Embed Size (px)
Citation preview

Pediatric Palliative Care in the 21st Century: Live as long and as well as possible
Stefan J. Friedrichsdorf, MD, FAAPMedical Director, Department of Pain Medicine, Palliative Care & Integrative MedicineChildren's Hospitals and Clinics of Minnesota, Minneapolis/St. Paul, MN
Associate Professor of Pediatrics, University of Minnesota Medical School
[email protected] Twitter: @NoNeedlessPain
Learning Objectives
• Review common obstacles for referral to Pediatric Palliative Care (PPC)
• Evaluate top myths in PPC
• Underscore importance of interdisciplinary team approach in PPC
Palliative Care
• Palliare (Latin) : to cloak
• Palliative care is about matching treatment to patient goals.
• Specialized medical care for children with serious illness
• Focused on relieving pain, distressing symptoms & stress of a serious illness
• Appropriate at any age and at any stage, together with curative treatment
• Goal is to improve quality of life for child/family

Myths, Misconceptions, and Assumptions...
• You are taking care of a seriously ill child. You would not be surprised if she might die within the next few months. You are considering a palliative care consult...
• What are arguments might you hear from colleagues (or family) not to do that?
Assumption # 1:
The death of a child is a rare event (especially in the USA...)
Death of Children
• 20 children die worldwide every second
• 1,200 children die worldwide every hour
• 29,000 children die worldwide every day
• 15-20 million children would benefit from PPC annually (low-estimate)
• ... and in the US?

Mortality 1-4 Year Olds worldmapper.org
PPC ... 2-3 generations ago?
Causes of Death in Children 0-19 years (USA, 2013)
1. Infant Mortality (<1year) 23,440Fetal Deaths > 20 wks gestation 24,073
2. 1-19 Years 18,888
4. Accidents 7,6455. Homicide 2,0216. Suicide 2,143
Total 42,328
3. Life-limiting diseases >10,800Congenital malformations, chromosomal abnormalities 5,740 Malignant Neoplasms 1850Heart Disease 693
Osterman MJ, Kochanek KD, MacDorman MF, Strobino DM, Guyer B. Annual summary of vital statistics: 2012-2013. Pediatrics 2015; 135:1115-1125.http://www.cdc.gov/nchs/data_access/Vitalstatsonline.htm#Fetal_Death

More than 115 children die in the US every day…
Osterman MJ, Kochanek KD, MacDorman MF, Strobino DM, Guyer B. Annual summary of vital statistics: 2012-2013. Pediatrics 2015; 135:1115-1125.
• More than 1 child every 15 minutes…
Life-Limiting Conditions (LLC)
• …are those for which there is no reasonable hope of cure and from which children will die before reaching adulthood.
• UK: Prevalence [32/10,000] Fraser LK, Miller M, Hain R, Norman P, Aldridge J, McKinney PA, Parslow RC: Rising national prevalence of life-limiting conditions in children in England. Pediatrics. 2012 Apr;129(4):e923-9
• White: 27/10,000
• Chinese: 32/10,000
• Black: 42/10,000
• South Asian: 48/10,000
• USA - Age 0-17: 74.3 million children (2014) http://www.childstats.gov/americaschildren/tables/pop1.asp
• Prevalence [32/10,000]: > 237,000 with LLC
• Mortality [1.5-1.9/10,000]: 10,800 - 13,700 die/year ACT & Royal College of Paediatrics and
Child Health, 2003
• 15,000 die/year Age (0-24), who would benefit from PPC Feudtner, 2001
How Many Children Would Benefit from PPC?
• UK: 32/10,000 (high income country)
• South Africa 150/10,000 (upper middle income country)
• Zimbabwe 180/10,000 (low income country)
• No accurate figure globally: ICPCN estimates 15-20 million children worldwide (low estimate)
http://www.icpcn.org
• World Health Assembly Resolution 67.19 on Palliative Care [May 2014]: ensure equitable access to palliative care, including pain relief, for neonates, children and young people and their families

Boeing 747-400 416 passengers
US Health Care System...?
• USA: (conservatively estimated)
• 237,000 children live with life-limiting conditions (LLC)
• 570 “Boeing 747”
• 10,800 -13,800 children 0-17 years die each year due to life-limiting conditions
• 26-33 “Boeing 747”
• one crash every 11-14 days
Assumption # 2:
Pediatric Palliative Care is usually for children with cancer...

