Embed Size (px)
DESCRIPTION
UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP, Brazil.
Citation preview
U P D A T I N G N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L
UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 1
Dental Caries in Pediatric Dentistry
1. Concept and risks
a. Conceptual and Epidemiological Aspects
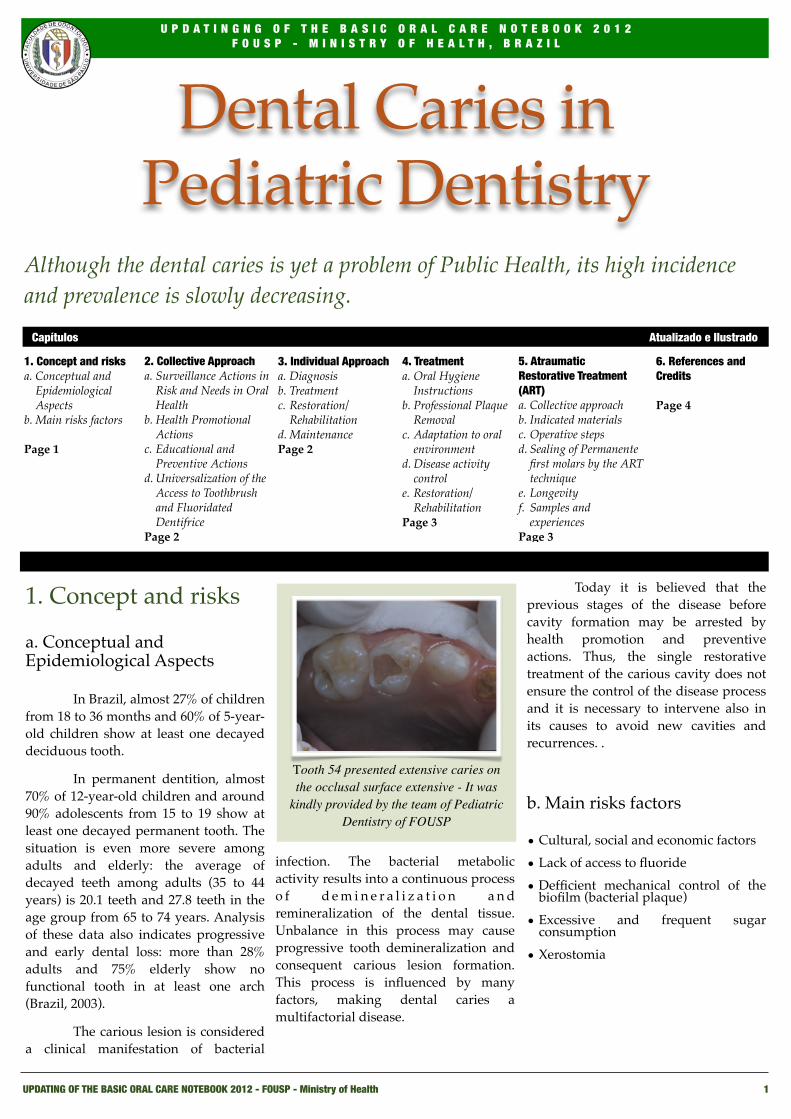
! In Brazil, almost 27% of children from 18 to 36 months and 60% of 5-year-old children show at least one decayed deciduous tooth.
! In permanent dentition, almost 70% of 12-year-old children and around 90% adolescents from 15 to 19 show at least one decayed permanent tooth. The situation is even more severe among adults and elderly: the average of decayed teeth among adults (35 to 44 years) is 20.1 teeth and 27.8 teeth in the age group from 65 to 74 years. Analysis of these data also indicates progressive and early dental loss: more than 28% adults and 75% elderly show no functional tooth in at least one arch (Brazil, 2003).
! The carious lesion is considered a clinical manifestation of bacterial
infection. The bacterial metabolic activity results into a continuous process o f d e m i n e r a l i z a t i o n a n d remineralization of the dental tissue. Unbalance in this process may cause progressive tooth demineralization and consequent carious lesion formation. This process is influenced by many factors, making dental caries a multifactorial disease.
! Today it is believed that the previous stages of the disease before cavity formation may be arrested by health promotion and preventive actions. Thus, the single restorative treatment of the carious cavity does not ensure the control of the disease process and it is necessary to intervene also in its causes to avoid new cavities and recurrences. .
b. Main risks factors
• Cultural, social and economic factors
• Lack of access to fluoride
• Defficient mechanical control of the biofilm (bacterial plaque)
• Excessive and frequent sugar consumption
• Xerostomia
Although the dental caries is yet a problem of Public Health, its high incidence and prevalence is slowly decreasing.
1. Concept and risksa. Conceptual and
Epidemiological Aspects
b. Main risks factors
Page 1
2. Collective Approacha. Surveillance Actions in
Risk and Needs in Oral Health
b. Health Promotional Actions
c. Educational and Preventive Actions
d. Universalization of the Access to Toothbrush and Fluoridated Dentifrice
Page 2
3. Individual Approacha. Diagnosisb. Treatmentc. Restoration/
Rehabilitationd. MaintenancePage 2
4. Treatmenta. Oral Hygiene
Instructions b. Professional Plaque
Removalc. Adaptation to oral
environmentd. Disease activity
controle. Restoration/
RehabilitationPage 3
5. Atraumatic Restorative Treatment (ART)a. Collective approachb. Indicated materialsc. Operative stepsd. Sealing of Permanente
first molars by the ART technique
e. Longevityf. Samples and
experiencesPage 3
6. References and Credits
Page 4
Capítulos Atualizado e Ilustrado
Tooth 54 presented extensive caries on the occlusal surface extensive - It was
kindly provided by the team of Pediatric Dentistry of FOUSP
UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 2
2. Collective Approach
a. Surveillance Actions in Risk and Needs in Oral Health
! As a multifactorial disease, caries is affected by social and economic conditions.
! Health actions to the control of caries should be directed to the population at social risk, providing access to treatments and fluoride use (fluoridated water and fluoridated dentifrice).
! Monitoring should be encouraged as to indicators such as dmft/DMFT mean and the percentages of groups free of caries at ages 5 and 12 as a minimum surveillance of dental caries. Each city should develop this monitoring up to the 18-year-old group, as well as track teeth loss according to its possibilities for a minimum period of four years in order to follow the historical series. For these populations, surveillance disease activity signs (white spots and cavities) in collective environments (schools, working places and nurseries) optimize the intervention planning of each reality.
b. Health Promotional Actions
! Intersectional and educational public health measures are necessary to control and prevent caries in the population. They should provide access to some form of fluoride, reduction in sugar consumption and availability of systematic information about risk factors and self-care. It is necessary to have policies related to the improvement of social and economic conditions, quality of life and access to the use of instruments of hygiene and support to health maintenance. As to this aspect, the health team must be committed to planning, organizing and providing technical support to the municipal
management so that effective priority is given to health promotion actions.
