Embed Size (px)
Citation preview

GENERAL CAUSAL FACTORS IN PHYSICAL ILLNESSAND DISEASEGenetic FactorsPsychosocial FactorsSociocultural Factors
Health Problems andBehavior
PSYCHOLOGICAL FACTORS IN HEALTH ANDDISEASEStress and the Stress ResponseBiological Costs of StressStress and the Immune SystemPsychoneuroimmunologyLifestyle Factors in Health and IllnessHealth, Attitudes, and Coping Resources
CARDIOVASCULAR DISEASEHypertensionCoronary Heart DiseaseWhat Psychological Factors Are Implicated in
Cardiovascular Disease?
TREATMENTS AND OUTCOMESBiological InterventionsPsychological InterventionsSociocultural Approaches
UNRESOLVED ISSUES:Does Clinical Practice Ignore the
Doctor-Patient Relationship?

re you under a lot of stress? Do you feel socially isolated? Do you tend often to berather hostile and angry? There is now a growing recognition that what we are likeas people and the way we live our lives have important implications for our over-all health and physical well-being.
You may have noticed that when you are tired or have a cold, you seem to havea much lower tolerance for psychological stress. You may also have observed thatwhen you are emotionally upset or are feeling pressured in some way, your bodyseems to have a lower resistance to physical disease. The medical profession hastraditionally concentrated on understanding and treating anatomical and physio-logical factors in disease. In psychopathology, on the other hand, the main focus ofinterest has been to identify and remedy psychological factors associated withmental disorders. Now we are coming to understand that, although a disorder maybe primarily physical or primarily psychological, it is always a disorder of the wholeperson - not just of the body or of the psyche. In other words, there is now a grow-ing appreciation for how the mind and the body work in concert.
A person's overall life situation influences when a disorder first develops and thenature, duration, and prognosis of that disorder. Recovery is likely to be more rapidfor a patient who is eager to get back to work and to family than for the person whowill be returning to a frustrating job or an unpleasant home life. In addition, socio-cultural influences affect the types and incidence of disorders found in members ofdifferent cultures and different gender and age groups. For example, men die anaverage of 7 years earlier than women; mortality from stroke in the United States is10 percent higher than average in 11 southern states that make up the "Stroke Belt"(e.g., Alabama, Arkansas, and Georgia); African-Americans have more coronary heartdisease than Caucasians; Latinos are less likely to smoke daily than are Caucasians;and Asian-Americans and Pacific Islanders are among the healthiest groups in theUnited States (see Whitfield et al., 2002). The ailments to which people are most vul-nerable-whether physical, psychological, or both-are determined in no small partby who we are, where we live, and how we live (see Figure 10.1).
Behavioral medicine is an interdisciplinary field thatfocuses on the role that psychological factors play in theoccurrence, maintenance, and prevention of medical prob-lems. The field of behavioral medicine naturally involvesprofessionals from many disciplines (such as medicine,psychology, and sociology) who take into account bio-
logical, psychological,and sociocultural influ-ences when consideringa person's health andwell-being.
Health psychologyis a psychological sub-specialty within behav-ioral medicine. It dealswith psychology's con-tributions to the diag-nosis, treatment, andprevention of psycho-
People who are hostile are more likely to
develop cardiovascular disease.
logical components of medical problems. Over the last30 years, the field has developed rapidly and has had anotable impact on almost the entire range of clinical med-icine (Belar, 1997; Smith, Kendall & Keefe, 2002; Smithet al., 2005).
A behavioral medicine approach to physical illness isconcerned with the following types of issues (adaptedfrom Gentry, 1984).
The psychological factors that may predispose anindividual to physical illness. Such psychological fac-tors include critical life events, particular types ofbehavior, and personality.
The ways in which the negative effects of stress can bereduced or buffered by personal resources. Examplesof such resources include coping styles, social sup-ports, and certain personality traits.
The biological mechanisms by which human physiol-ogy is altered by stressors, particularly those arising

Death rates per100,000 population
o 289.4 to 325.0
CJ 325.1 to 347.8
348.5 to 388.6
o 388.8 to 465-4
PuertoRico=
Death rates per100,000 population
o 128.4 to 167.5
C 168.1 to 192.6
194.8 to 211.8
o 212.8 to 259.9
PuertoRico=
Death rates per100,000 population
o 42.9 to 58.5
C 58.9 to 61.4
61.5 to 67.2
o 67.6 to 86.0
FIGURE 10.1Age-Adjusted Death Ratesby State
Source: American Heart Association(2002).
from maladaptive behavior, and the effects of stresson the immune, endocrine, gastrointestinal, and car-diovascular systems, among others.
The psychological processes involved in the healthchoices individuals make with respect to such matters
as hazardous lifestyles, health care decisions, andadherence to preventive regimens.The factors that determine compliance with soundmedical advice. These include the nature of the rela-tionship between the medical practitioner and the

patient, cultural factors, and personal factors (e.g.,denial of illness).
The effectiveness of psychological measures, such ashealth education and behavior modification, in alter-ing unhealthful lifestyles and in directly reducing ill-ness at both individual and community levels.
Consider, for example, the case of Joe, a 52-year-oldman who is suffering from depression. As you will soonlearn, Joe's depression may also contribute to the advance-ment of his cardiovascular disease (Glassman & Shapiro,1998; Smith & Ruiz, 2002). And it may hinder efforts totreat his heart problems by making Joe less likely to adhereto a prescribed exercise regimen (it's hard to exercise whenyou are depressed and have no interest in things). Thebehavioral medicine perspective gives health practitionersextra tools for conceptualizing and treating health prob-lems like Joe's. It encourages them to consider job and/orfamily circumstances that, if addressed, might make treat-ment of the primary medical problem more successful. Farfrom being merely supplementary, the behavioral medi-cine viewpoint may be critical in determining clinical out-comes, including survival versus death.
Years ago, the disorders in which psychological factorswere thought to playa role were called "psychosomatic dis-orders" (Alexander, 1950; Dunbar, 1943). Now, the termpsychophysiological disorders is preferred. Althoughsome people may think that the word psychosomatic meansthat a disorder is "all in your head," these are not imaginarydisorders but medical conditions that involve real symp-toms. In addition, whereas the focus in earlier times was ona limited set of disorders thought to be caused primarily bypsychological factors (e.g., ulcers, chronic headaches,asthma, and cardiovascular disease), we now view psycho-logical factors as important for almost any health problem.We have also discovered that some of the medical prob-lems that were thought to have purely psychological ori-gins can also have non psychological causes. For example,one important cause of gastric ulcers is the Helicobacterpylori bacterium. However, only about one in every fivepeople who has H. pylori develops an ulcer (Peek & Blaser,1997), and ulcers can also develop in the absence of thisbacterium (Ciociola et aI., 1999). This is because majorstressors (earthquakes, economic disasters) and commonlifestyle factors (skipping breakfast, use of stomach-irritating medications such as aspirin or ibuprofen, lack ofsleep) are also important in the development of ulcers (seeLevenstein, 2002).
To recognize that psychological problems can bedirectly related to medical problems, Axis I of DSM -IV-TRprovides a major category called "Mental Disorders Dueto a General Medical Condition" (American PsychiatricAssociation, 2000, p. 181). This diagnosis is to be usedwhen a general medical condition has played a direct rolein the development of a psychological disorder. Some cases
of depression, for example, are caused by an underactivethyroid.
The other side of the same coin is that psychologicalfactors can also playa role in the development, aggrava-tion, or maintenance of physical health problems.DSM -IV-TR acknowledges this with its reference to "Psy-chological Factors Affecting a General Medical Condition"(American Psychiatric Association, 2000, p. 731). Here thefocus is on psychological factors that have a "clinically sig-nificant effect on the course or outcome of a general med-ical condition." An individual who has high blood pressureand heart disease but who refuses to give up eating highlysalted junk food would fall into this category. The psycho-logical factor (here, the maladaptive behavior of unhealth-ful eating) is coded on Axis I, and the medical problem(here, cardiovascular disease) is coded on Axis III. Anotherexample is a man with schizophrenia who hears voicestelling him to refuse dialysis for his kidney disease (seeMorrison, 1995, p. 534). In this case, the schizophreniawould be coded on Axis I and the chronic renal failure onAxis III. Other psychological factors that could be codedon Axis I include hostile personality traits (linked to coro-nary artery disease, CAD, on Axis III), alcohol abuse(linked to liver problems), and the like.
PSYCHOLOGICALFACTORS IN HEALTHAND DISEASETo understand how psychological factors may playa role inkeeping us healthy or in making us sick, it is first necessaryto understand something about the way our bodies reactboth to stress and to challenges by infectious or toxicagents such as viruses and bacteria.
Stress and the Stress ResponseAs we have already discussed in Chapter 5, a stress responseinvolves a cascade of biological changes that prepares theorganism for the fight-or-flight reaction. The stressresponse begins in the hypothalamus, which stimulates thesympathetic nervous system (SNS). This, in turn, causesthe inner portion of the adrenal glands (the adrenalmedulla) to secrete adrenaline and noradrenaline. As thesecirculate through the blood, they cause an increase in heartrate (familiar to all of us). They also get the body to metab-olize glucose more rapidly.
In addition to stimulating the SNS, the hypothalamusreleases a hormone called "corticotropin-releasing hor-mone" (or CRH). Traveling in the blood, this hormonestimulates the pituitary gland. The pituitary then secretesadrenocorticotrophic hormone (ACTH), which induces

the adrenal cortex (the outer portion of the adrenal gland)to produce the stress hormones called "glucocorticoids." Inhumans, the stress glucocorticoid that is produced is calledcortisol. Figure 10.2 illustrates this sequence of events.
Cortisol is a good hormone to have around in anemergency. It prepares the body for fight or flight. It alsoinhibits the innate immune response. This means that if aninjury does occur, the body's inflammatory response to it isdelayed. In other words, escape has priority over healing,and tissue repair is secondary to staying alive. This obvi-ously has survival value if you need to run away from a lionthat has just mauled you. It also explains why cortisoneinjections are sometimes used to reduce inflammation indamaged joints.
But there is also a downside to cortisol. If the cortisolresponse is not shut off, cortisol can damage brain cells,especially in the hippocampus (see Sapolsky, 2000). At avery fundamental level, stress is bad for your brain. It mayeven stunt growth (babies who are stressed don't gainweight in the normal way and "fail to thrive"). Accordingly,the brain has receptors to detect cortisol. When these areactivated, they send a feedback message that is designed todampen the activity of the glands involved in the stressresponse. These are the ones described in Figure 10.2,which illustrates the HPA axis (the hypothalamic-pitu-itary-adrenal axis). But if the stressor remains, the HPAaxis stays active and cortisol release continues. Althoughshort-term cortisol production is higWy adaptive, a chron-
FIGURE 10.2The Hypothalamic-Pituitary-Adrenal (HPA) AxisProlonged stress leads to secretion of the adrenal hormonecortisol, which elevates blood sugar and increases metabolism.These changes help the body sustain prolonged activity but atthe expense of decreased immune system activity.Source: j. W. Kalat. Biological Psychology, 7th ed. Be/mont, CA:Wadsworth, 2001.
ically overactive HPA axis, with high levels of circulatingcortisol, may be more problematic.
Biological Costs of StressThe biological cost of adapting to stress is called theallostatic load (McEwan, 1998). When we are relaxed andnot experiencing stress, our allostatic load is low. When weare stressed and feeling pressured, our allostatic load willbe higher. Although efforts to relate specific stressors tospecific medical problems have not generally been success-ful, stress is becoming a key underlying theme in ourunderstanding of the development and course of virtuallyall physical illness. Moreover, the focus is now not just onmajor stressors such as job loss or the death of a loved one,but also on daily stressors such as commuting, unexpectedwork deadlines, or even computer problems (Almeida,2005). These ideas are in keeping with the diathesis-stressmodel we discussed in Chapter 3. For example, a personwith allergies may find his or her resistance further low-ered by emotional tension; similarly, as we will see, when avirus has already entered a person's body-as is thought tobe the case in multiple sclerosis, for example-emotionalstress may interfere with the body's normal defensiveforces or immune system. In like manner, any stress maytend to aggravate and maintain certain disorders, such asmigraine headaches (Levor et aI., 1986) and rheumatoidarthritis (Affleck et aI., 1994; Keefe et aI., 2002).