Causes of death in children due to life-limiting conditions
cancer 31%[22%]
neuromuscular / neurodegenerative
20% [17%]
congenital orgenetic 16% [13%]
cardio-vascular 12% [29%]
meta-bolic9%
[1%]
Germany: 0-15 years Friedrichsdorf SJ, Zernikow B: Care of Dying Children in Germany – Status Quo of Pediatric Palliative Care. (German: Die Versorgung sterbender Kinder in Deutschland – Status Quo der pädiatrischen Palliativmedizin). Praktische Pädiatrie 2004. (10):68-72[USA: 0-24 years] Feudtner C. Deaths Attributed to Pediatric Complex Chronic Conditions: National Trends and Implications for Supportive Care Services. PEDIATRICS. 2001;107(6):e99.
Pediatric Cancer: Epidemiology USA
• New cancer diagnosis: > 16,000 children (0-19 years) / year
• Large majority are cured of their malignancy (> 80% of children with cancer are alive 5 years after diagnosis [62% in the mid-1970s]).
• However, children with good fortune to attain cure nonetheless experience considerable suffering
• 1,960 children and adolescents are expected to die due to a malignancy in 2014
1. Ries LAG, Smith MA, Gurney JG, Linet M, Tamra T, Young JL, Bunin GR (eds). Cancer Incidence and Survival among Children and Adolescents: United States SEER Program 1975-1995, National Cancer Institute, SEER Program. NIH Pub. No. 99-4649. Bethesda, MD, 1999; 2. Li J, Thompson TD, Miller JW, Pollack LA, Stewart SL: Cancer Incidence Among Children and Adolescents in the United States, 2001–2003. Pediatrics 2008. 121(6):e1470-7 3. Ries LAG, Melbert D, Krapcho M, et al. (eds). SEER Cancer Statistics Review, 1975–2005. Bethesda, MD: National Cancer Institute. http://seer.cancer.gov/csr/1975_2005 4. Linet MS, Ries LA, Smith MA, Tarone RE, Devesa SS. Cancer surveillance series: recent trends in childhood cancer incidence and mortality in the United States. J National Cancer Inst 1999;91(12):1051-8 5. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention, Atlanta, GA. December 7, 2007. 56(48);1257-1261
Heron, M. Deaths: Leading Causes for 2010. National Vital Statistics Reports 2013 May 3, 2014]; Volume 62, Number 6:[Available from: http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_06.pdf.
• Prevalence of pain during treatment: Outpatient 9-26%, inpatient 39-54% (1) Elliott SC, Miser AW, Dose AM, Betcher DL, O'Fallon JR, Ducos RS, et al. Epidemiologic features of pain in pediatric cancer patients: a co-operative community-based study. North Central Cancer Treatment Group and Mayo Clinic). The Clinical journal of pain. 1991 Dec;7(4):263-8. (2) Forgeron PA, Finley GA, Arnaout M. Pediatric pain prevalence and parents' attitudes at a cancer hospital in Jordan. Journal of Pain and Symptom Management. 2006 May;31(5):440-8. (3) Miser AW, Dothage JA, Wesley RA, Miser JS. The prevalence of pain in a pediatric and young adult cancer population. Pain. 1987 Apr;29(1):73-83.
• Survivors: Prevalence of pain conditions (12% pain/abnormal sensation; 15.5% migraines; 20.5% other headaches) and using prescription analgesics higher among survivors than siblings Lu Q, Krull KR, Leisenring W, Owen JE, Kawashima T, Tsao JC, et al. Pain in long-term adult survivors of childhood cancers and their siblings: a report from the Childhood Cancer Survivor Study. Pain. 2011 Nov;152(11):2616-24.
• Pediatric brain tumor survivors experience many symptoms after treatment. lack of energy (52%), difficulty with sleep (38%), lack of concentration (36%), and headaches (36%). Macartney G, VanDenKerkhof E,
Harrison MB, Stacey D. Symptom experience and quality of life in pediatric brain tumor survivors: a cross-sectional study. J Pain Symptom Manage. Nov 2014;48(5):957-967.
Pediatric Cancer Survivors
http://www.popsugar.com/moms/Childhood-Cancer-Survivor-Photos-34819602

