Embed Size (px)
Citation preview

Advances in haemodynamic monitoring in Anaesthesia and ICU
Dr Tuong PhanStaff Specialist Anaesthetist
Dept Anaesthesia and Pain MedicineSt Vincent’s Hospital Melbourne

the technologyBeyond standard monitoringKeys to understanding
Recommendations and summary
utilityAccuracyTrending ability
utilityClinical studies
Min
imal
ly in
vasi
ve c
ardi
ac o
utpu
t m
onito
ring
Min
imal
ly in
vasi
ve c
ardi
ac o
utpu
t m
onito
ring

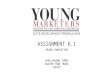
Method Proprietary device Invasive elements Parameters
Oesophageal Doppler
CardioQTM, Deltex Medical Oesoph. Doppler probe
CO, SV, Ftc
CardioQ PLUS OD plus arterial line
CO, SV
Transcutaneous Doppler
Ultrasound CO monitor, USCOMTM
Nil CO, SV
APCO uncalibrated
Vigileo/FloTracTM, Edwards Lifesciences (1)
Arterial line CO, SV, SVV
LiDCO Rapide, LiDCO Ltd Arterial line CO, SV, SVV, PPV
Finepress, Nexfin, Edwards Finger cuff CO, SV, SVV
Arterial Pressure CO calibrated
LiDCO Plus, LiDCO Ltd (2) Arterial line CO, SV, SVV, PPV
PiCCOplusTM, Pulsion Medical Systems
Central Venous catheter and femoral arterial line
CO, SV, ITBV, EVLW
Plethysmography Masimo Rainbow SET Pulse CO, Masimo Corp.
Pulse oximeter dPOPPVI
Min
imal
ly in
vasi
ve c
ardi
ac o
utpu
t m
onito
ring
Min
imal
ly in
vasi
ve c
ardi
ac o
utpu
t m
onito
ring

Method Proprietary device Invasive elements Parameters
Oesophageal Doppler
CardioQTM, Deltex Medical Oesoph. Doppler probe
CO, SV, Ftc
CardioQ PLUS OD plus arterial line
CO, SV
Transcutaneous Doppler
Ultrasound CO monitor, USCOMTM
Nil CO, SV
APCO uncalibrated
Vigileo/FloTracTM, Edwards Lifesciences (1)
Arterial line CO, SV, SVV
LiDCO Rapide, LiDCO Ltd Arterial line CO, SV, SVV, PPV
Finepress, Nexfin, Edwards Finger cuff CO, SV, SVV
Arterial Pressure CO calibrated
LiDCO Plus, LiDCO Ltd (2) Arterial line CO, SV, SVV, PPV
PiCCOplusTM, Pulsion Medical Systems
Central Venous catheter and femoral arterial line
CO, SV, ITBV, EVLW
Plethysmography Masimo Rainbow SET Pulse CO, Masimo Corp.
Pulse oximeter dPOPPVI
Min
imal
ly in
vasi
ve c
ardi
ac o
utpu
t m
onito
ring
Min
imal
ly in
vasi
ve c
ardi
ac o
utpu
t m
onito
ring

V = ∆f c .
2 ft cosθ
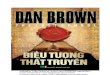
the technology
Oesophageal Doppler Monitor

Stroke Distance
SV = VTI x Area
SV = VTI/0.7 x est desc Aortic area
∆CO ∝ ∆VTI

Afterload Increase Afterload Reduction
Positive InotropyMyocardial Depression
Preload Reduction Preload Increase Predominant Change

Keys to
Oesophageal Doppler Monitor
• ∆CO ∝ ∆VTI– Good diagnostic and trend ability– Uncoupled from pressure entirely
• Continuously available• Learning curve

