Embed Size (px)
Citation preview
20/06/2017
1
Comorbidities and Aging
Guaraldi Giovanni
20/06/2017
2
Theorem:
HIV modifies the relationship between
age and comorbidities

20/06/2017
3
THE CONTEXT: Number of persons living
with HIV aged ≥50 by region (1995-2013)
The Gap Report. Available at: http://www.unaids.org/sites/default/files/media_asset/UNAIDS_Gap_report_en.pdf.
Accessed February 2015
� There are approximately 4.2 million
persons aged ≥50y living with HIV today.
� More than 2 million of which live in sub-
Saharan Africa.

20/06/2017
4
2000 2005 2010 2014
DrugToxicities
Co-morbidities Multi-morbidities
Frailty
DAY TO DAY MANAGEMENT OF HIV PATIENTS
Disability
2017
Age (years)
ADL-Mobility
Disability
Aging
“Accelerate
d”
65 100
Ph
ysi
cal
Fu
nct
ion
Robust
Frail and pre-frailReversible
DisableADL-MobilityDependence
Aging
“Normal”
Trajectories of physical function in older
subjects
20/06/2017
5
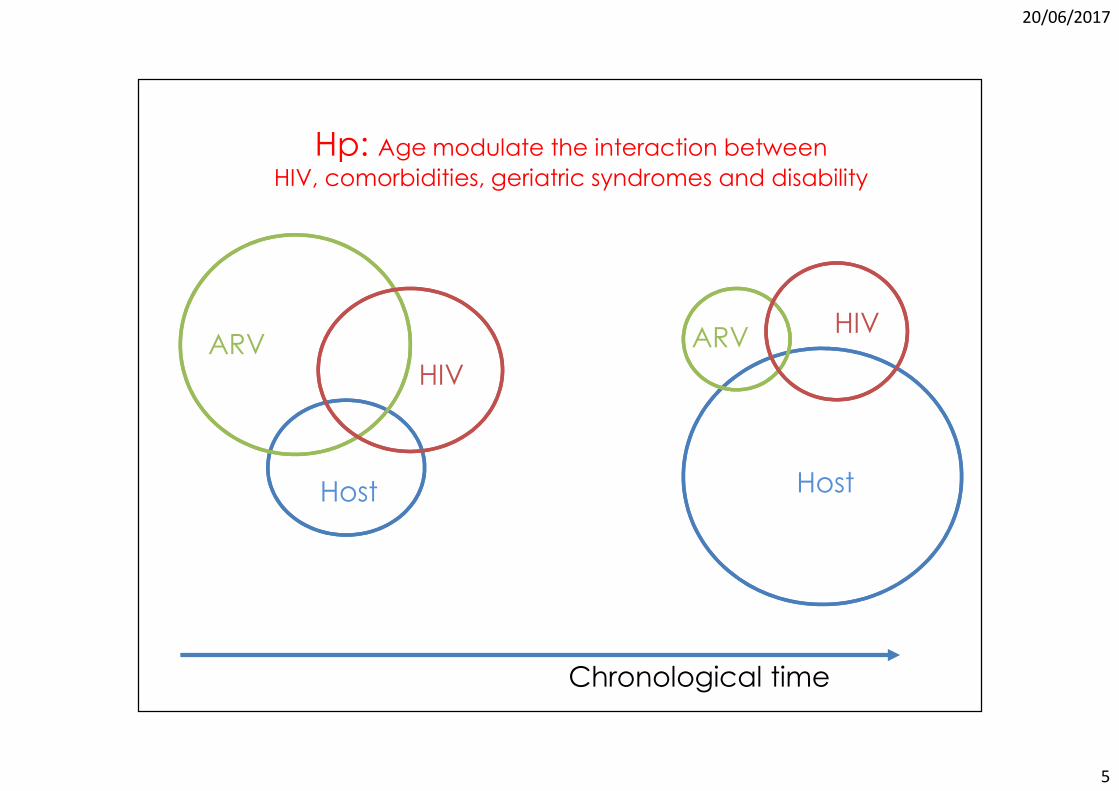
ARVHIV
Host
ARVHIV
Host
Hp: Age modulate the interaction between HIV, comorbidities, geriatric syndromes and disability
Chronological time
20/06/2017
6
Age distribution shift in HIV pts attending MHMC
2016: median age 52.2yrs IQR 48-572003: median age 43.4 yrs IQR 39-46
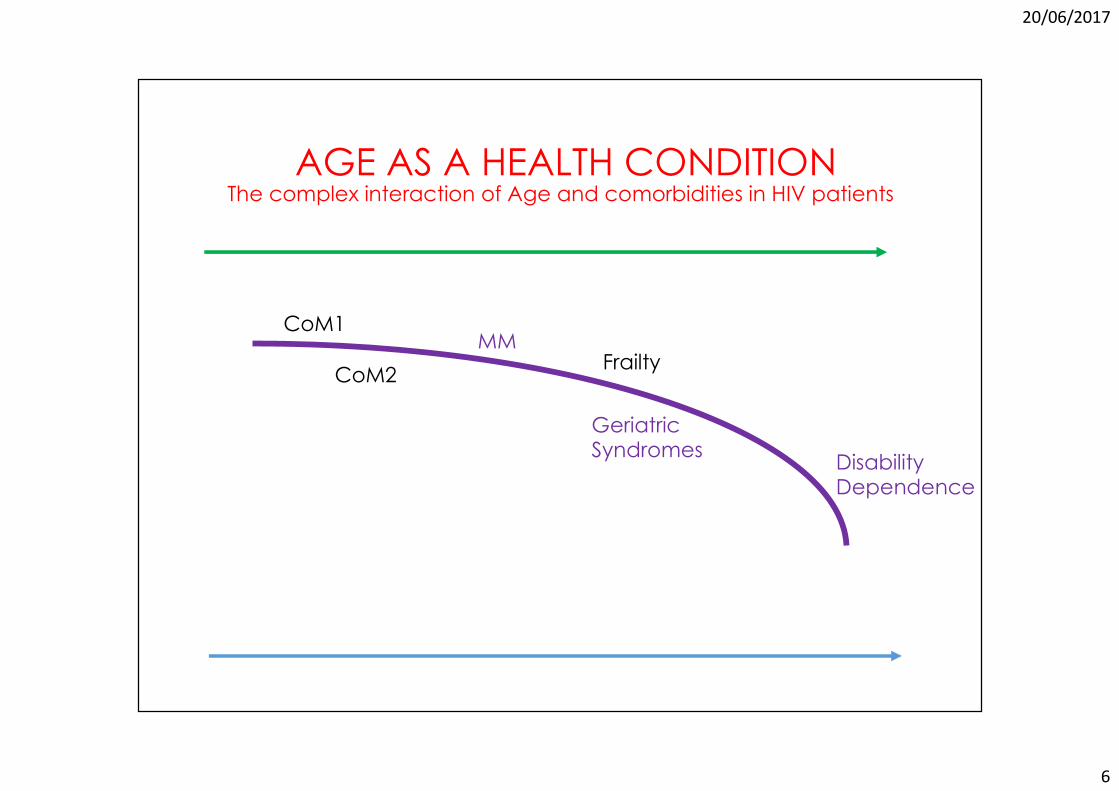
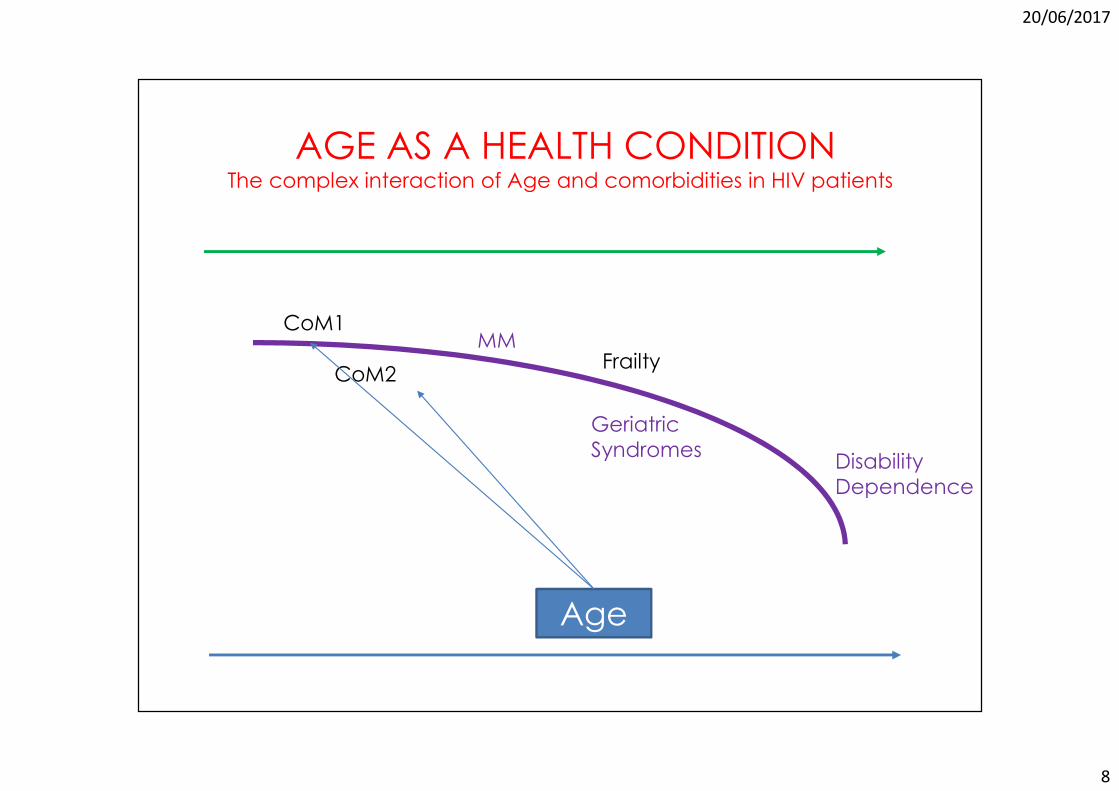
AGE AS A HEALTH CONDITIONThe complex interaction of Age and comorbidities in HIV patients
CoM1
CoM2
MMFrailty
GeriatricSyndromes
DisabilityDependence
20/06/2017
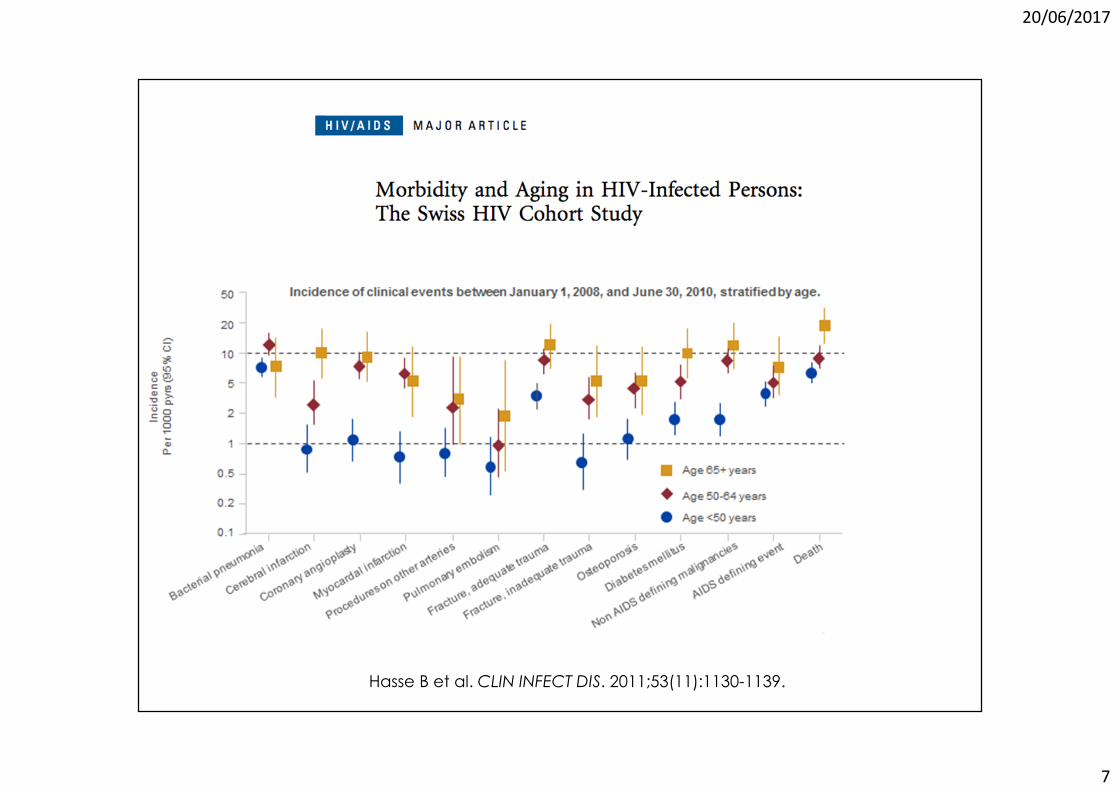
7
Hasse B et al. CLIN INFECT DIS. 2011;53(11):1130-1139.
20/06/2017
8
AGE AS A HEALTH CONDITIONThe complex interaction of Age and comorbidities in HIV patients
Age
CoM1
CoM2
MMFrailty
Geriatric
SyndromesDisability
Dependence

