Embed Size (px)
DESCRIPTION
ablatio retinal surgery
Citation preview

January/February 2014 retina today 45
cover story
Controversies in Vitreoretinal Surgery:
is Scleral buckling an important Mainstay in the treatment of retinal detachment in 2014?
Scleral Buckle for Retinal Detachment: Pro
By Gaurav K. Shah, MD; and Baseer Ahmad, MDIs scleral buckling surgery for retinal detach-ment (RD) repair here to stay? We believe the answer is “yes,” but only if ophthalmolo-
gists continue to perform and teach these procedures. If we do not, scleral buckling procedures will pass into history.
There is no doubt that pars plana vitrectomy (PPV) is an effective procedure, valued day in and day out. So are scleral buckling procedures, however, for appropri-ate cases. Even so, scleral buckling procedures have become eclipsed by PPV. A PubMed search revealed the following: since 1956, 2745 articles have been published on scleral buckling; since 1970, 12 341 articles have been published on PPV; since 1972, 1073 articles have been published on scleral buckling plus PPV. In the past 5 years, the difference is even more pronounced, with 395 articles on scleral buckling, 3126 on PPV, and 234 on both procedures.
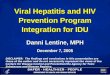
Medicare claims data (Figure 1) also reflect this trend. From 2000 to 2011, use of the PPV code has more than doubled, from about 15 000 annual procedures to about 32 000. Meanwhile, the use of scleral buckling has declined, from 6000 to 2000 procedures per year.
Several factors may be responsible for these changes.
The availability of small-gauge instrumentation, wide-angle viewing systems, high-speed cutters, and better illumination have made PPV much easier. Surgeons may also lack confidence in their skills with indirect ophthal-moscopy, and there is less time spent on scleral buck-ling by mentors and training programs. Economic and time factors play a role. In addition, there is no industry support of scleral buckling at this point.
At the same time, there is a growing list of misconcep-tions about scleral buckling. These include the following:
• The success rate with scleral buckling is lower than that with PPV;
• The choice of initial treatment does not make a dif-ference in failure outcomes;
• Scleral buckling has a high incidence of complications;• There is a significantly higher amount of myopia
after scleral buckling compared with PPV;• Rates of proliferative vitreoretinopathy (PVR) are
higher after scleral buckling than after PPV.
MISCONCEPTIONS EXAMINEDA look at the relevant literature shows that all of the
above are incorrect assumptions.Success rates. Reviewing the published results of
retrospective and prospective comparative case series from 2000 to the present,1-15 the single-operation success
Figure 1. Medicare claims data shows the increase in use of
the PPV code and the decline of scleral buckling.
These articles are based on the debate-style presenta-tions at the American Academy of Ophthalmology Retina Subspecialty Day in New Orleans November 15-16, 2013. The arguments presented by the authors, affirmative or negative, were assigned to them and do not necessarily reflect their own opinions and practices.
eyetube.netONLINE SURVEY

46 retina today January/February 2014
cover story
rate is better with PPV in some papers and with scleral buckling in others, with no preponderance of greater suc-cess with PPV or scleral buckling. However, when results are broken down into phakic and pseudophakic groups, it becomes clear that in pseudophakic eyes PPV is the more common procedure with the higher success rate. Conversely, in phakic eyes, single-operation success with scleral buckling seems to be equivalent, and in some cases superior, to PPV.
A recent multicenter study16 reached a similar conclusion. This nonrandomized retrospective study assessed success and failure of the primary procedure in the treatment of 7678 rhegmatogenous RDs by 176 sur-geons on 5 continents. Final success rate in phakic eyes was higher with scleral buckling than with PPV (99.5% vs 98.7%; P = .028). The study authors concluded that, in the treatment of uncomplicated phakic RD, repair using scleral buckling is at least equivalent to PPV.