Fluoridation of the water supply: Fluoridation of the water supply is considered a safe and efficient method to prevent dental caries, reaching the whole population that has access to treated water. The implementation of water fluoridation should be a political priority, as well as ensuring the monitoring of the fluoride content in water.
c. Educational and Preventive Actions
! They are performed with groups of people in the social spaces (day care units, schools, working place, community) and spaces of the health unit. Preschool and school children may be the focus of these actions because of the impact of preventive and educational measures in this age group and the importance of acting in a period when habits are established. Other groups can be locally defined according to risk, epidemiological data or local criteria. It is advised to increase access to these actions involving the families.
! Collective actions should be preferably performed by the auxiliary personnel in order to maximize the dentist’s work as to clinical activities. The collective approach can include the following procedures:
• Epidemiological examination
• Oral Health education
• Supervised tooth brushing
• Delivery of tooth brush and fluoridated dentifrice and, whenever possible, dental floss
• Topical Fluoride Application (TFA): To establish topical fluoride application collectively, attention must be given to the epidemiological situation of the local populations where action will be taken.
! Its universal reach is only recommended to the populations where one or more of the following situations occur: exposure to non-fluoridated supply water or with contents below 0.4 ppmF and no access to fluoridated dentifrice, DMFT higher than 3 and lower than 30% individuals caries-free at 12 years of age. TFA can be performed as weekly or daily fluoridated mouth rinses or quarterly fluoride gel application in the toothbrush, tray or strokes with a brush.
d. Universalization of the Access to Toothbrush and Fluoridated Dentifrice
! Once brushing with fluoridated dentifrice is of major importance in caries prevention, assuring its access on a universal basis should be considered an important policy in the actions on oral health. Universalization of dental floss access should always be encouraged.
3. Individual Approach
a. Diagnosis
! Visual diagnosis is used to identify the carious lesion. It is done by clinical examination and may be supported by radiographs. It is important to evaluate:
• Signs of disease activity: active lesions (rough white and opaque spots in enamel or light brown cavities with soft dentinal tissue) or inactive (bright white spots or cavities with dark smooth bright and hard dentinal tissue).
•Evaluation of present risk factors
U P D A T I N G N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L
C L U B E D A S E Q U Ó I A
UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 3
b. Treatment
The treatment of active caries disease has the objective of reestablishing the balance between the demineralization processes and remineralization of the dental structures, arresting or reducing the progression of lesions and promoting restoration/rehabilitation whenever necessary.
Treatment should be customized and comprises:
•Oral hygiene instructions including: directions about tooth brushing, dental floss use, tongue cleaning and hygiene frequency.
•Professional plaque removal by means of scaling and/or adequate rotary and vibrating instruments.
•Adaptation to Oral Environment including: plaque removal, carious dentin removal and cavity sealing with temporary material (glass ionomer or modified cement) and elimination of other plaque retention factors such as root remnants and calculus.
•Control of the disease activity: assessment of the identified unbalance causes and intervention on the determining factors, including:
•Educational actions to control plaque.
•Topical fluoride use according to indication and risk until disease is controlled.
•Diet counseling.
•Stimulation of the salivary flow
c. Restoration/Rehabilitation
Decision on tooth restoration should be conservative, avoiding intervention whenever possible. Injuries restricted to dental enamel should be monitored. Dark grooves should not be opened as they indicate chronic caries. Non cavitated lesions that present color alteration indicate the possibility of dentin caries and their diagnosis should include radiographs.
When treating cavitated lesions in dentin try to maintain the maximum
amount of dental tissues, avoiding pulp exposure, mainly by maintaining disorganized dentin in deep cavities. In the cases of pulp exposure, conservative treatments (pulpotomies and cappings) should always be encouraged as opposed to dental extractions.
d. Maintenance• Maintenance recalls should be
established as a routine. Attendance is defined by evaluating the disease activity and individual risk factors and should be scheduled according to each situation. O n m a i n t e n a n c e appointments, prevention and educational actions will stimulate health care independence.
• Sealers: the use of sealers in pits and fissures is not unanimous among dentists. Its utilization should be restricted to the individual indication of risk and should not be used routinely to prevent the carious lesion. The FSP-USP (Public Health School) follows a standard, indicating the utilization in the simultaneous presence of the following conditions:
• Tooth in the oral cavity for less than 2 (two) years.
• Homologous tooth shows caries or is diseased.
• Presence of clinically detectable plaque and poor oral hygiene.
4.TreatmentOral Hygiene Instructions:
Using the dental floss
30 to 50 cm (half a meter) of floss should be removed from packaging (raffia fiber
can be used: this material is used in
costumes during Carnival. Just unravel the raffia fibers of skirts turning them
into thin threads and use the same way as described below).
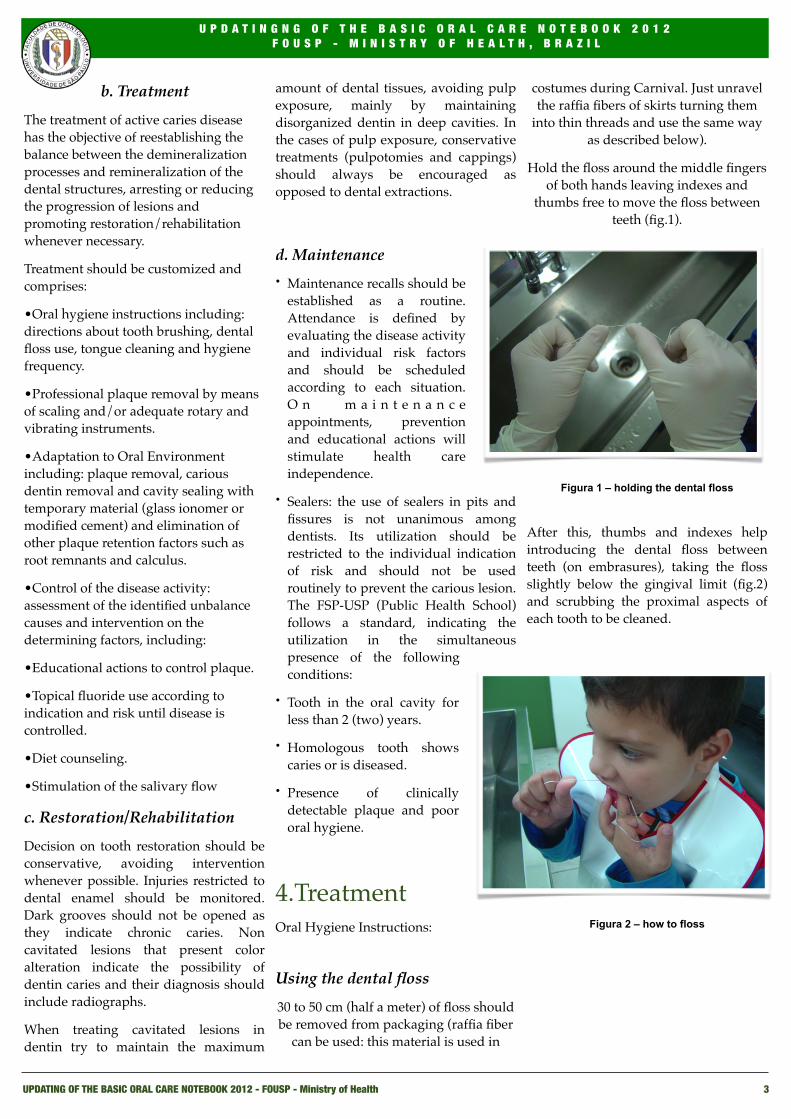
Hold the floss around the middle fingers of both hands leaving indexes and
thumbs free to move the floss between teeth (fig.1).
