Embed Size (px)
Citation preview

Lisa G. Winston, MD
University of California, San Francisco/ Zuckerberg San Francisco General
Disclosures I have nothing to disclose

Community‐Acquired Pneumonia (CAP) ‐ Outline
Epidemiology
Diagnosis
Microbiology
Risk stratification
Treatment
Prevention
Community‐Acquired Pneumonia Guidelines
Diagnosis and treatment of adults with community‐acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America
Update of 2007 guidelines
Different format and approach but few changes in management
Am J Respir Crit Care Med 2019 Oct 1;200:e45

Epidemiology: Acute Lower Respiratory Tract Infections
In U.S., influenza and pneumonia 8th most common cause of death per the Centers for Disease Control and Prevention (moved up from 9th in 2010)
55,672 deaths in 2017
Most common cause of death from infectious disease
Among those 85 and older, at least 1 in 20 hospitalized each year

Epidemiology: Acute Lower Respiratory Tract Infections
Inpatient mortality rate: may be influenced by coding
From 2003 – 2009, mortality rate for principal diagnosis pneumonia decreased from 5.8% to 4.2%
More patients coded with principal diagnosis sepsis or respiratory failure and secondary diagnosis pneumonia
Using all codes, little change in mortality rate
Lindenauer et al, JAMA 2012;307:1405‐13
Outpatient mortality < 1%; about 80% of CAP treated in outpatient setting
Diagnosis Chest radiograph – needed in all cases?
Avoid over‐treatment with antibiotics
Differentiate from other conditions
Specific etiology, e.g. tuberculosis
Co‐existing conditions, such as lung mass or pleural effusion
Evaluate severity, e.g. multilobar
Unfortunately, chest physical exam not sensitive or specific and significant variation between observers
Arch Intern Med 1999;159:1082-7

Microbiological Investigation
Sputum Gram stain and culture 30‐40% patients cannot produce adequate sample
Most helpful if single organism in large numbers
Culture (if adequate specimen): antibiotic sensitivities
Limited utility after antibiotics for most common organisms
Usually unnecessary in outpatients – 2019 guideline recommends against
May be most helpful in severe CAP and/or when treatment for MRSA or P. aeruginosa is considered
Severe Pneumonia
Am J Respir Crit Care Med 2019 Oct 1;200:e45

Obtain blood cultures?
Not recommended in outpatients
Obtain prior to antibiotics
Positive in 5 – 14% of hospitalized patients
Obtain with severe disease ‐most important predictor
2019 guidelines also recommend when empirically treating for MRSA or P. aeruginosa
Legionella and Pneumococcal Urinary Antigen Testing?
Evaluation for Legionella Urinary antigen test for L. pneumophila serogroup 1 (70‐90%)
Can also culture with selective media
Probably most helpful in severe disease or with epidemiologic risk (e.g., recent travel, suspected outbreak)
Pneumococcal urinary antigen test Simple, takes about 15 minutes
In adults, sensitivity 50‐80%, specificity ~90%
Consider in severe CAP

Other Microbiological Investigation?
Influenza testing
Treatment likely provides benefit for many
Test when influenza is circulating in the community
Multiplex PCR systems for respiratory pathogens
Benefit uncertain
Procalcitonin?
Procalcitonin is produced in response to endotoxin and endogenous mediators released in the setting of bacterial infections
Rises in bacterial infections much more than, e.g., viral infections or inflammatory states
Rises and falls quickly
Procalcitonin‐guided treatment in acute respiratory infections may decrease antibiotic exposure and might improve outcomes, particularly in the ICU
Decreased antibiotic exposure was not seen in large ED RCT
Not recommended to guide decision to start antibiotics
New Engl J Med 2018;379:236-249Lancet Infect Dis 2018;18:95-107