Initial treatment does not matter. In a retrospective study including 1402 eyes,17 those who failed initial treatment with scleral buckling required approxi-mately 30% fewer secondary retinal procedures, and a third less use of silicone oil, compared with those who underwent initial PPV or PPV plus scleral buckling. The study authors concluded that it is easier to fix a scleral buckle failure than a PPV failure.
High complication rate. In literature from the late 1990s,18 fairly high rates of diplopia (10–24%), strabismus (4–8%), and buckle extrusion (3–8%) were reported after SBP. Most of these reports of intractable strabismus and other complications were related to hydrogel buckling elements that are no longer used.
We presented data on the complications of 305 scleral buckling procedures in 2010.17 In that series, there were no cases of migration or removal of buckles. In addition, the rate of diplopia and strabismus was not
statistically significantly different between scleral buck-ling (5.2%) and PPV (3.6%; P = .29). It is true that there is a risk of complications with scleral buckling, as with any surgery. But the rates of diplopia, migration, and other complications are low.
Higher amount of myopia. It is also true that scleral buckling can induce significant myopia. With proper tensioning of the band or buckling element, however, this is often much less than many assume. It is not well-recognized that PPV itself can induce refractive shift, thought to be caused by changes in corneal curvature and scleral architecture after PPV. In a randomized sin-gle-center study,19 the mean change in refractive error was 1.38 D after scleral buckling and 0.85 after PPV.
Higher rate of PVR. Several of the prospective and retrospective studies cited above also looked at rates of PVR after scleral buckling and PPV. As with single-operation success rates, some reported a higher rate of PVR with scleral buckling and others with PPV. In our own series,17 there were no statistically significant dif-ferences after scleral buckling and PPV in the rates of redetachment secondary to PVR (4.3% vs 6.4%, respec-tively) or of PVR without detachment (0.7% vs 1.4%, respectively).
ADVANTAgES Of SCLERAL BUCkLINgScleral buckling offer some advantages over PPV.
In young patients, the crystalline lens—and therefore accommodation—is preserved. In older patients, the vitreous is preserved. For patients with extensive lattice degeneration or an abnormal vitreoretinal interface, scleral buckling provides 360° support of the vitreous base and peripheral retina. Scleral buckling is an extraocular surgery, unless drainage of subretinal fluid is required, and thus lessens the risk of complications related to entering the eye, such as endophthalmitis.
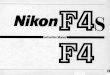
Figure 2. Color photo montage showing a classic case of
chronic retinal detachment due to atrophic holes, some
within lattice.
Figure 3. Color photo montage showing a broad inferior reti-
nal tear in a young myopic patient.
Figures 2 and 3 courtesy of Richard MacDonald, M
D.
eyetube.net
http://j.mp/LplIdV

January/February 2014 retina today 47
cover story
Also, if the procedure is done without use of gas, then there is no need for postoperative patient positioning or air travel restriction.
The equipment and personnel costs are lower with scleral buckling. A comparison of the costs of scleral buckling and PPV for RD repair found that, consider-ing all costs, including eventual cataract surgery, scleral buckling procedures were 10.7% less expensive than PPV for RD repair in phakic patients. In contrast, PPV was 12% less expensive than scleral buckling in pseu-dophakic or aphakic patients.20 The average cost per phakic patient was about $700 less for scleral buckling than for PPV. Equipment costs for surgery centers such as ours are approximately $105 for scleral buckling and range from roughly $540 to about $800 for PPV.
CONCLUSIONS
Scleral buckling certainly continues to deserve a place in the armamentarium for RD repair. Typical RD sce-narios in which scleral buckling might be the superior choice over PPV include the following:
• young patients with attached vitreous and chronic detachment due to atrophic holes in lattice;
• uncomplicated single tear in a phakic high myope; • retinal dialysis; • extensive lattice with abnormal vitreoretinal
interface or multiple breaks along the vitreous base.
We continue to use scleral buckling because this approach works well in appropriately selected cases (Figures 2 and 3); it involves no intraocular surgery, results in no cataractogenesis, and necessitates no post-operative positioning; it restores vision more quickly; it leads to better outcomes if patients are not corrected in a single procedure; and it is economically cost-effec-tive. Scleral buckiling surgery is our treatment of choice for phakic RD.