Figura 1 – holding the dental floss
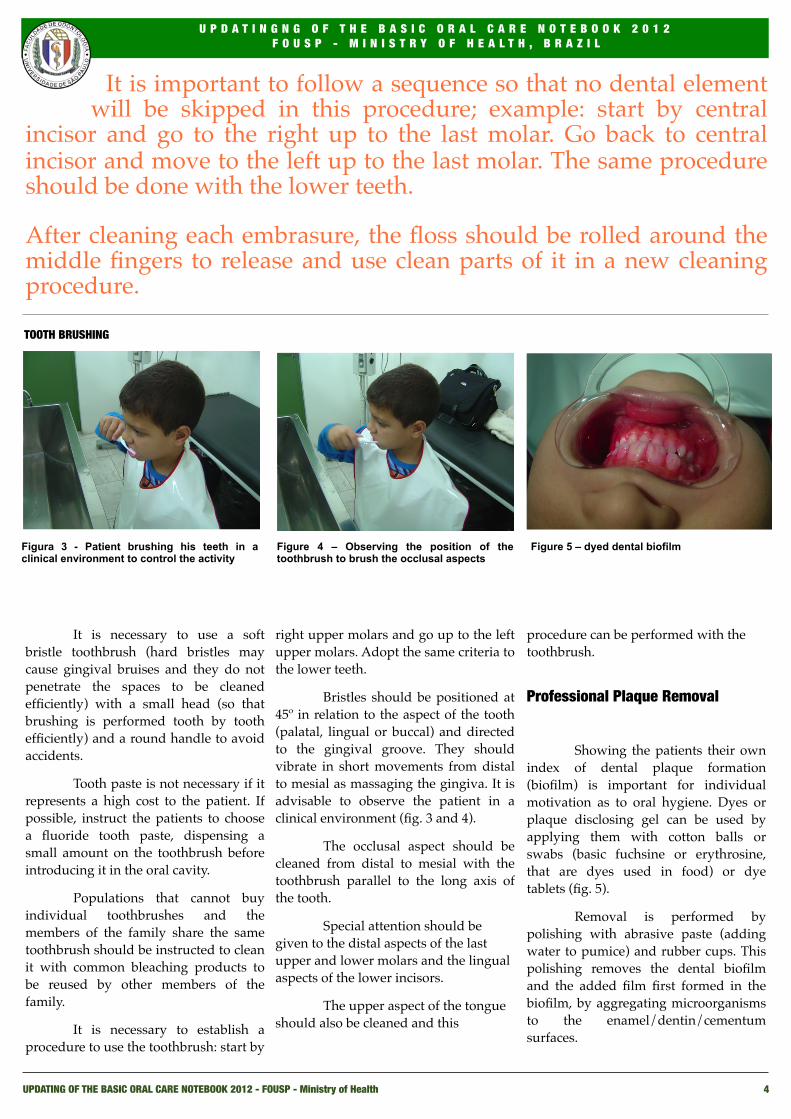
After this, thumbs and indexes help introducing the dental floss between teeth (on embrasures), taking the floss slightly below the gingival limit (fig.2) and scrubbing the proximal aspects of each tooth to be cleaned.
Figura 2 – how to floss
U P D A T I N G N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L
C L U B E D A S E Q U Ó I A
UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 4
It is important to follow a sequence so that no dental element will be skipped in this procedure; example: start by central
incisor and go to the right up to the last molar. Go back to central incisor and move to the left up to the last molar. The same procedure should be done with the lower teeth.
After cleaning each embrasure, the floss should be rolled around the middle fingers to release and use clean parts of it in a new cleaning procedure.
! It is necessary to use a soft bristle toothbrush (hard bristles may cause gingival bruises and they do not penetrate the spaces to be cleaned efficiently) with a small head (so that brushing is performed tooth by tooth efficiently) and a round handle to avoid accidents.!
! Tooth paste is not necessary if it represents a high cost to the patient. If possible, instruct the patients to choose a fluoride tooth paste, dispensing a small amount on the toothbrush before introducing it in the oral cavity.
! Populations that cannot buy individual toothbrushes and the members of the family share the same toothbrush should be instructed to clean it with common bleaching products to be reused by other members of the family.
! It is necessary to establish a procedure to use the toothbrush: start by
right upper molars and go up to the left upper molars. Adopt the same criteria to the lower teeth.
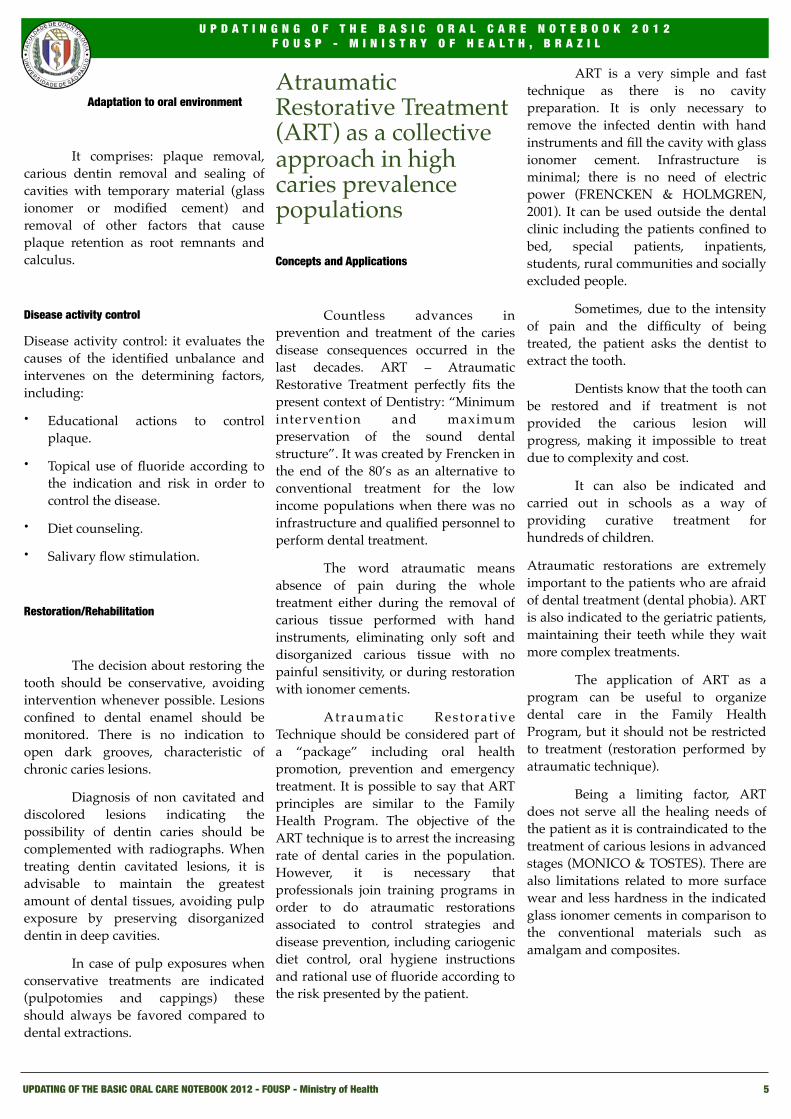
Bristles should be positioned at 45º in relation to the aspect of the tooth (palatal, lingual or buccal) and directed to the gingival groove. They should vibrate in short movements from distal to mesial as massaging the gingiva. It is advisable to observe the patient in a clinical environment (fig. 3 and 4).