Access to PPC?
• Comprehensive palliative care is the expected standard of care for patients with advanced cancer, however access to, and availability of palliative care expertise for the majority of children with life-threatening conditions, is still lacking compared with adult services.
• In the U.S., the vast majority of infants, children, and teenagers with advanced illnesses who are near the end of life do not have access to interdisciplinary pediatric palliative care (PPC) services either in their community or at the nearest children’s hospital.
Sibling Care “What do you gotta do to get some attention in this family...?”
• Oncology: Siblings report heightened concerns about the impending death Havermans, T. and C. Eiser, Siblings of a child with cancer. Child Care Health Dev, 1994. 20(5): p. 309-22.
• Siblings interviewed years after death spoke of wishing had received more information about sibling's death before terminal period Nolbris, M. and A.L. Hellstrom, Siblings' needs and issues
when a brother or sister dies of cancer. J Pediatr Oncol Nurs, 2005. 22(4): p. 227-33.
• Maternal, but not paternal, symptoms of PTSD & prolonged grief disorder directly associated with sibling outcomes Morris, A.T., et al., The Indirect Effect of Positive Parenting on the Relationship Between Parent and Sibling Bereavement Outcomes After the Death of a Child. J Pain Symptom Manage, 2016. 51(1): p. 60-70.
• Siblings benefit to be involved in conversations about mortality and care of their ill sibling. Gaab, E.M., G.R. Owens, and R.D. MacLeod, Siblings caring for and about pediatric palliative care patients. J Palliat Med, 2014. 17(1): p. 62-7.
• 99% of siblings present at time of death NOT regretting been there; 76% of siblings NOT being present, regretted it Lovgren, M., et al., Siblings' experiences of their brother's or sister's cancer death: a nationwide follow-up 2-9 years later. Psychooncology, 2015.
• PPC referral plus positive family functioning = normal psychological well being of siblings Humphrey, L.M., et al.,
Psychological Well-Being and Family Environment of Siblings of Children with Life Threatening Illness. J Palliat Med, 2015. 18(11): p. 981-4
http://opinionator.blogs.nytimes.com/2015/12/16/when-a-baby-dies

Assumption # 3:
The “sudden death”...
“Sudden” Death ? Advanced Illness Marked by Slow Decline with Periodic Crises and “Sudden” Death
Hea
lth
Stat
us
Time
Death
Decline
Crises
Multiply relapsed cancerCystic FibrosisAdvanced HIVRefractory Seizure DisorderSolid organ transplant recipientCongenital heart disease
Joanne Wolfe, MD (Boston Children’s Hospital & Dana Farber Cancer Institute), with permission
Outcomes Improved with PPC Involvement
• Parents of children with cancer report less distress from pain, dyspnea and anxiety at EOL Wolfe et al. J Clin Onc 2008
• Children who received PPC/Oncology more likely to have fun (70% versus 45%) and to experience events that added meaning to life (89% versus 63%) Friedrichsdorf SJ et al. J Palliat Med 2015
• Families who received PPC/Oncology report improved communication Kassam A, Skiadaresis J, Alexander S et al Differences in End-of-Life Communication for Children with Advanced Cancer who were Referred to a Palliative Care Team. Pediatr Blood Cancer, 2015. 62(8): p. 1409-13.
• Children receiving PPC experience shorter hospitalizations and fewer emergency department visits Ananth, P., et al., Hospital Use in the Last Year of Life for Children With Life-Threatening Complex Chronic Conditions. Pediatrics, 2015. 136(5): p. 938-46.

Assumption # 4:
Specifically trained Pediatric Palliative Care specialist are not required...
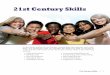
Fatigue 97%
Pain 82%
Dyspnea 82%
Poor appetite 82%
Nausea and vomiting 58%
Constipation 51%
Diarrhea 42%
76%
18%
64%
38%
42%
42%
18%
3%
4%
1%
Symptom treatedTreatment successful
28%
17%
10%
10%Wolfe J, Grier HE, Klar N, Levin SB, Ellenbogen JM, Salem-Schatz S, Emanuel EJ, Weeks JC: Symptoms and suffering at the end of life in children with cancer. N Engl J Med 2000. 342(5):326-33
103 Children With Cancer: Last Month of Life
29
Symptom prevalence and distress reported by children with advanced cancer
Wolfe J, Orellana L, Ullrich C et al Symptoms and Distress in Children with Advanced Cancer: Prospective Patient-Reported Outcomes from the PediQUEST Study, JCO 2015.