The myths about scleral buckling are simply not true. Treatment decisions are driven by perceptions and by economic, time, and convenience factors. We must tailor our treatments to patients’ needs, whether the choice be scleral buckling, scleral buckling plus PPV, or PPV alone, rather than adhering to a single approach.
Currently, many ophthalmology training programs are moving away from teaching scleral buckling. If the decline in scleral buckling teaching and use is not cor-rected, this skill will soon be lost to our profession. We believe that scleral buckling procedures continue to be important tools in the vitreoretinal surgeon’s arma-mentarium. The less frequent performance of scleral buckling is a reflection of current training patterns and time and economic factors rather than their true value.
Gaurav K. Shah, MD, is a Partner at The Retina Institute, St. Louis, MO. Dr. Shah states that he serves as a consultant for QLT, Dutch Ophthalmic, Alcon, Heidelberg Engineering, Allergan, Thrombogenics, Synergetics, and Johnson and Johnson. He may be reached at [email protected].
Baseer Ahmad, MD, is a retina fellow at The Retina Institute.
1. Oshima Y, Yamanishi S, Sawa M, Motokura M, Harino S, Emi K. Two-year follow-up study comparing primary vitrectomy with scleral buckling for macula-off rhegmatogenous retinal detachment. Jpn J Ophthalmol. 2000;44(5):538-549.2. Miki D, Hida T, Hotta K, Shinoda K, Hirakata A. Comparison of scleral buckling and vitrectomy for retinal detachment resulting from flap tears in superior quadrants. Jpn J Ophthalmol. 2001;45(2):187-191.3. Roider J, Hoerauf H, Hager A, Herboth T, Laqua H. Conventional ablation surgery or primary vitrectomy in complicated retinal holes. [Article in German] Ophthalmologe. 2001;98(9):887-891.4. Afrashi F, Erakgun T, Akkin C, Kaskaloglu M, Mentes J. Conventional buckling surgery or primary vitrectomy with silicone oil tam-ponade in rhegmatogenous retinal detachment with multiple breaks. Graefes Arch Clin Exp Ophthalmol. 2004;242(4):295-300. 5. Wickham L, Connor M, Aylward GW. Vitrectomy and gas for inferior break retinal detachments: are the results comparable to vitrectomy, gas, and scleral buckle? Br J Ophthalmol. 2004;88(11):1376-1379.6. Mansouri A, Almony A, Shah GK, Blinder KJ, Sharma S. Recurrent retinal detachment: Does initial treatment matter? Br J Ophthalmol. 2010;94(10):1344-1347.7. Tewari HK, Kedar S, Kumar A, Garg SP, Verma LK. Comparison of scleral buckling with combined scleral buckling and pars plana vitrectomy in the management of rhegmatogenous retinal detachment with unseen retinal breaks. Clin Experiment Ophthalmol. 2003;31(5):403-407.8. Ahmadieh H, Moradian S, Faghihi H, et al; Pseudophakic and Aphakic Retinal Detachment (PARD) Study Group. Anatomic and visual outcomes of scleral buckling versus primary vitrectomy in pseudophakic and aphakic retinal detachment: Six-month follow-up results of a single operation--report no. 1. Ophthalmology. 2005;112(8):1421-1429.9. Stangos AN, Petropoulos IK, Brozou CG, Kapetanios AD, Whatham A, Pournaras CJ. Pars-plana vitrectomy alone vs vitrectomy with scleral buckling for primary rhegmatogenous pseudophakic retinal detachment. Am J Ophthalmol. 2004;138(6):952-958.10. Sharma YR, Karunanithi S, Azad RV, et al. Functional and anatomic outcome of scleral buckling versus primary vitrectomy in pseudophakic retinal detachment. Acta Ophthalmol Scand. 2005;83(3):293-297.11. Brazitikos PD, Androudi S, Christen WG, Stangos NT. Primary pars plana vitrectomy versus scleral buckle surgery for the treatment of pseudophakic retinal detachment: a randomized clinical trial. Retina. 