Etiology – historical data Clinical syndrome and CXR not reliably predictive
Streptococcus pneumoniae 20‐60%
Haemophilus influenzae 3‐10%
Mycoplasma pneumoniae up to 10%
Chlamydophila pneumoniae up to 10%
Legionella up to 10%
Enteric Gram negative rods up to 10%
Staphylococcus aureus up to 10%
Viruses up to 10%
No etiologic agent 20‐70%
CAP Surveillance Study Adults hospitalized with CAP at 5 hospitals in Chicago and Nashville
Extensive diagnostic testing done via culture, serology, antigen testing, and molecular diagnostics
A pathogen was detected in only 38% of patients with specimens available Viruses 62%
Bacteria 29%
Bacteria and virus 7%
Fungus or mycobacteria 2%
NEJM 2015;373:415-27

Typical vs. AtypicalTypical
Visible on Gram stain, grows in routine culture
Susceptible to beta lactams
S. pneumoniae, H. influenzae
Atypical Not visible on Gram stain, special culture techniques
Not treated with beta lactams
M. pneumoniae, C. pneumoniae, Legionella
X X
S. pneumoniaeRisk factors
Extremes of ageAlcoholismCOPD and/or smokingNursing home residence
InfluenzaInjection drug useAirway obstructionHIV infection

Legionella Think about with severe disease, high fever, hyponatremia, markedly elevated LDH, CNS abnormalities
Fluoroquinolone or azithromycin drug of choice; usual rx 14‐21 days
Risk factors:
Older ageSmokingImmune compromise,
cell mediatedTravel
Renal diseaseLiver diseaseDiabetesMalignancy
Mycoplasma pnuemoniae Common cause respiratory infections in children/young adults
Pneumonia relatively uncommon
Epidemics in close quarters
May have sore throat, nausea, vomiting, hemolytic anemia, rash
Treatment with doxycycline, macrolide, or fluoroquinolone
Rising rate of macrolide resistance – U.S. 8.2%; China 90%
Pediatr Infect Dis J 2012;31:409-11

• Outpatient vs. inpatient?• Cost• Patient satisfaction• Safety
Risk Stratification
Risk Stratification – Pneumonia Severity Index
Outpatient vs. inpatient? Pneumonia Patient Outcomes Research Team (PORT) study (Fine et al, NEJM 1997;336:243‐250) Prediction rule to identify low risk patients with CAP
Stratify into one of 5 classes Class I: age < 50, none of 5 co‐morbid conditions, apx. normal VS, normal mental status
Class II‐V: assigned via a point system

Risk Stratification – Pneumonia Severity Index
Mortality < 1% for classes I, II
Low risk patients hospitalized more than necessary
Caveats:
Does not take into account social factors
Pneumonia Severity Index Calculator
https://www.mdcalc.com/psi-port-score-pneumonia-severity-index-cap
Age and sex; resident of nursing home {yes/no}
Comorbid diseases {yes/no}: renal disease, liver disease,CHF, cerebrovascular disease, neoplasia
Physical exam {yes/no}: altered mental status, SBP < 90,temp < 35 or >=40, RR>=30, HR>=125
Labs/studies {yes/no}: pH<7.35, PO2<60 or Sat<90, Na<130, HCT<30, gluc>250, BUN>30, pleural eff

Patient #1
60 year‐old man with diabetes presents with fever and dyspnea. Positive PORT items include HR=130, Na=129, glucose=300.
Should this patient be hospitalized?
Please vote: 1. Yes
2. No
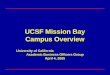
Pneumonia Severity Index Results
Risk Class Score MortalityLow I < 51 0.1%Low II 51 - 70 0.6%Low III 71 - 90 0.9%Medium IV 90 - 130 9.5%High V > 130 26.7%
Hospitalization is recommended for class IV and V. Class III should be based on clinical judgment.
Class: IVScore: 100

Patient #2
55 year-old woman with no other risk factors?Hospitalization? Please vote:
1. Yes2. No
Class : IIScore : 45Mortality : 0.1%
Patient #392 year-old man with no other risk factors?Hospitalization? Please vote:
1. Yes2. No
Class : IVScore : 92Mortality : 9.5%

Patient #4
20 year-old woman with SBP < 90 and a pleural effusion?
Hospitalization? Please vote:1. Yes2. No
Class : IIScore : 40Mortality : 0.6%
Other Scoring Systems
CURB‐65 (British Thoracic Society)
Has only 5 variables, compared with 20 for Pneumonia Severity Index