When aural/astatic load is high, we experience the biological signsof stress including high heart rate and increased levels of cortisol.
Stress and the Immune SystemThe link between stress and physical illness involves dis-eases (like colds) that are not directly related to nervoussystem activity. This suggests that stress may cause anoverall vulnerability to disease by compromising immunefunctioning. We turn now to this issue.
We have already seen how glucocorticoids can causestress-induced immunosuppression. In the short term, thiscan be adaptive (escape first, heal later). However, it is easyto see how longer-term stress might compromise thebody1s ability to heal and to fIght infections. 'P-arlystudiesthat examined the association between stress and immune
functioning rapidly established an assoClatlOn betweenstressful circumstances (e.g., medical school exams) anddiminished immune reactivity. Such diminished immunereactivity would make a person more susceptible to infec-tions. There may be substantial individual differences inthis type of reactivity to stress (Kosslyn et al., 2002;Manuck et al., 1991). To appreciate why this might be, weneed to describe briefly the basics of immune functioning.
The word immune comes from the Latin immunis,
which means "exempt:' The immune system protects thebody against such things as viruses and bacteria. It hasbeen likened to a police force (Kalat, 1998). If it is too weak,it cannot function effectively, and the body succumbs todamage from invading viruses and bacteria. Conversely, ifthe immune system is too strong and un selective, it canturn on its own normal cells. This is what may happen inthe case of autoimmune diseases such as rheumatoidarthritis and lupus.
The front line of defense in the immune system is thewhite blood cells. These leukocytes (or lymphocytes) areproduced in the bone marrow and then stored in variousplaces throughout the body, such as the spleen and thelymph nodes. There are two important types ofleukocytes.One type, called a B-cell because it matures in the bonemarrow, produces specific antibodies that are designed torespond to specific antigens. Antigens (the word is a con-traction of antibody generator) are foreign bodies such asviruses and bacteria, as well as internal invaders such astumors and cancer cells. The second important type ofleu-cocyte is the T-cell (so named because it matures in thethymus, which is an important endocrine gland). Whenthe immune system is stimulated, B-cells and T-cellsbecome activated and multiply rapidly, mounting variousforms of counterattack (see Figure 10.3).
T-cells circulate through the blood and lymph sys-tems in an inactive form. Each T-cell has receptors on itssurface that recognize one specific type of antigen. How-ever, the T-cells are unable to recognize antigens by them-selves. They become activated when immune cells called"macrophages" (the word means "big eater") detect anti-gens and start to engulf and digest them. To activate theT-cells, the macrophages release a chemical known asinterleukin-l. Interleukins are a class of chemicals calledcytokines. Cytokines are chemical messengers that appearto be of crucial importance for health (see Developmentsin Research 10.1). With the help of the macrophages, theT-cells become activated and are able to begin to destroyantigens (Maier et al., 1994).
B-cells are different in structure from T-cells. When aB-cell recognizes an antigen, it begins to divide and to pro-duce antibodies that circulate in the blood. This process isfacilitated by cytokines that are released by the T-cells. Pro-duction of antibodies takes 5 days or more (Maier et al.,1994). However, the response of the imm une system will bemuch more rapid if the antigen ever appears in the future,because the immune system has a "memory" of the invader.

Bacteriaenter throughpuncturedskin
Virgin B-cellbinds
Macrophage envelopsthe antigen
Some B-cell progenydifferentiate into memory cellsthat prepare an early defensein case the antigen returns
Macrophage displaysthe antigen portion ofthe bacteria
.1 Cytokines: The Linkbetween the Brain andthe Immune System
C ytokines are chemical messengers that allowimmune cells to communicate with each other.Cytokines are small protein molecules-youcan think of them as being like hormones ofthe immune system. Currently there are about
18 known cytokines, although more may have been identi-fied by the time you read this. A cytokine that you mayalready have heard about is interferon, which is given topatients with cancer, multiple sclerosis, and hepatitis C.
Cytokines play an important role in mediating theinflammatory and immune response (see Kronfol & Remick,2000, for a review). They can be divided into two main cat-egories: pro-inflammatory cytokines and anti-inflammatorycytokines. Pro-inflammatory cytokines such as interleukin-1(iL-1), IL-6, or tumor necrosis factor help us deal with chal-lenges to our immune system by augmenting the immuneresponse. In contrast, anti-inflammatory cytokines such asIL-4,IL-10, and IL-13 decrease or dampen the response that
the immune system makes. Sometimes they accomplishthis by blocking the synthesis of other cytokines.
What makes cytokines so interesting is that in addi-tion to communicating with the immune system, they alsosignal to the brain. Because the brain and the immunesystem can communicate via the cytokines, we can regardthe immune system almost as another sensory organ. Farfrom being a self-contained system, the immune systemcan monitor our internal state and send the brain infor-mation about infection and injury. The brain can thenrespond. What this means is that the brain is capable ofinfluencing immune processes. With this in mind, some ofthe findings discussed in this chapter (the link betweendepression and heart disease, for example, and thehealth benefits of optimism and social support) makemuch more sense. In a very tangible way, what is going onat the level of the brain can affect what is going on withthe body, and vice versa.

We also know that IL-1 and other cytokines can stimu-late the HPA axis (see again Figure 10.2). The resultingincrease in cortisol sets off a negative feedback loop that isdesigned to prevent an excessive or exaggerated immuneor inflammatory response. However, if this feedback sys-tem fails and is either too sensitive or not sensitiveenough, serious disorders such as cancer, infection, orautoimmune diseases can develop. Because the brain isalso involved in this feedback loop, emotional factors andpsychosocial stresses may tilt the balance in the feedbackloop in either a helpful or a detrimental way.
One implication of developments in cytokine researchis that disorders of the brain could potentially have "down-stream" effects on the immune system. In the oppositedirection, problems with the immune system may also leadto some behavioral changes or even to psychiatric prob-lems. For example, when you are ill you sleep more, have adiminished appetite, and have little sexual interest. This isclassic sickness behavior. It may also result, at least inpart, from the effects of specific cytokines on the brain.When cytokines such as IL-1 or interferon are injected, sub-jects become lethargic, lose their appetites, and have trou-ble concentrating, among other problems (Reichenberg
et aI., 2001). In short, they have some of the symptoms ofdepression. And when cancer patients are treated withcytokines such as interferon, they experience both flu-likesymptoms and depression, the latter of which is typicallytreated with paroxetine (Paxi!), an antidepressant (Mussel-man et aI., 2001).
A century ago, Bruce and Peebles (1904) noted thatpatients in a mental asylum in Britain had white blood cellsthat were abnormal in type and number. As knowledge ofcytokine biology progresses, we may finally begin tounderstand why this would be. It is plausible to suggestthat mental disorders will be found to have immune conse·quences (psychotic patients have already been found tohave elevated levels of IL-6; see Smith & Maes, 1995). Weshould also not be too surprised if future research revealsthat perturbations of the immune system also result in psy-chological changes. Although this idea is highly specula-tive at present, it may eventually explain why depression isso closely linked to chronic fatigue syndrome (see TheWorld Around Us 10.7 on p. 367). In short, cytokines mayhave great potential for helping us understand the linksbetween physical and mental well-being that are at theheart of behavioral medicine.
The protective activity of the B- and T-cells is sup-ported and reinforced by other specialized components ofthe system, most notably natural killer cells, macrophages(which we have already mentioned), and granulocytes. Theimmune system's response to antigen invasion is intri-cately orchestrated, requiring the intact functioning ofnumerous components. And, as Developments in Research10.1 illustrates, it is certain that the brain is centrallyinvolved in this control of immune system events.
PSYCHOLOGICAL FACTORS AND IMMUNE FUNCTION-ING AIDS is a disease of the immune system. After expo-sure to the virus that causes AIDS, the person becomes HIV(human immunodeficiency virus) positive. Leserman andher colleagues (2000) followed 82 men who were HIV pos-itive, interviewing them every 6 months for over 7 years.Specifically, the researchers wanted to learn which psy-chological, behavioral, and biological factors were associ-ated with faster progression from HIV to full-blownAIDS. Illustrating the interrelationship between stressand the immune response, greater overall levels of stress-fullife events were associated with more rapid transitionfrom HIV-positive status to AIDS. Higher levels of circu-lating stress hormones (serum cortisol), use of denial as ameans of coping, and greater dissatisfaction with avail-able social support were also predictive of faster develop-ment of AIDS.
As the study described above highlights, the earlycross-sectional investigations that showed a relationshipbetween stress and illness have now been fortified by stud-
ies that support a stronger causal inference concerning therole of stress in reducing immunocompetence (seeKiecolt-Glaser et al., 2002a, 2002b; Schneiderman et al.,2005). For example, after the death of a spouse, there is aperiod of immunosuppression that can last 1 to 3 years(Hafen et al., 1996, p. 25). Immunosuppression can also becaused by short-term threats to our sense of well-being.Strauman, Lemieux, and Coe (1993) designed an experi-ment that (temporarily) manipulated the self-evaluationsof their subjects. They found that natural killer cell cyto-toxicity (i.e., its power to eradicate an antigen) was signifi-cantly diminished with induced negative self-evaluations,an effect that was especially strong for persons who wereanxious and/or dysphoric in mood before the experiment.
Finally, there is evidence from animal studies thatbeing exposed to a single stressful experience can enhanceresponsiveness to stressful events that occur later (John-son, O'Connor, et al., 2002). Rats that were exposed tostressful tail shocks produced more of the stress hormonecortisol when they were later exposed to another stressfulexperience (being placed on a platform). Levels of ACTH(see again Figure 10.2) were also higher in these rats.These results suggest that prior stressful experiences maysensitize the HPA axis to later stressful experiences.
PsychoneuroimmunologyPsychoneuroimmunology is the study of the interactionbetween the nervous system and the immune system(Kiecolt-Glaser et al., 2002a, 2002b; Maier & Watkins,