2005;25(8):957-964.12. Weichel ED, Martidis A, Fineman MS, et al. Pars plana vitrectomy versus combined pars plana vitrectomy-scleral buckle for primary repair of pseudophakic retinal detachment. Ophthalmology. 2006;113(11):2033-2040.13. Heimann H, Bartz-Schmidt KU, Bornfeld N, et al; Scleral Buckling versus Primary Vitrectomy in Rhegmatogenous Retinal Detachment Study Group. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment: A prospective randomized multicenter clinical study. Ophthalmology. 2007;114(12):2142-2154.14. Shah GK, Almony A, Blinder K, Ahmad B. Recurrent retinal detachment. Paper presented at: Retina Subspecialty Day, Annual Meeting of the American Academy of Ophthalmology; November 10, 2012; Chicago.15. Mansouri A, Almony A, Shah GK, Blinder KJ, Sharma S. Recurrent retinal detachment: Does initial treatment matter? Br J Ophthalmol. 2010; 94(10):1344-1347.16. Adelman RA, Parnes AJ, Ducournau D; European Vitreo-Retinal Society (EVRS) Retinal Detachment Study Group. Strategy for the management of uncomplicated retinal detachments: the European vitreo-retinal society retinal detachment study report 1. Ophthalmology. 2013;120(9):1804-1808. 17. Shah GK, Almony A, Blinder KJ. Postoperative complications of retinal detachment repair with scleral buckles. Paper presented at: Retina Subspecialty Day, Annual Meeting of the American Academy of Ophthalmology; October 16, 2010; Chicago.18. Regillo CD, Benson WE. Retinal Detachment: Diagnosis and Management. Philadelphia: Lippincott-Raven: 1998.19. Sharma YR, Karunanithi S, Azad RV, Vohra R, Pal N, Singh DV, Chandra P. Functional and anatomic outcome of scleral buckling versus primary vitrectomy in pseudophakic retinal detachment. Acta Ophthalmol Scand. 2005;83(3):293-297.20. Seider MI, Naseri A, Stewart JM. Cost comparison of scleral buckle versus vitrectomy for rhegmatogenous retinal detachment repair. Am J Ophthalmol. 2013;156(4):661-6666.
Scleral Buckle for Retinal Detachment: Con
By Szilárd Kiss, MDA key term in the title of this debate is the phrase an important mainstay. One cannot say that there is no longer a role for scleral buckling surgery in 2014, but rather, we can
say that in the era of modern vitreoretinal surgery this role has become extremely limited.
Scleral buckling surgery is, therefore, not an impor-tant mainstay in the treatment of retinal detachment (RD). It has been an important surgical technique in

48 retina today January/February 2014
cover story
the past, and it can still be effective in selected cases. However, other techniques, specifically pars plana vitrectomy (PPV) and pneumatic retinopexy, have advanced RD repair to a higher level of technology, accuracy, and precision (Figures 1-4).
When a technology has advanced, it does not mean we cannot use the old technology, but we may not wish to. This is reflected in a worldwide trend away from scleral buckling.
DECLININg USEThe Preferences and Trends (PAT) surveys by the
American Society of Retina Specialists1 offer insights into current practices among our colleagues. When asked in 2011 “In what percentage of RD cases do you implant a scleral buckle?” about 45% of respondents (n=335) said they used scleral buckling 20% of the time or less often. Only about 25% said they would use scleral buckling more than 60% of the time.
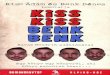
Figure 1. A 47-year-old phakic man with 1 week of infranasal
visual field cut presents with a superotemporal horseshoe
tear and a macula-off, fovea-threatening retinal detachment.
Figure 3. A 64-year-old pseudophakic myopic woman pre-
sented with a 2-week of history of worsening infranasal visual
field cut. Examination showed multiple retinal holes and a
larger horseshoe tear superotemporally.