Is coverage of “atypical” organisms important?
In Europe, amoxicillin commonly used as a single drug with data supporting a short course (3 days in responding patients)
Some studies show no benefit of empirical atypical coverage on survival or clinical efficacy in hospitalized patients
el Moussaoui et al, BMJ 2006;332:1355 - 62
Shefet et al, Arch Intern Med 2005;165:1992-2000
JAMA 2014;311(21):2199-2208
• V.A. retrospective, cohort study of patients 65 and older hospitalized with pneumonia 2002-2012
• 31,863 patients treated with azithromycin compared with 31,863 propensity matched patients with no exposure
• 90 day mortality significantly lower 17.4% vs. 22.3%, O.R. 0.73 • Myocardial infarct significantly higher 5.1% vs. 4.4%, O.R. 1.17

NEJM 2015;372:1312-23
• Cluster-randomized trial in 7 hospitals in the Netherlands with rotating strategies• Adults with CAP not requiring ICU• Beta-lactam alone (656 patients) vs. beta-lactam plus macrolide (739 patients)
vs. fluoroquinolone alone (888 patients)• Primary outcome 90-day mortality: beta-lactam monotherapy non-inferior to
other strategies• No difference in length of stay or complications
JAMA 2016;315:593-602
• Two RCTs evaluated beta-lactam + macrolide combination therapy vs. beta-lactam monotherapy – includes study prior slide• One failed to demonstrate non-inferiority of monotherapy
• 6 of 8 observational studies favored beta-lactam + macrolidecombination therapy vs. beta-lactam monotherapy
• 3 of 3 observational studies favored fluoroquinolone monotherapyover beta-lactam monotherapy
*Based on these data, 2019 guidelines do not recommend beta-lactammonotherapy for inpatients

Antibiotic Treatment: Outpatient
Without co‐morbidities or risk factors for resistant organisms
Amoxicillin 1 g three times daily
Doxycycline 100 mg twice daily
Azithromycin or clarithromycin, if pneumococcal resistance < 25%
With co‐morbidities or risk factors for resistant organisms Amoxicillin/clavulanate or cephalosporin (cefuroxime or cefpodoxime) plus a macrolide or doxycycline
Respiratory fluoroquinolone: moxifloxacin, gemifloxacin, or levofloxacin (750 mg daily)
Antibiotic Treatment: Outpatient
Data to guide antibiotic selection are limited
Available studies suggest good outcomes with few differences
Co‐morbidities include heart, lung, liver, renal disease; diabetes, alcohol use disorder, malignancy, asplenia
Risk factors for resistance include previous MRSA or P. aeruginosa from respiratory culture or recent hospitalization with parenteral antibiotics (in last 90 days)
Lefamulin and omadacycline not added due to cost, tolerability, and less experience
Editorial comment: Not clear why combination therapy does not include amoxicillin as a beta‐lactam option

Antibiotic Treatment: Inpatient, Nonsevere
Standard • Beta-lactam (ampicillin/sulbactam, cefotaxime, ceftriaxone, or ceftaroline) + macrolide OR
• Respiratory fluoroquinolone
Prior respiratory isolation MRSA
Add MRSA coverage and obtain respiratory cultures and/or nasal PCR to allow for de-escalation or continuation
Prior respiratory isolation P. aeruginosa
Add P. aeruginosa coverage and obtain respiratory cultures to allow for de-escalation or continuation
Recent hosp with IV abx and local risk factors MRSA
Obtain respiratory cultures and/or nasal PCR; add coverage if positive
Recent hosp withIV abx and local risk factors P. aeruginosa
Obtain respiratory cultures; add coverage if positive
Antibiotic Treatment: Inpatient, Nonsevere
Guidance beyond standard regimen intended to help with circumstances previously covered by healthcare‐associated pneumonia (HCAP) guidelines
More circumspect / influenced by antimicrobial stewardship
Doxycycline, instead of a macrolide, included as a conditional recommendation in combination with a beta‐lactam
Limited data
No need for specific anaerobic coverage with suspected aspiration pneumonia