1998; Maier et al., 1994). It is a developing field that isyielding exciting new findings. Although it was oncethought that the immune system was essentially "closed"and responsive only to challenges from foreign sub-stances (i.e., antigens), we now realize that this is not thecase. The nervous system and the immune system com-municate in ways that we are only just beginning tounderstand. Evidence continues to grow that the braininfluences the immune system and that the immune sys-tem influences the brain. Maier and colleagues (Maier &Watkins, 1998; Maier et al., 1994) present strong evidencethat a person's behavior and psychological states doindeed affect immune functioning, but the status ofimmunologic defenses also feeds back to influence cur-rent mental states and behavioral dispositions by affect-ing the blood levels of circulating neurochemicals, whichin turn modify brain states.
STRESS, DEPRESSION, AND SUPPRESSION OF THEIMMUNE SYSTEM Research over the past 30 years hasdemonstrated a link between chronic stress and suppres-sion of the immune system (Segerstrom & Miller, 2004),with the most enduring stressors (e.g., unemployment)being associated with the most global immunosuppres-sion. Reviews (see Kiecolt-Glaser et al., 2002a; Weisse,1992) also indicate a strong association between dysphoricmood and compromised immune function, which is, atleast partially, independent of specific situations or eventsthat may have provoked depressed feelings. (In otherwords, the state of being depressed adds something beyondany negative effects of the stressors precipitating thisdepressed mood.) Another review of the relevant researchfound that depressed affect was reliably associated withlowered numbers of white cells following challenge by aforeign protein, with lowered natural killer cell activity,and with lowered quantities of several varieties of circulat-ing white cells (Herbert & Cohen, 1993).
The list of conditions that have been demonstrated tobe associated with diminished immune function is a longone. Besides psychological depression, it includes sleepdeprivation, marathon running, spaceflight, being thecaregiver for a patient with dementia, and death of aspouse (Cacioppo, et al., 1998; Schleifer, Keller, & Stein,1985; Schleifer et al., 1989; Vasiljeva et al., 1989). Immuneresponsiveness has also been shown to vary with even nor-mal, diurnal variations in mood (Stone et al., 1987). Rele-vant to many readers of this book, a group of researchershas repeatedly demonstrated the compromise of whiteblood cell proliferation, including diminished naturalkiller cell activity, among students undergoing the stressof academic examinations (Glaser et al., 1985, 1987). Nat-ural killer cells are believed to playa key role in tumor sur-veillance and in the control of viral infections. Stress haseven been shown to slow the healing of wounds by asmuch as 24 to 40 percent (Kiecolt-Glaser et al., 1998). Foranyone about to have surgery, this is clearly a very impor-tant finding.
STRESS, DEPRESSION, AND INCREASED IMMUNERESPONSIVENESS There is a great deal of evidencelinking stress to suppression of the immune system.However, a shift in thinking is now taking place.Researchers are beginning to pay attention to the possi-bility that chronic stress and depression may actuallyenhance certain immune system responses, although notin a good way (Robles et al., 2005). Chronic stress anddepression may trigger the production of pro-inflamma-tory cytokines such as interleukin-6 (IL-6). One studyshowed that women who were caring for a family memberwith Alzheimer's disease had higher levels of IL-6 thanwomen who were either anticipating the stress of reloca-tion or who were experiencing neither of these stressors(Lutgendorf et al., 1999). This difference was found eventhough the women who were caregivers were 6 to 9 yearsyounger than the women in the other two groups andeven though IL-6 levels are known to increase with age.Major depression has also been linked to enhanced pro-duction of pro-inflammatory cytokines, including IL-6,and treatment with antidepressant medications canreduce this elevation (Kenis & Maes, 2002).
These findings are especially interesting in light ofresearch showing a relationship between IL-6 and aging,as well as to chronic diseases including certain cancersand cardiovascular disease (Papanicolaou et al., 1998).Also, higher levels of IL-6 are associated with being over-weight, smoking, and having a sedentary lifestyle (Fer-rucci et al., 1999).
One group of investigators has reported that olderadults (average age 71 years) who regularly attended churchhad lower levels of IL-6 and were less likely to die during thecourse of a 12-year follow-up than those who did not (Lut-gendorf et al., 2004). These findings also held when otherpotential confounding variables such as age, social support,being overweight, having medical problems, or beingdepressed were also considered. Given all of these findings,it is not hard to see why researchers are becoming excitedabout the possibility that pro-inflammatory cytokines likeIL-6 could be key mediators in the link between psychoso-cial factors and disease. Overall, what the research findingssuggest is that chronic stress and depression can result inthe immune system going out of balance in ways that maycompromise health (see Robles et al., 2005). In short, thepotential for psychological factors to influence our healthand for our health to affect our psychological well-being isbecoming ever more apparent.
Lifestyle Factors in Health and IllnessA great deal of attention is being paid today to the role oflifestyle in the development and/or maintenance of manyhealth problems. Do you smoke? How often do you exer-cise? Numerous aspects of the way we live have beenimplicated in the development of some severe medicalproblems. Death from heart disease is linked to lack ofphysical exercise (Dubbert, 2002). Tobacco use contributes

to 450,000 deaths each year (Niaura & Abrams, 2002).Some 61 percent of adult Americans are either overweightor obese (Wadden et al., 2002). Particularly relevant forcollege students, even partial sleep loss for as little as onenight is associated with elevated levels of cortisol the fol-lowing evening (Leproult et al., 1997).
Lifestyle factors-habits or behavior patterns pre-sumably under our own control-play a major role inthree of the leading causes of death in this country: coro-nary heart disease, automobile accidents, and alcohol-related deaths. Even when they know they are doing thingsthat can cause Irreparable physkal harm, It is difficult formany people to change their lifestyles to reduce their risk
of disease. Even after having two heartattacks and surgery to remove a cancer-ous lung, one man continued to smoke21/2 packs of cigarettes a day. He fre-quently said, "I know these things arekilling me a little at a time ... , but theyhave become so much a part of my lifeI can't live without them!" Most of usknow someone who behaves in a simi-lar way.
Health, Attitudes, andCoping ResourcesBecause the brain influences theimmune system, a variety of psycholog-ical factors may be of great importanceto our health and well-being. You havealready learned how important depres-sion is with regard to the immune sys-tem. How you view problems, copewith challenges, and even your tem-perament may directly affect yourunderlying physical health.
OPTIMISM Hopeless and helplessattitudes can have devastating effectson organic functioning. For example, asense of hopelessness accelerates pro-gression of atherosclerosis, the under-lying process leading to heart attacksand strokes (Everson et al., 1997). Opti-mists, who expect that good things willhappen, may fare much better (Carver& Scheier, 2002). Today, many surgeonswill delay a major operation until theyare convinced that the patient is reason-ably optimistic about the outcome.Optimism in a more global, everydaysense seems to serve as a buffer againstdisease (Scheier & Carver, 1987, 1992).Although it is possible that being toooptimistic about their health could
cause people not to seek help for potentially dangeroushealth problems (e.g., Davidson & Prkachin, 1997; Fisher& Fisher, 1992; Friedman et al., 1994; Kalichman et al.,1993; Tennen & Affleck, 1987), most of the data suggestthat the benefits of being optimistic outweigh the possibledisadvantages (Carver & Scheier, 2002).
People with too little optimism experience a psycho-logical sense of helplessness. As we saw in Chapter 5, thiscan be associated with poor health outcomes. In an inter-esting study of Hall of Fame baseball players, Peterson andSeligman (1987) found that in this group of athletes, neg-ative attltudes were significantly associated with healthproblems following their active playing years. Peterson

Is Holding a Grudge Badfor Your Health?o.
511"of us feel mistreated from time to time.Perhaps a friend who offered to pick us upat the airport didn't show because some-thing else came up. Perhaps someonespreads mean gossip about us behind our
back. Perhaps a work supervisor or college professor failsto recognize the effort we have put into a piece of work andgives us an unfairly low evaluation. For all of us, suchslights are an unfortunate-but inevitable-fact of life.
Does how we handle such situations have any bearingon our health? To examine this issue, Witvliet et al. (2001)
studied the emotional and physiological consequences ofbeing forgiving or unforgiving. College students wereasked to select a real-life interpersonal offense that theyhad experienced in the past. Most of these offenses hadbeen committed by friends, romantic partners, siblings, orparents, and they included such things as rejection, betray-als of trust, and personal insults. The researchers thencollected self-reports as well as psychophysiological data(heart rate, blood pressure, and facial muscle tension)from the students while they were imagining responding tothe real-life transgression in a way that was either forgivingor unforgiving. In the forgiving condition, the studentswere asked to think about granting forgiveness or develop-ing feelings of empathy for the perpetrator. In the unforgiv-ing condition, they were asked to stay in the victim role, togo over the hurt in their minds, and to nurse a grudge.
Did thinking about the same event in these differentways change the moods and physiological states of theparticipants? The answer is yes. When they were asked tobe forgiving, the participants reported more feelings ofempathy and forgiveness. When asked to ruminate and beunforgiving, however, participants reported that they feltmore negative, angry, sad, aroused, and out of control.They also showed greater tension in their brows. Impor-tantly, their heart rates went up, their blood pressuresincreased, and their skin conductance (a measure of SNSarousal) revealed more arousal. Even more striking was thefinding that even after the grudge-harboring imagery wasover and the subjects were told to relax, they were unableto do so. In other words, the high state of physiologicalarousal that had been triggered by dwelling on the pasthurt could not easily be turned off.
What are the implications of these findings? Althoughfleeting feelings of anger probably do us no real harm, peo-ple who have a tendency to brood about the wrongs thatother people have done to them may be doing themselvesa major disservice. To the extent that perpetuating feelingsof anger and increasing cardiovascular reactivity have con-sequences for heart disease and immune system function-ing, harboring grudges may be hazardous to our health.Although it is not always easy, forgiving those who haveoffended us may lower our stress levels and enhance ourwell-being.
and colleagues (1998) also reported a significantly ele-vated mortality rate among a group of intellectually giftedindividuals who had, a half-century earlier, a tendency totreat negative events as catastrophes. There are clearlyadvantages to seeing the glass as half full rather than ashalf empty.
NEGATIVE AFFECT Perhaps negative emotions shouldcarry with them a health warning similar to that found onpackets of cigarettes. Certainly, evidence is accumulatingthat negative emotions can be associated with poor health(Kielcolt-Glaser et al., 2002a). Depression, as we havealready emphasized, is associated with measurable andundesirable changes in immune functioning (Robles et al.,2005; Zorillo et al., 2001). And, as we will see later, peoplewith major depression run a greater risk of having a heartattack than people with no history of depression (Prattet al., 1996). Depression also seems to be associated withincreased mortality from all causes in medical inpatients(Herrmann-Lingen et al., 2001). In women, depressionappears to heighten the risk for osteoporosis (Michelson
et al., 1996), and in men, one prospective study showedthat depression at baseline predicted decline in musclestrength over a 3-year period (Rantanen et al., 2000).
Although this effect has not been as well studied,anxiety also seems to be associated, in both men andwomen, with the development of coronary heart disease.Finally, it is well documented that chronic anger and hos-tility can be risk factors for coronary heart disease anddeath (Miller et al., 1996). The most familiar example hereis the Type A behavior pattern, which we will discuss inmore detail later. Taken together, the research findingsindicate that an optimistic outlook on life, as well as anabsence of negative emotions, may have some beneficialhealth consequences. Indeed, there is currently a growinginterest in studying positive psychology (Snyder & Lopez,2002). This school of psychology focuses on human traitsand resources that might have direct implications for ourphysical and mental well-being. Positive affectivity (thetendency to experience positive emotional states; Watson,2002), compassion (Cassell, 2002), gratitude (Emmons &Shelton, 2002), humor (Lefcourt, 2002), and spirituality