20/06/2017
9
Guaraldi G, CLIN INFECT DIS. 2011;53(11):1120-1126.
20/06/2017
10
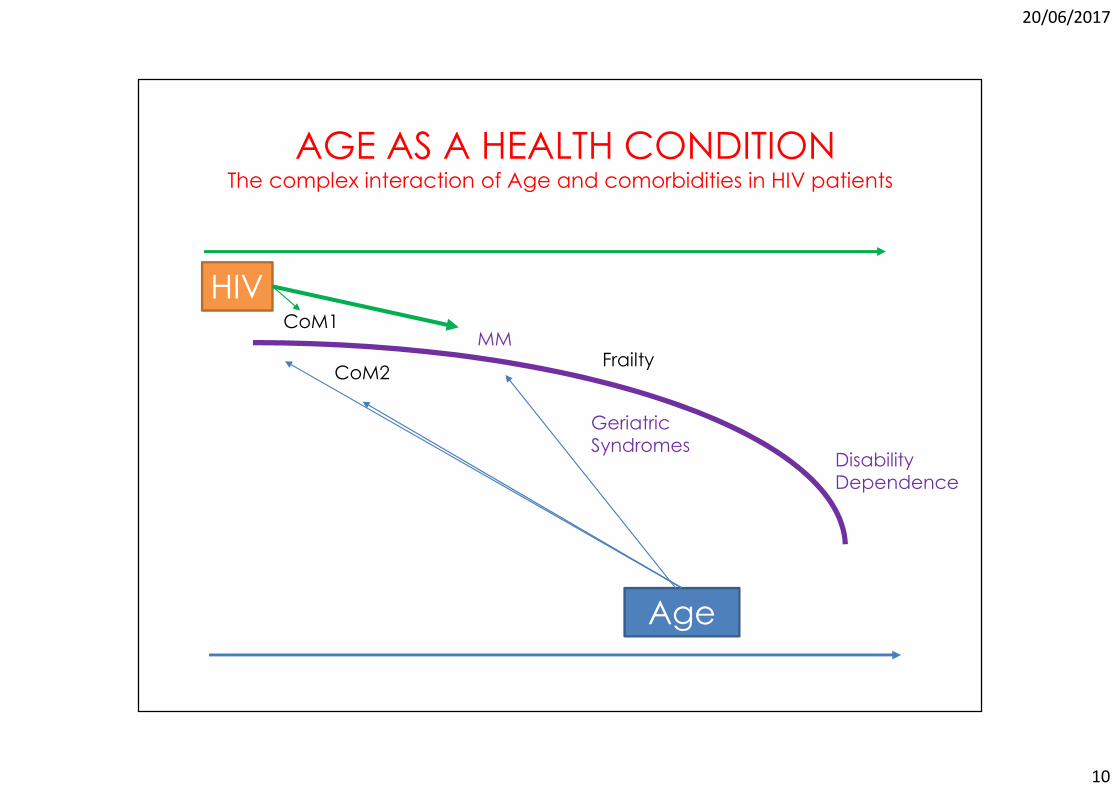
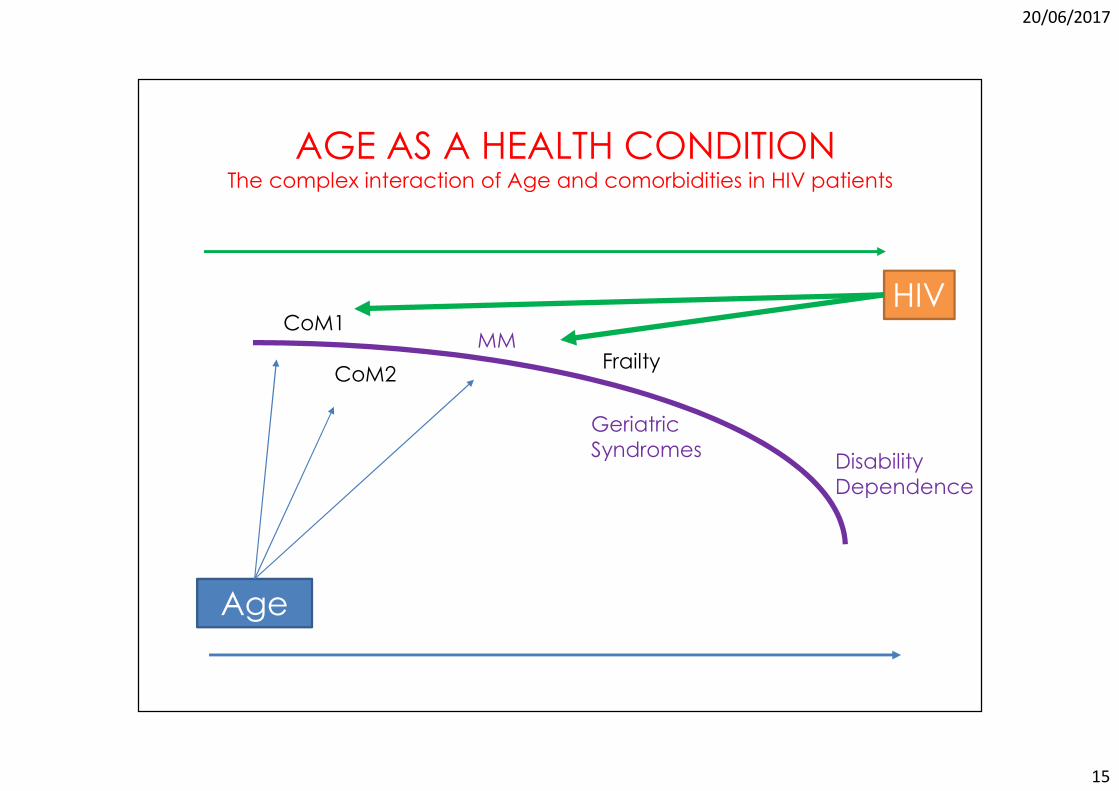
AGE AS A HEALTH CONDITIONThe complex interaction of Age and comorbidities in HIV patients
Age
HIVCoM1
CoM2
MMFrailty
GeriatricSyndromes
DisabilityDependence

20/06/2017
11
Age distribution shift in HIV pts attending MHMC
2016: median age 52.2yrs IQR 48-572003: median age 43.4 yrs IQR 39-46

20/06/2017
12
The pyramid of age in pts attending MHMC is a composite of a diverse population living with HIV since the pre-HAART period or living with HIV since 2006