Method Proprietary device Invasive elements Parameters
Oesophageal Doppler
CardioQTM, Deltex Medical Oesoph. Doppler probe
CO, SV, Ftc
CardioQ PLUS OD plus arterial line
CO, SV
Transcutaneous Doppler
Ultrasound CO monitor, USCOMTM
Nil CO, SV
APCO uncalibrated
Vigileo/FloTracTM, Edwards Lifesciences (1)
Arterial line CO, SV, SVV
LiDCO Rapide, LiDCO Ltd Arterial line CO, SV, SVV, PPV
Finepress, Nexfin, Edwards Finger cuff CO, SV, SVV
Arterial Pressure CO calibrated
LiDCO Plus, LiDCO Ltd (2) Arterial line CO, SV, SVV, PPV
PiCCOplusTM, Pulsion Medical Systems
Central Venous catheter and femoral arterial line
CO, SV, ITBV, EVLW
Plethysmography Masimo Rainbow SET Pulse CO, Masimo Corp.
Pulse oximeter dPOPPVI
Min
imal
ly in
vasi
ve c
ardi
ac o
utpu
t m
onito
ring
Min
imal
ly in
vasi
ve c
ardi
ac o
utpu
t m
onito
ring

CO-from-ABP
• MAP positively but imperfectly correlates with CO– Variable changes in SVR make
MAP unreliable– ABP waveform analysis
assumes other features are less affected by confounders such as Vascular resistance
• MAP is a control in Sun et al

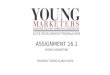
CO-from-ABP
• All 8 methods superior to MAP as directional qualitative indicators of major changes in CO-Thermodilution
• Differ drastically in magnitude. Only one method was superior than MAP when comparing limits of agreement cf CO.
8 different algorithms8 different algorithms
Cardiac Index: 95% limits of agreement l/min
Liljestrand*** -1.76 1.41Corr Impedance -1.91 1.57Pulse Pressure -2.07 1.73Systolic Area -2.07 1.73Sys Area with Kouchoukos corr -2.08 1.71AC power RMS -2.09 1.73Diastolic decay -2.23 1.77MAP -2.20 1.82Herd -2.66 1.89

SPV
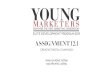
Respiratory coupled parameters
Inspiration- blood squeezed from lung- ↑LV preload ↑systemic BP
↑intrathoracic pressure ↓ RV preload ↓ RV stroke vol

Respiratory coupled parametersPerel, CCM 2009
SPV SVVPPV

© 2011 International Anesthesia Research Society . Published by International Anesthesia Research Society.2
Respiratory Variation in Pulse Pressure and Plethysmographic Waveforms: Intraoperative Applicability in a North American Academic Center.Maguire, Sinead; Rinehart, Joseph; Vakharia, Shermeen; Cannesson, Maxime; MD, PhD
Anesthesia & Analgesia. 112(1):94-96, January 2011.DOI: 10.1213/ANE.0b013e318200366b
Respiratory coupled parameters

the technologyPiCCO injection
t
T
P
t
Transpulmonary thermodilution calibrationPulse contour analysis

the keys
PiCCO
• Requires femoral arterial line• Requires central line• Calibrated• Provides additional
haemodynamic variables• Continuous CO

LiDCOplusTM
Proprietary algorithm - PulseCOTM
the technology

LiDCOrapidTM
Proprietary algorithm - PulseCOTM
Uncalibrated
Cardiac Index
SVV
PPV - Pulse Pressure Variation

the keys to
LiDCO Plus and Rapid
• Fick principle Lithium dilution calibration• Pulse power algorithm
– “Morphology independent”
• Arterial line required but utilises data cable from standard monitoring system. No specific transducer is needed

the technology
Vigeleo Flotrac
• Arterial pulsatility - sd of pressure wave
• K• sex, age, ht and wgt• Waveform characteristics
(skewness and kurtosis)

the technologyVigeleo Flotrac
• Graphic User Interface: • “Drive screen”
• Graphic User Interface: • “Trend screen”

• GUI– Additional
functionality– ScvO2– GEDI and ELWI
the technology
Vigeleo Flotrac

the keys to
Vigeleo Flotrac
• Equipment: arterial line• Flow sensor connected directly to arterial line• Accuracy has been dependent on software
upgrades/version.– Previously struggled with changes in compliance,
low SVR states– version 4 being released.