(Pargament & Mahoney, 2002) are valuable human gifts.Although research into these and other aspects of "accen-tuating the positive" is still in its infancy, there are alreadyhints of their potential health benefits. For example, thereis evidence that laughter is associated with enhancedimmune functioning (Berk et al., 1988; Lefcourt, 2002).There are also physiological benefits associated with for-giving people who have wronged us (see Developments inResearch 10.2).
Ironically, some of the positive characteristics ofhumans may also complicate efforts to determine the trueeffectiveness of new treatment techniques, such as newdrugs. A patient who believes a treatment is going to beeffective has a much better chance of showing improve-ment than one who is neutral or pessimistic-even whenthe treatment is subsequently shown to have no direct orrelevant physiological effects. This placebo effect accountsin part for the controversies that arise periodicallybetween the scientific community and the general publicabout the efficacy of certain drugs or other treatments. Asyou may recall from Chapter I, the placebo effect appearsto explain why people experience clinical benefit frommagnet therapy.
It has even been suggested that without the placeboeffect, the medical profession as we know it would nothave survived to the twentieth century. Until the early1900s, medical practitioners had little else to offer diseasesufferers; indeed, many widely employed specific treat-ments (such as bleeding) were plainly harmful (bleedingkilled George Washington, for example). The profession'ssurvival and prosperity from ancient times is to a largeextent a demonstration of the power of faith in healing(Shapiro & Morris, 1978). Thus the fundamental inti-macy of the mind and body is perhaps nowhere betterdocumented than in the history of the medical profes-sion itself.
In ReVlew~ How does a person's attitude and outlook on
life affect health maintenance anddeterioration?
~ How can optimism or negative attitudeseither enhance or compromise a person'sability to cope with illness?
~ What physiological mechanisms are involvedin autonomic nervous system arousal?
~ Describe the relationship between stress andthe immune system.
CARDIOVASCULARDISEASEBecause cardiovascular disease is the leading cause ofdeath in the United States (American Heart Association,2001), we will use this disease to illustrate the many linksbetween psychological factors and physical disease. Someof these are highlighted in the following case.
Dr. M was a 44-year-old physician. The middle son of par-ents who had emigrated from Italy, he was ambitious anddetermined to make a successful life for himself and hisfamily. He worked long hours helping patients with can-cer, and he was caring and compassionate_ His patientsloved him. But his job was also very stressful. Added tothe many demands of maintaining a busy medical prac·tice was the great sadness that he felt when (inevitably)many of his terminally ill patients died.
At home Dr. M was a loyal husband and devotedfather to his three children. But he was not an easy per-son to live with. He found it hard to relax, and he had avery volatile disposition. He was frequently angry andwould shout at everyone whenever he had a bad day.Often his moods were caused by his feeling that he wasnot fully appreciated by the other doctors with whom heworked. Although his wife realized that he "just neededto vent," his moods took a toll on the family. His childrendistanced themselves from him much of the time, and hiswife became less and less happy in the marriage.
One day at work, Dr. M started to feel unwell. Hebegan to sweat and experienced a heavy pressure in hischest. It was difficult for him to breathe. Dr. M recognizedthe severity of his problem and called out for medicalhelp. He had a sudden and severe heart attack and sur·vived only because he was working in a hospital at thetime of the attack. If he had not received prompt medicalattention, he almost certainly would have died.
After his heart attack Dr. M became very depressed.It was almost as though he could not accept that he, aphysician, had a severe medical problem. Although helived in fear of having another heart attack, his efforts tolose weight (which his doctor had told him to do) weresabotaged by his unwillingness to follow any diet. Hewould try and then give up, coming back from the Italianbakery with bags of pastries. Making the problem worsewas the fact that because he was a doctor, his own doc-tors were somewhat reticent about telling him what hehad to do to manage his illness. Hewent back to work and

his family walked on eggshells, afraid to do or say any-thing that might stress him. His wife tried to encouragehim to follow the doctors' recommendations. However,Dr.M's attitude was that ifhe was going to die anyway, hemight as well enjoy himself until he did.
Diseases of the cardiovascular system (the heart andits connected tree of vessels) involve many interrelatedclinical conditions. Here we focus on three:
hypertension (high blood pressure);
coronary heart disease (CHD), where arteriessupplying blood to the heart muscle itself becomeclogged (see Figure 10.4); and
stroke, where the same types of clogging affect thearterial blood supply to the brain.
Plaque(fatty deposits)
Buildup ofplaque
Partiallyblockedartery
In this chapter we deal with hypertension and CHD.Stroke, which is in many ways similar to CHD in etiology,is covered in Chapter 15.
HypertensionWhen a physiologically normal person is calm, his or herheartbeat is regular, the pulse is even, the blood pressure isrelatively low, and the visceral organs are well suppliedwith blood. With stress, however, the vessels of the visceralorgans constrict (become more narrow), and blood flowsin greater quantity outward to the muscles of the trunkand limbs. This is a part of the fight-or-flight pattern youlearned about earlier. When the tiny blood vessels supply-ing the visceral organs become constricted, the heart mustwork harder. As it beats faster and with greater force, thepulse quickens and blood pressure mounts. Usually, whenthe crisis passes, the body resumes normal functioning andthe blood pressure returns to normal. Under continuingemotional strain, however, high blood pressure maybecome chronic.
Ideally, blood pressure should be 120/80. (By conven-tion, the first number given is the systolic pressure when theheart contracts; the second is the diastolic or between-beatpressure. The unit of measurement is millimeters of mer-cury, Hg.) The definition of hypertension is having a per-sisting systolic blood pressure of 140 or more and a diastolicblood pressure of 90 or higher. Blood pressure below140/90 was once regarded as normal. However, pressures inthe range of 130-139/85-89 are now classified as "high nor-mal" (Joint National Committee, 1997). In general, bloodpressure increases as we age. In younger adults, more menthan women suffer from high blood pressure. After aboutage 50, however, the prevalence of hypertension is greater inwomen (Burt et aI., 1995), probably because menopauseamplifies the stiffness in the arteries that naturally occurswith increasing age (Takahashi et aI., 2005). Current esti-mates suggest that sustained hypertension afflicts almost 50million Americans (see Blumenthal et aI., 2002).
Many clinicians and investigators think that hyperten-sion begins when a person has a biological tendency towardhigh cardiovascular reactivity to stress (e.g., Tuomisto,1997; Turner, 1994), and then, given difficult life circum-stances, that person progresses through borderline to frankhypertension in the adult years.
Organic malfunctions that induce hypertensionaccount for only a small percentage of hypertension cases;the large remainder of cases are called essential hyperten-sion, meaning that there is no specific physical cause.Essential hypertension is often symptomless until its effectsshow up as medical complications. In addition to makingcoronary heart disease and stroke more likely, it is often acausal factor in occlusive (blocking) disease of the periph-eral arteries, congestive heart failure (due to the heart'sinability to overcome the resistance of constricted arteries),

kidney failure, blindness, and a number of other seriousphysical ailments. High blood pressure is thus an insidiousand dangerous disorder. Ironically, it is both simple andpainless to detect by means of the familiar inflated arm cuff.
HYPERTENSION AND AFRICAN-AMERICANS African-Americans in the United States have very high rates ofhypertension. They also tend to have a much more severehypertension than do whites (Clark, 2005; Grundy et al.,2001; Hall et al., 1997). Higher levels of stress from suchfactors as inner-city living, economic disadvantage, expo-sure to violence, and race-based discrimination may playakey role in this (Din-Dzietham et al., 2004; Wilson et al.,2004). Lifestyle may also be a factor. African-Americanwomen in particular are more likely to be overweight thanCaucasian women (see Whitfield et al., 2002), and African-Americans as a group are less likely to exercise than Cau-casians (Bassett et al., 2002; Whitfield et al., 2002).
African-Americans may also be at greater risk of hyper-tension for biological reasons. Heavy salt use is common inthe dietary preferences of blacks, and there is evidence thatthe black population as a group excessively retains ingestedsodium, which results in fluid retention and endocrinechanges that in turn elevate blood pressure (Anderson &McNeilly, 1993). Renin, an enzyme produced by the kidneysthat is linked to blood pressure, is also processed differentlyby African-Americans. Finally, studies suggest that nitricoxide (a dissolved gas that is crucial for the proper func-tioning of blood vessels and blood cells) is produced inlower levels in the blood vessels of African-Americans andmay also be destroyed more quickly too. All of these biolog-ical differences as well as the presence of some specific genes(see Kumar et al., 2005) may increase the risk that African-Americans have of developing hypertension.
HYPERTENSION AND ANGER Although for a long timeresearchers hypothesized that people with hypertensionsuffered from repressed rage, more current research pointsnot to whether anger is suppressed or expressed, but,rather, to whether anger is communicated constructively.
Davidson and his colleagues (2000) explored this bymeasuring whether people scored high or low on a scaleof constructive anger. Constructive anger was rated byobservers. The observers watched an interview duringwhich the person being assessed discussed how he or shetypically responded in a variety of stressful situations. Peo-ple who scored high in constructive anger generally triedto resolve their anger by dealing with the target of theiranger more directly, expressing why they felt angry, andtrying to reach an understanding by engaging in opencommunication with that person. They also solicited theopinions of other people to obtain an objective view of thesituation and to find other ways to resolve it. Davidsonet al. (2000) found that people who expressed their angermost constructively had the lowest resting blood pressure(i.e., there was a negative correlation). Significantly, use of
constructive anger was also associated with lower self-reported anxiety and depression, as well as lower measuresof destructive hostility-factors that are also implicated incoronary heart disease.
Coronary Heart DiseaseCoronary heart disease is a potentially lethal blockage ofthe arteries that supply blood to the heart muscle, ormyocardium. Its chief clinical manifestations are(1) myocardial infarction (a blockage of a section of thecoronary arterial system) resulting in death of the myocar-dial tissue supplied by that arterial branch; (2) angina pec-toris, severe chest pain signaling that the delivery ofoxygenated blood to the affected area of the heart is insuf-ficient for its current workload; and (3) disturbance of theheart's electrical conduction consequent to arterial block-age, resulting in disruption or interruption of the heart'spumping action, often leading to death. Many instances ofsudden cardiac death, in which victims have no prior his-tory of CHD symptoms, are attributed to silent CHD. Thisoften occurs when a piece of the atherosclerotic materialadhering to the arterial walls (a "plaque") breaks loose andlodges in a smaller vessel, blocking it. Some of the warningsigns of a heart attack are described in The World AroundUs 10.3.
What Psychological Factors AreImplicated in Cardiovascular Disease?PERSONALITY Attempts to explore the psychologicalcontribution to the development of CHD began with theidentification of the Type A behavior pattern (Friedman& Rosenman, 1959). This is characterized by
excessive competitive drive,
extreme commitment to work,
impatience or time urgency, and
hostility.
Type A people play to win-even when they are play-ing with children! Many of us know people who are likethis, and the term Type A is now quite commonly used ineveryday language.
Interest in Type A behavior escalated after the resultsof the Western Collaborative Group Study were published.This investigation involved some 3,150 healthy menbetween the ages of 35 and 59 who, on entry, were typed asto A or B status. (Type B personalities do not have Type Atraits and tend to be more relaxed, more laid-back, and lesstime-pressured people.) All the men were then carefullyfollowed for 81/2 years. Compared to Type B personality,Type A personality was associated with a twofold increasein coronary artery disease and an eightfold increased riskof recurrent myocardial infarction over the course of thefollow-up (Rosenman et al., 1975).