! The occlusal aspect should be cleaned from distal to mesial with the toothbrush parallel to the long axis of the tooth.
! Special attention should be given to the distal aspects of the last upper and lower molars and the lingual aspects of the lower incisors.
! The upper aspect of the tongue should also be cleaned and this
procedure can be performed with the toothbrush.
Professional Plaque Removal
! Showing the patients their own index of dental plaque formation (biofilm) is important for individual motivation as to oral hygiene. Dyes or plaque disclosing gel can be used by applying them with cotton balls or swabs (basic fuchsine or erythrosine, that are dyes used in food) or dye tablets (fig. 5).
! Removal is performed by polishing with abrasive paste (adding water to pumice) and rubber cups. This polishing removes the dental biofilm and the added film first formed in the biofilm, by aggregating microorganisms to the enamel/dentin/cementum surfaces.
U P D A T I N G N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L
Figura 3 - Patient brushing his teeth in a clinical environment to control the activity
Figure 4 – Observing the position of the toothbrush to brush the occlusal aspects
Figure 5 – dyed dental biofilm
TOOTH BRUSHING
C L U B E D A S E Q U Ó I A
UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 5
Adaptation to oral environment
! It comprises: plaque removal, carious dentin removal and sealing of cavities with temporary material (glass ionomer or modified cement) and removal of other factors that cause plaque retention as root remnants and calculus.
Disease activity control
Disease activity control: it evaluates the causes of the identified unbalance and intervenes on the determining factors, including:
• Educational actions to control plaque.
• Topical use of fluoride according to the indication and risk in order to control the disease.
• Diet counseling.
• Salivary flow stimulation.
Restoration/Rehabilitation
! The decision about restoring the tooth should be conservative, avoiding intervention whenever possible. Lesions confined to dental enamel should be monitored. There is no indication to open dark grooves, characteristic of chronic caries lesions.
! Diagnosis of non cavitated and discolored lesions indicating the possibility of dentin caries should be complemented with radiographs. When treating dentin cavitated lesions, it is advisable to maintain the greatest amount of dental tissues, avoiding pulp exposure by preserving disorganized dentin in deep cavities.
! In case of pulp exposures when conservative treatments are indicated (pulpotomies and cappings) these should always be favored compared to dental extractions.
Atraumatic Restorative Treatment (ART) as a collective approach in high caries prevalence populations
Concepts and Applications
! Countless advances in prevention and treatment of the caries disease consequences occurred in the last decades. ART – Atraumatic Restorative Treatment perfectly fits the present context of Dentistry: “Minimum intervention and maximum preservation of the sound dental structure”. It was created by Frencken in the end of the 80’s as an alternative to conventional treatment for the low income populations when there was no infrastructure and qualified personnel to perform dental treatment.
! The word atraumatic means absence of pain during the whole treatment either during the removal of carious tissue performed with hand instruments, eliminating only soft and disorganized carious tissue with no painful sensitivity, or during restoration with ionomer cements.
! Atraumatic Restorat ive Technique should be considered part of a “package” including oral health promotion, prevention and emergency treatment. It is possible to say that ART principles are similar to the Family Health Program. The objective of the ART technique is to arrest the increasing rate of dental caries in the population. However, it is necessary that professionals join training programs in order to do atraumatic restorations associated to control strategies and disease prevention, including cariogenic diet control, oral hygiene instructions and rational use of fluoride according to the risk presented by the patient.
! ART is a very simple and fast technique as there is no cavity preparation. It is only necessary to remove the infected dentin with hand instruments and fill the cavity with glass ionomer cement. Infrastructure is minimal; there is no need of electric power (FRENCKEN & HOLMGREN, 2001). It can be used outside the dental clinic including the patients confined to bed, special patients, inpatients, students, rural communities and socially excluded people.
! Sometimes, due to the intensity of pain and the difficulty of being treated, the patient asks the dentist to extract the tooth.
! Dentists know that the tooth can be restored and if treatment is not provided the carious lesion will progress, making it impossible to treat due to complexity and cost.
! It can also be indicated and carried out in schools as a way of providing curative treatment for hundreds of children.
Atraumatic restorations are extremely important to the patients who are afraid of dental treatment (dental phobia). ART is also indicated to the geriatric patients, maintaining their teeth while they wait more complex treatments.
! The application of ART as a program can be useful to organize dental care in the Family Health Program, but it should not be restricted to treatment (restoration performed by atraumatic technique).
! Being a limiting factor, ART does not serve all the healing needs of the patient as it is contraindicated to the treatment of carious lesions in advanced stages (MONICO & TOSTES). There are also limitations related to more surface wear and less hardness in the indicated glass ionomer cements in comparison to the conventional materials such as amalgam and composites.
U P D A T I N G N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L
C L U B E D A S E Q U Ó I A
UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 6
ADEQUATE MATERIALS IN THE ATRAUMATIC RESTORATIVE TECHNIQUE
!
! C h e m i c a l l y a c t i v a t e d conventional glass ionomer cement is the correct material to the restorative stage because its main characteristics include adhesion to dental structures, biocompatibility, fluoride release and assimilation. It is fundamental to manipulate the glass ionomer cements correctly to assure a good clinical result.
!
! Glass ionomer cements developed to apply ART present changes as to curing time. This time was reduced by increasing tartaric acid in the formulation and accelerating curing of the material. They also show less surface wear as a consequence of the increase in the powder-liquid ratio, making it difficult to manipulate the material, once it is necessary to add more powder to only a drop of liquid.
!
Due to less surface wear, they can be used in areas where there is greater masticatory demand (RAGGIO & IMPARATO, 2005).
!
! The improved zinc oxide-eugenol cement showed similar result as to durability when compared to glass ionomer cement in restorations done with
!
! ART after 12 month clinical evaluation. The conventional glass ionomer cement had a superior performance as to masticatory efficiency (OLIVEIRA, 2000).