20/06/2017
13
Guaraldi G, et alPLoS One. 2015 Apr 13;10(4):e0118531
At any age, long-term infected people (ageing patients) had a 5-fold accentuated risk of multimorbidity than HIV-negative controls, while more recently infected people (aged patients) had an intermediate risk compared with the control group
Pro
bab
ility
of
mu
ltim
orb
idit
y 0.6
0.4
0.2
0
20 30 40 50 60 70Age
HIV aged HIV ageing HIV negative
Risk for Multy-
Morbidity
20/06/2017
14
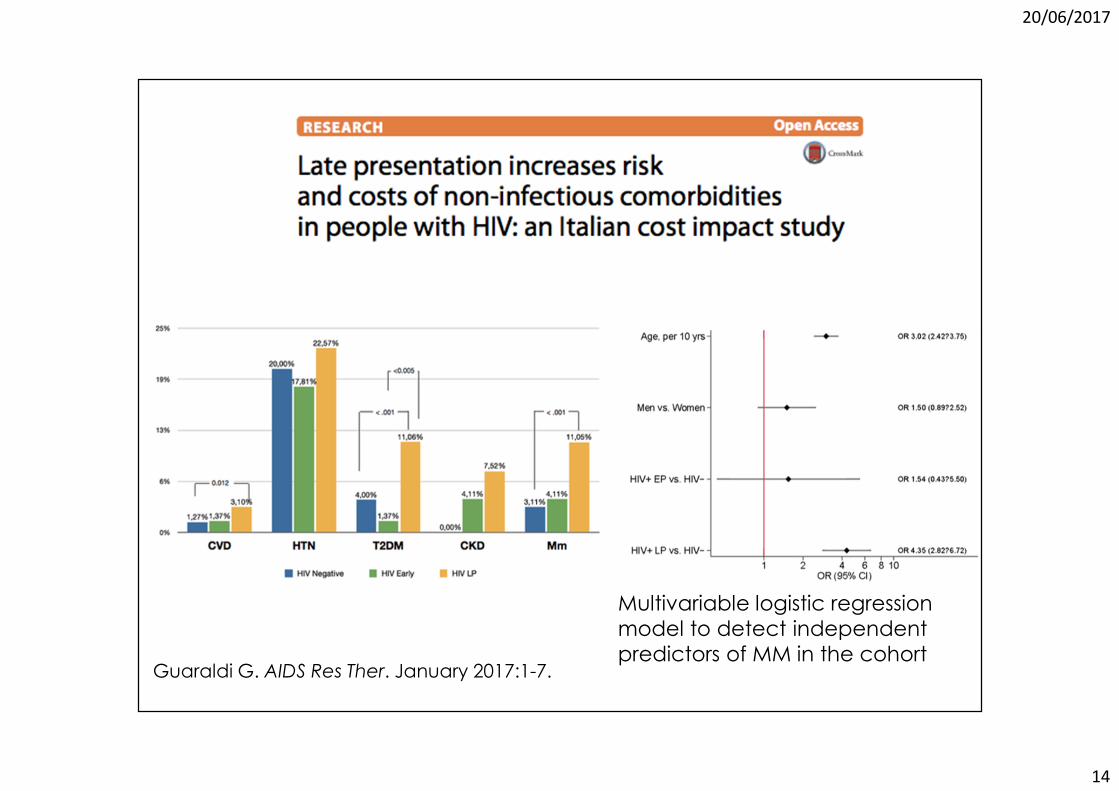
Guaraldi G. AIDS Res Ther. January 2017:1-7.
Multivariable logistic regression
model to detect independent
predictors of MM in the cohort
20/06/2017
15
AGE AS A HEALTH CONDITIONThe complex interaction of Age and comorbidities in HIV patients
Age
HIVCoM1
CoM2
MMFrailty
Geriatric
SyndromesDisability
Dependence
20/06/2017
16
Outline
1. What is unique in the relationship
between age and comorbidities in
people living with HIV (PLWH)?a) One year with HIV impacts on your biological
age more than one chronological year

20/06/2017
17
OBJ: to compare prevalence and risk factors for frailty, sarcopenia,
disability and QoL in HIV patients living with HIV for more than 20 years
(pre-HAART era) or less than 10 years (contemporary HIV care)
GERIATRIC SYNDROMES IN PATIENTS
ENTERING CONTEMPORARY HIV CARE
FRAILTY
Quality of Life
� EuroQol - EQ-5D-5L
Cut off value<100
DISABILITY

20/06/2017
18
Objectiveto compare prevalence and risk factors for frailty,
sarcopenia, disability and QoL in HIV patients living with
HIV for more than 20 years (pre-HAART era) or less than
10 years (contemporary HIV care)
Study Hypothesis
Older HIV patients are at increased risk for aging related complications.
We hypothesized that recent seroconvertors starting contemporary HIV treatments may have a reduced prevalence and risk of aging related outcomes, asncompared to patients living with HIV for more than 20 years
SARCOPENIA AND FRAILTY IN PATIENTS
ENTERING CONTEMPORARY HIV CARE