10.3
V arryl Kile was a Major League baseballall-star pitcher who died suddenly of aheart attack in his hotel room at the ageof 33. His death emphasizes the impor-tance of health knowledge and interven-
tion in the prevention of cardiovascular disease, especiallyin young people.
Many young people mistakenly assume that cardio-vascular disease is not something they should be con-cerned about. Research suggests otherwise. Iribarren andcolleagues (2000) examined 374 Caucasian and African-American men and women between the ages of 18 and 30,looking for signs of calcification in the subjects' coronaryarteries (a warning sign of the hardening of arteries, or ath-erosclerosis). Even when controlling for demographics,lifestyle, and physiological variables, the researchersfound that those subjects who had scored higher on an ini-tial measure of hostility that had been completed 10 yearsearlier were more than twice as likely to have coronary cal-cification as those subjects who had scored low in hostility.These findings not only challenge the common belief thatcardiovascular disease is of little concern to young peoplebut also accentuate the importance of starting as early aspossible to engage in preventive measures (e.g., minimiz-ing hostile attitudes, getting treated for depression, avoid-ing weight gain, and not smoking).
The second major study of Type A behavior and CHDwas the Framingham Heart Study. This began in 1948 andhas involved the long-term follow-up of a large sample ofmen and women from Framingham, Massachusetts (seeKannel et aI., 1987). Approximately 1,700 CHD-free sub-jects were typed as A or B in the mid-1960s. Analysis of thedata for CHD occurrence during an 8-year follow-upperiod not only confirmed the major findings of the earlierWestern Collaborative Group Study but extended them towomen as well.
Not all studies reported positive associations betweenType A behavior and risk of coronary artery disease, how-ever (Case et aI., 1985; Shekelle et aI., 1985). Moreover, asresearch with the construct has continued, it has becomeclear that it is the hostility component of the Type A con-struct (including anger, contempt, scorn, cynicism, andmistrust) that is most closely correlated with coronaryartery deterioration (see Rozanski et aI., 1999, for a sum-mary of studies).
A recent development is the identification of the "dis-tressed" or Type D personality type (Denollet et aI., 2000).As shown in Figure 10.5 on page 358, people with Type D
Cardiovascular Disease in a" ..Year..Old Athlete
Prevention of cardiovascular disease begins withhealth education, which includes knowing your medicalhistory. Kile's father, for example, had died from a strokeafter suffering a heart attack at the age of 44. It is alsoimportant to be able to recognize the symptoms of a heartattack. Kile had mentioned to his brother, the night beforehis death, that he was tired and was experiencing sorenessin his shoulder (Gorman, 2002). But because of his age,and because he was a pitcher, he may not have attributedthese symptoms to an impending heart problem. The fol-lowing warnings of heart attack are often (but not always)present: (1) a pain that spreads along the shoulders, arm,neck, or jaw; (2) sudden sweating; (3) a heavy pressureand pain in the center of the chest; and (4) nausea, vomit-ing, and shortness of breath. The symptoms may come andgo. Denial of symptoms and stubbornness are commonreasons why people who are having myocardial infarctionsdelay getting medical help (O'Carroll et aI., 2001). Aware-ness of these findings is extremely important for youngadults, who often think they are impervious to physicalproblems. In 1998 more than 3,000 people in Americabetween the ages of 15 and 34 died suddenly of heart dis-ease (Gorman, 2002). Although we may all want to assumethat it could never happen to us, it is wise for all of us toknow our family histories and be able to recognize theearly signs of potential problems.
personality have a tendency to experience negative emo-tions and also to feel insecure and anxious. Althoughresearch exploring Type D personality is just beginning,men with CHD who scored high on measures of chronicemotional distress were more likely have fatal and nonfatalheart attacks over the 5-year follow-up period than weremen who did not have these Type D personality traits(Denollet et aI., 2000). The Type D personality constructalso provides a way to tie in some of the other findings link-ing negative emotions and CHD, which we discuss below.
DEPRESSION Depression is commonly found in peoplewho already have heart disease. People with heart diseaseare approximately three times more likely than healthypeople to be depressed (Chesney, 1996; Shapiro, 1996).Furthermore, if heart attack patients are depressed at thetime of their heart attack or shortly afterward, they show agreatly increased risk for future coronary events and car-diac death (Chesney, 1996; Shapiro, 1996). In one study of222 patients who had experienced a heart attack, thosewho were clinically depressed were five times more likelythan their nondepressed counterparts to die in the next

The social and emotional problems associated with Type Dpersonality can increase your chances of developing heart disease.Read each statement and circle the appropriate number to indicateyour answer. There are no right or wrong answers: your ownimpression is the only thing that matters.
Q)Q)III
:§ ~ EQ)
III "5 III Q)III
C;; III Q) III :::lQ) Q) t=:l.L- -J Z -J
4 3 2 1 0
0 1 2 3 4
4 3 2 1 0
0 1 2 3 4
4 3 2 1 0
0 1 2 3 4
4 3 2 1 0
0 1 2 3 4
4 3 2 1 0
0 1 2 3 4
4 3 2 1 0
0 1 2 3 4
4 3 2 1 0
TAKE THE TESTCircle your answers:
1. I make contact easily when I meet people
2. I often make a fuss about unimportant things
3. I often talk to strangers
4. I often feel unhappy
5. I am often irritated
6. I often feel inhibited in social interactions
7. I take a gloomy view of things
8. I find it hard to start a conversation
9. I am often in a bad mood
10. I am a closed kind of person
11. I would rather keep people at a distance
12. I often find myself worrying about something
13. I am often down in the dumps
14. When socializing. I don't find the right thingsto talk about 0 1 2 3 4
ADD YOUR ANSWERSNegative Affectivity:Add scores for questions 2. 4. 5, 7, 9 12 and 13
Social Inhibition: IAdd scores for questions 1, 3. 6, 8, 10. 11,and 14 _
SCORE THE RESULTSYou qualify as a Type D personality if your Negative Affectivityis 10 or higher and your Social Inhibition is 10 or higher.
FIGURE 10.5Characteristics of the Type 0 Personality
Source: Adapted from "0514: Standard Assessment of Negative Affectiv-ity, Social Inhibition, and Type 0 Personality" by johan Oenof/et. PhO.Psychosomatic Medicine, 2005. january-February;67(1);89-97. Used withpermission by Lippincott;Wi//iams & Wilkins.
6 months (Frasure-Smith et aI., 1993). Moreover, depres-sion was as good a predictor of death from heart disease aswere medical variables such as prior heart attacks and poorheart functioning. After adjustment for these other vari-ables, it was estimated that the relative risk of death associ-ated with depression was still four times greater. Risk ofdeath is also increased even if the symptoms of depressionare not especially severe (Bush et aI., 2001).
Depression also appears to be a risk factor for the devel-opment of CHD. Pratt and her colleagues (1996) followedover 1,500 men and women with no prior history of heart dis-ease for 14 years. They found that 8 percent of those whohad suffered major depression at one time and 6 percent of
those who had suffered mild depression at some pointhad a heart attack during the 14-year follow-up inter-val. By contrast, only 3 percent of those without a his-tory of depression suffered heart attacks. When medicalhistory and other variables were taken into account,those who had suffered major depression were found tobe four times more likely to have had a heart attack.Similar findings have also been reported in other stud-ies (Ferketich et al.. 2000; Ford et al.• 1998).
Evidence further points to the importance ofhopelessness (an important element of depression) inincreasing risk for CHD. For example, Anda and col-leagues (1993) found that people who answered yes tothe question, "In the past month, have you felt so sad,discouraged, hopeless, or had so many problems thatyou wondered if anything was worthwhile?" had twicethe risk for CHD than did people who answered no tothis question. Experiencing what is referred to as vitalexhaustion (fatigue, irritability, and demoralization)also predicts future CHD and cardiac events, even inpeople who are currently quite healthy (Appels &Mulder, 1988).
Why should depression and CHD be linked? Twomechanisms have been proposed to explain the asso-ciation. The first possibility is that depressed peoplemay engage in more behaviors known to put them atrisk for CHD. For example, depressed people are lesslikely to eat well or exercise, are more likely to smoke,and may not take their medications appropriately(e.g., Carney, Freedland, et aI., 1995). Depressed peo-ple are also known to lack social support, another fac-tor linked to CHD (Eriksen, 1994).
Second, it is likely that depression is linked toCHD through various biochemical mechanisms(Krantz & McCeney, 2002; Lesperance et aI., 2004;Markovitz et al., 2000; Miller et aI., 2002; Musselmanet aI, 2000).As we noted in Chapter 7, many depressedpeople have elevated levels of the stress hormone cor-
tisol as well as elevated levels of interIeukin-6 (Robles et aI.,2005). They also have elevated levels of norepinephrine intheir blood, which can increase blood pressure. Thus,although depressed people may appear lethargic, their ele-vated stress hormones may damage their hearts. Further-more, depressed individuals show less variability in heartrate in response to behavioral changes (for example, theheart rate when walking should be different from the heartrate when sitting down). High heart rate levels and lowheart rate variability are also known to be associated withchanges in sympathetic-parasympathetic balance, whichmay increase the cardiac arrhythmias that often precedesudden death (Carney, Saunders, et aI., 1995; Frasure-Smith et aI., 1993).
ANXIETY Given the strong links between anxiety andmood disorders discussed in Chapter 6, it is not surprising

Depression increases the risk at developing heart disease and atdying tram a heart attack.
that a similar link may exist between anxiety and CHD.Research has demonstrated a relationship between phobicanxiety and increased risk for sudden cardiac death.Kawachi, Colditz, and colleagues (1994) followed for 2years nearly 34,000 male professionals who had beenassessed for panic disorder, agoraphobia, and generalizedanxiety. Men with the highest levels of phobic anxiety werethree times more likely to have a fatal heart attack thanmen with the lowest levels of phobic anxiety. Sudden car-diac death was six times higher in the men with the highestlevels of anxiety. However, no association was foundbetween anxiety and nonfatal attacks. The findings werereplicated in a second study of nearly 2,300 men who wereparticipating in a normative aging study (Kawachi, Spar-row, et aI., 1994, 1995).
SOCIAL ISOLATION AND LACK OF SOCIAL SUPPORTStudies point to the strong link between social factors andthe development of CHD. For example, monkeys housedalone have four times more atherosclerosis (fatty depositsin blood vessels that eventually create a blockage) thanmonkeys housed in social groups (Shively et aI., 1989).Similarly, people who have a relatively small social networkor who consider themselves to have little emotional sup-port are more likely to develop CHD over time (see Rozan-ski et aI., 1999, for a review).
For people who already have CHD, there is a similarassociation. In one study among people who had alreadysuffered a heart attack, those who reported that they hadlow levels of emotional support were almost three timesmore likely to experience another cardiac event (Berkmanet aI., 1992). And in another study, death in CHD patients
was three times more likely over the next 5 years if theywere unmarried or had no one that they could confide in(Williams et aI., 1992). Echoing these findings, Coyne andhis colleagues (2001) have shown that the quality of themarital relationship predicts 4-year survival rates inpatients with congestive heart failure.
CHRONIC AND ACUTE STRESS Stress can come in avariety of forms. In some respects, all of the factors we havejust described can be considered forms of stress. Certainly,having little or no social support can be stressful. Anger,depression, and anxiety can also be viewed as forms ofinternal stress.
What is perceived as stressful is often highly subjec-tive. One person may sit in terror on a roller-coaster ridewhile the person in the next seat is exhilarated by the expe-rience. Going to a party may be stressful for the shy personbut not for the extrovert. What we experience as stressful isvery much linked to who we are. This makes the measure-ment of stressful experiences very problematic.
Although some forms of stress may have a large sub-jective element, there are other forms of stress that we uni-versally recognize as severe, objective, and external. Anobvious example is earthquakes. Several researchers havenow reported that deaths from CHD rise in the days andweeks following a severe earthquake (see Pickering, 2001).After the Northridge earthquake in Los Angeles in 1995,the number of sudden deaths due to CHD rose from anaverage of 4.6 (in the days preceding the earthquake) to 24on the day of the earthquake (Kloner et aI., 1997). Therewas also an increase in sudden death from cardiac eventsafter the Hanshin-Awaji earthquake in Japan (Kario &Ohashi, 1997).
Everyday forms of stress can also elevate risk for CHDand death (Matthews & Gump, 2002; Smith & Ruiz, 2002).A good example is work-related stress (see The WorldAround Us lOA). Here the key factors appear to be havinga highly demanding job and having little control over deci-sion making. Both of these types of job stress increase riskfor future CHD. Moreover, this association still holds whenother negative health behaviors (such as smoking) are con-trolled (see Peter & Siegrist, 2000).
Finally, simply being asked to give a 5-minute speechabout an assigned topic to a small (but evaluative) audi-ence was enough to produce detectable changes in cardiacfunction in about 20 percent of patients with existingcoronary artery disease (see Sheps et aI., 2002). Moreover,the patients who were most reactive to this form of mentalstress were almost three times as likely as the less reactivepatients to die in the next 5 to 6 years. Mental stress isknown to raise systolic blood pressure and also to cause anelevation in epinephrine. Mental stress may also reduce theoxygen supply to the heart muscle (Yeung et aI., 1991).What the results of the Sheps study illustrate, however, isthat stress does not have to be extreme or severe to be asso-ciated with lethal consequences "down the road."

