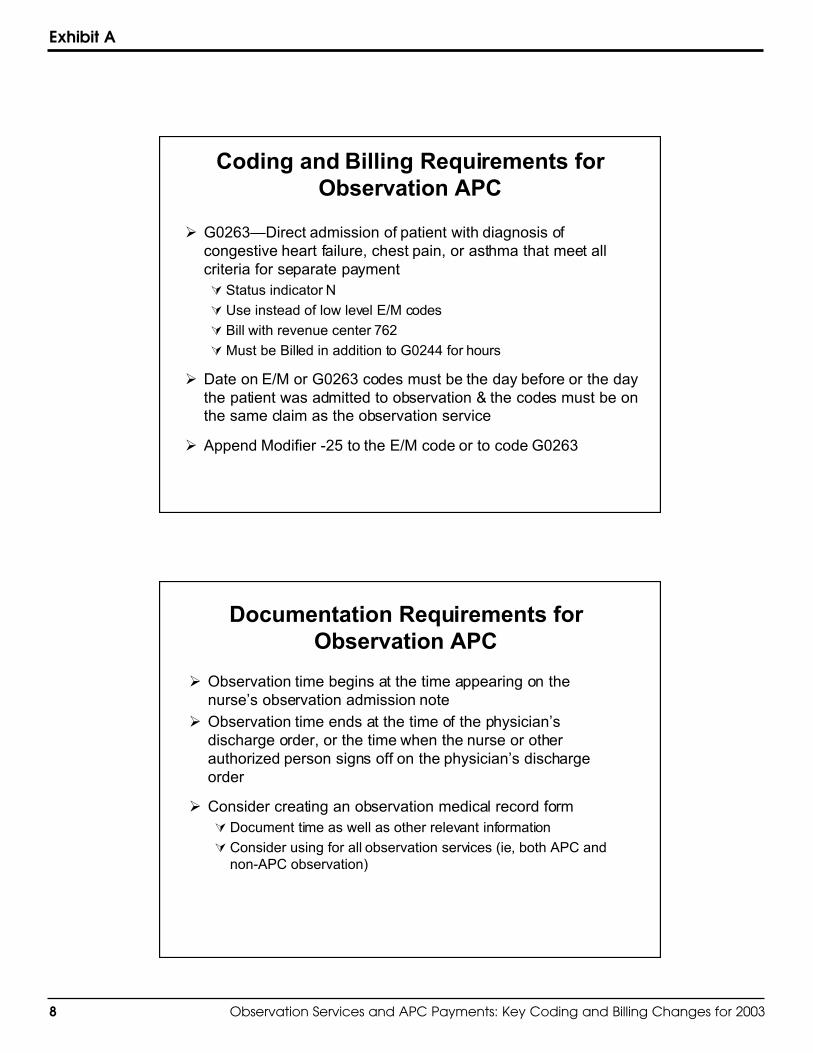
Exhibit A
8 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Coding and Billing Requirements forObservation APC
� G0263—Direct admission of patient with diagnosis ofcongestive heart failure, chest pain, or asthma that meet allcriteria for separate payment� Status indicator N
� Use instead of low level E/M codes
� Bill with revenue center 762
�Must be Billed in addition to G0244 for hours
� Date on E/M or G0263 codes must be the day before or the daythe patient was admitted to observation & the codes must be onthe same claim as the observation service
� Append Modifier -25 to the E/M code or to code G0263
Documentation Requirements forObservation APC
� Observation time begins at the time appearing on thenurse’s observation admission note
� Observation time ends at the time of the physician’sdischarge order, or the time when the nurse or otherauthorized person signs off on the physician’s dischargeorder
� Consider creating an observation medical record form� Document time as well as other relevant information
� Consider using for all observation services (ie, both APC andnon-APC observation)
9Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Exhibit A
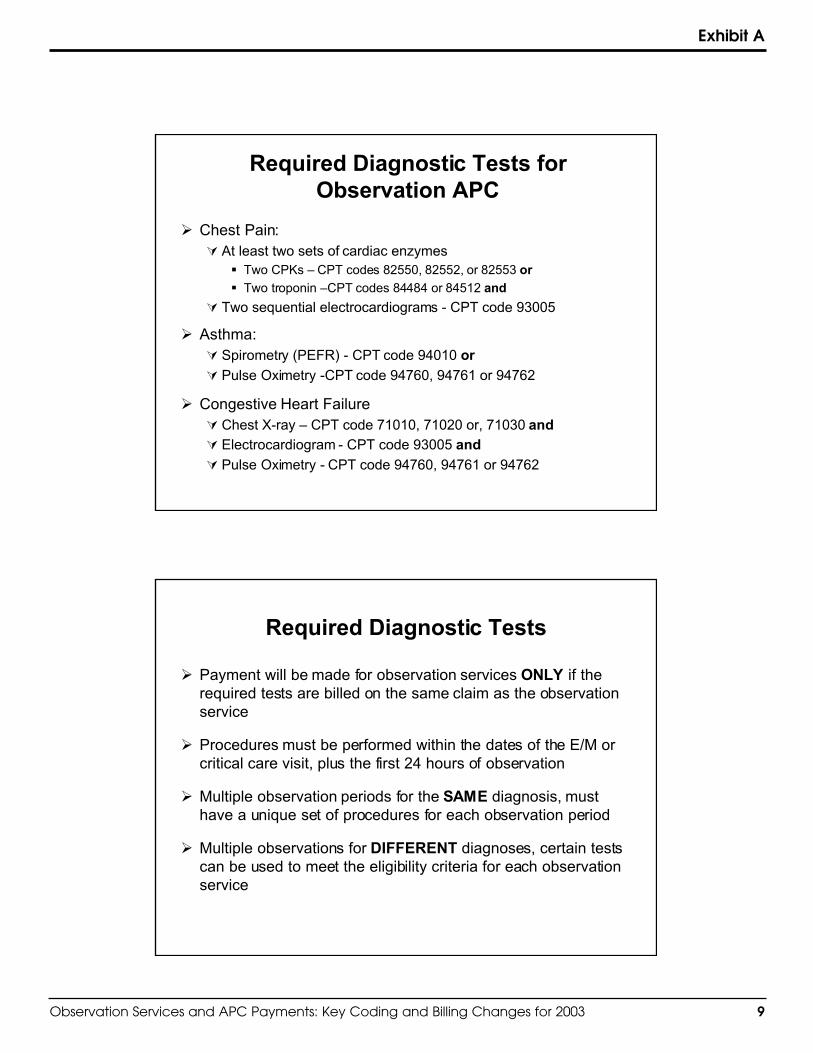
Required Diagnostic Tests forObservation APC
� Chest Pain:� At least two sets of cardiac enzymes
� Two CPKs – CPT codes 82550, 82552, or 82553 or
� Two troponin –CPT codes 84484 or 84512 and
� Two sequential electrocardiograms - CPT code 93005
� Asthma:� Spirometry (PEFR) - CPT code 94010 or
� Pulse Oximetry -CPT code 94760, 94761 or 94762
� Congestive Heart Failure� Chest X-ray – CPT code 71010, 71020 or, 71030 and
� Electrocardiogram - CPT code 93005 and
� Pulse Oximetry - CPT code 94760, 94761 or 94762
