-
Double-BundleReconstruction of theAnterior Cruciate
Ligament:Anatomic andBiomechanical Rationale
AbstractPatients continue to suffer residual pain and
instability followinganterior cruciate ligament reconstruction.
Although overalloutcomes of anterior cruciate ligament
reconstruction arefavorable, improved outcomes can be achieved.
Recentbiomechanical studies have questioned the ability of
conventionalsingle-bundle anterior cruciate ligament constructs to
adequatelyrestore normal knee kinematics. Consequently, the use of
double-bundle anterior cruciate ligament constructs has
beenrecommended to restore knee stability more effectively.
Recentbiomechanical data indicate that double-bundle anterior
cruciateligament reconstruction may provide better anteroposterior
androtational knee stability than do conventional
single-bundletechniques. Studies are needed to evaluate the
clinical impact ofdouble-bundle reconstruction techniques on
long-term functionaloutcomes.
Surgical management of anteriorcruciate ligament (ACL)
defi-ciency has been the subject of in-creased interest for the
past severaldecades. Surgical techniques haveadvanced from direct
repair and extra-articular reconstructions to mini-mally invasive
arthroscopic tech-niques, with various graft choices,sophisticated
fixation options, andadvanced rehabilitation protocols.
Most current ACL reconstructiveprocedures have focused on
arthro-scopic reconstruction of the antero-medial (AM) bundle of
the ACL,with little regard for the posterolat-eral (PL) bundle.
Although most pa-tients have no detectable residual in-
stability following single-bundleACL reconstruction, a subset of
pa-tients has residual instability andpain. Recent reports of ACL
recon-struction have demonstrated that aconsiderable number of
patientshave persistent anteroposterior lax-ity and a persistent
pivot shift; manypatients will not return to their pre-vious level
of athletic activity afterACL reconstruction.1-4 Moreover, re-cent
in vivo studies have shown thatsingle-bundle ACL
reconstructionsufficiently restores the anteroposte-rior tibial
translation but is associat-ed with increased internal tibial
ro-tation during running activities.5
These results prompted knee sur-
Boris A. Zelle, MD
Armando F. Vidal, MD
Peter U. Brucker, MD, MSc
Freddie H. Fu, MD, DSc (Hon),
DPs (Hon)
Dr. Zelle is Resident, Department ofOrthopaedic Surgery,
University ofPittsburgh School of Medicine,Pittsburgh, PA. Dr.
Vidal is AssistantProfessor, Department of OrthopaedicSurgery,
University of Colorado atDenver and Health Science Centers,Denver,
CO. Dr. Brucker is ResearchFellow, Department of
OrthopaedicSurgery, Division of Sports Medicine,University of
Pittsburgh. Dr. Fu isChairman and David Silver Professor,Department
of Orthopaedic Surgery,Division of Sports Medicine, Universityof
Pittsburgh.
None of the following authors or thedepartments with which they
areaffiliated has received anything of valuefrom or owns stock in a
commercialcompany or institution related directly orindirectly to
the subject of this article:Dr. Zelle, Dr. Vidal, Dr. Brucker,
andDr. Fu.
Reprint requests: Dr. Fu, Department ofOrthopaedic Surgery,
University ofPittsburgh School of Medicine,Kaufmann Building, Suite
1011, 3471Fifth Avenue, Pittsburgh, PA 15213.
J Am Acad Orthop Surg 2007;15:87-96
Copyright 2007 by the AmericanAcademy of Orthopaedic
Surgeons.
Perspectives on Modern Orthopaedics
Volume 15, Number 2, February 2007 87
-
geons to devise a double-bundle ACLreconstruction technique with
thegoals of achieving a more anatomicrestoration of the ACL and its
twobundles and of improving knee sta-bility and patient
outcomes.6-16
Historical Perspective
Initial reports of double-bundle ACLreconstruction appeared in
the liter-ature in the 1980s.14,17 In 1983,Mott17 described a
double-bundleACL reconstruction technique usingsemitendinosus
autograft throughtwo separate tibial and femoral tun-nels. In 1987,
Zaricznyj14 described adouble-bundle ACL reconstructiontechnique
using a single femoraltunnel and two tibial tunnels. He re-ported
good to excellent results in 12of 14 patients at an average of
3.6years postoperatively.14
Radford and Amis18 studied thebiomechanical significance of
recon-structing both bundles of the ACL.They believed that the
normal func-tion of the ACL was too complex tobe recreated using
standard single-bundle techniques. They hypothe-sized that ACL
behavior might be
modeled more closely by implantswhich seek to duplicate its
complex-ity.18 These authors compared thebiomechanical
characteristics of bothover-the-top and
through-the-condylesingle-bundle reconstructions with
adouble-bundle reconstruction con-sisting of a posterolateral graft
passedthrough a femoral drill hole and ananteromedial graft in the
over-the-top position. The double-bundle re-construction was the
only constructthat reproduced the function of theintact ACL at both
20 and 90 ofknee flexion.