Patient-centered care...?
• Ce#azidim,CefuroximoderCe#riaxon?
• YourChoice!Hereisthedata…
31
An early palliative care intervention (even from the point of diagnosis) = appropriate and beneficial treatments, increased quality of life and may in fact lead to prolonged (!) life.
• RCT, n=151; adult cancer patients receiving palliative care early in their illness lived longer (11.6 months vs. 8.9 months, P=0.02), with better quality of life, including decreased depression
• Results underscore the need for palliative care early in a serious illness
• This appear to refute the notion that palliative care means giving up. Patients received palliative care alongside their curative treatment.
• Although this is only one study, it is an exciting one & results are not surprising: PC clinicians regularly see these outcomes in practice - even in pediatric patients. Temel JS, Greer JA, Muzikansky A,
Gallagher ER, Admane S, Jackson VA, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010 Aug 19;363(8):733-42. 32
• Chemotherapy for end-stage cancer does not prolong life, but reduces quality of life. (n=158, 3.8 months before death) Prigerson, H.G., et al.,
Chemotherapy Use, Performance Status, and Quality of Life at the End of Life. JAMA Oncol, 2015. 1(6): p. 778-84.

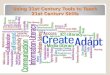
Assumption # 5:
Pediatric palliative care starts:
• when curative treatment stops,
• and when a child is close to dying
• and ends at death
Curative TreatmentPPC /
Hospice
Death
35
@LindyLandzaat
Pediatric Palliative Care
"Palliative care no longer means helping children die well, it means helping children and their families to live well and then, when the time is certain, to help them die gently.”
Mattie Stepanek, 1990-2007

Pediatric Palliative Care• Earlier recognition by both
physicians & parents that child had no realistic chance of cure led to stronger emphasis on treatment to lessen suffering & integrate PPC in pediatric cancer patients Wolfe, J., Klar, N., Grier, H. E., Duncan, J., Salem-Schatz, S., Emanuel, E. J., et al. (2000). Understanding of prognosis among parents of children who died of cancer: Impact on treatment goals and integration of palliative care. The Journal of the American Medical Association, 284(19), 2469–2475.
• Religion, Spirituality or Life Philosophy play an important role in live of most parents whose children receiving PPC Hexem KR, Mollen CJ, Carroll K, Lanctot DA, Feudtner C. How parents of children receiving pediatric palliative care use religion, spirituality, or life philosophy in tough times. Journal of Palliative Medicine. 2011 Jan;14(1):39-44.
• FICA Spiritual Assessment Tool (Puchalski 2010)
• Link between spiritual coping and outcome for adolescents Grossoehme,
D.H., et al., Is adolescents' religious coping with cystic fibrosis associated with the rate of decline in pulmonary function?-A preliminary study. J Health Care Chaplain, 2013. 19(1): p. 33-42.; Reynolds, N., S. Mrug, and K. Guion, Spiritual coping and psychosocial adjustment of adolescents with chronic illness: the role of cognitive attributions, age, and disease group. J Adolesc Health, 2013. 52(5): p. 559-65.
• Focused on relieving pain, distressing symptoms & stress of a serious illness
• Appropriate at any age and at any stage, together with curative treatment
• Goal is to improve quality of life for child/family
Curative Care? Or Pediatric Palliative Care? Well...the answer is yes!
Assumption # 6:
• Parents have to choose between “Fighting For a Cure” or “To Give Up”
• PPC translates into “Giving Up Hope” and “Doing Nothing”