Required Diagnostic Tests
� Payment will be made for observation services ONLY if therequired tests are billed on the same claim as the observationservice
� Procedures must be performed within the dates of the E/M orcritical care visit, plus the first 24 hours of observation
� Multiple observation periods for the SAME diagnosis, musthave a unique set of procedures for each observation period
� Multiple observations for DIFFERENT diagnoses, certain testscan be used to meet the eligibility criteria for each observationservice
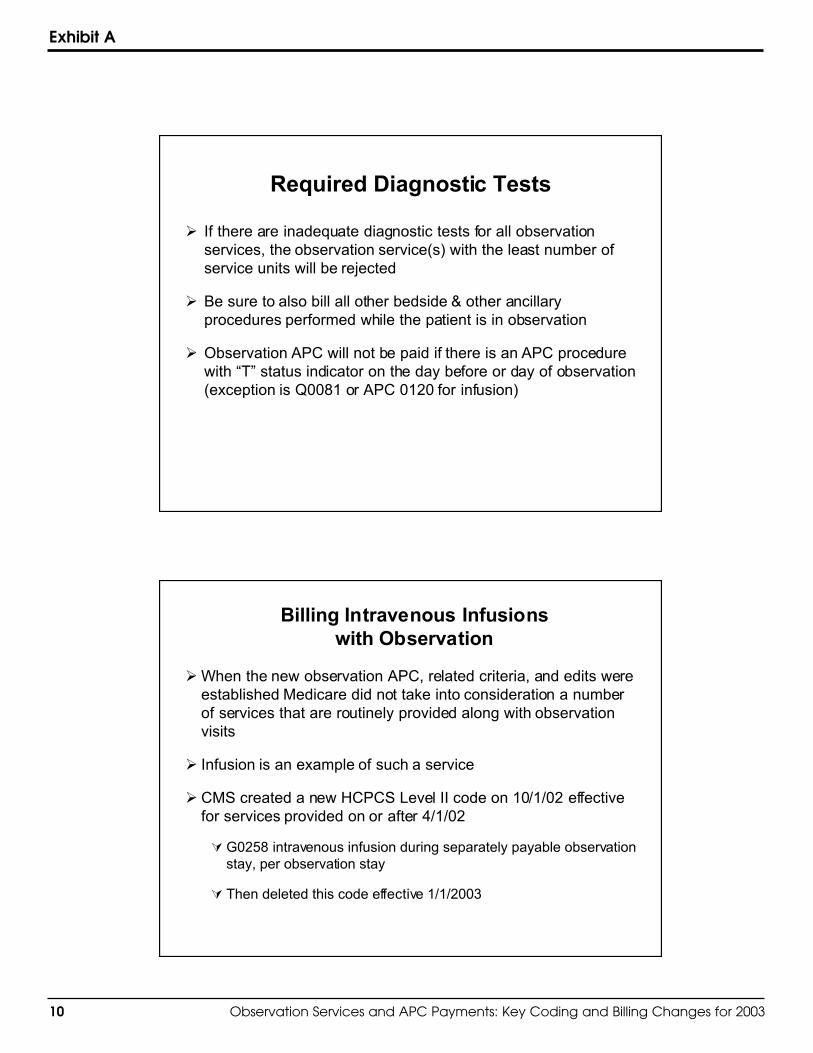
Exhibit A
10 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Required Diagnostic Tests
� If there are inadequate diagnostic tests for all observationservices, the observation service(s) with the least number ofservice units will be rejected
� Be sure to also bill all other bedside & other ancillaryprocedures performed while the patient is in observation
� Observation APC will not be paid if there is an APC procedurewith “T” status indicator on the day before or day of observation(exception is Q0081 or APC 0120 for infusion)
Billing Intravenous Infusionswith Observation
�When the new observation APC, related criteria, and edits wereestablished Medicare did not take into consideration a numberof services that are routinely provided along with observationvisits
� Infusion is an example of such a service
� CMS created a new HCPCS Level II code on 10/1/02 effectivefor services provided on or after 4/1/02
�G0258 intravenous infusion during separately payable observationstay, per observation stay
� Then deleted this code effective 1/1/2003
11Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Exhibit A
Billing Intravenous Infusionswith Observation