Outside the ICU…we love doxycycline Adult inpatients June 2005 – December 2010
Compared those who received ceftriaxone + doxycycline to those who received ceftriaxone alone
2734 hospitalizations: 1668 no doxy, 1066 with doxy
Outcome: CDI within 30 days of doxycycline receipt
CDI incidence 8.11 / 10,000 patient days in those receiving ceftriaxone alone; 1.67 / 10,000 patient days in those who received ceftriaxone and doxycycline
Doernberg et al, Clin Infect Dis 2012;55:615-20
Antibiotic Treatment Inpatient, SevereStandard • Beta-lactam (ampicillin/sulbactam, cefotaxime, ceftriaxone, or
ceftaroline) + macrolide OR• Beta-lactam + respiratory fluoroquinolone
Prior respiratory isolation MRSA
Add MRSA coverage and obtain respiratory cultures and/or nasal PCR to allow for de-escalation or continuation
Prior respiratory isolation P. aeruginosa
Add P. aeruginosa coverage and obtain respiratory cultures to allow for de-escalation or continuation
Recent hosp with IV abx and local risk factors MRSA
Add MRSA coverage and obtain respiratory cultures and/or nasal PCR to allow for de-escalation or continuation
Recent hosp withIV abx and local risk factors P. aeruginosa
Add P. aeruginosa coverage and obtain respiratory cultures to allow for de-escalation or continuation

What about steroids?
Lancet 2015: http://dx.doi.org/10.1016/S0140-6736(14)62447-8
• Randomized, double blind trial in Switzerland• 785 adult inpatients received 50 mg prednisone daily x 7 days or placebo• Primary outcome clinical stability: 3.0 days prednisone vs. 4.4 days placebo,
p<.0001• Time to hospital discharge 6 days prednisone vs. 7 days placebo, p=.01• No difference complications except slightly higher in-hospital hyperglycemia
with prednisone
Questions re study 2911 patients assessed to randomize 802
Why was length of stay so long?
4% prednisone and 6% placebo admitted to ICU
Death from any cause 4% prednisone and 3% placebo

What about steroids?
Multicenter, double‐blind, RCT at 3 hospitals in Spain
Adults with severe CAP (75% in ICU)
Methylprednisolone 0.5 mg/kg q 12h x 5 days (n=61) vs. placebo (n=59)
Recruited 2004 – 2012
Primary outcome: treatment failure (composite) 13% vs. 31%, P=.02
Mortality 10% vs. 15%, P=.37
JAMA 2015;313(7):677-86
What about steroids?
Systematic review and meta‐analysis of steroids for patients hospitalized with CAP
Included 13 RCTs with 2005 patients total
Both studies on previous slides included
Outcomes:
Possible 2.8% reduction in mortality
5% reduction mechanical ventilation
1 day decrease hospital stay
3.5% increase in hyperglycemia requiring treatment
Ann Intern Med 2015;163(7):519-28

What about steroids? At least 2 multicenter trials with data anticipated
ESCAPe: patients with severe CAP, VA hospitals, methylprednisolone
Study completed; results not yet reported
CAPE_COD: patients with severe CAP, French hospitals, hydrocortisone
Recruitment in progress
Guidelines do not recommend steroids
Can be considered with refractory septic shock
https://clinicaltrials.gov/
Length of Therapy
7 – 10 days had been standard but probably not necessary
Convincing data for 5‐day course with azithromycin or high dose levofloxacin
Meta‐analysis: patients with mild to moderate disease can be treated with 7 days or less
Guidelines suggest 5 days appropriate for most patients
Am J Med. 2007;120(9):783-90

Switch to Oral Therapy Reduces costs, shortens length of stay, may reduce complications
As soon as improving clinically, able to take POs, GI tract functioning Usually within 3 days; no need to observe in hospital
Empirical therapy: macrolide, doxycycline, respiratory fluoroquinolone, or combination therapy
Amoxicillin if susceptible organism, usually S. pneumoniae, identified
Prevention
There are stepspatients and providerscan take….

Prevention
Vaccination Influenza vaccine
Pneumococcal vaccines
Smoking cessation Smoking, with or without COPD, is a significant risk factor
But, what happened to healthcare‐associated pneumonia (HCAP)?