Radford et al19 subsequently stud-ied the in vivo effects of
double-bundle reconstruction in a sheepmodel using synthetic
polyestergrafts. In the double-bundle group,the authors reported
increased boneresorption at the bone tunnels, asubsequent increase
in anteriortranslation, and more pronounceddegenerative changes.
Their conclu-sions were limited by the animalmodel and choice of
graft. Despitethese limitations, the authors rec-ommended that
double-bundle re-constructions in ACL surgery werenot indicated.
Subsequently, double-
bundle reconstruction for ACL in-sufficiency received limited
atten-tion in the literature for manyyears.
Clinical reports and more sophis-ticated biomechanical studies
ofdouble-bundle ACL reconstructionsappeared in the literature 5
yearslater.6-13,15,16,20 Several studies de-scribed different
techniques and graftoptions. As techniques developed,sophisticated
methods of studyingthe biomechanical influences of graftplacement
and geometry furtherdeepened understanding of the influ-ence of
both conventional single-and double-bundle reconstructionson knee
kinematics.13,20-22 Specifi-cally, the ability to evaluate the
in-fluence of graft placement on bothanterior translation and
coupled ro-tation greatly advanced the under-standing of the PL
bundle and its rolein both knee kinematics and ACL
re-construction.
Anatomy andBiomechanics
Anatomy of the AnteriorCruciate Ligament
The ACL consists of dense con-nective tissue enveloped in a
syn-ovial membrane, which places theligament in an intra-articular
but ex-trasynovial position.23,24 The liga-ment originates from a
fossa on theposterior aspect of the lateral femo-ral condyle and
runs in an obliquecourse distally, anteriorly, and medi-ally to
insert between the medialand lateral spines of the tibial pla-teau.
The ACL attaches to the femurand the tibia, not as a singular
cord,but rather as a collection of fasciclesthat fan out as they
approach theirinsertion sites.23-27 The area of inser-tion is 3 to
3.5 times larger than thecross-sectional area of the
ligamentmidsubstance.27 The cross-sectionalarea of the midsubstance
ACL is ap-proximately 36 to 44 mm2,28 whilethe cross-sectional area
of the femo-ral and tibial insertion sites is be-tween 113 and 136
mm2.27 This
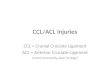
Figure 1
Location of the anteromedial bundle (AMB) and posterolateral
bundle (PLB) of theanterior cruciate ligament in a left knee. The
AMB attaches more proximally to thelateral femoral condyle (LFC)
than does the PLB. The PLB runs more nearlyhorizontally and
attaches more distally to the LFC. MFC = medial femoral condyle,PCL
= posterior cruciate ligament
Double-Bundle Reconstruction of the Anterior Cruciate
Ligament
88 Journal of the American Academy of Orthopaedic Surgeons
-
anchor-shaped design of the relative-ly broad ACL footprint may
serve tominimize stresses on the ligament-bone interface.27
The ACL consists of individual fi-ber bundles (Figure 1).
Palmer29 firstprovided anatomic descriptions ofthe ACL bundles in
the 1930s. Re-searchers have since confirmed thatthe ACL consists
of two separateand functionally distinct anatomicbundles.23,26,27
These bundles dem-onstrate clearly different biome-chanical
properties and tensioningpatterns with varying degrees ofknee
flexion.30,31
Each bundle is named accordingto its insertion on the tibial
foot-print. On the tibial side, the AMbundle inserts anteromedially
andthe PL bundle inserts posterolateral-ly. On the femoral side,
the AM bun-dle originates more proximally thandoes the PL
bundle24,26,27 (Figure 2).On the whole, the AM and PL bun-dles
comprise relatively equal pro-portions of the overall ligament
in-sertion on both the femoral andtibial footprints.27
Physiologic Function of theAnterior Cruciate LigamentBundles
Biomechanical investigationshave demonstrated that the ACL
fi-ber bundles are not isometricthroughout knee flexion and
exten-sion. The AM bundle tightens inflexion and the PL bundle
relaxes,whereas in extension, the PL bundletightens and the AM
bundle relax-es.23,32,33 Cadaveric investigationshave demonstrated
that both the AMand PL bundles show their maxi-mum shortening peak
at 30 of kneeflexion. In extension from this posi-tion, the PL
bundle elongates. Con-versely, with increasing flexion, theAM
bundle elongates while thelength of the PL bundle
essentiallyremains constant.33
In response to anterior and com-bined rotatory loads, forces are
dis-tributed differentially between theAM and the PL bundles.