� Effective for services on or after 1/1/2003 use code Q0081,infusion therapy other than chemotherapy (“T” procedure)
� The OCE has been modified to allow code Q0081 duringobservation
� Continue to code and bill all other services such as:
� Code 90784 for IV push injection (“X” procedure)
� Code 51702 for insertion of temporary indwelling bladder catheter(eg, foley) (“N” procedure)
Documentation Requirements for APCObservation - Risk Stratification
� Documentation must indicate that the physician used “risk stratificationcriteria” to determine that the patient would benefit placement inobservation status
� The manner in which documentation of risk stratification is made is atthe discretion of the physician
� In Nov. 30, 2001 (FR pp59882-59883), CMS stated they finalizedrequirement for risk stratification that may be based upon generally-accepted or hospital-specific standards, however, CMS “did not meanto require any extra documentation in the medical record. We wish toput physicians and hospitals on notice as to what type of medicalrecord evidence reviewers will use…We believe a well-documentedobservation record will satisfy this requirement without any extradocumentation.”
Exhibit A
12 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Documentation
� The reason for admission to observation must be described
� The order to observation outpatient status must be clear
�Orders for diagnostic services & performance/findings ofdiagnostic services must be present
�Medical necessity documentation must be present
� The patient must be under the care of a physician during theperiod of observation
� This will be indicated by admission, discharge, and otherappropriate progress notes, timed, written, and signed by thephysician.