the technology
Nexfin, aka Finepress • Volume clamp with finger cuff• HRS: heart reference system
– measures and corrects pressure difference btw finger and heart•200Hz sampling rate
• Stroke Volume – 3 element Windkessel model• Up to 12% may have inadequate signal


Fischer M O et al. Br. J. Anaesth. 2012;109:514-521
© The Author [2012]. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: [email protected]
• Nexfin and arterial pressure– MAP
correlates well– SBP
underestimates
– CI has looser agreement
the technology
Finepress

Edwards EV1000
• EV1000– Flotrac– Nexfin– VolumeView– ScVO2
– PAC thermodilution

the technologyMasimo• Pulse oximetry• Plethysmographic
variability index (PVI)– It measures the dynamic
changes in perfusion index (PI) over respiratory cycles and calculated as follows:
– PVI = [(PImax – PImin)/PImax] x 100%.
• ∆POP• COHb• Continuous Hb

utilityAccuracy
• Peyton and Chong– Anesthesiology 2010
• Metaanalysis 4 CO monitor types
• Mean bias, precision, percentage error cf thermodilution
• All 40%• Limitation of BA is the
reference TD

limitations Accuracy
↘
TD vs OD TD vs FT TD vs Li

limitations Accuracy
Lorsomradee, JCVA 2009

Truly Not Fluid Responsive
Accuracy: “functional” vs static, receiver operating curves
Trul
y Fl
uid
Resp
onsi
ve
22%
12%
5%

utilityAccuracy• Marik et al, CCM 2009
Summative ROC area
PPV (n=19)0.94 (0.92-0.96)
SVV 0.84 (n=5) (0.81-0.87)
CVP 0.55GEDI 0.56

Limitations : comparison of SVV
• LiDCO SVV cf FT SVV• Large percentage
error• Different methods of
calculating SV• Not interchangeable

utilityClinical Application
Stroke volume based parameters

utilityClinical Application
Respiratory coupled parameters

Survey of tools for GDT

Oesoph dopplerClinical Application
↘
↘

Oesoph Doppler
(1) Use the Stroke Volume Index (SVI); average over 10 cycles(2) Hypotension can be absolute or relative(3) A large change in the SV, ie. >10%, represents the fluid responsiveness(4) A small change in the SV, ie <10% represents the plateau phase and represents an optimised preload(5) Once an optimised phase is reached, a fluid bolus should be given if the SVI falls >10% * The Doppler values will vary from measurement to measurement. However, a trend over several measurements will be more informative.

Arterial Pressure CO algorithm

“Optimal Fluid therapy”
Opt
imum
Incr
easi
ng
Mor
bidi
ty
HypervolemiaHypovolemia
Min
imal
ly in
vasi
ve c
ardi
ac o
utpu
t m
onito
ring
Min
imal
ly in
vasi
ve c
ardi
ac o
utpu
t m
onito
ring
Editorial “Wet, dry or something else?”
Bellamy, BJA 97 (6), Dec2006

my observations
• Mythen and Hamilton 1995 ICM
• Exanguinate 6 healthy volunteers– BP drops modestly– SV drops markedly

the technologyDoppler, APCO, Plethysmography
recommendations and summaryThey are just monitors. Outcomes will be dependent on how they
are utilised to make decisions
utility: Accuracy and Trending abilityKeep in mind the key parameters, their underlying assumptions and be critical. Nevertheless estimations of stroke volume, respiratory coupled parameters do represent a significant addition to standard monitoring eg. Arterial pressure, urine output, CVP
utility: Clinical studiesDevices can be used to target the delivery of fluids and inotropes
Min
imal
ly in
vasi
ve c
ardi
ac o
utpu
t m
onito
ring
Min
imal
ly in
vasi
ve c
ardi
ac o
utpu
t m
onito
ring