20/06/2017
19
Materials and methodsWe performed cross-sectional study including consecutive HIV patients having access in 2005-2016 at the Modena HIV Metabolic Clinic
“Contemporary” HIV care model:
� HIV duration: <10 years
� Start ART: >2006
“Old” HIV care model:
� HIV duration: >20 years
� Start ART: <2005
Outcome measuresSARCOPENIA
� Muscle mass (DEXA)
Baumgarten criteria
ASMI <7.26 kg/m2
ASMI <5.45 kg/m2
� Muscle strength
Hand grip assessment below the mean for sex and age
FRAILTY
� Frailty phenotype Fried
criteria >3 out of 5 phenotypic items
� Frailty Index
37-item frailty indexCut off value for frailty >0.38
Disability
� IADL
Cut off value>1
Quality of Life
� EuroQol - EQ-5D-5L
Cut off value<100
20/06/2017
20
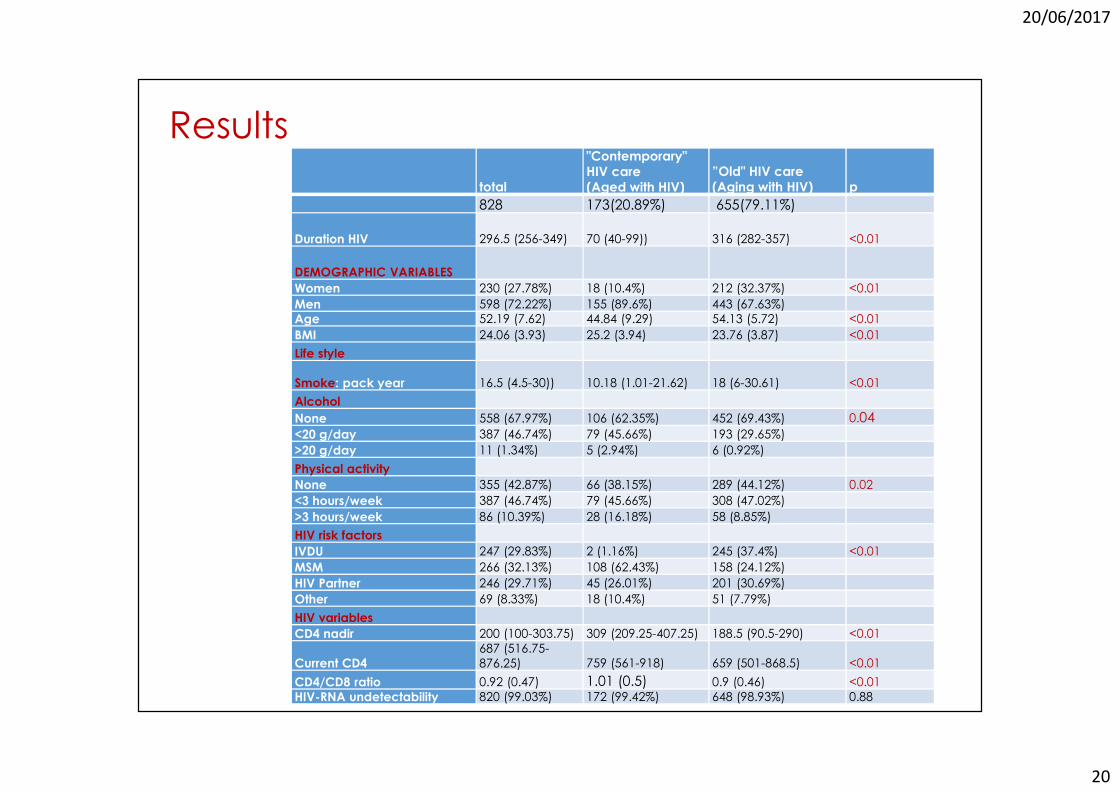
Results
total
"Contemporary" HIV care
(Aged with HIV)
”Old" HIV care
(Aging with HIV) p
828 173(20.89%) 655(79.11%)
Duration HIV 296.5 (256-349) 70 (40-99)) 316 (282-357) <0.01
DEMOGRAPHIC VARIABLES
Women 230 (27.78%) 18 (10.4%) 212 (32.37%) <0.01
Men 598 (72.22%) 155 (89.6%) 443 (67.63%)
Age 52.19 (7.62) 44.84 (9.29) 54.13 (5.72) <0.01
BMI 24.06 (3.93) 25.2 (3.94) 23.76 (3.87) <0.01
Life style
Smoke: pack year 16.5 (4.5-30)) 10.18 (1.01-21.62) 18 (6-30.61) <0.01
Alcohol
None 558 (67.97%) 106 (62.35%) 452 (69.43%) 0.04<20 g/day 387 (46.74%) 79 (45.66%) 193 (29.65%)
>20 g/day 11 (1.34%) 5 (2.94%) 6 (0.92%)
Physical activity
None 355 (42.87%) 66 (38.15%) 289 (44.12%) 0.02
<3 hours/week 387 (46.74%) 79 (45.66%) 308 (47.02%)
>3 hours/week 86 (10.39%) 28 (16.18%) 58 (8.85%)
HIV risk factors
IVDU 247 (29.83%) 2 (1.16%) 245 (37.4%) <0.01
MSM 266 (32.13%) 108 (62.43%) 158 (24.12%)
HIV Partner 246 (29.71%) 45 (26.01%) 201 (30.69%)
Other 69 (8.33%) 18 (10.4%) 51 (7.79%)
HIV variables
CD4 nadir 200 (100-303.75) 309 (209.25-407.25) 188.5 (90.5-290) <0.01
Current CD4
687 (516.75-
876.25) 759 (561-918) 659 (501-868.5) <0.01
CD4/CD8 ratio 0.92 (0.47) 1.01 (0.5) 0.9 (0.46) <0.01
HIV-RNA undetectability 820 (99.03%) 172 (99.42%) 648 (98.93%) 0.88