� There must be documentation of continuous monitoring
OCE Edits
� There are now five OCE edits related to the observation APC� Edits 51 and 53 have not been changed
� Edit 52 has been revised to edit hours in observation, qualifyingdiagnoses and status “T” procedures
� New edits 56 and 57 will edit E/M and ancillary procedureconditions and the line item date for observation code G0244
� All changes are retroactive to 4/1/02 except the addition of thenew direct admission code G0263 to the E/M logic in edits 56and 57
13Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Exhibit A
OCE Edits
� Edit 51: Multiple Observations Overlap In Time (Return ToProvider)
� Still not activated as of 1/01/03
� Reserved for future identification of overlapping periods ofobservation
� Edit 53: Code G0244 Is Allowed Only With Bill Type 13X (Line-Item Rejection)
� Separate additional observation service coverage is only availablewith Bill Type 13X
� All other Bill Types will be rejected for payment.
Revised OCE Edit
� Edit 52: Observation Does Not Meet Minimal hours, qualifyingdiagnosis, and/or “T” procedure conditions (Return To Provider)
� HCPCS code G0244 on claim and one of the following is true
� Observation hours are less than 8
� One of the required qualifying diagnoses is not present on the claim
� A surgical procedure (payment status code “T”) other than Q0081 wasbilled on the day of or the day before observation was initiated
Exhibit A
14 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
New OCE Edits
� Edit 56: E/M or ancillary procedure conditions are not met andline item date for observation code G0244 IS NOT12/31 or 1/1(Return To Provider)
� Edit 57: E/M or ancillary procedure conditions are not met andline item date for observation code G0244 IS 12/31 or 1/1(Suspend)
� HCPCS code G0244 on claim and one of the following is true
� Accompanying clinic, ED, or critical care E/M code or direct admitcode G0263 is not assigned on the day before or the day ofobservation
� Modifier –25 is not appended to the E/M code, and the date of servicematches that of the observation service code
� All qualifying diagnostic procedures are not reported within 24 hours ofthe date of the observation service code
Observation Services for Other thanChest Pain, CHF & Asthma
� Payment for observation services provided for all otherdiagnostic reasons are packaged into other APC-payableservices
� Packaged services are still required to be reported on outpatienthospital claims
� It’s important to remember that the rules for observationservices which were in effect prior to the creation of this newAPC are still in effect (Hospital Manual Section 230.6)
� These observation services can be labeled Other ObservationServices
15Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Exhibit A
Billing Other Observation Services
� Hospitals are still required to bill Medicare for observationservices for other reasons using:
� Revenue code 762
�May use observation E/M code, but not required
� Report number of hours in the units field (1-48 hours)
� Begin counting hours when the patient is placed in observation
� Note that while Medicare has no requirement that the hourlycharge be no more than the 24-hour room & board rate dividedby 24, most private payers refuse to pay 24 hours of observationthat add to more than the inpatient room & board rate
Billing Other Observation Services
� Again, direct admits to observation are appropriate
� Another new HCPCS Level II code effective January 1, 2003�G0264—Initial nursing assessment of patient directly admitted to
observation with diagnosis other than congestive heart failure,chest pain, or asthma or patient directly admitted to observation fordiagnosis of congestive heart failure, chest pain or asthma whenthe observation stay does not qualify for separate payment.
� APC 0600 – Low Level Clinic Visit
� Status indicator V - $43.96
� Use G0264 instead of low level E/M codes
� Bill with revenue code 762
� If a clinic or ED E/M code is used with observation revenue code762, the claim will fail OCE Edit 44
Exhibit A
16 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Other Observation Services
� Documentation of medical necessity must be present
� Correct diagnosis assignment is crucial
� Hospitals are required to include observation charges on the billeven though they are not separately reimbursable.