Figure 2. Same eye as Figure 1. Three days after an office pro-
cedure involving cryotherapy and pneumatic retinopexy, gas
can be seen superiorly with the retina completely attached.
Figure 4. Same eye as Figure 3. Four weeks following small
gauge transconjunctival 25-gauge vitrectomy, endolaser and
SF6 gas, the retina is completely reattached. Vision returned
to 20/20 without correction.

Other questions on the PAT surveys ask about spe-cific cases. In the 2013 survey, for a pseudophakic 3.00 D myope with a superior, macula-on RD and a single tear anterior to the equator, roughly 8% of US surgeons (n= 685) said they would choose scleral buckling, 53.4% chose PPV alone, 13% chose PPV plus scleral buckling, and 25.3% chose pneumatic retinopexy. That is, close to 80% expressed preference for PPV or pneumatic retino-pexy, compared with less than 10% for scleral buckling.
Traditionally, there has been a preference for scleral buckling in phakic patients, as the extraocular sur-gery does not routinely lead to cataract progression. However, in this population scleral buckling shows signs of being replaced by pneumatic retinopexy. In the 2012 PAT survey, for a phakic 3.00 D myope with a superior, macula-on RD and a single tear anterior to the equa-tor, 25% of US respondents (n=543) said they would choose scleral buckling, 21% chose PPV without scleral buckling, 7% chose PPV plus scleral buckling, and 46% chose pneumatic retinopexy. That is, almost double the number of respondents chose pneumatic retinopexy as chose scleral buckling for this phakic patient.
NOT ThE SAME SURgERYAnother reason for the trend away from scleral buck-
ling is that the PPV used in some of the studies cited by Gaurav Shah, MD, and Baseer Ahmad, MD, in their caccompaying article is not the same as the PPV being performed today. Transconjunctival sutureless PPV with 23-, 25-, and 27-gauge instrumentation is a differ-ent experience—for the surgeon and the patient—from traditional 20-gauge vitrectomy.
With small-gauge instrumentation and widefield viewing systems, surgeons have reported excellent outcomes, in some series achieving a 95% or greater single-operation success rate with PPV.2,3 Even patients traditionally considered relatively poor candidates for vitrectomy, including phakic patients and those with inferior retinal breaks, may also be treated with PPV.
Until the middle of the past decade, there was no prospective randomized multicenter trial comparing scleral buckling with PPV. Reviewing the literature in 2006, Schwartz and Flynn said the consensus “appears to be that scleral buckling and primary PPV may yield comparable single-operation success rates and visual acuity outcomes for a wide variety of rhegmatogenous retinal detachments.”4
In 2007, a prospective randomized trial comparing scleral buckling and PPV in rhegmatogenous RD found a visual benefit for scleral buckling in phakic patients. In pseudophakic patients, there was no significant dif-ference in visual benefit with scleral buckling compared

50 retina today January/February 2014
cover story
with PPV. Based on better anatomic outcomes with PPV, the study authors recommended the use of PPV in these patients.5
ADVANTAgES Of PARS PLANA VITRECTOMYThere are numerous advantages of PPV over scleral
buckling surgery. With PPV, the surgeon is better able to visualize all retinal breaks and tears and to ensure removal of all media opacities and synechiae. PPV affords the opportunity to relieve the vitreous trac-tion that caused the RD. Small-gauge PPV techniques are associated with shorter surgical times, less surgical trauma, lower levels of postoperative inflammation, and faster postoperative recovery.
In addition, a number of complications have been associated with scleral buckling but not with PPV. These include extraocular muscle dysfunction, choroi-dal detachment, anisometropia, significant postopera-tive pain, residual subretinal fluid, and short- and long-term buckle infection or extrusion.