20/06/2017
21
Results
total
"Contemporary" HIV care
(Aged with HIV)
”Old" HIV care(Aging with
HIV) p828 173(20.89%) 655(79.11%)
Multi-Morbidity 93 (11.23%) 4 (2.31%) 89 (13.59%) <0.01
Frailty
Frailty Index Score 0.29 (0.1) 0.22 (0.08) 0.31 (0.1) <0.01Frailty Index cathegorical (>0.28) 346 (42.04%) 29 (16.86%) 317 (48.69%) <0.01Frailty Phenotype 24 (2.92%) 1 (0.58%) 23 (3.54%) 0.07
SarcopeniaASMI (Sarcopenia cathegorical) 334 (40.34%) 63 (36.42%) 271 (41.37%) 0.27
Hand Grip - mean (Kg), Dominant hand 35.9 (10.09) 38.59 (9) 35.19 (10.25) <0.01Hand Grip - mean (Kg), Non Dominant hand 34.42 (10.19) 37.74 (8.84) 33.55 (10.34) <0.01
Low HG 327 (39.49%) 112 (64.74%) 215 (32.82%) <0.01Geriatric outcomes
Depression (CESD ) 12 (6-21) 10 (5-18) 13 (6-22) 0.04QoL Impairment 523 (75.8%) 105 (70.95%) 418 (77.12%) 0.15
FALLS 72 (12.2%) 12 (13.79%) 60 (11.93%) 0.75IADL impairment 64 (10.22%) 8 (6.61%) 56 (11.09%) 0.2
20/06/2017
22
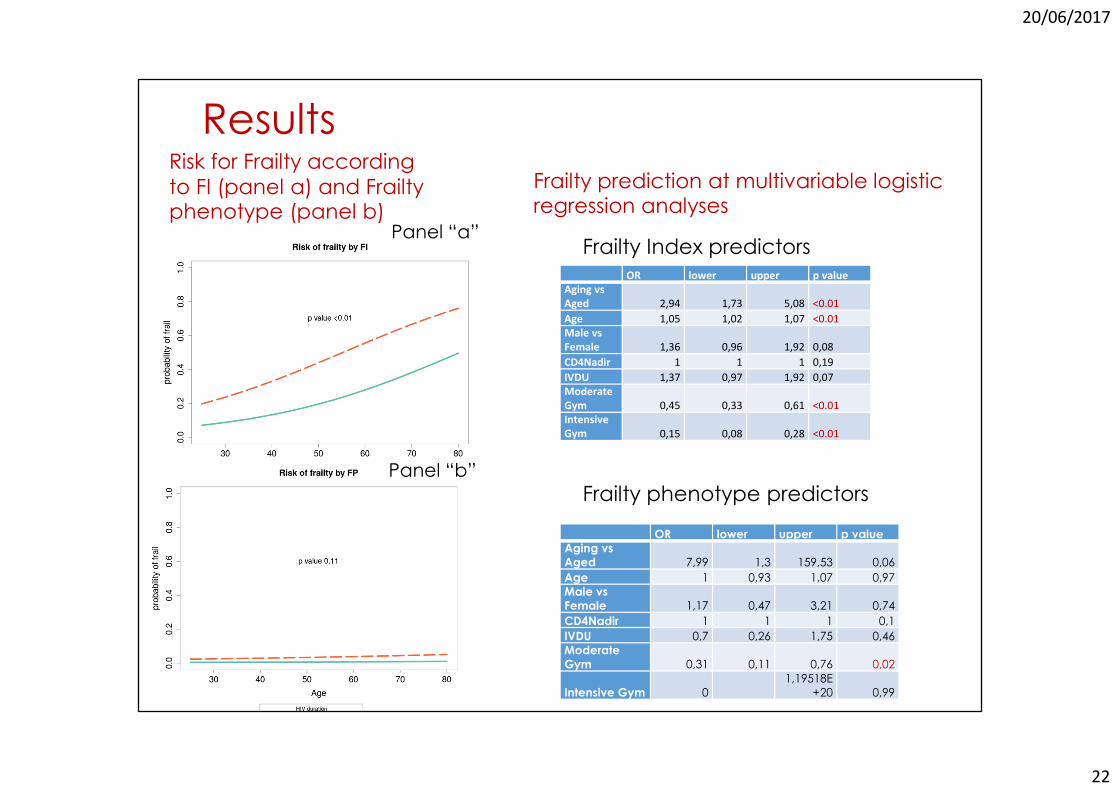
Results
Frailty prediction at multivariable logistic regression analyses
Panel “b”
Panel “a”
Risk for Frailty according
to FI (panel a) and Frailty phenotype (panel b)
OR lower upper p value
Aging vs
Aged 2,94 1,73 5,08 <0.01
Age 1,05 1,02 1,07 <0.01
Male vs
Female 1,36 0,96 1,92 0,08
CD4Nadir 1 1 1 0,19
IVDU 1,37 0,97 1,92 0,07
Moderate
Gym 0,45 0,33 0,61 <0.01
Intensive
Gym 0,15 0,08 0,28 <0.01
OR lower upper p value
Aging vs
Aged 7,99 1,3 159,53 0,06
Age 1 0,93 1,07 0,97
Male vs
Female 1,17 0,47 3,21 0,74
CD4Nadir 1 1 1 0,1
IVDU 0,7 0,26 1,75 0,46
Moderate
Gym 0,31 0,11 0,76 0,02
Intensive Gym 0
1,19518E
+20 0,99
Frailty Index predictors
Frailty phenotype predictors

20/06/2017
23
ResultsRisk for Sarcopenia according to ASMI (panel a) and hand Grip (panel b)
Sarcopenia prediction at
multivariable logistic regression analyses
Panel “b”
Panel “a”
OR lower upper p value
Aging vs
Aged 1,13 0,7 1,81 0,62
Age 1 0,98 1,02 0,84
Male vs
Female 1,77 1,26 2,5 <0.01
CD4Nadir 1 1 1 0,06
IVDU 1,04 0,74 1,45 0,82
Moderate
Gym 0,7 0,52 0,94 0,02
Intensive
Gym 0,29 0,16 0,51 <0.01
OR lower upper p value
Aging vs
aged 0,72 0,44 1,17 0,18
Age 0,91 0,89 0,94 <0.01
Male vs
Female 2,9 1,99 4,27 <0.01
CD4Nadir 1 1 1 0,23
IVDU 0,69 0,48 0,98 0,04
Moderate
Gym 0,82 0,59 1,13 0,23
Intensive
Gym 0,53 0,31 0,91 0,02
Muscle strength predictors
Muscle mqss predictors

20/06/2017
24
Results
Risk for disability in patients entering “old” vs “contemporary” HIV care
Disability was defined for >1 item at IADL assessment
OR lower upper p value
Aging vs Aged 1,23 0,45 3,72 0,7
Age 0,99 0,94 1,04 0,68
Male vs Female 0,15 0,08 0,28 <0.01
CD4Nadir 1 1 1 0,44
IVDU 0,8 0,41 1,49 0,48
Moderate Gym 0,69 0,38 1,23 0,21
Intensive Gym 0,63 0,18 1,78 0,43
Disability predictors

20/06/2017
25
Results
Risk for Impaired QoL in patients entering “old” vs “contemporary” HIV care
QoL impairment was defined for any value <100
OR lower upper p value
Aging vs Aged 0,94 0,52 1,68 0,84
Age 1 0,97 1,03 0,9
Male vs Female 0,81 0,51 1,25 0,34
CD4Nadir 1 1 1 0,28
IVDU 1,63 1,04 2,59 0,04
Moderate Gym 0,59 0,39 0,88 0,01
Intensive Gym 0,23 0,13 0,41 <0,01
QoL predictors

20/06/2017
26
AGE AS A HEALTH CONDITIONThe complex interaction of Age and comorbidities in HIV patients
Age
HIVCoM1
CoM2
MMFrailty
Geriatric
SyndromesDisability
Dependence
HIV