� Outlier and transitional corridor payments may be affected
Other Observation Services
�Other services performed in conjunction with observation shouldbe billed
�Observation services do NOT include patients who aretransferred to an observation area to complete their recoveryfrom a procedure (medically necessary recovery time outsidethe PACU may be reported as hourly charges under revenuecode 719 with no HCPCS)
�Observation provided for the convenience of the patient, familyor physician is not appropriate
� It is not appropriate to change the status from inpatient toobservation if it is determined that the patient does not meethospital level of care criteria
17Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Exhibit A
Issues Related to CodingDiagnostic Tests
� Coding of pulse oximetry� Physician order must be present with findings documented�Order may be written in chart or part of a formalized protocol� Test must be for diagnostic purposes, not monitoring� Evaluate screening services preformed as part of ED triage –
should not be coded separately unless ordered or part of triageprotocol for diagnostic purposes
� If pulse oximetry readings are automatically generated byequipment that monitors a combination of things, it should not becoded separately
� Coding of Peak Expiratory Flow Rate� CMS continues to refer to PEFR as 94010 – however, this code is
defined as spirometry, including graphic record, total and timedvital capacity, expiratory flow rate measurement(s), with or withoutmaximal voluntary ventilation
Issues Related to CodingDiagnostic Tests
� Use the appropriate modifiers when necessary� Use modifiers -76 or -77 with repeated EKG codes
�Modifier -91 must be appended to repeated CPKs or troponincodes
� Either manually enter modifiers for repeat services or createadditional line items in CDM for these required repeat services
� Revise screens for charge entry to ask if test is repeated andprompt for modifiers
Exhibit A
18 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Issues Related to CodingDiagnostic Tests
�Many hospitals have taken packaged procedures (statusindicator N) out of their CDM� Bladder catheterization is a packaged service and should be
coded
� Pulse oximetry is a packaged services and must be coded whenperformed on CHF patients for separate observation APC payment
Issues related to coding bedsideservices
� Nursing services performed at bedside are often not coded orcaptured as charges on observation patients
� This applies to both APC and Non-APC observation patients� Services include such activities as:
� IM/SQ Injections 90782 (APC 0353 “X” $20.72)� Antibiotic Injections 90788 (APC 0359 “X” $59.12)� IV Injections 90784 (APC 0359 “X” $59.12)� Infusion Q0081(APC 0120 “T” $113.70)� Bladder Irrigation 51700 (APC 0164 “T” $58.62)�Gastric lavage 91105 (APC 0360 “X” $84.90)� Venous Access Device Declotting 36550 (APC 0677 “T” $137.96)
� Observation charge form can be used to prompt coding & billingof these services
19Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Exhibit A
Other Issues to consider
�Who’s responsible for coding G0244?
�HIM versus CDM
�Establish a policy
�Some facilities have HIM coders review all claims that potentially maymeet criteria for separate payment
�Consider having case managers evaluate and determine when G0244should be assigned when assignment is CDM driven
�Have case managers or audit nurses review medical records ofpatient’s admitted to observation to make sure that required testing isperformed and documentation is present
�Provide physician education on documentation, tests, treatments, etc.required for each diagnosis and for all other observation stays
Other Issues to consider
� Often hospitals don’t have enough beds in the ED for observation
� May have to use nursing units where expenses will be higher
� Specialty care units such as ICU or CCU are valid for observation
� Often observation services consume considerably more resources than thehospital is being reimbursed when in fact the patient could have beenadmitted as an inpatient to the hospital
� If a patient meets hospital level of care criteria consider having the physicianadmit the patient to the hospital as an inpatient as soon as possible
� It’s important that hospitals establish clinical documentation guidelines inorder to document the patient’s medical problems sufficiently in theseinstances
� Report hourly observation and bedside service charges for the period inobservation status even when the patient is subsequently admitted as aninpatient
Exhibit A
20 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Operational Issues
� Are ED and Clinic forms conducive to encouraging physiciansto write clear observation orders and to time discharge order?
� Again, consider developing an observation charge form and/orobservation medical record form
� Use same form/record for all observation admissions
� Could See More Conditions Added to the List, but only ifhospitals properly report Non-APC Observation Charges
� Continue providing accurate and complete data
� Continue providing comments to CMS
Summary
� Provide ongoing education to HIM coders and those assigningcharges for observation services
� Educate physicians on OPPS issues related to observationsservices
� All observation cases should be reviewed prior to admission toobservation status for medical necessity
� Involve case management in the ongoing evaluation of patientsadmitted to observation
� All observation claims should be reviewed with medical recordprior to billing
� Expect the OIG to target observation stays
Exhibit B
Articles from our HCPro, Inc newsletter; Briefings on APCs
• Documentation key in establishing medical necessity for observation
• Physician documentation drive observation payment
hcProhcPro
Exhibit B
22 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Documentation key in establishing medicalnecessity for observation
As with other types of outpatient care it is important to establish the medical necessity for observation services.Medical necessity is proven through documentation by the physicians, nurses, and others providing care for thepatient.