10.4511 mericans are working more and taking
fewer vacations. The pace of life is fastand work is no exception. Deadlines loom,bosses threaten, and expectations arehigh. For many people, work is a major
source of stress in their daily lives.Does stress in the workplace affect our health?
Research indicates that people who report facing a suddenshort-term increase in work pressure or a great deal ofcompetition at work have a sixfold greater risk of having aheart attack during the next 24 hours (Moller et aI., 2005).
Work stress also seems to increase our risk for devel-oping depression. Wang (2005) recently reported theresults of a study of 6,633 workers in Canada. Theemployed participants were interviewed about their lives,their health, their jobs, and about how much work stressthey experienced (see Figure accompanying this feature).Two years later, they were interviewed again. The resultsshowed that workers who reported the highest levels ofwork stress (Le., highest quartile) were 2.3 times morelikely to have developed an episode of major depression inthe time between the two interviews. This is an interestingfinding, especially because people with a past history ofdepression were excluded from the analysis. Moreover, theassociation between work stress and the development ofdepression was not explained by other variables such aseducation level, chronic medical problems, trauma, orother negative life events that the workers experienced.Overall, the results of this study indicate that work stressmay be a risk factor for the development of depression.The findings also highlight the potential importance ofmodifying work conditions to help employees stay healthyand productive (e.g., Theorell et aI., 2001).
In ReVIew~ What is essential hypertension, and what are
some of the factors that contribute to itsdevelopment?
~ What are the clinical manifestations of, andpotential risk factors for, coronary heartdisease eCHD)?
~ What is a Type A personality? What is themost important element of the Type Apattern? What evidence links this behaviorpattern to coronary heart disease?
• Not being required to learn new things• Not having a job that requires a high level
of skill• Having to do the same things over and over• Not having freedom to decide how to do
your job• Not having a say in what happens in your job• Having a hectic job• Having others make conflicting demands
on you• Having little job security• Having a job that requires a lot of physical
effort• Being exposed to conflict and hostility at work• Having an unhelpful supervisor• Not having helpful co-workers
(From Wang, 2005.)
GENERAL CAUSALFACTORS IN PHYSICALILLNESS AND DISEASE _~_.What factors determine who gets one disorder and whogets another? Why does Michael suffer from migraines andwhy does Sam develop hypertension? Genetic differencesmay be part of the answer.
Our understanding of genetic contributions to disease,including diseases with a psychological component, is stillquite limited. Genetic contributions may include:

an underlying physical vulnerability to the disease inquestion, such as excessive cardiovascular reactivityin hypertension;
the psychological makeup of the individual and hisor her stress tolerance, such as an aggressive or inhib-ited temperament; and
the nature of any interaction between factors (1)and (2).
If biological and psychological contributions toenhanced risk are both partly inherited, then disentanglingtheir separate influences is bound to be difficult-all themore so if the expression of one influence is somehow mod-ified by the presence of the other (that is, if they "interact").
Despite these difficulties of interpretation, nearly alldiseases of genetic/psychological origin can be shown torun in families to at least some extent. We must keep inmind that social learning (for example, children modelingthe inadequate coping skills of their parents) could be afactor in such family resemblances. As in other areas ofpsychopathology, whenever we assess the psychologicalaspects of physical illness, we struggle with the problem ofdifferentiating the effects of shared genes from those ofshared environments.
We will undoubtedly discover more as the HumanGenome Project progresses and identifies all of the genesin the human organism (see Plomin & McGuffin, 2003).Genes that are associated with increased risk of hyperten-sion in Caucasians and African-Americans (Kumar et aI.,2005) have already been identified. A genetic polymor-phism (variant form of a specific gene) of the serotonin-transporter gene has also been linked to increased risk ofdepression, but only when carriers of the gene are understress (Caspi et aI., 2003). As this study nicely illustrates,life circumstances (e.g., stress) may interact with inheritedgenetic vulnerabilities to determine who develops a spe-cific problem or disease. The likelihood that genetic riskcan be modified by psychosocial factors is a major reasonwhy all of us should pay close attention to lifestyle factorsin our efforts to stay well.
INDIVIDUAL DIFFERENCES IN STRESS RESPONSESEven very young infants reveal marked differences in theirsensitivities to upsetting stimuli. Some infants react tosuch stressors by developing digestive upsets, others bydeveloping sleep disturbances. These differences in reac-tivity continue into adult life and may be linked to individ-ual differences in susceptibility to disease and in the typesof diseases a given person is most likely to develop (seeBlanchard & Scharff, 2002; Schneiderman et aI., 2005).
Genetic inheritance undoubtedly plays a role in deter-mining how we respond to stress. However, early experi-ences are also crucially important. Studies show that ratsthat were repeatedly exposed to 3-hour separations fromtheir mothers were hyperactive when they were placed in anovel environment and had more extreme responses to
stress compared to rats that were separated from theirmothers for only 15 minutes each time (Brake et al., 2004).Also, rats that are raised by highly nurturing and attentivemothers develop into low-anxious adults compared to ratsthat are raised by mothers who have a less caring maternalstyle (see Fish et aI., 2004). Moreover, when rat pups thatwere born to less attentive biological mothers were cross-fostered so that they were raised by more attentive adoptivemothers, they developed into less stress-sensitive adultscompared with their original littermates who remainedwith their biological mothers. Conversely, when rats pupswere removed from their attentive, nurturing biologicalmothers and raised by adoptive mothers who were lessattentive and less nurturing, the rat pups developed intomore reactive and stress-sensitive adults compared withtheir biological siblings who stayed with their biologicalmothers (see Fish et aI., 2004). Overall, the animal data sug-gest that differences in maternal care are causally related toindividual differences in stress sensitivity later in life.
Characteristics of the early family environment arealso associated with physiological vulnerability to stressin humans (see Luecken & Lemery, 2004). For example,children raised in high-conflict families show greater car-diovascular reactivity when they hear audiotapes of argu-ments compared to children who come from familieswhere there is less conflict and marital friction (EI-Sheikh& Harger, 2001).
Finally, research illustrating the interaction of genesand environment shows that children who have fearful ornegative temperaments may be especially vulnerable to thenegative effects of stress. These children showed muchmore extreme physiological reactivity in the face of stressthan did their more laid-back peers (Gunnar et aI., 1996).This highlights the importance of the interaction between
Children who are exposed to a lot of marital conflict in the homeare more reactive physiologically when they are stressed.

genetic predispositions and environmental factors in ourunderstanding of how people respond to negative situa-tions in their lives.
Psychosocial FactorsPERSONALITY CHARACTERISTICS If we could clearlydescribe a "disease-prone" or "hypertensive" personalitylinked to particular diseases, it would be of great value inunderstanding and treating illnesses and perhaps even inpreventing them. Just as useful would be a clear picture ofthe so-called "disease-resistant personality"-one possess-ing a high degree of "hardiness"-or the ability to with-stand stress and bounce back from it (e.g., see Hafen et a1.,1996). Research has shown that negative attitudes are asso-ciated with higher levels of physical and mental illness(especially depression). Developmental research, such asthat described above, also indicates that children with fear-ful or negative temperaments tend to be especially reactivewhen they experience stress. However, as of now, no clearassociations between specific personality characteristicsand particular diseases have been identified.
SOCIAL SUPPORT In our previous discussions, we haverepeatedly noted the destructive effects that stressful inter-personal patterns-including marital unhappiness anddivorce-may have on personality adjustment. Such pat-terns may also influence physiological functioning (Gra-ham et al., in press). In fact, death rates from various
o.V 0 regular visits from volunteers who have
been trained to provide emotional andpractical support extend the lives of peo-ple who are terminally ill? In an effort toaddress this question, one group of
researchers studied hospice patients who were notexpected to live more than 6 months (Herbst-Damm &Kulik, 2005). These patients were, on average, about 73years old and were living in their own homes. Because theirconditions were considered hopeless, they were not receiv-ing any curative medical treatments. The researchers thenlooked to see if those patients who had requested andreceived visits from hospice volunteers survived longerthan those who either did not request any visits or thosewho requested visits but did not receive any (usuallybecause of scheduling reasons). Hospice volunteers arepeople who visit terminally ill patients in their homes andare trained to listen, provide conversation, read to them, orhelp with basic grooming tasks.
causes, including physical disease, are markedly higher inpeople who have recently experienced marital problems ordivorce than in the general population (Burman & Mar-golin, 1992; Johnson et a1., 2000). Loss of a spouse throughdeath also puts the survivor at elevated risk, but men aremore adversely affected by the death of their wives than arewomen by the death of their husbands (Helsing et a1.,1981; Stroebe & Stroebe, 1983).
Findings such as these suggest that being "connected"with others in mutually supportive ways-such as in well-functioning families-is a significant protective factor inmaintaining physical health. Available research stronglysupports that conclusion and extends it beyond the con-fines of the family. Having a good social support system isa significant predictor of good health maintenance (seeGraham et a1., in press; Uchino et al., 1996). As Develop-ments in Practice 10.5 also shows, high-quality supportmay even prolong life in terminally ill patients. Morespecifically, people with higher levels of social supporthave lower blood pressure than people with lower levels ofsocial support. Social support is important for the immunesystem too. College freshman who reported low numbersof social ties showed a poorer immune system responsewhen they were vaccinated for influenza than did fresh-men with more extensive social networks (Pressman et a1.,2005). In other words, the same vaccination provided lessprotection for the more isolated students than it did for thestudents who were more socially integrated. Natural killercell activity (those are the cells that kill tumors) is also
The majority of patients (58 percent) did not requestany visits from the volunteers. However, patients whorequested and received visits lived an average of 80 dayslonger than patients who did not receive any visits. Impor-tantly, patients who had requested visits but who had notreceived them for various reasons had survival times thatwere just like those of the patients did not want to be vis-ited. This suggests that what was important to survivaltime was actually being visited by the hospice volunteer.
The data from this study provide no clues as to whythe patients who received the social support lived longer.Information about the quality of the patients' lives duringthis time was also not available. However, the finding thatpatients who received support visits from volunteers livedalmost 3 months longer than those who did not is an inter-esting and potentially very important finding. Brief, regularvisits from caring people who are good listeners may be arelatively simple way of helping dying patients live slightlylonger and better-quality lives.