OPERATIVE STEPS IN THE ATRAUMATIC RESTORATIVE TECNIQUE
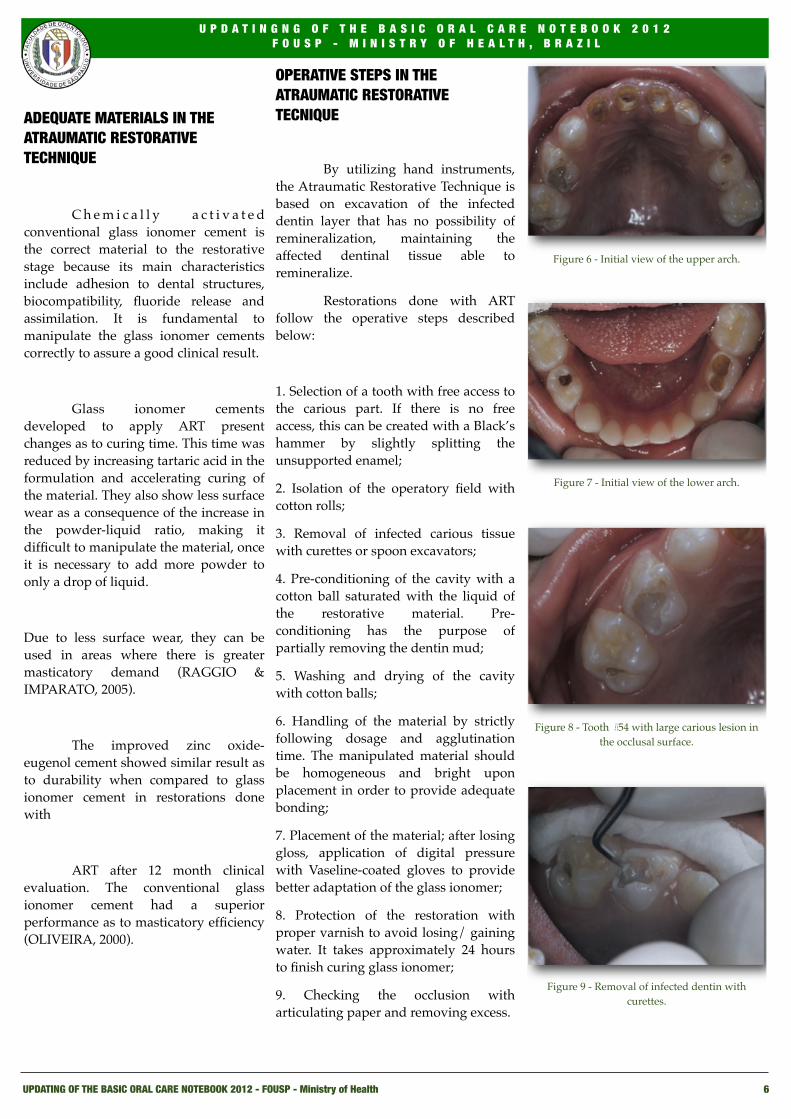
! By utilizing hand instruments, the Atraumatic Restorative Technique is based on excavation of the infected dentin layer that has no possibility of remineralization, maintaining the affected dentinal tissue able to remineralize.
! Restorations done with ART follow the operative steps described below:
1. Selection of a tooth with free access to the carious part. If there is no free access, this can be created with a Black’s hammer by slightly splitting the unsupported enamel;
2. Isolation of the operatory field with cotton rolls;
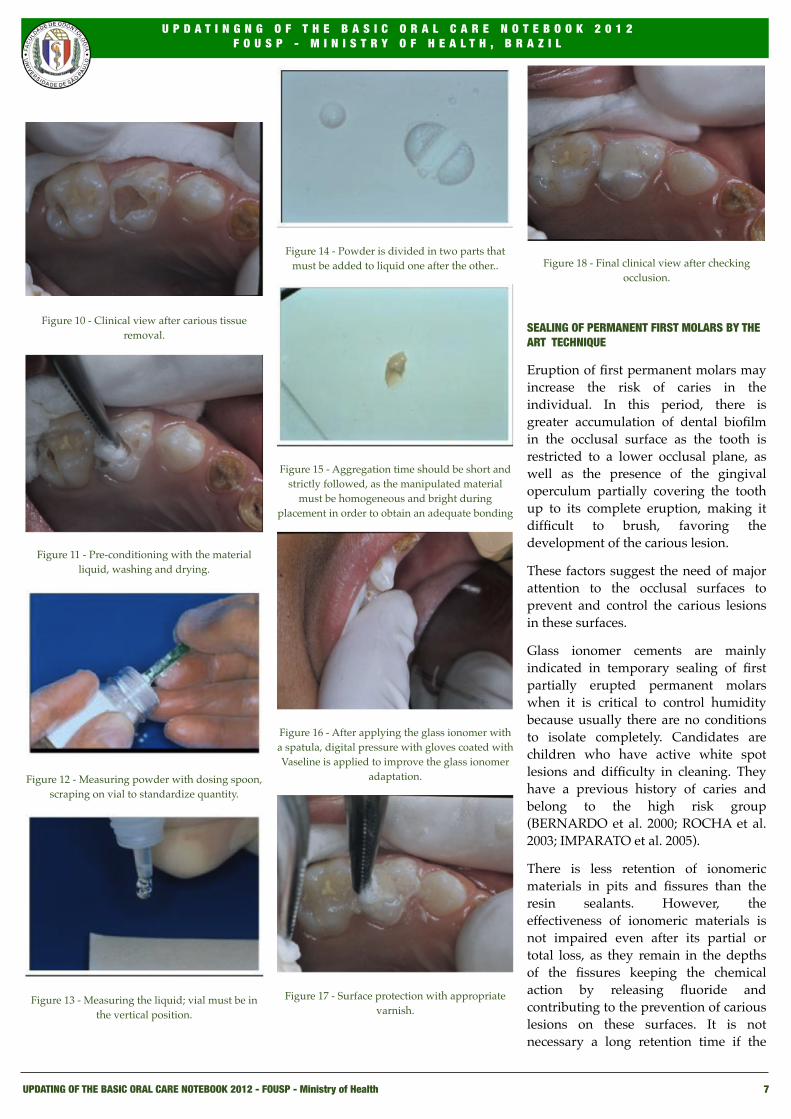
3. Removal of infected carious tissue with curettes or spoon excavators;
4. Pre-conditioning of the cavity with a cotton ball saturated with the liquid of the restorative material. Pre-conditioning has the purpose of partially removing the dentin mud;
5. Washing and drying of the cavity with cotton balls;
6. Handling of the material by strictly following dosage and agglutination time. The manipulated material should be homogeneous and bright upon placement in order to provide adequate bonding;
7. Placement of the material; after losing gloss, application of digital pressure with Vaseline-coated gloves to provide better adaptation of the glass ionomer;
8. Protection of the restoration with proper varnish to avoid losing/ gaining water. It takes approximately 24 hours to finish curing glass ionomer;
9. Checking the occlusion with articulating paper and removing excess.
Figure 6 - Initial view of the upper arch.
Figure 7 - Initial view of the lower arch.
Figure 8 - Tooth #54 with large carious lesion in the occlusal surface.
Figure 9 - Removal of infected dentin with curettes.
U P D A T I N G N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L
C L U B E D A S E Q U Ó I A
UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 7
Figure 10 - Clinical view after carious tissue removal.
Figure 11 - Pre-conditioning with the material liquid, washing and drying.
Figure 12 - Measuring powder with dosing spoon, scraping on vial to standardize quantity.
Figure 13 - Measuring the liquid; vial must be in the vertical position.
Figure 14 - Powder is divided in two parts that must be added to liquid one after the other..