“Thorough, accurate documentation that clearly communicates the acuity of the patient and the intensity of servicesprovided is critical,” says Candace Shaeffer, RN, MBA, vice president of coding/quality management at LYNXMedical System.
According to Shaeffer, in addition to the general requirements for good documentation in the healthcare record(such as timed and initialed entries, appropriate signatures, legibility, etc.), observation specific documentationshould include the following:
• The site of service from which the patient was admitted such as the ED, physician’s office or clinic • A summary of the patient’s reason for the observation admit including a brief history and treatment prior to the
observation admit • A listing of allergies and current medications, and an assessment of the patients pain, if any • An admission assessment per hospital or observation policy including vital signs and pertinent systems review • Interventions and reassessments as appropriate, including the patient’s responses to treatments • An evaluation of the patients psychosocial needs with any limitations and accommodations for them • Involvement of the family and/or significant others, if appropriate • Discharge planning arrangements, discharge instructions, and referrals if any
23Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Exhibit B
Physician documentation drive observation payment
Write it right if you want to get paid
As hospitals get ready to expand observation services under the 2003 final rule, there are still many questions abouthow to handle billing the observation APC. Most revolve around documentation requirements and whether a physi-cian has to be present during the patient’s stay.
“The physician’s documentation is what drives the coding process and the facility’s success or failure to get paid forthe effort,” says Candace Shaeffer, RN, MBA, vice president of coding and quality management at Lynx MedicalSystems in Bellevue, WA. “The physician’s documentation has to show medical necessity for every test and proce-dure. If your clinical staff don’t follow the rules, you won’t get paid.”
Failed claims will kick back with edit 52, failure to meet criteria for separate APC payment. You can avoid edit 52if your claim reports:
• minimum of eight hours on the UB-92• services provided under revenue code 762• appropriate diagnosis code(s) for the patient’s condition• properly documented and coded tests and procedures• modifier -25 assigned to the ED or outpatient E/M in addition to the observation code G0244
If all observation criteria are met, for Medicare patients, facilities will be reimbursed the APC payment rate obser-vation of patients with chest pain, congestive heart failure, and asthma who meet the APC criteria. Accurate clinicaldocumentation is the key to getting paid.
What makes good clinical documentation? Shaeffer says that in general, it has to meet a variety of standards set bythe facility, the state, CMS, and the Joint Commission AHO. An observation patient should be monitored duringhis/her stay to be sure their condition is stable and that the goals of why they were placed in the observation in thefirst place are being met.
In short, notes need to be made in the record to reflect interactions between staff and the patient—be it to perform aprocedure, treatment, or evaluation. The notes should reflect patient reaction and outcomes of the intervention orinteraction.
These are clues that will lead a coder through the record to assign the appropriate codes for reimbursement.
Observation begins with the time recorded on the nursing observation admission note and ends with the timerecorded on the physician’s discharge order. If the physician does not record the time on his order, the time that thenurse recorded as signing off on the physicians order is acceptable as the end of the observation time.

Exhibit B
24 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
The physician does not have to be present at all times during the observation stay but must be actively directing thepatient’s care. In most cases, a physician cannot leave standing orders for observation to qualify for APC payment.CMS will not pay APC reimbursement for:
• services not reasonable and necessary for diagnosis and treatment of patient. If a patient comes to the hospitalfor cardiac catheterization and the test is delayed, you cannot admit the patient to observation.
• services that are secondary to a standing order for observation following outpatient surgery. If a patient has abiopsy and is held in the recovery area until discharged home, this time is not considered for APC payment.
• physician-ordered inpatient services billed as outpatient services. This might include a patient admitted to thefacility by an ED physician, who is then seen by an attending physician who decides the patient didn’t need tobe admitted at all. An inpatient can not be converted back to an outpatient observation patient if the goal is torelease to home within 24 hours.
In short, the goal of observation is to resolve symptoms or clarify a patient’s diagnosis. These goals and outcomesneed to be clearly stated so clinical care is focused and a coder can process the record into a payable claim.