10.6CJ t is a situation that we are all familiar with. We
are rushed, busy, and under pressure. There is adeadline to meet, or an exam is imminent. Orperhaps we have had a major argument with aparent, a friend, or a romantic partner. And then,
just when it seems like life is against us and it couldn't getmuch worse, it does. We get a cold.
As we have repeatedly pointed out in this chapter,stress causes our immune systems to function less effi-ciently. Evidence from our everyday lives confirms this, asdoes scientific evidence from the laboratory. SheldonCohen and his colleagues at Carnegie Mellon Universityhave studied people's susceptibility to the common coldfor many years. By deliberately exposing healthy collegestudents to the common cold virus by means of nasaldrops, they have been able to record exactly who gets acold in the days afterward and who doesn't.
In one study Cohen and his colleagues exposed quar-antined, healthy volunteer subjects to the cold virus andassessed the outcome in terms of actual contraction of anupper respiratory infection (URI). Stressful life events, self-perceived stress, and negative emotion, all assessed beforeexposure, each significantly predicted which subjects wouldcome down with colds (Cohen, Tyrrell, & Smith, 1993).
In another study they showed that people who hadmore extensive social support networks (friends in a vari-ety of domains such as work, home, and church) were lesslikely to develop a cold than people who had less diversesocial networks (Cohen, Doyle, et al., 1997). This highlightsthe protective effects of social support on the immune sys-tem. Most recently, Cohen and his colleagues have used aprospective research design to explore how stress andsocial support variables interact (Hamrick et aI., 2002).
Healthy students came to the laboratory and completedmeasures of life events, measures of social network diver-sity, and some other scales. Then, for the next 12 weeks,they kept a diary about any cold or flu symptoms theynoticed. If they felt unwell, they were asked to go to theclinic so that the researchers could confirm that the stu-dents had an upper respiratory infection.
Who developed colds in this observational study?Interestingly, the students who developed colds were theones who had experienced higher levels of negative life
higher in people who have more social support than inpeople who have less. Such findings may help explain whybeing alone and lonely predicts vulnerability to illness anddeath from multiple causes (Graham et aI., in press; Tayloret aI., 2005).
To what extent do such factors as social supportpredict even minor health problems such as colds? As
Stress causes our immune system to function lessefficiently.
events and who also had highly diverse social networks.These findings suggest that although it is generally benefi-cial to the immune system to have a broad network offriends, this is not the case when we are under stress andour resistance to infection is compromised. Under thesecircumstances, having more friends in different placesmeans that we are exposed to a greater range of infectiousagents than would otherwise be the case. In short, whenwe are not stressed, being popular is a good thing. Whenwe are stressed, however, the fewer people we come intocontact with, the better.
The World Around Us 10.6 illustrates, social support isimportant here too, although there is also a downside tobeing popular.
THE LEARNING OF ILLNESSES Although Pavlov andmany subsequent investigators have demonstrated thatautonomic responses can be conditioned-as in the case

of salivation-it was long assumed thatpeople could not learn to control suchresponses "voluntarily." We now knowthat this assumption was wrong. Notonly can autonomic reactivity be con-ditioned involuntarily via the classicPavlovian model, but operant condi-tioning of the autonomic nervous sys-tem can also take place.
What this means is that certainphysical disorders may arise throughaccidental reinforcement of symptom-and-behavior patterns. In short, itappears that some physical disordersmay be acquired and/or maintained inmuch the same way as other behaviorpatterns. As Lang (1970, p. 86) notedlong ago, "A child who is repeatedlyallowed to stay home from school whenhe has an upset stomach may be learning the visceralresponses of chronic indigestion." Some of these factorsare apparent in the case of Annette.
As we have seen, the incidence of spe-cific disorders, both physical and men-tal, varies in different societies, indifferent strata of the same society, andover time. In general, what Cannon(1915) called diseases of civilization donot occur among nonindustrializedsocieties such as the aborigines of theAustralian Western Desert (Kidson &Jones, 1968), the Navajo Indians of Ari-zona, and certain isolated groups inSouth America (Stein, 1970). As thesesocieties are exposed to social change,however, gastrointestinal, cardiovascu-lar, and other diseases begin to appear.There is also evidence of change in thenature and incidence of such disordersin Japan, paralleling the tremendous
social changes that have taken place there since WorldWar II (Ikemi et aI., 1974). For example, hypertension andcoronary heart disease have increased markedly with thepostwar westernization of Japanese culture. In general, itappears that any sociocultural conditions that boost lifestress tend to play havoc with the biological human organ-ism and lead to an increase in disease as well as in otherphysical and mental problems.
In contrast to experimentalresearch (which involvesmanipulating variables in someway and seeing what happens),in observational research theresearcher observes or assessesthe characteristics of differentgroups, learning much aboutthem without manipulating theconditions to which they areexposed. Observational researchis sometimes called "correlationalresearch," although the formerterm is the preferred term.
Annette was 27 years old when she was referred to a ther-apist by her doctor. She had graduated from college andworked for a large insurance company. Although she wasgood at her job, her life was miserable. She was plaguedby stomach problems and was always fearful that shewould have a stomach upset at work. Her biggest fearwas that she would become sick and throw up.
A review of Annette's history revealed that she hadalways been a nervous child. She was very attached toher mother and hated to leave her. Going to school was abig worry for her, and she often developed stomach painsor felt sick shortly before the school bus arrived. Whenthis happened, Annette's mother would allow her to stayhome, and Annette would soon feel better.
Annette's problems with anxiety and stomach upsetscontinued into her adult life. When she was at home, andon weekends, she usually felt fine and would eat fullmeals without any problem. Weekdays, however, were adifferent matter. She became highly attentive to how shewas feeling, and she avoided eating before she went towork. On days when she knew she would have to make apresentation at work, she often felt particularly bad.Sometimes when she got to work and was busy, shewould feel better. But whenever she felt bored or stressed,she usually noticed that she felt a little nauseated. If thisdid not resolve after eating a cracker, she would start toworry that she was going to be sick. At least once a week,things got so bad that she left work early.
In ReVIew~ What biological factors are important in
determining what disorders people aresusceptible to?
~ What personality and psychosocial factorsappear to be associated with resistance todisease?
~ Explain how learning may be involved in thedevelopment of certain illnesses.
TREATMENTS ANDOUTCOMESEven though a particular environmental stressor may havebeen closely linked to the development of a physical illness,removal of this stressor, even when combined with learn-ing more effective coping techniques, may not be enoughto bring about recovery if organic changes have alreadytaken place. Such changes may have become chronic and

irreversible. This further emphasizes the importance ofprevention.
Biological InterventionsAside from immediate and long-range medical measures,such as emergency care for a hypertensive crisis or bypasssurgery for coronary heart disease, good clinical practicerequires that patients receive appropriate biological treat-ments for their problems. For patients with CHD, suchtreatments might include lipid-lowering medications, aswell as aspirin or other drugs that can act as anticoagu-lants. Anxiolytic (anxiety-reducing) medications of thebenzodiazepine family, such as clonazepam (Klonopin) oralprazolam (Xanax), might also be used to reduce emo-tional tension. Such drugs do not address the stressful sit-uation or the coping reactions involved; but by alleviatingemotional tension and distress they may give the person anopportunity to regroup his or her resources and developmore effective means of coping with life's problems. Ofcourse, clinicians must guard against too readily prescrib-ing tranquilizers to insulate patients against everyday stressthat they might be better off facing and resolving in somemanner. Some patients may also come to rely too much ontheir prescriptions for easy cures, and fail to addressaspects of their lifestyles that are unhealthy and destruc-tive. The development of dependence on anxiolytic med-ications is also a very real problem.
In light of the strong associations between depressionand risk for CHD, treating depression is of the utmostimportance. Unfortunately, most people with clinicaldepression go untreated, giving them unnecessary addedrisk for CHD. Moreover, even though there is no medicalrisk factor that is more important in predicting mortalityfor patients who have already had a heart attack (Welinet aI., 2000), physicians often fail to treat depression intheir cardiac patients. Instead, they dismiss it as an under-standable consequence of having had a life-threateningmedical scare (Glassman, 2005). Of those with majordepression at the time of a heart attack, approximatelyone-half of those who have gone without treatmentremain depressed or else have relapsed again 1 year later(Hance et aI., 1996).
New research data are highlighting the thousands oflives that can be saved each year by giving antidepressantmedications to patients who have suffered a myocardialinfarction and who are depressed. In the most thoroughinvestigation of this issue to date, Taylor et al. (2005)reported that patients treated with selective serotoninreuptake inhibitors (SSRls) were much less likely to die orhave another heart attack than patients who were not tak-ing antidepressant medications. Perhaps surprisingly, inthis study treatment with cognitive behavior therapy(CBT) was not associated with reduced mortality in thepatients, although CBT treatment did help alleviatedepression (see Berkman et aI., 2003; Glassman, 2005).
TRADITIONAL PSYCHOTHERAPY Even though psy-choanalytic theory has long emphasized associationsbetween emotions and physical illness, psychotherapy hasbeen largely ineffective in treating psychophysiologicaldisorders (Agras, 1982). One-on -one, nonspecificallydirected, verbally oriented psychotherapies-aimed athelping patients understand their personality problems-just don't seem to help alleviate psychophysiological ill-nesses. On the other hand, "opening up" and writingexpressively about life problems in a systematic way doesseem to be an effective therapy for many persons with ill-nesses (Pennebaker, 1997; Smyth, 1998).
In the first study of emotional disclosure in peoplewith rheumatoid arthritis, Kelley, Lumley, and Leisen(1997) found that people who had written about theiremotions had significantly less physical dysfunction thanthose assigned to a control condition. In another study,people with either rheumatoid arthritis or asthma wereasked either to write about their most traumaticallystressful life experience or (in the case of the controlgroup) to write about their plans for the day. Subjectswrote for 20 minutes for 3 consecutive days. When theywere assessed 4 months later, the participants withrheumatoid arthritis who were assigned to the emotionaldisclosure condition were doing significantly better thanthe participants with rheumatoid arthritis who wereassigned to the control group.
In studies that involve emotional disclosure, patientsoften experience initial increases in emotional distressduring the writing phase but then show improvement intheir medical status over follow-up. Why emotional dis-closure provides clinical benefits for patients is still notclear, however. One reason could be that patients aregiven an opportunity for emotional catharsis, or "blow-ing off steam." Another possibility is that writing givespeople an opportunity to rethink their problems. Givenwhat we know about the link between emotional andphysical well-being, it is not unreasonable to speculatethat both of these processes could help improve immunefunction or perhaps decrease levels of circulating stresshormones.
There is also some evidence that psychological inter-ventions can help post-heart attack patients who aredepressed. In a review of the literature, Linden and col-leagues (1996) reported that psychosocial interventionscan decrease depression, systolic blood pressure, heart rate,and cholesterol levels in CHD patients. Moreover, patientswho did not receive psychosocial treatment were 1.7 timesmore likely to die from their CHD-and 1.8 times morelikely to have another heart attack in a 2-year follow-upperiod-than patients who were treated for their depres-sion and anxiety. Another study has shown that the cardiacrehabilitation and exercise programs that are frequentlysuggested to patients who have had a heart attack to

improve their physical condition also significantly improvetheir depression (Milani et al., 1996).
BIOFEEDBACK Somewhat ironically in light of its focuson altering physiological states, biofeedback treatment hasgenerally failed to live up to the enthusiasm it generatedwhen it was first introduced. However, biofeedback doesseem to be helpful in treating some conditions, such asheadaches, for example (E. B. Blanchard, 1992, 1994; Blan-chard, Appelbaum, Radnitz, Morrill, et al., 1990). Flor andBirbaumer (1993) have also reported impressive effective-ness, especially in long-term follow-up, for electromyo-graphic (muscle tonus) biofeedback in the control ofmusculoskeletal pain. In general, however, the effects ofbiofeedback tend to be small and they rarely exceed thosethat could be obtained in simpler (and less expensive)ways, such as by providing systematic relaxation trainingwithout biofeedback equipment (Carlson & Hoyle, 1993;Reed, Katkin, & Goldband, 1986).
BEHAVIOR THERAPY Behavioral approaches playamaj?r role in helping people alter dangerous lifestylechOKes such as smoking and excessive alcohol use (seeChapter 12). These obviously have major implications forphysical health. Giving up smoking, for example, leads to a40 percent reduction in mortality in patients with CHD(Wilson, Gibson, et al., 2000).
Researchers have also examined the effects of variousbehavioral relaxation techniques on selected stress-relatedillnesses. The results have been variable, though generallyencouraging. For example, simple tension headaches haveproved quite amenable to general relaxation treatmentprocedures (E. B. Blanchard, 1992; Blanchard, Appelbaum,Radnitz, Michultka, et al., 1990; see also Holroyd, 2002). In
Though biofeedback may be nothing more than an elaboratemeans to teach patients how to relax, it has been used~ff~Niv~lyto ~Mtr~1rnu~tul~~k~l~taJpain and reduceheadache pain.
addition, there is evidence that relaxation techniques canhelp patients with essential hypertension (see Blumenthalet al., 2002).
A growing topic of interest is meditation. Schneiderand colleagues (2005) have recently shown that the dailypractice of Transcendental Meditation may be helpful inreducing blood pressure. In this study, 194 African-American patients with chronic hypertension were ran-domly assigned to receive training in either TranscendentalMeditation or progressive muscle relaxation (whichinvolves tensing and relaxing various muscle groups in asystematic way), or else to receive general informationabout lifestyle changes that would be helpful to them.Patients who practiced Transcendental Meditation for20 minutes twice a day reduced their diastolic bloodpressure significantly more than did patients who prac-ticed muscle relaxation or who received sound healthcare advice.
COGNITIVE-BEHAVIOR THERAPY CBT has beenshown to be an effective intervention for headache (E. B.Blanchard, 1992; Blanchard et al., 1990a, 1990b; Holroyd,2002) as well as for other types of pain (Keefe et al., 1992).CBT-oriented family therapy was markedly more success-ful than routine pediatric care in alleviating children'scomplaints of recurrent abdominal pain (Sanders et al.,1994). Deale and colleagues (1997) have also demon-strated that CBT is an effective treatment for chronicfatigue syndrome (see The World Around Us 10.7), theclinical status of which continues to be a matter of contro-versy (e.g., Jason et al., 1997). Some CBT techniques havealso been used for stress management (Hafen et al., 1996).
Sociocultural ApproachesSoci?cultural treatment measures are aimed more at pre-ventIOn and are typically applied to selected populationso~ subcultural groups thought to be at risk for developingdIsorders, as we will discuss more in Chapter 18. Withinthese .groups, people attempt to alter certain lifestylebe~avIOrs to reduce their overall level of susceptibility toa dIsorder. For example, cigarette smoking is associatedwith increased risk for lung cancer and heart disease; toreduce the general risk of these illnesses, persistent effortshave been made to reduce or prevent smoking. Similarly,some association exists between high-cholesterol dietsand coronary heart disease, and efforts are made to con-vince people to alter their diets to reduce the rate of coro-nary .heart dis.ease in the total population. Obviously,such mterventIOn efforts involve substantial amounts ofpersuasion-often employing the media and, in the caseo~ s.moking, changes in federal and local laws restrictingmIme, restaurant, and workplace smoking. If you smokeand need yet another reason to quit, you might also con-