Figure 15 - Aggregation time should be short and strictly followed, as the manipulated material
must be homogeneous and bright during placement in order to obtain an adequate bonding
Figure 16 - After applying the glass ionomer with a spatula, digital pressure with gloves coated with Vaseline is applied to improve the glass ionomer
adaptation.
Figure 17 - Surface protection with appropriate varnish.
Figure 18 - Final clinical view after checking occlusion.
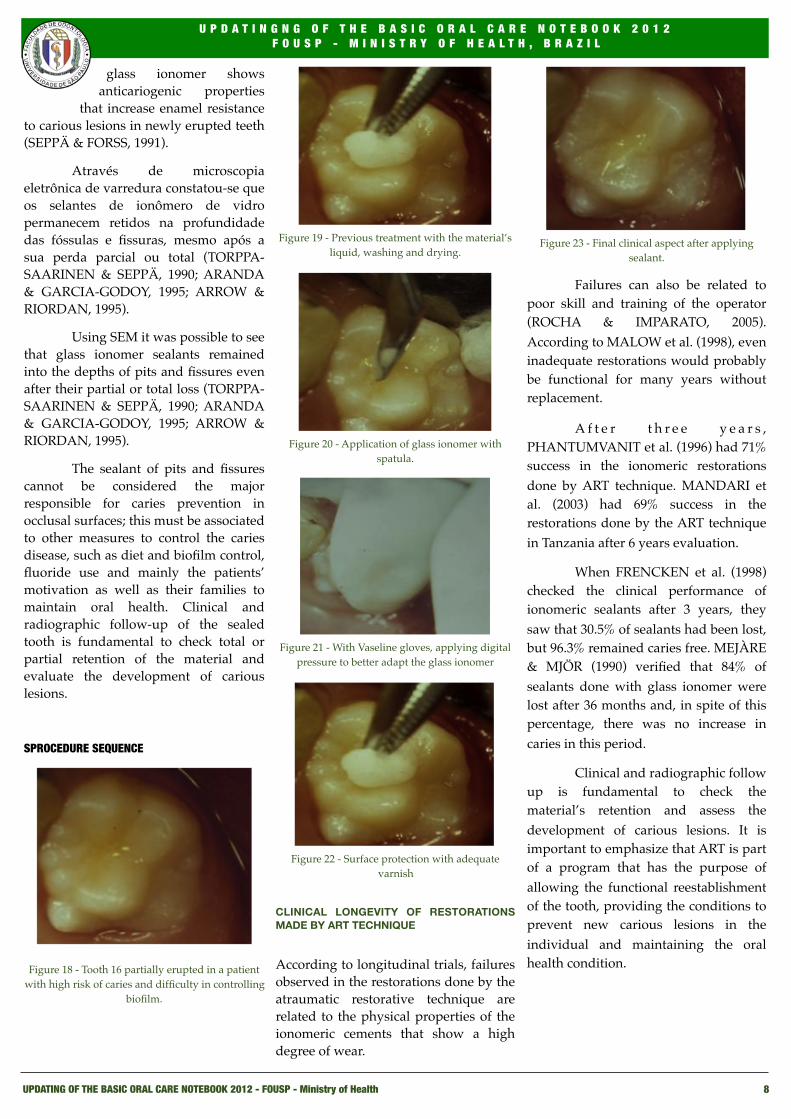
SEALING OF PERMANENT FIRST MOLARS BY THE ART TECHNIQUE
Eruption of first permanent molars may increase the risk of caries in the individual. In this period, there is greater accumulation of dental biofilm in the occlusal surface as the tooth is restricted to a lower occlusal plane, as well as the presence of the gingival operculum partially covering the tooth up to its complete eruption, making it difficult to brush, favoring the development of the carious lesion.
These factors suggest the need of major attention to the occlusal surfaces to prevent and control the carious lesions in these surfaces.
Glass ionomer cements are mainly indicated in temporary sealing of first partially erupted permanent molars when it is critical to control humidity because usually there are no conditions to isolate completely. Candidates are children who have active white spot lesions and difficulty in cleaning. They have a previous history of caries and belong to the high risk group (BERNARDO et al. 2000; ROCHA et al. 2003; IMPARATO et al. 2005).
There is less retention of ionomeric materials in pits and fissures than the resin sealants. However, the effectiveness of ionomeric materials is not impaired even after its partial or total loss, as they remain in the depths of the fissures keeping the chemical action by releasing fluoride and contributing to the prevention of carious lesions on these surfaces. It is not necessary a long retention time if the
U P D A T I N G N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L
C L U B E D A S E Q U Ó I A
UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 8
glass ionomer shows anticariogenic properties
that increase enamel resistance to carious lesions in newly erupted teeth (SEPPÄ & FORSS, 1991).
! Através de microscopia eletrônica de varredura constatou-se que os selantes de ionômero de vidro permanecem retidos na profundidade das fóssulas e fissuras, mesmo após a sua perda parcial ou total (TORPPA-SAARINEN & SEPPÄ, 1990; ARANDA & GARCIA-GODOY, 1995; ARROW & RIORDAN, 1995).
! Using SEM it was possible to see that glass ionomer sealants remained into the depths of pits and fissures even after their partial or total loss (TORPPA-SAARINEN & SEPPÄ, 1990; ARANDA & GARCIA-GODOY, 1995; ARROW & RIORDAN, 1995).
! The sealant of pits and fissures cannot be considered the major responsible for caries prevention in occlusal surfaces; this must be associated to other measures to control the caries disease, such as diet and biofilm control, fluoride use and mainly the patients’ motivation as well as their families to maintain oral health. Clinical and radiographic follow-up of the sealed tooth is fundamental to check total or partial retention of the material and evaluate the development of carious lesions.
SPROCEDURE SEQUENCE
Figure 18 - Tooth 16 partially erupted in a patient with high risk of caries and difficulty in controlling
biofilm.
Figure 19 - Previous treatment with the material’s liquid, washing and drying.
Figure 20 - Application of glass ionomer with spatula.
Figure 21 - With Vaseline gloves, applying digital pressure to better adapt the glass ionomer
Figure 22 - Surface protection with adequate varnish
CLINICAL LONGEVITY OF RESTORATIONS MADE BY ART TECHNIQUE
According to longitudinal trials, failures observed in the restorations done by the atraumatic restorative technique are related to the physical properties of the ionomeric cements that show a high degree of wear.
Figure 23 - Final clinical aspect after applying sealant.
! Failures can also be related to poor skill and training of the operator (ROCHA & IMPARATO, 2005). According to MALOW et al. (1998), even inadequate restorations would probably be functional for many years without replacement.
! A f t e r t h r e e y e a r s , PHANTUMVANIT et al. (1996) had 71% success in the ionomeric restorations done by ART technique. MANDARI et al. (2003) had 69% success in the restorations done by the ART technique in Tanzania after 6 years evaluation.
! When FRENCKEN et al. (1998) checked the clinical performance of ionomeric sealants after 3 years, they saw that 30.5% of sealants had been lost, but 96.3% remained caries free. MEJÀRE & MJÖR (1990) verified that 84% of sealants done with glass ionomer were lost after 36 months and, in spite of this percentage, there was no increase in caries in this period.