Am J Respir Crit Care Med 2005;171:388-416
The concept of HCAP has been removed – why?• Increasing evidence that most patients with HCAP are not at
high risk for resistant pathogens• Other features besides exposure to the healthcare system
may be important• May be covered by new CAP guidelines However, concept of HCAP as an entity not maintained

Practical tips for HCAP
Most patients with “HCAP” can be treated like CAP
Consider expanded initial therapy if
Severely ill
History of resistant organism or other risk factors such as extensive antibiotic exposure
Knowledge of local flora/resistance patterns is helpful
If using expanded therapy, prioritize microbiologic diagnosis
De‐escalate based on results
2016 guidelines: take home points for both HAP and VAP
Perform microbiologic testing – preferred over empirical therapy
Obtain non‐invasively – expectorated, induced sputum, endotracheal aspirate
BAL, mini‐BAL, protected‐brush specimens not recommended
Not recommended for decision to initiate therapy
Procalcitonin
C‐reactive protein
Clinical Pulmonary Infection Score (CPIS)
Most patients should be treated for 7 days

2016 guidelines: initial treatment of HAP (based on very low quality evidence) Use local pathogen and antibiotic resistance data
Cover MRSA in selected patient
Prior IV antibiotics within 90 days
> 20 of S. aureus isolates on unit are MRSA
High risk of mortality
Cover Pseudomonas aeruginosa
Double coverage of P. aeruginosa with risk factors
Prior IV antibiotics within 90 days
High risk for mortality
2016 guidelines: initial treatment of HAP (based on very low quality evidence)
Not at high risk of mortality and no risk factors increasing likelihood of MRSA (cover MSSA and P. aeruginosa)
One of the following:
Piperacillin‐tazobactam 4.5 g IV q 6h
Cefepime 2 g IV q 8h
Levofloxacin 750 mg IV daily
Imipenem 500 mg IV q 6h
Meropenem 1 g IV q 8h

2016 guidelines: initial treatment of HAP (based on very low quality evidence) Not at high risk of mortality but increased risk of MRSA:
Piperacillin‐tazobactam 4.5 g IV q 6h
Cefepime 2 g IV q 8h
Levofloxacin 750 mg IV daily
Imipenem 500 mg IV q 6h
Meropenem 1 g IV q 8h
Aztreonam 2 g IV q 8h
PLUS
Vancomycin 15 mg/kg IV q 8h‐12h (goal trough 15 – 20) OR
Linezolid 600 mg IV q 12h
2016 guidelines: initial treatment of HAP (based on very low quality evidence)
High risk of mortality or IV antibiotics with 90 days:
Antipsuedomonal beta lactam: piperacillin‐tazobactam, cefepime, ceftazidime, aztreonam, imipenem, meropenem
PLUS
A second antipseudomonal antibiotic: levofloxacin, ciprofloxacin, amikacin, gentamicin, tobramycin
PLUS
Vancomycin or linezolid

2016 guidelines: initial treatment of VAP
Use local pathogen and antibiotic resistance data
Do not treat ventilator‐associated tracheobronchitis with antibiotics
2016 guidelines: initial treatment of VAP (based on very low quality evidence) Cover S. aureus, P. aeruginosa, and other Gram‐negative bacilli in all empirical regimens
Cover MRSA with vancomycin or linezolid when > 10 – 20% of S. aureus isolates in unit are MRSA
Use two antipseudomonal antibiotics if
• Prior IV antibiotic use within 90 days• Septic shock• ARDS preceding VAP• 5 or more days of hospitalization preceding VAP
• > 10% of Gram negative isolates resistant to planned monotherapy
• Susceptibility rates unknown

ZSFG / SF VAMC HAP and VAP antibiotic guideline: initial therapy
Mild HAP: ceftriaxone or ertapenem or levofloxacin
Severe HAP (e.g. high O2 requirement, cavitary disease): vancomycin plus cefepime or piperacillin/tazobactam
VAP, intubated < 5 days without complications (e.g. multifocal or cavitary disease): ceftriaxone or ertapenem or levofloxacin
VAP, intubated > 5 days or complicated: vancomycin plus cefepime or piperacillin/tazobactam