In the original 2002 rule on observation, CMS said physicians had to use risk stratification criteria to assignpatients to observation. Risk stratification is an analysis of the many facets of a patient and his/her condition, fromage, medical history, life style risks like smoking or level of stress, and current symptoms. It makes good clinicalsense to use these kinds of measures to benchmark a patient’s condition and eligibility for observation. A clearlydocumented record will suffice, and that is accomplished when staff follow common sense rules and document tosupport medical necessity of every service provided.

Resources
hcProhcPro
Resources
26 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Speaker Resources
Cheryl D’Amato, RHIT, CCSDirector of Health Information Management, HSS, Inc.HSS, Inc.2321 Whitney Avenue 4th floorHamden, CT 06518www.hss-info.com
Valerie A. RinkleRevenue Cycle DirectorAsante Health Systemwww.asante.org
HCPro Sites
HCPro: www.hcpro.comIt is HCPro’s mission to meet the specialized information, advisory, and education needs of the health care industryand to learn from and respond to our customers with services that meet or exceed the quality they expect. VisitHCPro’s Web site and take advantage of our new Internet resources.
Here’s what visitors will discover:
• List of products and services• Supersites for health care professionals: ➢ accreditinfo.com -The Healthcare Accreditation Supersite™➢ complianceinfo.com - The Healthcare Corporate Compliance Supersite™➢ credentialinfo.com - The Healthcare Credentialing Information Supersite™➢ healthsafetyinfo.com – The Health Safety Supersite™➢ himinfo.com – The Health Information Management Supersite™➢ snfinfo.com – The Long-Term Care Information Supersite™➢ msleader.com – The Medical Staff Information Supersite™• A link to Healthcare Marketplace—the electronic retail store where you can shop for the health care manage-
ment resources you need. By bringing together the premier vendors of information resources, the HealthcareMarketplace makes it easy for you to find what you need, when you need it, in one secure and user-friendly e-commerce store.
• HCPro will continue to offer the expert advice and practical guidance you’ve come to rely on to meet yourdaily challenges. This valuable information will be available to you 24 hours a day, seven days a week—via theInternet.
27Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Resources
The Greeley Company: www.greeley.comGet connected with leading health care consultants and educators at The Greeley Company’s Web site at www.greeley.com. This online service provides the fastest, most convenient, and most up-to-date information on our qual-ity consulting, national education offerings, and multimedia training products for health care leaders. Visitors willfind a complete listing of all our products, and services that include consulting services, seminars and conferences,audioconferences, publications, online resources, and videos and multimedia.
Here’s what visitors will find:
• Faculty and consultant biographies—learn about our senior-level clinicians, administrators, and faculty who areready to assist your organization with your consulting needs, seminars, workshops, and symposiums
• Detailed descriptions of all The Greeley Company consulting services• List of Greeley clients• Catalogue and calendar of Greeley’s national seminars and conferences and available CMEs• A schedule of upcoming audioconferences and listing of audiocassette packages• Subscriptions and books• Direct links to supersites for health care professionals• Training videos, CDs, and multimedia products• User-friendly online registration/order forms for seminars and audioconferences• Audioconference “Q&A” archives
Healthcare Marketplace: www.hcmarketplace.comThe Healthcare Marketplace is a focal point of all our vertical niche Web sites. This e-commerce site offers secure,online purchases of various tools and materials geared toward our core audiences. This site showcases HCPro’sproducts and services, as well as those of vendors. Visitors to this site will find: listings of newsletters, books, soft-ware, and video products with a direct link to the online order form; information on consulting services; and adirectory of trade shows and seminars and the ability to register for them online. Site visitors will also find a conve-nient store directory, new product highlights, and ongoing specials.
HIM Info: www.himinfo.comInformation managers responsible for the management of medical records and related data use this site to obtaincurrent federal regulations, to exchange advice on meeting outside legal and accreditation requirements, and to pur-chase related products. HCPro has published in this field since its founding and is known to be the authoritativesource on medical records management. Visitors to the site will be able to obtain guidance on each area of man-agement of medical records. A key feature is a unique directory of the hundreds of vendors who offer computerproducts, software, services, and supplies to this large industry.