! Clinical and radiographic follow up is fundamental to check the material’s retention and assess the development of carious lesions. It is important to emphasize that ART is part of a program that has the purpose of allowing the functional reestablishment of the tooth, providing the conditions to prevent new carious lesions in the individual and maintaining the oral health condition.
U P D A T I N G N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L
C L U B E D A S E Q U Ó I A
UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 9
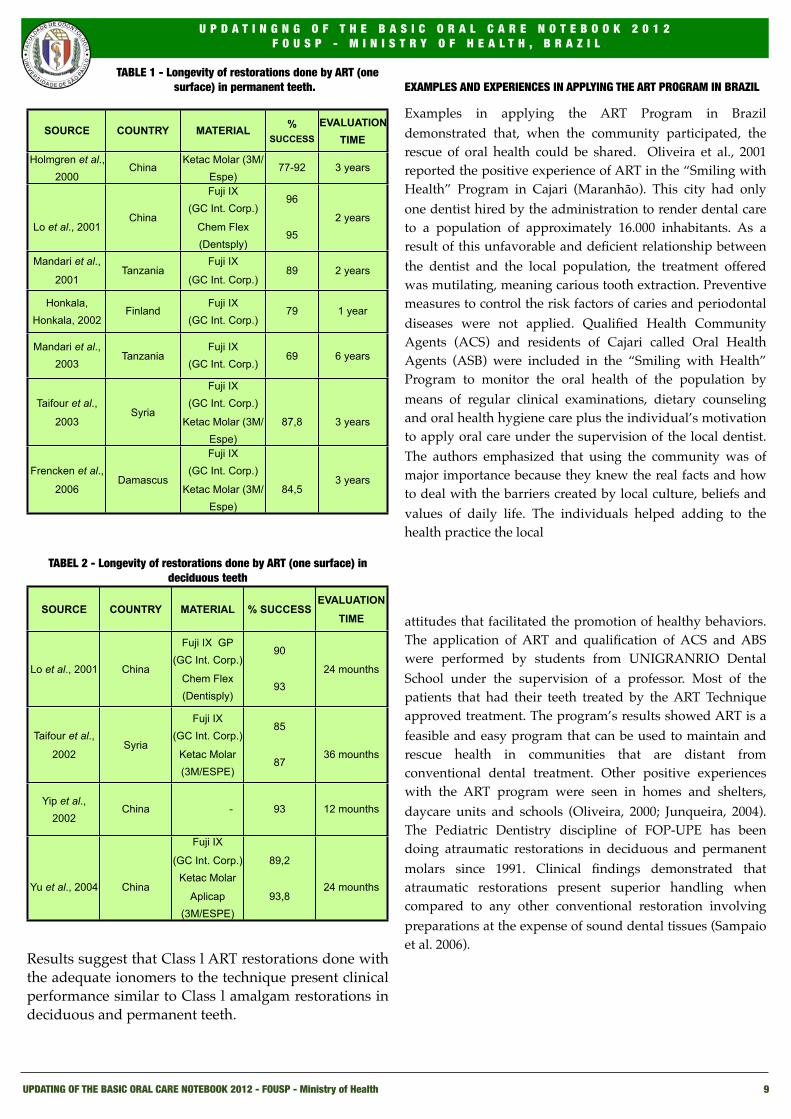
TABLE 1 - Longevity of restorations done by ART (one surface) in permanent teeth.
SOURCE COUNTRY MATERIAL % SUCCESS
EVALUATION TIME
Holmgren et al., 2000
ChinaKetac Molar (3M/
Espe)77-92 3 years
Lo et al., 2001China
Fuji IX(GC Int. Corp.)
Chem Flex (Dentsply)
96
952 years
Mandari et al.,
2001Tanzania
Fuji IX
(GC Int. Corp.)89 2 years
Honkala, Honkala, 2002
FinlandFuji IX
(GC Int. Corp.)79 1 year
Mandari et al., 2003
TanzaniaFuji IX
(GC Int. Corp.)69 6 years
Taifour et al.,
2003Syria
Fuji IX(GC Int. Corp.)
Ketac Molar (3M/Espe)
87,8 3 years
Frencken et al.,
2006Damascus
Fuji IX(GC Int. Corp.)
Ketac Molar (3M/Espe)
84,53 years
TABEL 2 - Longevity of restorations done by ART (one surface) in deciduous teeth
SOURCE COUNTRY MATERIAL % SUCCESSEVALUATION
TIME
Lo et al., 2001 China
Fuji IX GP(GC Int. Corp.)
Chem Flex (Dentisply)
90
9324 mounths
Taifour et al.,
2002Syria
Fuji IX(GC Int. Corp.)
Ketac Molar (3M/ESPE)
85
8736 mounths
Yip et al., 2002
China - 93 12 mounths
Yu et al., 2004 China
Fuji IX
(GC Int. Corp.)Ketac Molar
Aplicap(3M/ESPE)
89,2
93,824 mounths
Results suggest that Class l ART restorations done with the adequate ionomers to the technique present clinical performance similar to Class l amalgam restorations in deciduous and permanent teeth.
EXAMPLES AND EXPERIENCES IN APPLYING THE ART PROGRAM IN BRAZIL
Examples in applying the ART Program in Brazil demonstrated that, when the community participated, the rescue of oral health could be shared. Oliveira et al., 2001 reported the positive experience of ART in the “Smiling with Health” Program in Cajari (Maranhão). This city had only one dentist hired by the administration to render dental care to a population of approximately 16.000 inhabitants. As a result of this unfavorable and deficient relationship between the dentist and the local population, the treatment offered was mutilating, meaning carious tooth extraction. Preventive measures to control the risk factors of caries and periodontal diseases were not applied. Qualified Health Community Agents (ACS) and residents of Cajari called Oral Health Agents (ASB) were included in the “Smiling with Health” Program to monitor the oral health of the population by means of regular clinical examinations, dietary counseling and oral health hygiene care plus the individual’s motivation to apply oral care under the supervision of the local dentist. The authors emphasized that using the community was of major importance because they knew the real facts and how to deal with the barriers created by local culture, beliefs and values of daily life. The individuals helped adding to the health practice the local
attitudes that facilitated the promotion of healthy behaviors. The application of ART and qualification of ACS and ABS were performed by students from UNIGRANRIO Dental School under the supervision of a professor. Most of the patients that had their teeth treated by the ART Technique approved treatment. The program’s results showed ART is a feasible and easy program that can be used to maintain and rescue health in communities that are distant from conventional dental treatment. Other positive experiences with the ART program were seen in homes and shelters, daycare units and schools (Oliveira, 2000; Junqueira, 2004). The Pediatric Dentistry discipline of FOP-UPE has been doing atraumatic restorations in deciduous and permanent molars since 1991. Clinical findings demonstrated that atraumatic restorations present superior handling when compared to any other conventional restoration involving preparations at the expense of sound dental tissues (Sampaio et al. 2006).