...in face of serious illness
Hope in face of serious illness• Engaging in advance care planning
increases knowledge without diminishing hope, increasing hopelessness, nor inducing anxiety in adult patients with advanced cancer. Green, M.J., et al., Advance Care Planning Does Not Adversely Affect Hope or Anxiety Among Patients With Advanced Cancer. J Pain Symptom Manage, 2015. 49(6): p. 1088-96.
• Disclosure of a terminal prognosis does not mean loss of patient hope. Instead, hope was redefined on a goal other than cure. Coulourides Kogan, A., M. Penido, and S. Enguidanos, Does Disclosure of Terminal Prognosis Mean Losing Hope? Insights from Exploring Patient Perspectives on Their Experience of Palliative Care Consultations. J Palliat Med, 2015. 18(12): p. 1019-25.
• Many pediatric MDs/NPs/RNs feel prepared to actively participate in advanced care directives, but that does not always translate into action Sanderson, A., A.M. Hall, and J. Wolfe, Advance Care
Discussions: Pediatric Clinician Preparedness and Practices. J Pain Symptom Manage, 2016. 51(3): p. 520-8.
• Most clinicians (90.3%) believed they were prepared to elicit parent's hopes (however only 21.2% patient's hopes)
• Notably, 40% of clinicians believe that caring for patients with poor prognoses is depressing, and this was more common among less-experienced
Continued treatment in face of serious illness
• Parents and pediatric patients may opt for continued treatment of underlying disease even when there is no realistic hope for cure Wolfe, J., et al. (2000) Understanding of prognosis among
parents of children who died of cancer: Impact on treatment goals and integration of palliative care. Journal of American Medical Association 284(19), 2469–2475. Goldman, A., Heller, K.S. (2000) Integrating palliative and curative approaches in the care of children with life-threatening illnesses. Journal of Palliative Medicine 3(3), 353–359.
• Motivated either by hope for a miracle, desire to extend life, or desire to palliate symptoms related to progressive disease
• In discussions of treatment options with families, Wolfe and Grier suggest “The very nature of miracles is that they are rare. However, we have seen miracles, and they have occurred both on and off treatment” Pizzo, P.A., Poplack, D.G. (Eds) (2002)
Principles and Practice of Pediatric Oncology (4th edn). Philadelphia, PA: Lippincott Williams & Wilkins.

Continued treatment in face of serious illness
• In other words, a child does not have to continue on disease-directed therapy in order to preserve hope, especially when the therapy significantly impacts child’s remaining quality of life
• Regardless, decisions regarding continued disease-directed therapy need to be carefully considered, weighing the potential for life extension and impact on quality of life.
• Oncology: Placing DNR/AND order did not result in reduction of the level, quality and priority of children’s medical care Baker JN, Kane JR, Rai S, Howard SC, Hinds PS; PCS Research Working Group.Changes in medical care at a pediatric oncology referral center after placement of a do-not-resuscitate order. J Palliat Med. 2010 Nov;13(11):1349-52.
• Even when the underlying condition can not be cured, sophisticated medical technology will be used to control symptoms and improve a child quality of life
• It is a very active and advanced approach to pain & symptom management and family support
Hope
• Caring for a dying child is emotionally very difficult
• It may be particularly challenging for physicians and other caregivers to consider the integration of palliative care because this may be perceived as ‘giving up’
• More importantly, parental loss of a child is certainly considered to be the most difficult type of loss Saunders, C.M. (1979–1980) A comparison of adult bereavement in the death of a spouse, child, and parent. Omega 10, 302–322.: Whittam, E.H. (1993) Terminal care of the dying child. Psychosocial implications of care. Cancer 71(10 Suppl.), 3450–3462.
• As a result, the emotional cost of recognizing that a child may die impedes planning for optimal care and support.
Cheat-Sheet Hope Language 1/2 • Tell me about little Claire on a
good day! Do you have any pictures?
• Considering what little Johnny is up against, what are you hoping for?
• I am hoping for a miracle, too. And I have seen miracles, but they are very rare and happen on treatment or off treatment...
• Just in case, the miracle or the cure is not going to happen (...if God/Allah has different plans for Sarah), what else are you hoping for?
• We want to make sure that Karen lives as long as possible, as well as possible!
• We are hoping for the best, but preparing for the worst.
• “He is not dying because he is not eating...he is not eating, because he is dying...”