CASE fOR PNEUMATIC RETINOPEXYPneumatic retinopexy is a minimally invasive, cost-
effective office procedure that can be a useful alternative for RD repair. There is a relatively high single-procedure success rate (65%–70% in most series), and final success rate approaches 100%, most often with 1 additional pro-
cedure.6,7 Anatomic outcomes are equivalent between scleral buckling and pneumatic retinopexy.8
In a recent 10-year retrospective analysis of 258 eyes,7 successful initial attachment was achieved in 66% of eyes. Of failed cases, 77% were attached with 1 more operation, and final anatomic success was achieved in 99.2% cases.
CONCLUSIONSAt current levels of scleral buckling usage, as future
generations of retinal surgeons are trained, their ability to perform buckling procedures will not be equal to that of previous generations. Surgical experience itself has been shown to have a significant effect on the suc-cess of RD repair surgery, regardless of the technique in question.6 Lack of experience with scleral buckling among young ophthalmologists may result in worse anatomic and visual outcomes than are now found in the published literature.
In their article arguing “pro” for scleral buckling sur-gery, Drs. Shah and Ahmad acknowledge that today’s fellows are not learning scleral buckling techniques. That is 1 of the reasons why scleral buckling will not continue to be an important surgical skill.
For all the reasons I have pointed out, scleral buckling is not an important mainstay procedure in 2014. It has largely been replaced by PPV and pneumatic retino-pexy. Future generations of retina surgeons will con-tinue the trend toward higher and higher technology for repair of RD, and that will not include the routine use of scleral buckles. n
Szilárd Kiss, MD, is an Associate Professor of Ophthalmology and Director of Clinical Research at Weill Cornell Medical College and an Associate Attending Physician at the New York Presbyterian Hospital. He is on the Retina Today Editorial Board. Dr. Kiss states that he has no financial relationships to disclose. He may be reached at [email protected].
1. American Society of Retina Specialists 2013 Preferences and Trends Survey. Access for members only. http://www.asrs.org/asrs-community/pat-survey.2. Schaal S, Sherman MP, Barr CC, Kaplan HJ. Primary retinal detachment repair: comparison of 1-year outcomes of four surgical techniques. Retina. 2011;31(8):1500-1504. 3. Schneider EW, Geraets RL, Johnson MW. Pars plana vitrectomy without adjuvant procedures for repair of primary rhegmatogenous retinal detachment. Retina. 2012;32(2):213-219. 4. Schwartz SG, Flynn HW. Primary retinal detachment: scleral buckle or pars plana vitrectomy? Curr Opin Ophthalmol. 2006;17(3):245-250.5. Heimann H, Bartz-Schmidt KU, Bornfeld N, et al; Scleral Buckling versus Primary Vitrectomy in Rhegmatogenous Retinal Detachment Study Group. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detach-ment: a prospective randomized multicenter clinical study. Ophthalmology. 2007;114(12):2142-2154.6. Mazinani BA, Rajendram A, Walter P, Roessler GF. Does surgical experience have an effect on the success of retinal detachment surgery? Retina. 2012;32(1):32-37. 7. Han DP, Mohsin NC, Guse CE, Hartz A, Tarkanian CN. Comparison of pneumatic retinopexy and scleral buckling in the management of primary rhegmatogenous retinal detachment. Southern Wisconsin Pneumatic Retinopexy Study Group. Am J Ophthalmol. 1998;126(5):658-668.8. Fabian ID, Kinori M, Efrati M, et al. Pneumatic retinopexy for the repair of primary rhegmatogenous retinal detachment: a 10-year retrospective analysis. JAMA Ophthalmol. 2013;131(2):166-171. detachment surgery? Retina. 2012;32(1):32-37.
https://www.surveymonkey.com/s/RT20
Weigh in on this topic noW!
1. Were you trained scleral buckling in your retina fellowship program?
Yes No
2. What is your approach to retina detachment surgery?
Pars plana vitrectomy (PPV) alone Scleral buckling alone PPV with scleral buckling
2. Do you think that as PPV instrumentation gets smaller scleral buckling will be phased out com-pletely?
Yes No