10.7rw e have all had days when we feel so
tired that even small tasks seem torequire too much effort. For most of us,this situation is usually temporary andis alleviated by rest. Imagine what life
would be like, however, if you felt physically exhausted formonths or years on end. This is what chronic fatigue syn-drome is like.
Chronic fatigue syndrome (CFS) is distinguished bydebilitating fatigue that cannot be explained by a knownmedical condition, substance use, or mental disorder. Tomeet the criteria for this diagnosis, the fatigue has to last6 months or more. For many sufferers, however, CFS canlast for years. Many patients also report diminishedappetite, low-grade fever, balance problems, nausea, andnight sweats. Although it was initially thought that CFSmight be a form of "atypical depression," evidence is grow-ing that this is not the case (e.g., Moss-Morris & Petrie,2001). Some of the symptoms of CFS (such as sore throat,joint pain, and swollen lymph nodes) are not characteristicof depression. In addition, many of the symptoms that aretypical of depression, such as guilt and lack of motivation,are virtually absent in CFS (Komaroff & Buchwald, 1998).
The typical patient with CFS is a white, middle-classfemale in her thirties_ However, CFS is found in both chil-dren and adults and in people of all races, ethnicities, andsocial classes. The prevalence of the disorder in adults isaround 0.1 percent. Although the causes of CFS are stillunclear, viral infection and immunological and neuroen-docrine abnormalities seem to be involved. Very often CFSbegins with a sudden flu-like illness or another kind ofmedical problem. However, when the medical conditionsubsides, the physical problems and the social and occu-pational impairments continue (Komaroff & Buchwald,1998). Keith Jarrett, the jazz pianist, suffers from CFS. Sodoes Laura Hillenbrand, author of the best-selling bookabout the racehorse called "Sea biscuit." She describes theonset of her CFS in the following way:
"In the spring of 1987 I was a sophomore at Kenyon Col-lege, majoring in English and history. I was nineteen,healthy and fit, playing tennis and cycling several times
sider the following: One study has shown that 41 percentof all current smokers have some form of current mentaldisorder (Lasser et aI., 2000). The fact that someonesmokes is therefore a cue that she or he might be morelikely to have mental problems than someone who doesnot smoke.
a week. On the night of March 20th, while traveling backto Kenyon from spring break, I developed apparent foodpoisoning and became sick enough that my roommatescalled paramedics. For three weeks, I couldn't seem toshake the stomach upset. Then one morning, I awoke soweak that I was unable to sit up. It took me two hours towork up the strength to stand. I expected the exhaustionto pass, but it didn't. For weeks, I couldn't even makethe short walk to the dining hall. ... I had to drop out ofschool. I spent the next eight months bedridden. I wasunder siege from constant infections, unremitting fever,chills, soaking sweats, acute light sensitivity, and bal-ance and cognitive problems. In the first month alone Ilost twenty pounds, weight I couldn't afford to lose; Ifinally leveled off at one hundred pounds. I was diag-nosed with Chronic Fatigue Syndrome by the head ofinfectious diseases at Johns Hopkins.
Though my health has fluctuated since then,and at times I have enjoyed improvement, I've neverrecovered."
CFS is still poorly understood. There is controversyover the direction of the correlation between fatigue anddistress: whether psychological disorder is a cause of CFS,whether psychological problems maintain CFS, or whetherpsychological problems are a secondary reaction to CFS.Some of the confusion may stem from diagnostic prob-lems. People who are depressed or overworked but whopresent to their doctors with extreme fatigue may be mis-diagnosed as having CFS. Certainly there is evidence thatthe immune system is activated in CFS sufferers. Givenwhat we know about cytokines (see Developments inResearch 10.1), it is quite possible that CFS reflects thebody's inability to return to a state of equilibrium afterbeing challenged by an infectious agent. Moreover, in viewof the links between the brain and the immune system, itis not surprising that the treatments of choice for CFS donot involve antiviral agents or medications of any sort.Rather, patients appear to do best when they are involvedin a graded exercise program or else receive cognitive-behavioral therapy (Whiting et aI., 2001), although thesetreatments are not curative.
As we learn more about the role of biological, psy-chosocial, and sociocultural factors in the etiology of dis-ease, it becomes increasingly possible to identify high-riskpersons and groups, such as heart-attack-prone personal-ities with chronic negative affect, young singles whoengage in unsafe sex) and groups living in precarious and

rapidly changing life situations. This ability to identifythose at risk enables treatment efforts to focus on earlyintervention and prevention. In this context, programsaimed at fostering changes in maladaptive lifestyles and atremedying pathological social conditions seem highlyworthwhile.
In ReVIew~ What psychosocial approaches are helpful
for people with diseases that have apsychological component?
~ What are the major objectives of socioculturalmeasures taken to treat diseases that have apsychological component?
~ Why is it important that patients with heartdisease be screened for depression andtreated if depression exists?
Does Clinical Practice Ignore theDoctor-Patient Relationship?
5li s we've already mentioned in this chapter,for most of its history the medical professionsurvived and prospered not so muchbecause it had available, effective remediesfor illnesses but, rather, because physicians
were able unwittingly to rely on the power of the placeboresponse in their patients. As medicine moved into the modernera, treatment of illness became increasingly an application ofrapidly advancing and technologically sophisticated biologicalscience. Enormous progress has been made in the control andactual conquering of many diseases that were once scourges ofhumankind. Virtually all of this progress has been due to medi-cine's adoption of a relentlessly scientific approach.
There are increasing signs, however, that somethingvaluable may have been lost in this enthusiastic embrace ofscience and the "objectivity" it both bestows on anddemands of its practitioners. The inherent temptation is forthe physician to become a mere technician who administers
the marvels of modern medical science to objectified patients(or, in a worse scenario, to objectified parts of patients). Thattemptation is strengthened by economic trends and therelated development of "managed care" medicine, whereinphysicians have fewer options and patients are often"processed" in assembly-line fashion. There is obvious andgrowing public restlessness about this model of "servicedelivery." The need for something more satisfying to patientsshows up in the increasing interest in "alternative" varietiesof medicine, the proliferation of medical self-help publica-tions, and a heightened interest among members of the U.S.Congress in the details of medical practice.
Given what we now know about the intricate connec-tions among mind, body, and society in disease processes,the ongoing reorganization of the medical care delivery sys-tem seems thus far to have ignored what behavioral medicinehas taught us: It is important to treat not only the disease butalso the person with the disease.

~ Emotional factors influence the development of many cytokines," dampen the response that the immunephysical disorders and play an important role in the system makes when it is challenged.course of disease. DSM-IV-TR recognizes this with the ~ Negative emotional states, such as being under a lotcategory called "Psychological Factors Affecting a of stress or having low social support, can impair theGeneral Medical Condition." functioning of the immune system and the
~ To recognize that psychological problems can also cardiovascular system, leaving a person moreresult from medical problems, DSM-IV-TRalso has a vulnerable to disease and infection. Damaging habitscategory called "Mental Disorders Due to a General and lifestyles such as smoking and obesity alsoMedical Condition." enhance risk for physical disease.
~ The field of behavioral medicine grew out of the ~ Many physical illnesses seem to be linked to chronicgeneral recognition that physical and emotional well- negative emotions such as anger, anxiety, andbeing are intimately interrelated. It seeks to extend depression. Hostility is well established as anour conception of disease beyond the traditional independent risk factor for CHD. The same is true ofmedical focus on physical breakdown of organs and depression.organ systems. ~ Positive psychology is an emerging field that is
~ When we are stressed, the autonomic nervous system concerned with human traits and resourcesresponds in a variety of ways. One consequence of associated with health and well-being. One factorstress is increased production of cortisol. High levels that is associated with greater well-being is having anof this stress hormone may be beneficial in the short optimistic outlook on life.term but problematic over the longer term, ~ Factors such as genetic vulnerabilities, excessive
~ In the immune system, specialized white blood cells autonomic reactivity, and possible organ weaknessescalled B-cells and T-cells respond to antigens such as remain important in our understanding of the causesviruses and bacteria. They are assisted by natural of physical diseases. They must be a part ofkiller cells, granulocytes, and macrophages. treatment considerations whenever physical disease
~ Psychoneuroimmunology is an exciting and occurs, regardless of strong evidence of
developing field. It is concerned with the interactions psychological contributions to its development.
between the nervous system and the immune system. ~ A common factor in much psychosocially mediated
~ Cytokines are chemical messengers that allow the physical disease is inadequacy in an individual's
brain and the immune system to communicate with coping resources for managing stressful life
each other. Some cytokines respond to a challenge to circumstances. Cognitive-behavioral therapy, in
the immune system by causing an inflammatory particular, shows much promise in alleviating this
response. Other cytokines, called "anti-inflammatory type of health-endangering problem.
allostatic load (P. 347)
antigens (P. 348)
B-cell (P. 348)
behavioral medicine (P. 344)
biofeedback (P. 366)
chronic fatigue syndrome (US)(p.367)
cortisol (P. 347)
cytokines (P. 348)
essential hypertension (P. 355)
health psychology (P. 344)
HPAaxis (P. 347)
hypertension (P. 355)
immunosuppression (P. 350)
observational study (P. 363)
placebo effect (p, 354)
positive psychology (P. 353)
psychoneuroimmunology (p, 350)
psychophysiological disorders(p.346)
T-cell (P. 348)
Type A behavior pattern (P. 356)
Type 0 personality (P. 357)




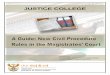











![[XLS] · Web viewNICMAR 07 Oct 1997 NICO BASSON VAN VELDEN - DUFFEY TERBLANCHE J BOX 2381 PRETORIA 0001 NICO ROUX FAMILY 16 Jul 2007 (012) 21 9521 LOGISTA 012-43 2826 NICOLE POTGIETER](https://img.pdfslide.us/doc/110x75/5ae8edec7f8b9acc2690cd29/xls-viewnicmar-07-oct-1997-nico-basson-van-velden-duffey-terblanche-j-box-2381.jpg)