20/06/2017
27
Outline
1. What is unique in the relationship
between age and comorbidities in
people living with HIV (PLWH)?a) One year with HIV impacts on your biological
age more than one chronological year
b) Older people with HIV have similar geriatric
outcomes regardless duration of HIV infection
20/06/2017
28
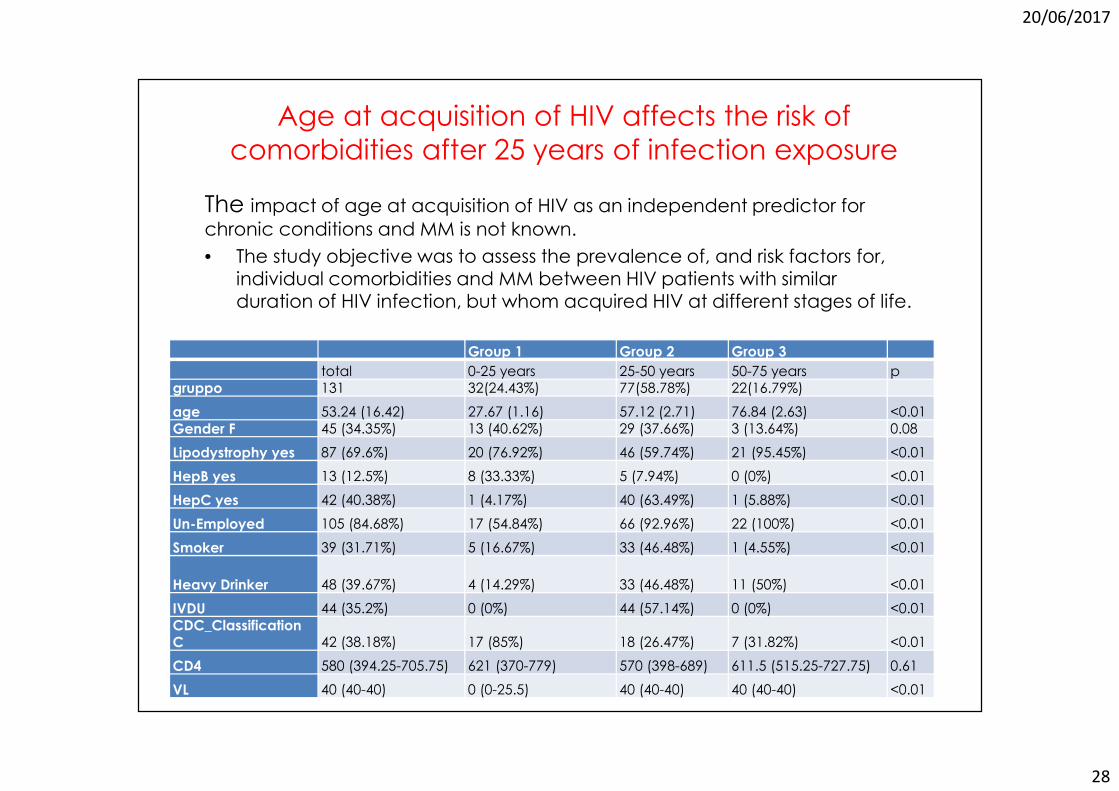
Age at acquisition of HIV affects the risk of
comorbidities after 25 years of infection exposure
The impact of age at acquisition of HIV as an independent predictor for chronic conditions and MM is not known.
• The study objective was to assess the prevalence of, and risk factors for, individual comorbidities and MM between HIV patients with similar duration of HIV infection, but whom acquired HIV at different stages of life.
Group 1 Group 2 Group 3
total 0-25 years 25-50 years 50-75 years p
gruppo 131 32(24.43%) 77(58.78%) 22(16.79%)
age 53.24 (16.42) 27.67 (1.16) 57.12 (2.71) 76.84 (2.63) <0.01
Gender F 45 (34.35%) 13 (40.62%) 29 (37.66%) 3 (13.64%) 0.08
Lipodystrophy yes 87 (69.6%) 20 (76.92%) 46 (59.74%) 21 (95.45%) <0.01
HepB yes 13 (12.5%) 8 (33.33%) 5 (7.94%) 0 (0%) <0.01
HepC yes 42 (40.38%) 1 (4.17%) 40 (63.49%) 1 (5.88%) <0.01
Un-Employed 105 (84.68%) 17 (54.84%) 66 (92.96%) 22 (100%) <0.01
Smoker 39 (31.71%) 5 (16.67%) 33 (46.48%) 1 (4.55%) <0.01
Heavy Drinker 48 (39.67%) 4 (14.29%) 33 (46.48%) 11 (50%) <0.01
IVDU 44 (35.2%) 0 (0%) 44 (57.14%) 0 (0%) <0.01
CDC_Classification C 42 (38.18%) 17 (85%) 18 (26.47%) 7 (31.82%) <0.01
CD4 580 (394.25-705.75) 621 (370-779) 570 (398-689) 611.5 (515.25-727.75) 0.61
VL 40 (40-40) 0 (0-25.5) 40 (40-40) 40 (40-40) <0.01

20/06/2017
29
Age at acquisition of HIV affects the risk of
comorbidities after 25 years of infection
exposure
�=2.09
p=ns
�=1.01
p=ns
�=11.98
p=0.02
�=16.08
p=0.04
Driver is AgeDriver is HIV
Guaraldi G. ICAR 2017

20/06/2017
30
Outline
1. What is unique in the relationship
between age and comorbidities in
people living with HIV (PLWH)?a) One year with HIV impacts on your biological
age more than one chronological year
b) Older people with HIV have similar geriatric
outcomes regardless duration of HIV infection
c) Age of HIV acquisition modulates the impact of
HIV duration on global health

20/06/2017
31
Theorem:
The relationship between age and comorbidities
is UNIQUE, in people living with HIV (PLWH)
CLINICAL IMPLICATION� Patients awareness and education may promote
healthy life styles and successful aging
� Clinical management of aging HIV patients refers to
people with longer HIV exposure, low nadir CD4 or who
acquired HIV at an older age regardless their
chorological age
� These patients must be considered vulnerable to MM, geriatric syndromes and disability
� A multidimensional geriatric-like approach is needed
including proactive switch to less toxic drugs and active
intervention to reduce the risk of polypharmacy
20/06/2017
32
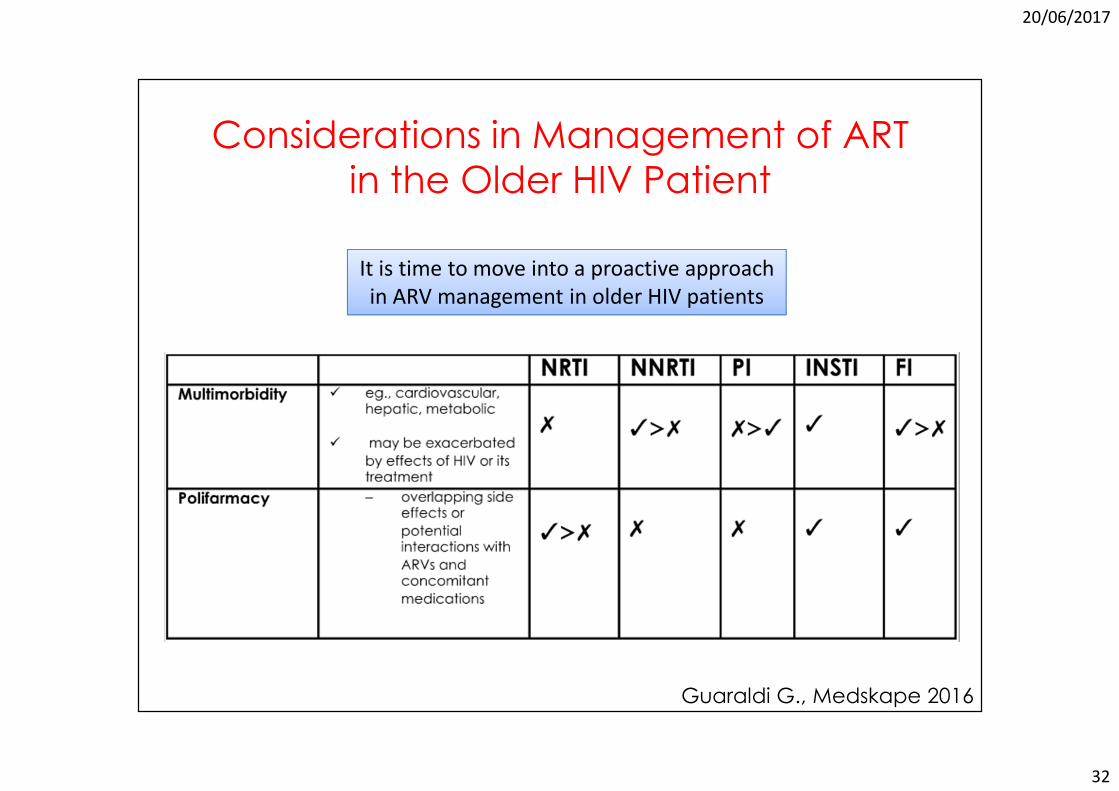
It is time to move into a proactive approach
in ARV management in older HIV patients
Considerations in Management of ART
in the Older HIV Patient
Guaraldi G., Medskape 2016
20/06/2017
33