Sakane et
al31 evaluated the magnitude of thein situ forces within the
individualbundles of the ACL in response toapplied anterior loads
at varyingknee flexion angles. The highest insitu force within the
PL bundle in re-sponse to an anterior load occurredbetween 0 and 45
of knee flexion,with a maximum in situ forcereached at 15. Between
0 and 15 ofknee flexion, the in situ forceswithin the PL bundle in
response toan anterior load were significantlyhigher (P < 0.05)
than those observedin the AM bundle. In contrast, themagnitude of
the in situ forceswithin the AM bundle in responseto an anterior
load was relativelyconstant throughout knee flexionand
extension.
Similar results were obtained byGabriel et al,30 who
investigated thedistribution of the in situ forces inthe ACL in
response to both anteriorand combined rotatory loads.
Theydiscovered that in response to an an-terior tibial load of 134
N, the in situforce in the PL bundle increased withknee extension
and decreased withknee flexion. In extension, the in
situ force in the AM bundle in re-sponse to anterior loads was
lowerthan in the PL bundle. However, theforces in the AM bundle
increasedwith knee flexion, reaching a maxi-mum at 60. In response
to a com-bined rotatory load of 10 Nm valgustorque and 5 Nm
internal tibialtorque, the AM bundle experiencedgreater in situ
forces than did the PLbundle at 15 and 30 of knee flexion.However,
both bundles demon-strated significant (P < 0.05) in situforces
in response to a combined ro-tatory load, especially at 15.
Evaluations of the length changepatterns and in situ forces in
the in-dividual bundles of the ACL indicatethat both the AM and PL
bundles areimportant to the stability of the kneejoint. The AM
bundle is an impor-tant stabilizer of the knee in flexion,whereas
the PL bundle acts as a sta-bilizer against anterior loads whenthe
knee is in extension. Both theAM and the PL bundles provide
sig-nificant contributions to the stabil-ity of the knee in
response to com-bined rotatory loads.
Figure 2
Tibial and femoral insertion sites of the left knee. A, On the
femoral side, theanteromedial (AM) bundle inserts more proximally
than the posterolateral (PL)bundle. B, On the tibial side, the AM
bundle inserts anteromedially and the PLbundle inserts
posterolaterally. ANT = anterior, DIST = distal, POST =
posterior,PROX = proximal
Boris A. Zelle, MD, et al
Volume 15, Number 2, February 2007 89
-
Biomechanics ofSingle-Bundle VersusDouble-Bundle
ACLReconstruction
In 1994, Radford et al19 succinct-ly stated that single-bundle
ACL re-constructions are a great simplifi-cation of the complexity
of thenatural ligament structure and thatit would therefore be
surprising ifsuch a reconstruction were capableof recreating all
the subtleties of nor-mal knee behavior. The advent ofnewer
biomechanical testing meth-ods has resulted in a better
appreci-ation of knee kinematics followingACL reconstruction. The
use ofrobotic/universal force-moment sen-sor testing systems has
allowed re-searchers to assess knee kinematicsin cadaveric models
with multipledegrees of freedom. Additionally,these systems allow
for assessmentof the in situ forces within recon-structed ligaments
in response toknown loads and translations.13,20-22
Recently, Woo et al22 demon-strated in vitro that
conventionalsingle-bundle ACL reconstructionsare relatively
successful at limitinganterior translation of the tibia in
re-sponse to anterior-directed tibialloads, but they are
ineffective at re-sisting combined rotatory loads.These
investigators believed thatconventional single-bundle tech-niques
place the graft too close to thecentral axis of the knee, thus
limit-ing the ability of the graft to resist ro-tatory loads.
Several biomechanical studieshave since been published
docu-menting the superiority of double-bundle techniques at
limiting notonly anterior translation but, moreimportantly,
translation in responseto combined rotatory loads. In a ca-daveric
study, Mae et al34 demon-strated that double-bundle
ACLreconstruction using hamstring ten-don grafts and two femoral
tunnelsprovides greater anterior stabilitythan do current
single-bundle tech-niques.
Yagi et al13 observed that double-
bundle ACL reconstruction is moresuccessful at restoring knee
kine-matics to normal than is conven-tional single-bundle ACL
recon-struction, which simply reconstructsthe AM bundle. In an in
vitro study,these authors demonstrated that, onapplication of an
anterior tibial loadof 134 N, anterior tibial translationwas
significantly (P < 0.05) closer tonormal with double-bundle
ACLreconstruction than with single-bundle ACL reconstruction.
Addi-tionally, with application of a com-bined rotatory load of 10
Nm valgustorque and 5 Nm internal tibialtorque at 30 of knee
flexion, the ki-nematics of the double-bundle re-construction were
significantly (P