Cheat-Sheet Hope Language 2/2
• So what I hear you saying, is the following...
• Did I get this right...?
• Then I would recommend the following...
• DNR/DNI (AND, limiting of painful interventions)
• I recommend to put in an order to protect your daughter from experiencing painful situations, such as chest compressions or intubation, in case the breathing or heart stops - are you fine with that?
Assumption # 7:
Increasing the dose of opioids causes respiratory depression and quickens death
(Morphine = Euthanasia?)
Opioids for Pain & Dyspnea• "Morphine kills the pain, not
the patient" MD killing patient in name of pain relief is not merciful, just incompetent Sykes, N.P., Morphine kills the
pain, not the patient. Lancet, 2007. 369(9570): p. 1325-6.
• An enduring misconception is the belief that in the management of pain and dyspnea, opioids will hasten death and should only be administered as a last resort. This was contradicted in the adult literature... Thorns A, Sykes N. Opioid use in last week of life and implications for end-of-life decision-making.Lancet. 2000;356:398-399.,
• ...and our PPC team commonly observes that administering opioids and/or benzodiazepines, together with comfort care to relieve dyspnea and pain, not only prolongs life but also improves the child’s quality of life. Friedrichsdorf SJ: Pain management in children with advanced cancer and during end-of-life care. Pediatr Hematol Oncol. 2010 May;27(4):257-61.
• Retrospective cohort study (n=223 adult oncologic patients) Lopez JM. Opioid use at the end of life and survival in a Hospital at Home unit. Journal of Palliative Medicine. 2010 Sep;13(9):1079-83.
Mean Survival:
• < 2-fold increase in their initial opioid dose = 9 days
• > 2-fold increase in their initial opioid dose = 22 days

Assumption # 8:
PPC takes patients away from primary care / pediatric specialists
Primary versus Subspecialty PPC
• Why is it, that we ask an infectious disease specialist for a consult, if we can prescribe antibiotics ourselves?
Primary PPC
• Team provides interdisciplinary support and integrates a palliative care approach
Subspecialty PPC
• Clinical: more complex care
• Skills in advanced pain & symptom management
• Education: enhance knowledge, skills, attitudes & behaviors
• Innovation and research: advancing the field
• Advocacy: system wide changes
Pediatric Palliative Care Consult• Complementary
• “How can we help...?”
• May involve second opinion regarding
• Decision making
• Symptom management
• Coordination of care
• Home care

Assumption # 9:
A part time (0.2 FTE) physician can certainly address all pertinent PPC issues in a Children’s Hospital
PPC• PPC applies to all children with
life-threatening illness
• PPC Specialists provide:
• Direct patient consultation
• Advocacy
• Education
• Quality Improvement
• Research
PPC Example...
• “If you have seen one Pediatric Palliative Care program ...
• ... you have seen one Pediatric Palliative Care program!

Conclusions
Ghostbusters, 1984
Not providing PPC to children with serious illness is now considered “bad”
ConclusionsPediatric Palliative Care is...
• Specialized medical care for children with serious illness
• Focused on relieving pain, distressing symptoms & stress of a serious illness
• Appropriate at any age and at any stage, together with curative treatment
• Goal is to improve quality of life for child/family
• Provided by an interdisciplinary team who work with the patient’s other physicians & health care providers: provides an extra layer of care
• P.S.: Morphine & Midazolam do not shorten a child’s life
Conclusions• Hope and PPC include each
other
• Pediatric Palliative Care:
• Multi--> Inter---> Trans-disciplinary Team
• (1) “How can we help?”
• (2) Then listen…

"If you can't add life to my son's days, then don't add days to my son's life" Father of a toddler to Dr. Sunny Anand on PICU
Twitter: @NoNeedlessPain
Stefan J. Friedrichsdorf, MD, FAAP Medical Director, Department of Pain Medicine, Palliative Care & Integrative Medicine
Associate Professor of Pediatrics, University of Minnesota Medical School
Children's Hospitals and Clinics of Minnesota2525 Chicago Ave S | Minneapolis, MN 55404 | USA
612.813.6450 phone | 612.813.7199 fax
[email protected]://www.childrensmn.org/painpalliativeintegrativemed
Further Training
10th Annual Pediatric Pain Master Class • Minneapolis, Minnesota, USA | June 17-23, 2017
Education in Palliative & End-of-life Care [EPEC]: Become an EPEC-Pediatrics Trainer • Montréal, Québec, Canada | April 29-30, 2017 (Professional Development Workshop: 04/28/17)
Contact: [email protected]
Blog: http://NoNeedlessPain.org