U P D A T I N G N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L
C L U B E D A S E Q U Ó I A
UPDATING OF THE BASIC ORAL CARE NOTEBOOK 2012 - FOUSP - Ministry of Health 10
UPDATINGNG OF THE BASIC ORAL CARE NOTEBOOK 2012 (original link) and images:
Profa. Luciana Butini Oliveira – SLMandic
Prof. Marcelo Strazzeri Bönecker - FOUSP
REFERENCES
Aranda M, Garcia-Godoy F. Clinical evaluation of the retention and wear of a light-cured pit and fissure glass ionomer sealant. J Clin Ped Dent 1995;19(4): 273-277.
Arrow P, Riordan PJ. Retention and caries preventive effects of a GIC and a resin based fissure sealant. Community Dent Oral Epidemiol 1995;23(5): 282-285.
Bernardo PC. et al. Avaliação clínica de um cimento de ionômero de vidro utilizado como selante oclusal. Pesqui Odontol Bras 2000;14(1):53-57.
Frencken JE, Makoni F, Sithole WD. ART restorations and glass ionomer sealants in Zimbabue: survival after 3 years. Community Dent Oral Epidemiol 1998;26(6):372-381.
Frencken JE, Holmgren CJ. Tratamento Restaurador Atraumático para a cárie dentária. São Paulo: Santos, 2001. 106p. (livro).
Frencken JE, Taifour D, van’t Hof MA. Survival of ART and amalgam restorations In permanent teeth of children after 6.3 years. J Dent Res 2006; 85(7): 622-626.
Honkala S, Honkala E. Atraumatic dental treatment among finnish elderly persons. J Oral Rehabil, v.29, p.435-440, 2002.
Holmgren CJ, Lo ECM, Hu DY, Wan HC: ART restorations and sealants placed in Chinese school children. Results after three years. Community Dent Oral Epidemiol 2000; 28: 314-320.
Imparato JCP, Delmondes FS, Rodrigues-Filho LE. Selamento provisório de primeiros molares permanentes em erupção. In: Imparato JCP et al. Tratamento Restaurador Atraumático. Técnicas de mínima intervenção para o tratamento da doença cárie dentária. Curitiba: Editora Maio, 2005. Cap.9, p.135-147. (livro)
Junqueira FP. Avaliação de um programa de tratamento restaurador atraumático modificado em crianças institucionalizadas de 02 a 05 anos, 2002. Dissertação (Mestrado em Odontopediatria). São Leopoldo Mandic. Campinas, 2004. 89f.
Lo ECM, Holmgren CJ. Provision of atraumatic restorative treatment (ART) restorations to Chinese pre-school children: A 30 month evaluation. Int J Paediatr Dent 2001a; 11:3-10.
Lo ECM, Luo Y, Fan MW, Wei SHY. Clinical investigation of two glass-ionomer restoratives used with the atraumatic restorative treatment approach in China: two-years results. Caries Res 2001b; 35: 458-463.
Mallow PK, Durward CS, Klaipo, M. Restoration of permanent teeth in young rural children in Cambodia using the atraumatic restorative treatment (ART) technique and Fuji II glass ionomer cement. Int J Pediatr Dent 1998;8:35-40.
Mandari GJ, Truin GJ, van’t Hof MA et al. Effectiveness of three minimal intervention approaches for managing dental caries: survival of restorations after 2 years. Caries Res 2001; 35: 90-94.
Mandari GJ, Frencken JE, van Hof MA. Six-year success rates of oclusal amalgam and glass-ionomer restorations placed using three minimal intervention approaches. Caries Res 2003;37(4):246-253.
Mejàre I, Mjör IA. Glass ionomer and resin-based fissure sealants: a critical study. Scand J Dent Res 1990;98(4):345-350.
Mônico M, Tostes M. Tratamento restaurador simplificado para atendimento infantil (A.R.T.). J Bras Odontopediatr Odontol Bebê 1998;1(4):9-16.
Oliveira LMC. Avaliação de um programa de tratamento restaurador atraumático em crianças institucionalizadas. Tese (Doutorado em Odontopediatria). Rio de Janeiro, 2000. 168f. Universidade Federal do Rio de Janeiro, Rio de Janeiro.
Oliveira LMC et al. Avaliação qualitativa do impacto do ART na população de Cajari. v.15, 2001.
Phantumvanit P. et al. Atraumatic restorative treatment (ART): a three-year community field trial in Thailand – survival o fone-surface restorations in the permanent dentition. J Public Health Dent 1996;56:141-145.
Raggio DP, Imparato JCP. Tratamento Restaurador Atraumático: Estudos in vitro. In: Imparato JCP. et al. Tratamento Restaurador Atraumático. Técnicas de mínima intervenção para o tratamento da doença cárie dentária. Curitiba: Editora Maio, 2005. Cap.5, p.85-93. (livro)
Rocha RO. et al. Cimento de ionômero de vidro como selante de fossas e fissuras. Rev Assoc Paul Cir Dent 2003;57(4):287-290.
Rocha RO, Imparato JCP. Tratamento Restaurador Atraumático: Estudos Clínicos. In: Imparato JCP.. et al. Tratamento Restaurador Atraumático. Técnicas de mínima
U P D A T I N G N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L
C L U B E D A S E Q U Ó I A
Caderno de Atenção Básica no 17 - Saúde Bucal - Ministério da Saúde 11
intervenção para o tratamento da doença cárie dentária. Curitiba: Editora Maio, 2005. Cap.6, p.
96-104. (livro)
Sampaio MS, Maltz M, Sperb JB, Caufield WP, Rosenblatt A, Costa MCF, Guimarães CD, Sá EMO, Coelho EBC, Guerra MAA. Tratamento restaurador atraumático no Brasil - relato de experiências. Artigo publicado no Odontologia.com.br em 11 de Maio de 2006, disponível no endereço: http://www.odontologia.com.br/artigos.asp?id=291
Schriks MCM, van Amerongen WE. Atraumatic perspective of ART: psychological aspect of treatment with or without rotary instruments. Community Dent Oral Epidemiol 2003;31(1):15-20.
Seppä l; Forss H. Resistance of occlusal fissures to desmineralization after loss of glass ionomer sealant in vitro. Pediatr Dent 1991;13(1):39-42.
Taifour D, Frencken JE, Beiruti N. Effectiveness of glass-ionomer (ART) and amalgam restorations in the deciduous dentition: results after 3 years. Caries Res 2002; 36: 437-444.
Taifour D, Frencken JE, Beiruti N et al. Comparison between restorations in the permanete dentition prodeced by hand and rotatory instrumentation – survival after 3 year. Community Dent Oral Epidemiol 2003; 31: 122-128.
Torppa-Saarinen E, Seppä l. Short-term retention of glass-ionomer fissure sealants. Proc Finn Dent Soc 1990;86(2):83-86.
Yip HK, Smales RJ, Yu C et al. The effects of two cavity preparation methods on the longevity of glass ionomer cement restorations. JADA 2002; 133:744-751.
Yu C, Yip H-K, Smales RJ. Survival of glass ionomer restorations placed in primary molars using atraumatic restorative treatment (ATR) and conventional cavity preparations: 2-years results. Int Dent J 2004; 54: 42-46.
U P D A T I N G N G O F T H E B A S I C O R A L C A R E N O T E B O O K 2 0 1 2F O U S P - M I N I S T R Y O F H E A L T H , B R A Z I L