Resources
28 Observation Services and APC Payments: Key Coding and Billing Changes for 2003
Observation Services and APC Payments: Key Coding and BillingChanges for 2003 – 03/12/2003
This program is pending prior approval by the American Academy of Professional Coders for 1.5 ContinuingEducation Units. Granting of this approval in no way constistutes endorsement by AAPC of the program, content,or the program sponsor. In order for the certificate in the back of your material packet to be valid, the names of allindividuals receiving the certificate must be supplied HCPro, Inc.
Please fill in the First name, last name, title, organization and signature of each attendee and RETURN THIS FORM TO [email protected] or fax it to 781/639-2982
First Name Last Name Title Organization Signature
For more information call 800/801-6661, or visit us on the Web at www.greeley.comSeminars offer 10 category I CME or 12 nursing contact hours and 10 NAMSS CEU’s
Advanced Medical Staff LeadershipRetreat Series I & II:How to resolve today’s toughest medical staff challenges
Credentialing and Privileging:What physician leaders and credentialing professionals must know today!
6th Annual Credentialing Resource Center Symposium
Effective JCAHO Survey Preparation for the Medical Staff
Medical Executive Committee Institute:The essential training program for all medical staff leaders
Medical Staff Quality:How to measure outcomes and improve performance
Patient Safety and Medical ErrorReduction:In pursuit of safe and trusted healthcare
Legal Issues for Medical Staff Leaders:Common-sense approaches to today’s legal challenges and pitfalls
A Practical Approach to JCAHO SurveyPreparation 13.5 Nursing Contact Hours!
VPMA Forum NEW! 1-Day Program!
Series IApril 3-4Fairmont
Copley PlazaBoston, MA
March 13-14Ritz CarltonPhoenix, AZ
March 13-14Ritz CarltonPhoenix, AZ
May 15-16Marriott
Golf ResortHilton Head, SC
April 3-4Fairmont
Copley PlazaBoston
March 3-4Pier 66 Hyatt
Ft. Lauderdale
May 1-2Walt Disney World Swan,Orlando,FL
2003
© 2003 The Greeley Company, a Division of HCPro. The Greeley Company, a Division of HCPro is not affiliated in any way with the Joint Commission on Accreditation of Healthcare Organizations, which owns the JCAHO trademark.MT9594
March May October November
Series INovember 6-7
Laguna CliffsMarriott
Laguna, CA
October 23-24Ritz Carlton
Amelia Island, FL
Series IIOctober
23-24Ritz Carlton
Amelia Island, FL
November20-21
Ritz CarltonPalm Beach, FL
April
November20-21
Ritz CarltonPalm Beach, FL
October 9-10Fairmont
Chicago, IL
November 6-7Laguna Cliffs
MarriottLaguna, CA
November 13-14
Sheraton CrescentPhoenix, AZ
October 9-10Fairmont
Chicago, IL
October 8Fairmont
Chicago, IL
November 19Ritz Carlton
Palm Beach, FL
SPECIAL OFFER!ADUIOCONFERENCE ATTENDEES RECEIVE $100 OFF ANY SEMINAR. TO REGISTER, CALL ANGELA SIMPSON
AT 800/801-6661 AND REFERENCE CODE MT9594
Education Program Schedule
CE
RT
IFIC
AT
EO
FA
TT
EN
DA
NC
E
atte
nded
“Obs
erva
tion
Ser
vice
s an
d A
PC
Pay
men
ts:
Key
Cod
ing
and
Bill
ing
Cha
nges
for
200
3”
Thi
s pr
ogra
m i
s pe
ndin
g ap
prov
al b
y th
e A
mer
ican
Aca
dem
y of
Pro
fess
iona
l C
oder
s fo
r 1.
5 co
ntin
uing
edu
cati
on u
nits
. G
rant
ing
of t
his
appr
oval
in
no w
ay c
onst
itut
es e
ndor
sem
ent
by A
AP
C o
f th
e pr
ogra
m, c
onte
nt, o
r th
e pr
ogra
m s
pons
or.
a 90
-min
ute
audi
ocon
fere
nce
onM
arch
12,
2003
Suz
anne
Per
ney
HC
Pro
hcPr
o










![F AC 31 08 [a] Gas Chromatogrphy](https://img.pdfslide.us/doc/110x75/577cdad31a28ab9e78a6a2a2/f-ac-31-08-a-gas-chromatogrphy.jpg)


