20/06/2017
34
ARV therapy in geraitric HIV patients
In mono/dual therapy for 384 patients, there were 68
different ARV regimens
In the triple/mega group 839 patients, there were
113 different ARV regimens
High prevalence of non
conventional ARV regimens in elderly HIV pateinbts suggeststhat clinicians try to tailor ARV
regimensaccording to age, HIV duration, MM and PP
20/06/2017
35
GILEAD CONFIDENTIAL. FOR INTERNAL TRAINING USE ONLY. NOT TO BE USED WITH HCPS.
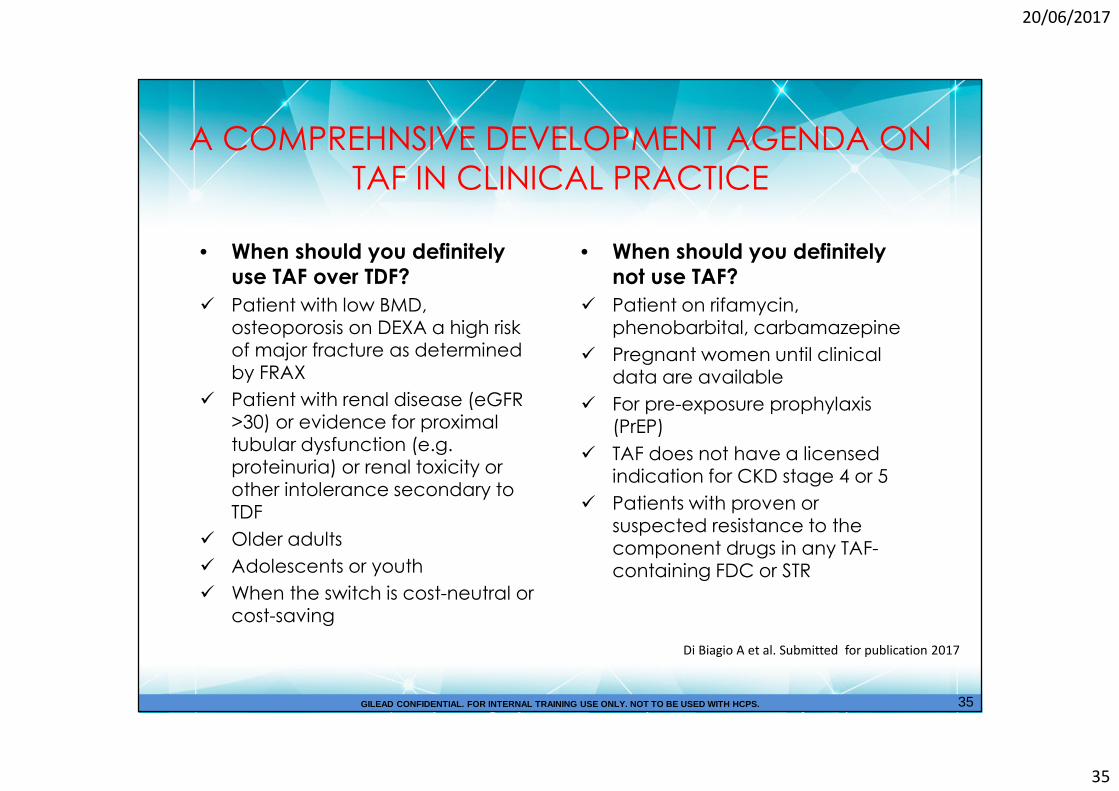
A COMPREHNSIVE DEVELOPMENT AGENDA ON
TAF IN CLINICAL PRACTICE
• When should you definitely use TAF over TDF?
� Patient with low BMD, osteoporosis on DEXA a high risk of major fracture as determined by FRAX
� Patient with renal disease (eGFR>30) or evidence for proximal tubular dysfunction (e.g. proteinuria) or renal toxicity or other intolerance secondary to TDF
� Older adults
� Adolescents or youth
� When the switch is cost-neutral or cost-saving
• When should you definitely not use TAF?
� Patient on rifamycin, phenobarbital, carbamazepine
� Pregnant women until clinical data are available
� For pre-exposure prophylaxis (PrEP)
� TAF does not have a licensed indication for CKD stage 4 or 5
� Patients with proven or suspected resistance to the component drugs in any TAF-containing FDC or STR
35
Di Biagio A et al. Submitted for publication 2017
20/06/2017
36
The role of TAF in the jungle of ARV
prescription
Geriatrics-focused research end points, including frailty,
geriatric syndromes and physical function, will hopefully
be also used to assess the benefit of ARV strategies,
comparing single tablet regimens with less drug
regimens.
This “game changer” in clinical studies will take some
time, while right now a significant reduction in the
jungle of ARV prescriptions is taking place, with clear
benefits for both patients and prescribers.
Conceptual slide - based on Expert Opinion of the presenter
‡










![Silas Martí – Teatro, Oficina, Torre - averyreview.com · [5] Bo Bardi, Teatro Oficina, 6. [6] Bo Bardi, Teatro Oficina, 6. [7] Edson Elito joined the efforts to renovate the Teatro](https://img.pdfslide.us/doc/110x75/5c49c6e593f3c350ba7a0090/silas-marti-teatro-oficina-torre-5-bo-bardi-teatro-oficina-6-6.jpg)


















